New and emerging organ perfusion systems

Health Policy Advisory Committee on
Technology
Technology Overview
New and Emerging Organ Perfusion Systems
July 2014
© State of Queensland (Queensland Department of Health) 2014
This work is licensed under a Creative Commons Attribution Non-Commercial No Derivatives 3.0
Australia licence. In essence, you are free to copy and communicate the work in its current form for non-commercial purposes, as long as you attribute the authors and abide by the licence terms. You may not alter or adapt the work in any way.
To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/3.0/au/ deed.en.
For further information, contact the HealthPACT Secretariat at:
HealthPACT Secretariat c/o Clinical Access and Redesign Unit, Health Service and Clinical Innovation Division
Department of Health, Queensland
Level 2, 15 Butterfield St
HERSTON QLD 4029
Postal Address: GPO Box 48, Brisbane QLD 4001
Email: HealthPACT@health.qld.gov.au
Telephone: +61 7 3646 9100
For permissions beyond the scope of this licence contact: Intellectual Property Officer, Department of Health, GPO Box 48, Brisbane QLD 4001, email ip_officer@health.qld.gov.au
, phone (07) 3328
9824.
Electronic copies can be obtained from: http://www.health.qld.gov.au/healthpact
DISCLAIMER: This Overview is published with the intention of providing information of interest. It is based on information available at the time of research and cannot be expected to cover any developments arising from subsequent improvements to health technologies. This Overview is based on a limited literature search and is not a definitive statement on the safety, effectiveness or costeffectiveness of the health technology covered.
The State of Queensland acting through Queensland Health (“Queensland Health”) does not guarantee the accuracy, currency or completeness of the information in this Overview. Information may contain or summarise the views of others, and not necessarily reflect the views of Queensland
Health.
This Overview is not intended to be used as medical advice and it is not intended to be used to diagnose, treat, cure or prevent any disease, nor should it be used for therapeutic purposes or as a substitute for a health professional's advice. It must not be relied upon without verification from authoritative sources. Queensland Health does not accept any liability, including for any injury, loss or damage, incurred by use of or reliance on the information.
This Overview was commissioned by Queensland Health, in its role as the Secretariat of the Health
Policy Advisory Committee on Technology (HealthPACT). The production of this Overview was overseen by HealthPACT. HealthPACT comprises representatives from health departments in all
States and Territories, the Australian and New Zealand governments and MSAC. It is a subcommittee of the Australian Health Ministers’ Advisory Council (AHMAC), reporting to AHMAC’s
Hospitals Principal Committee (HPC). AHMAC supports HealthPACT through funding.
This Overview was prepared by Linda Mundy from the HealthPACT Secretariat.
Disease description and associated mortality and morbidity ................................. 7
Cost ............................................................................................ 17
Safety and effectiveness ............................................................ 17
Economic evaluation .................................................................. 21
Cost ............................................................................................ 24
Safety and effectiveness ............................................................ 25
Economic evaluation.................................................................. 27
Airdrive™ hypothermic kidney perfusion transport system ..................... 27
XVIVO™ and XPS lung perfusion systems .................................................. 32
Cost ............................................................................................ 34
Safety and effectiveness ........................................................... 35
Economic evaluation ................................................................. 37
Cost ........................................................................................... 39
Safety and effectiveness ........................................................... 39
Liver Assist- Hypothermic Oxygenated PErfusion - HOPE ......................... 46
Organ Care System™- OCS™ HEART .......................................................... 49
Technology, Company and Licensing
Register ID WP186
Technology name
Patient indication
New and emerging organ perfusion systems – an overview
Technologies for the preservation, optimisation and transportation of solid organs for transplantation which may maximise the number and condition of organs available to patients on transplant waiting lists.
Reason for assessment
Innovative technology that may increase the number of organs able to be transplanted, which in turn may have a significant impact on morbidity and mortality associated with long organ transplant waiting lists.
Description of the technology
Transplantation is often the only treatment option for patients with end-stage organ failure.
To preserve organ function two strategies have been used: static cold storage (SCS) and machine perfusion (MP). During the 1970s, hypothermic MP was the method of choice for
the preparation of organs for transplantation.
During hypothermic MP a preservative
solution in the temperature range of 0°C to 4°C is continuously pumped through the organ at a controlled rate. Depending on the perfusate used, oxygen and nutrients can be provided to the organ allowing metabolism to continue. In addition, toxins can be removed
if the perfusate is renewed or filtered.
By the mid-1980s the use of MP decreased when
several studies found that there was no clear clinical benefit gained from the use of this more expensive and labour intensive technology to preserve organs, in particular kidneys from ‘ideal’ donors, that is, high-quality kidneys, when compared to SCS. SCS then became
the method of choice for the preservation of high-quality organs.
flushed through with a perfusion or preservation fluid and then kept on ice for up to 24hours, which has the effect of reducing damage to the organ by slowing the metabolic rate
As with most jurisdictions, the number of patients on the transplant waiting list in Australia and New Zealand outweighs the number of organs available. Several strategies have been proposed to increase the number or organs available for transplantation, including the expansion of donor criteria to those previously deemed unsuitable, such as older donors
(>60 years) or those with pre-existing medical conditions, for example diabetes or high blood pressure. Another strategy is the use of organs donated after circulatory death (DCD), also referred to as non-beating heart donors. After withdrawal of therapy, cardiorespiratory death may usually occur within 60 minutes but may take up to 3-days. Compared to organs donated after brain death (DBD) which are perfused until the time of preservation, organs donated after circulatory death may be exposed to long periods of warm ischaemia. The deprivation of oxygen and nutrients may lead to permanent organ damage, which may
New and emerging organ perfusion systems: July 2014 1
result in post-transplant graft dysfunction or failure. Exposure to warm ischaemia results in
DCD kidneys being prone to delayed graft function while DCD lungs appear to function as well as those donated after brain death. DCD liver grafts have poor survival due to higher
DCD donors are categorised as either controlled or uncontrolled (Table 1). With
uncontrolled donors, death is usually unexpected and the length of warm ischaemia time is generally unknown. The length of time organs are exposed to warm ischaemia is more precise in controlled donors, as circulatory arrest is planned and the timing of therapy
withdrawal is known. The majority of DCD donors are category III.
protocol for DCD stipulates that if warm ischaemic time exceeds 30 minutes for liver and pancreas, 60 minutes for kidneys, and 90 minutes for lungs, then organ donation must not
Table 1
Classification of non-beating heart donors 6
Uncontrolled
Category I
Category II
Category V
Dead on arrival
Unsuccessful resuscitation
Cardiac arrest in a hospital inpatient
Controlled
Category III
Category IV
Awaiting cardiac arrest
Cardiac arrest in brain-dead donor
DCD raises significant ethical and logistical concerns. The decision to withdraw therapy in potential donors must be taken independently of any consideration of the potential for
DCD. The national protocol for DCD stipulates that a discussion regarding DCD must take place only after the withdrawal of therapy has been discussed and agreed to by family members. If DCD is agreed to, a number of ante-mortem interventions may be necessary to maintain organ viability, determine organ suitability and allow identification of suitable recipients. These interventions may include the administration of heparin to prevent
thrombi, bronchoscopy and serological tissue typing.
It should be noted that individual
Australian states and territories may have enacted laws that prohibit ante-mortem interventions such as those described.
With the expansion of the donor pool by using ‘marginal’ organs, the optimisation of organ viability between retrieval and implantation is of great importance. This need has resulted in a renewed interest in MP, which, despite higher initial costs, may result in cost-savings from a reduced risk of delayed graft function and therefore increased graft survival and improved
long-term outcomes when compared to SCS.
In the past most MP systems were
hypothermic and designed to preserve kidneys; however more systems are being developed
New and emerging organ perfusion systems: July 2014 2
for specific organs (lung, liver, heart, pancreas and small bowel) that are oxygenated hypothermic systems as well as oxygenated warm (normothermic) perfusion systems. In addition to providing oxygenation, normothermic conditions may restore cellular function and metabolism faster than hypothermic conditions, thus helping to negate the detrimental
effects of any ischemia-reperfusion injury that may have been suffered.
perfusion systems identified by the search strategy are summarised in Table 2.
In theory, MP provides an opportunity to assess the viability of the donated organ.
Specifically the presence or concentration of biomarkers in the perfusate, which may be organ specific, or MP parameters such as pressure and flow, may be used to estimate graft
The use of oxygen during perfusion is another area of interest. There has been
much debate as to the value of adding oxygen during hypothermic perfusion to support the low level of metabolism. Evidence suggests that in kidneys transplanted after warm or cold ischemic injury, oxygen restores cellular levels of adenosine triphosphate, which has a
beneficial effect. 8 In addition, many research groups are investigating the use of additives
to perfusates in an effort to minimise ischemia-reperfusion injury. In animal studies thrombin added to the preservation solution has been demonstrated to improve kidney graft recovery. Other proteins have been used to reduce immune cell fixation on the endothelial wall and other drugs have been used to stimulate metabolism, reducing
oxidative stress and acidosis. 10 Although the University of Winsconsin (UW) preservative
solution is considered the gold standard, several other products have been developed including:
the low-viscosity histidine-tryptophan-ketoglutarate (HTK) solution that may improve microperfusion;
the colloid Celsior solution, which may prevent tissue oedema;
hypertonic citrate (HOC) or Marshall’s solution that prevents entry of fluids into cells;
Perfadex, a low potassium dextran solution that is used for lungs;
Polysol, an experimental solution for ischaemically damaged organs with added amino acids, vitamins and anti-oxidants; and
Institute George Lopez (IGL-1) solution which combines the advantages of UW and
Another area of interest is the use of mesenchymal stem cells as cellular therapy in solidorgan transplantation as well as tissue-engineered organ replacement. MP may offer a means of delivering the stem cells throughout the donated organ, and it is thought that stem cells may reduce ischemia-reperfusion injury and to promote graft survival by reducing
acute and chronic rejection. 4
Company or developer
New and emerging organ perfusion systems: July 2014 3
Stage of development in Australia
Some MP systems would be considered investigational; however some systems such as the
LifePort®, the Organ Care Systems HEART and LUNG, and the Vivoline® LS1 are nearly established in Australia.
Yet to emerge
Experimental
Investigational
Nearly established
Established
Established but changed indication or modification of technique
Should be taken out of use
Licensing, reimbursement and other approval
Several organ perfusion systems were identified, some of which are listed on the Australian
Register of Therapeutic Goods. Table 2 summarises the regulatory status of these systems.
New and emerging organ perfusion systems: July 2014 4
Table 2 Summary of identified perfusion systems
System name Company Organ
XVIVO Organ
Chamber™ (manual)
XPS
Distributed by Vitrolife
Pty Ltd, Victoria
Lung
Description/stage of development
Intended to be used as a temporary receptacle for isolated donor lungs in preparation for eventual transplantation into a recipient.
Normothermic
Regulatory status
XVIVO
Listed on the ARTG: 177195
CE marked
Not FDA approved
XPS
Not approved by TGA, FDA or CE Marked
Vivoline ® LS1
Vivoline Medical, Lund,
Sweden. Distributed by
Magee Medical Pty Ltd
(NSW, Australia)
Organ Care System™
Transmedics ® Pty Ltd
LifePort Kidney
Transporter
Organ Recovery
Systems Inc (Chicago
USA)
Distributed by Emergo
Asia Pacific Pty Ltd
(Sydney, Australia)
Sherpa Pak™ cardiac transport
Sherpa Perfusion™
Cardiac Transport
System
Paragonix Technologies
Inc (Massachusetts,
USA)
Lung
Intended for ex-vivo reconditioning, evaluation and preservation of lungs after donation and before transplantation for up to 24 hours.
Normothermic
Listed on the ARTG: 188872 and 188873
(chamber set)
CE marked
Not FDA approved
OCS™ HEART
OCS™ LUNG
Kidney
Liver
A portable perfusion, ventilation, and monitoring system used to support and maintain an organ in a near-physiologic state especially during transport to the receiver hospital until it is transplanted.
Normothermic
Kidney:
A portable MP unit designed to contain and perfuse a transplantable kidney under cold and aseptic conditions.
Hypothermic
In use at the Princess Alexandria Hospital in Queensland
Listed on the ARTG: 146269 (organ not specified)
CE marked
Not FDA approved
Kidney:
Listed on the ARTG: 164957
FDA approval in 2003
European CE mark in 2004
Liver:
Submission to the FDA
Heart
Kidney
Oxygenated hypothermic organ transport.
Cardiac:
FDA approved February 2013
Kidney:
Submission to the FDA Dec 2013
New and emerging organ perfusion systems: July 2014 5
System name
OrganOx metra™
WAVES
RM3 ®
Kidney Assist
Lung Assist
Liver Assist
ECOPS
Airdrive™
LifeCradle ® HR
Company
OrganOx ® Ltd (Oxford,
United Kingdom)
IGL-group (France), formerly Waters Medical
Systems (USA)
Organ Assist,
Groningen, The
Netherlands
Portable Organ
Perfusion, Amsterdam,
The Netherlands
Organ Transport
Systems, Inc (Texas,
USA)
VASOWAVE ®
TBC
Smart Perfusion (USA)
Perfusion Solutions Pty
Ltd (Victoria, Australia)
Organ
Liver
Kidney
Kidney
Lung
Liver
Kidney
Heart
Kidney
Liver
Heart
Description/stage of development
Fully automated normothermic liver perfusion device.
Regulatory status
Anticipate CE mark early 2014
Pulsatile hypothermic MP of kidneys for preservation, transportation, and eventual transplantation into a recipient
Both CE marked
Both FDA approved Feb 2012
Portable oxygenated hypothermic MP for kidney, lung and liver.
ECOPS: Extra Corporal Organ Perfusion System of Organ Assist. For pulsatile, normothermic and oxygenated perfusion of in-situ abdominal donor organs (liver, kidneys, small bowel and pancreas).
All CE marked
A portable, disposable sterile hypothermic organ perfusion transport system.
CE marked
Seeking 510k from FDA in Q3 of 2014
Hypothermic portable cardiac perfusion system.
An investigative device in the preclinical stage of development.
An investigative device in the preclinical stage of development.
ARTG = Australian Register of Therapeutic Goods, MP = machine perfusion, FDA = the US Food and Drug Administration
CE marked
Not yet tested extensively on humans or approved for commercial sale by the
TGA, FDA or by any other regulatory body.
Not yet tested extensively on humans or approved for commercial sale by the
TGA, FDA or by any other regulatory body.
New and emerging organ perfusion systems: July 2014 6
Technology type
Technology use
Patient Indication and Setting
Device
Therapeutic
Disease description and associated mortality and morbidity
Chronic kidney disease
Kidney disease is classified into five stages of disease severity based on evidence of kidney damage and the degree of kidney function reduction, classified by glomerular filtration rate
(GFR). Patients with chronic kidney disease (CKD stage 5 a
) or end-stage kidney disease
(ESKD) may need to be prepared for kidney replacement therapy (dialysis or transplant),
which will be required when kidney function is no longer sufficient to sustain life.
Australia, there were 4,740 new cases of ESKD reported in 2007, equivalent to 21 per
100,000 population. The incidence was higher in males than females (26 vs 17 per 100,000) and the incidence in indigenous Australians was six times the rate compared to the nonindigenous population. Not all patients with ESKD receive dialysis, with treatment
decreasing with age, as demonstrated by Figure 1.
Figure 1 Number of new cases of ESKD, by treatment status and age at ESKD onset,
In Australia at the end of 2009 there were 10,300 patients receiving dialysis, and of these,
11 per cent were on the kidney transplant waiting list, with 20 per cent of these patients having already received a transplant. At the same time point, 7,900 patients had a
functioning kidney transplant. 13 The number of end stage kidney disease (ESKD) patients is
a GFR less than 15 mL/min/1.73 m 2
New and emerging organ perfusion systems: July 2014 7
increasing in Australia and New Zealand each year mainly due to the increase in cases of
diabetic nephropathy (Figure 2).
In 2009, approximately 2,300 individuals began dialysis
or transplant treatment, an increase of 19 per cent since the year 2000. In Australia, the rate of new cases of treated ESKD is expected to increase over time, from 11 to 19 per 100,000 between 2009 and 2010. The largest transplant waiting list is for kidney transplantation,
with an average waiting time of approximately four years. 13
Figure 2 The number of new patients commencing renal replacement therapy (dialysis or transplantation) in
Heart failure
Heart failure is a progressive condition where the heart is unable to maintain a strong enough blood flow to meet the body’s needs. Although heart failure can occur suddenly, it usually develops slowly over many years, with the heart becoming weaker and working less efficiently over time. Most patients will progress to end-stage heart failure despite optimal medical care. Treatment options for patients with end-stage heart failure include
implantation with a left ventricular assist device or heart transplantation.
prevalence of heart failure is difficult to estimate, however in 2007–08 the National Health
Survey estimated that 1.3 per cent, or 277,800 Australians had heart failure or oedema, with
the prevalence increasing with age.
It should be noted that one patient may have multiple hospital separations and that only a small proportion of these patients would be eligible or require heart transplantation.
Few heart transplants are performed in Australia due to a shortage of organs. Of the 76 transplants performed in 2007–08, a high proportion were performed in young patients less
than 35 years (>25%) and the majority of patients were male (71%).
2012, the majority of patients had a pre-transplant diagnosis of idiopathic dilated cardiomyopathy (40%) or ischaemic heart disease (35%). Of the 84 patients on the heart
New and emerging organ perfusion systems: July 2014 8
transplant waiting list in 2012, 49 and 13 per cent were classified as NYHA b
III and IV, respectively, whilst 35 per cent were supported by a left ventricular assist device. The mean waiting time (± SD) until heart transplantation in 2012 was 202 ± 213 days (median 139 days, range 2-1,181 days). The mean age (± SD) of all heart transplant recipients in 2012 was
42 ± 16 years (median 47 years, range 1-67 years). Heart transplant recipients in Australia and New Zealand survive on average 14 years after transplantation, with one-third of patients surviving >20 years. Over the 1984-2012 period, the most common cause of death in heart transplant recipients was transplant coronary artery disease (18.4%), followed by
malignancy (15.2%), infection (14%) and acute rejection (10.2%).
Lung
The majority of heart-lung transplant recipients were performed in patients with a pretransplant diagnosis of primary pulmonary hypertension (26%), Eisenmenger's syndrome c
(20.6%), cystic fibrosis (14.4%) and congenital heart disease (13.9%). The most common pretransplant diagnoses in those patients who received a single lung transplant were emphysema (51%) and idiopathic pulmonary fibrosis (25%). In patients who received a bilateral lung transplant, the most common pre-transplant diagnoses were cystic fibrosis
(34.3%) and emphysema (25.9%).
Cystic fibrosis is an inherited, progressive multi-system
condition that begins in early childhood. The defective gene results in a dysfunctional protein that normally controls the flow of cellular water and salts. The epithelium lining the lung is affected and a thick mucus accumulates in the lung as a result, impairing respiratory function. Although life expectancy is reduced in CF patients, new treatments have resulted in an increased life expectancy of up to 40 to 50 years. When patients experience a significant decline in lung function and therapy has been optimised, patients may be referred for lung transplantation. Reliable, recent data on the incidence of CF are difficult to identify. In Australia, CF was newly diagnosed at a rate of one in every 4,700 births in 2005, compared to one in every 3,800 births in 2003. At the end of 2005, there were an estimated
2,472 Australians individuals with cystic fibrosis. Emphysema is the underlying condition of chronic obstructive pulmonary disease (COPD), which is defined as the progressive
destruction of lung tissue and the narrowing of air passages.
In 2011-12 it was estimated that COPD affected 2.4 per cent of the Australian population.
was the fifth leading cause of death with 5,878 people dying from COPD, representing four per cent of all deaths. It is likely that this figure may be even higher as determining the
cause of death in the elderly may be difficult, especially in relation to COPD.
b NYHA = New York Heart Association classification. NYHA III: Marked limitation in activity due to symptoms, even during less-than-ordinary activity, e.g. walking short distances (20–100 m). Comfortable only at rest. NYHA IV: Severe limitations. Experiences symptoms even while at rest. Mostly bedbound patients. c Eisenmenger's syndrome is caused by a congenital heart defect in the fetal heart causes increased flow through the pulmonary vasculature, causing pulmonary hypertension.
New and emerging organ perfusion systems: July 2014 9
All heart-lung transplants have been performed in Australian hospitals, however single and bilateral lung transplants are performed in both Australia and New Zealand. The rate of bilateral transplant has increased steadily over time, with 55 performed in 2001 compared to 153 performed in 2012. This increase corresponds with a decrease in the rate of single lung transplantation, with 29 performed in 2001 and only four performed in 2012. Only four heart-lung transplants were performed In 2012. The mean waiting time (± SD) until lung transplantation in 2012 was 186 ± 216 days (median 120 days, range 0-1,195 days). The mean age (± SD) of heart-lung, single lung and bilateral lung recipients was 25 ± 9, 57 ± 9 and 47 ± 15 years, respectively. Five-year survival rates for heart-lung, single lung and bilateral lung transplants are 51.4, 48 and 61.5 per cent, respectively. Five-year survival of transplants appears to be better in DCD organs (70.9%) compared to non-DCD organs
(63.5%), although numbers are fewer in the former group. The most common cause of death in all lung transplant recipients in the period 1986-2012 was bronchiolitis obliterans
(33.9%) followed by infection (21.7%).
Liver
As with many conditions, true prevalence data is difficult to identify. In 2012 it has been estimated that 6.2 million Australians are affected by liver disease, the most prevalent of which is non-alcoholic fatty liver disease (NAFLD) affecting 5.5 million, followed by persons infected with hepatitis C and B (Hep C 307,040 and Hep B 211,089, respectively). These numbers have been projected to rise by roughly 30 per cent by 2030. Although NAFLD is responsible for a high number of deaths (2,264), the biggest cause of mortality in liver disease patients is in those infected with Hep C (2,550). Liver transplantation is needed in a minority of Hep C cases and is considered fairly rare. Patients with primary biliary cirrhosis or primary sclerosing cholangitis, conditions that only affected 433 and 872 people in 2012, may cause liver failure and therefore require a liver transplant. Neonatal hepatitis and biliary atresia affects approximately 15-20 paediatric patients each year, with biliary atresia, an aggressive liver disease, being responsible for 60 per cent of all paediatric liver transplants. In 2012, there were a total of 261,288 cases of liver disease in Australians aged
Pancreas/intestine
To date, machine perfusion has not been utilised in intestinal or pancreatic
Number of patients
In Australia the overall rate of deceased organ donation rose slightly from 15.1 in 2011 to
15.6 per million population (dpmp) in 2012. The rate of donation in New Zealand remained steady at 8.6 dpmp. These figures translate to 354 and 38 donors in Australia and New
Zealand, respectively, however only 342 and 34 donors were considered to have suitable
New and emerging organ perfusion systems: July 2014 10
organs for donation and had at least one of their organs successfully transplanted. Rates of organ donation vary considerably between the States and Territories, ranging from 12 dpmp in New South Wales to 34 dpmp in the Northern Territory. Over the past 15 years, organ donation rates have increased mainly due to the increase in donations after circulatory
Figure 3
Deceased organ donations by type in Australia, 1998-2012 24
An average of 3.1 and 2.9 organs per donor were transplanted, and 3.1 and 3.0 recipients were transplanted per donor in Australia and New Zealand, respectively. The number and
type of recipient are summarised in Table 3.
Table 3
Type of organ transplant recipient from deceased donors, 2012 24
Australia: Number (pmp) New Zealand: Number (pmp) Transplant recipients
Total deceased donors
Kidney
Liver
Heart
Heart-lung
Lung
Pancreas
Pancreas islets
Intestine
Total number of organs transplanted
Total number of transplant recipients
354 (15.6)
607 (26.8)
230 (10.1)
72 (3.2)
4 (0.2)
144 (6.3)
38 (1.7)
4 (0.2)
1 (0.04)
1,110 (48.9)
1,053 (46.4)
38 (8.6)
54 (12.3)
32 (7.27)
12 (2.7)
13 (2.95)
2 (0.45)
113 (25.7)
110 (25.0)
New and emerging organ perfusion systems: July 2014 11
An intended donor is a person from whom authority has been given or volunteered, but organ donation did not proceed, due to a number of reasons including a positive virology test, cardiac arrest or cancer or infection. Intended DCD donors may not proceed to donation due to the time to cardiac standstill being exceeded. In Australia during 2012, 75 donors did not proceed down the donation pathway, 20 of who were DBD (27%) and 55
(73%) were DCD. In 2012 there were no DCD donors in New Zealand. 24
The Australia and New Zealand Organ Donation Registry does not directly collect information in respect to organ waiting lists but does collate information from a number of registries. Therefore the provided waiting list data is incomplete. This data is also not an accurate indication of the actual demand for organs as many patients are not placed on the waiting list. The number of patients listed as waiting for organ transplantation are
summarised in Table 4. The number of patients listed as waiting for transplantation of liver
or lung has remained steady since 2008. During this time there has been a slight increase in the number of patients listed as waiting for a heart transplant, with 61 patients listed in
2008, rising to 78 in 2012. The waiting list for kidney transplantation has decreased slightly from 1,386 in 2007 to 1,299 in 2010. This corresponds to an increase in the number of kidney transplantations performed, up from 349 in 2007 to 617 in 2012. This increase is due in part to an increase in the number of DCD donors (27 in 2007 vs 129 in 2012) but also to
an increase in the number of live donors.
Table 4
Australian and New Zealand transplant waiting list, 2012* 24
Kidney Liver Heart Lung
Active at start of year
New listings
Removed from list
Transplanted – deceased donor
Transplanted – live donor
Transplant overseas
Died on list
Active at end of year
1,299
651
160
533
59
1
7
1,190
192
347
60
268
29
182
78
108
15
85
8
78
Transplanted – live donor not on list 237
Total live donor 296
* Note: All waiting list data refers to 2012 with the exception of the kidney waiting list which is data collected from 2010
112
186
16
161
14
107
Pancreas
2
48
43
60
16
37
Graft survival can be defined as the ability of the transplanted organ to sustain life without other organ replacement therapy. A loss of graft function may result in death or retransplantation, or in the case of kidneys and the pancreas, resumption of dialysis and insulin therapy, respectively.
New and emerging organ perfusion systems: July 2014 12
Table 5
Proportion of grafts surviving 24
Organ
Kidney – deceased donor Australia
Kidney – deceased donor New Zealand
Liver
Heart
Heart-lung
Lung
Pancreas
1-year
0.93
0.93
0.90
0.87
0.71
0.92
0.89
5-year
0.81
0.79
0.81
0.82
0.64
0.64
0.85
Speciality
Technology setting
Transplantation
Specialist hospital
Impact
Alternative and/or complementary technology
Additive and substitution: Technology can be used as a substitute in some cases, but may be used in combination with current technologies in other instances.
Current technology
The current gold standard method used to maintain and preserve the viability of highquality solid organs between the time of retrieval and time of transplantation is static cold storage (SCS). During preservation with SCS, the donated organ is flushed with a cold preservation solution via the arterial supply and suspended in a bath of the storage media on ice. A number of SCS solutions exist on the market, some of which are organ specific, such as Perfadex a low potassium dextran solution used for lungs, however the most commonly used solution is the University of Wisconsin (UW) solution, a lactobionate-based static storage solution. The role of the organ storage solution is to prevent injury to the stored organ induced by cold temperature and hypoxia, and reduce damage that may occur
from mechanical injury during the preservation process.
Diffusion of technology in Australia
The Vivoline® LS1 lung perfusion system is currently in use in at least one Australian centre, the Prince Charles Hospital in Brisbane. A brief summary of their experience with this
technology can be found in Appendix 1. St Vincent’s Hospital in Sydney is currently
participating in the INSPIRE trial using the OCS™ LUNG normothermic perfusion system. The
LifePort Kidney Transporter system is currently in use at Princess Alexandra Hospital in
Brisbane. The Royal Perth Hospital in Western Australia is currently using the Transmedics™
OCS™ HEART for cardiac transplantation.
New and emerging organ perfusion systems: July 2014 13
Ethical, cultural or religious considerations
There is an imperative to increase the number of potential organs available for donation to patients on the transplantation waiting list. However, a number of ethical issues are raised when discussing organ donation, especially donations after cardiac death, with concerns regarding the withdrawal of therapy and the determination of death. In Australia, there are differences in State and Territory legislation and the interpretation of these statutes results in a variation in the way that DCD is practised within Australia. First and foremost, the patient’s wishes need to be taken into account, followed by consent and authorisation of the patient or family members for donation to take place. A number of interventions are required ante-mortem that are performed for the benefit of potential recipients rather than the donor patient. These interventions are considered ethical if they will contribute to the likely success of the transplantation and do not cause pain or discomfort to the donor. The ethical justification for these interventions relies on a broad interpretation of the patient’s
(both donor and recipient) interests.
New and emerging organ perfusion systems: July 2014 14
Evidence and Policy
Kidney
By far the most mature evidence base for machine perfusion of organs relates to the use of
MP for the preservation of kidneys for transplantation. During MP the kidney is attached to the perfusion system via the renal artery. Further surgical preparation of the kidney is then required to make the seal to the perfusion device airtight. Although it would appear to be accepted practice that organs obtained from expanded criteria donors would benefit from
MP, the evidence base is unclear. In addition, its use and results in DCD donors is variable.
Several recent systematic reviews comparing the use of MP to SCS for the preservation of kidneys were identified. It is difficult to make conclusions in respect to these systematic reviews as many of the studies included were conducted more than 20-years ago, used a variety of devices and included a relatively small number of patients. The methodological quality of these studies was poor or uncertain. In addition, comparisons are difficult due to confounding from advances in surgical technique, and differences in perfusate and
immunosuppression regimens, and perfusion pressures used.
Two systematic reviews included studies that used kidneys donated from both DCD and DBD
donors, one of which included only RCTs (n=7)
and the other included both RCTs (n=7) and
non-RCTs (n=11) but stratified results.
When only the RCTs were considered, O'Callaghan
et al found that the relative risk (RR) of delayed graft function was lower with MP than with
SCS (RR= 0·81, 95% CI [0·71, 0·92], p =0·002), with no significant heterogeneity. When results were stratified according to donor type, there was no significant difference between MP and SCS in the rate of delayed graft function for DBD kidneys (RR=0.84, 95% CI [0.69, 1.03], p =0.09) or for DCD kidneys (RR= 0.80, 95% CI [0.62, 1.04], p=0.094). Graft survival results varied greatly between the included studies, with one study (LifePort Kidney Transporter
device, study summarised below)
finding that graft survival improved with MP compared
to SCS (hazard ratio (HR)=0.52, p =0.03) with the effect appearing to persist for 3-years.
Three trials found no difference in 1-year graft survival (Watson et al, summarised below), however two studies appeared to favour MP over SCS but were underpowered to show an effect. One of these two studies was conducted in 1985 and the other in 2001 with a
Gambro MP system that does not appear to be in current manufacture. There was no overall difference between MP and SCS for the rate of primary non-function (RR = 1.15, 95%
CI [0.46, 2·90], p =0.767), however there was moderate heterogeneity across the trials. One year patient survival was reported by three of the RCTs. Two studies reported patient survival at 17 and 22 months. No relationship between patient survival and preservation
Although the systematic review by Lam et al also included seven RCTs, two studies differed from those assessed by O'Callaghan. The majority of the included RCTs were conducted with the Waters MOX-100 (n=5), mostly in the 1980s, using DBD kidneys. The remaining two
New and emerging organ perfusion systems: July 2014 15
studies by Moers et al (2009) (mixed DBD and DCD) and Watson et al (2010) (only DCD) were conducted with the LifePort Kidney Transporter system and are summarised separately below. MP significantly reduced the rate of delayed graft function (RR= 0.83, 95%
CI [0.72, 0.96], p =0.01 with no heterogeneity) compared to SCS, but no difference in rates of primary non-function (3 trials only: RR=0.76, 95% CI [0.45, 1.28], p =0.3 with some but not significant heterogeneity), 1-year graft loss (RR= 0.87, p=0.39 with moderate heterogeneity) or patient death at one year (RR=0.64, p=0.64). Interestingly a sub-group analysis found no difference in the relative risk of developing delayed graft function between those studies published prior to the year 2000 and those published after (RR= 0.82). Although there was a difference in the relative risk of delayed graft function between donor type, this did not
reach significance (DBD RR = 0.80 vs DCD RR = 0.91).
The remaining two systematic reviews included studies that compared the use of MP and
SCS in kidneys obtained only from DCD donors . The meta-analysis by Deng et al (2013) only included RCTs (n=4), however the review by Bathini et al (2013) included both RCTs (n=4)
and non-randomised controlled trials (n=4) and reported stratified results.
The review by Deng included the two recent LifePort Kidney Transporter studies that are
in addition to a 2001 study using the Gambro device
and a very small (n=13 in each arm) 1994 study using a Nikkiso
, which again appears to have ceased
manufacture. The pooled estimate of odds ratio (OR) showed that MP significantly reduced the odds of delayed graft function in DCD kidneys (OR= 0.56, 95% CI [0.36, 0.86], p =0.008) when compared to SCS. There was no significant difference between MP and SCS for the outcome of primary non-function (OR = 1.30, p =0.60), and although 1-year graft or patient survival tended towards favouring MP, neither reached significance (OR = 0.64, p =0.29 and
OR= 0.37, p =0.19, respectively), which may be due to the small number of these events occurring. One of the limitations of this systematic review is that of clinical heterogeneity, with studies pooled for analysis that used organs donated from both controlled and
Bathini et al (2013) included the same RCTs as those assessed by Deng et al and reported the same results. When the results of all RCTs and the non-randomised controlled trials were pooled for analysis MP significantly decreased the risk of delayed graft function when compared to SCS in organs from DCD donors (RR=0.64, 95% CI [0.43, 0.95], p =0.03), however there was significant heterogeneity across the studies (I
2
= 63%, p =0.06). Similar to the results in just the RCTs, there was a trend towards improved graft survival at 1-year but
this did not reach significance (RR= 0.74, 95%CI [0.48, 1.13], p=0.17).
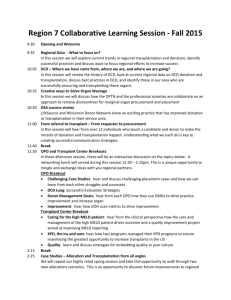
LifePort Kidney Transporter
The LifePort Kidney Transporter is a fully self-contained, portable machine perfusion unit that is designed to contain and perfuse a transplantable kidney under cold and aseptic
conditions (Figure 4). The unit is relatively compact (dimensions 61x36x36cm), however it
New and emerging organ perfusion systems: July 2014 16
weighs 20.4 kg when fully loaded and may require two people to transport it. The unit has the capacity to perfuse one kidney, which is placed in the disposable perfusion circuit cassette and loaded into the LifePort Kidney Transporter. Although the unit can run off
mains power, it also has a 24 hour battery capacity.
The LifePort Kidney Transporter pump
is currently in use at Princess Alexandra Hospital in Brisbane.
Disposable perfusion circuit cassette with cannulas
Figure 4
Cost of the LifePort Kidney Transporter
The LifePort Kidney Transporter, printed with permission 34
The current Australian listing for equipment costs are $16,000 for the pump and $2,600 for the single use, sterile perfusion circuit cassettes. Initial training is included in the purchase price and ongoing annual refresher training is also provided. Initial training includes a wet lab with discard kidneys, dissection and cannulation, which is followed by LifePort Kidney
Transporter training including setup, operation, monitoring and troubleshooting (personal communication Organ Recovery Systems).
Safety and effectiveness of the LifePort Kidney Transporter
The largest study reported to date is a European multi-centre randomised controlled trial
(RCT) where each pair of kidneys from one donor were divided by the type of preservation, with one kidney preserved using SCS whilst the other was preserved using the LifePort
This study along with several others was included in the 2009
Updated HealthPACT Brief describing the use of the LifePort Kidney Transporter, which can be accessed via this link . This RCT found that at one year post-transplantation, patient
New and emerging organ perfusion systems: July 2014 17
survival was 97 per cent in both groups (level II intervention evidence). One-year graft survival was significantly higher in the LifePort group compared to the cold storage group
(94% vs 90%, p =0.04). Logistic regression analysis showed that machine perfusion significantly reduced the odds of delayed graft function (OR= 0.57, 95% CI [0.36, 0.88], p =0.01). In addition, one-year graft survival was significantly higher in the machine perfusion group with a significant reduction of graft failure (HR= 0.52, 95% CI [0.29, 0.93], p =0.03).
Data from the original 672 recipients who received a DCD or DBD kidney were recently
analysed to determine 3-year graft survival.
Overall, the 3-year graft survival was better
for the MP kidneys compared to controls. When organs were stratified according to donor,
MP was superior to SCS when organs came from the DBD and extended criteria donors, however organs from the DCD donors had slightly poorer survival rates for MP when
Table 6
3-year graft survival with LifePort Kidney Transporter perfused kidneys 35
Machine perfusion
Cold storage
Hazard ratio for graft failure
[95% CI] p value
Overall transplanted kidneys(n=672) 91% 87%
0.60
[0.37, 0.97]
0.04
Kidneys from DBD donors (n=588)
Kidneys from DCD donors (n=164)
91%
90%
86%
92%
0.54
[0.32, 0.90]
1.16
[0.41, 3.28]
0.02
0.78
Kidneys from expanded criteria DBD donors*
(n=188)
86% 76%
0.38
[0.18, 0.80]
0.01
* Extended criteria donors are donors aged >60 years, or those aged between 50 and 60 years with either a history of hypertension, death due to cerebrovascular causes, serum creatinine >132 μ mol/L before removal of kidney
A further analysis of the data from extended criteria DBD donors reported that at 1-year,
MP reduced the risk of delayed graft function (OR 0.46, p =0.047) and significantly lowered the incidence of primary non-function ( p =0.04). In recipients who did experience delayed graft function, 3-year graft survival was significantly higher in those recipients who received a MP kidney compared to controls (68.7% vs 32.9%, p
Several papers have reported similar results when reporting on the use of kidneys donated from DCD donors only. An earlier RCT reported on the results of 82 kidney pairs obtained from consecutive, controlled DCD donors (level II intervention evidence). The incidence of delayed graft function was reduced in the LifePort MP recipients compared to controls (OR
0.43 95% CI [0.20, 0.89], p =0.025), although 1-year patient and graft survival rates were similar in both groups (93.9% vs 95.1%). The median duration of delayed graft function was
New and emerging organ perfusion systems: July 2014 18
shorter by four days in the MP group; however this did not reach significance. In addition, creatinine clearance was higher in MP kidneys up to one month post-transplantation
compared to control kidneys (p= 0.027).
Similarly, a UK study randomly assigned 45 pairs of kidneys from DCD donors to undergo preservation either by LifePort MP or SCS (level II intervention evidence). There was no difference in the baseline characteristics of the recipients in both groups. In addition, there was no significant difference in the mean cold ischaemic time between the MP intervention group and controls (13.9 vs 14.3 hours, p =0.77). Importantly there was no reported difference between MP and SCS in the rate of delayed graft function (57.8% vs 55.6%, p =0.99), rejection-free survival at 1-year (91% vs 78%, p =0.1), graft survival at 1-year (93.3% vs 98%, p =0.3) and patient survival at 1-year (93% vs 100%, p =0.08). The authors favoured the use of SCS in kidneys from DCD donors, as not only were outcomes similar to those
obtained with MP, SCS was cheaper and less technically challenging.
Sedigh et al (2013) reported on their experience using the LifePort device in 52 recipients compared to matched historical SCS controls (level III-3 intervention evidence). Median cold ischaemia time was similar in both groups at 12.8 hours in the MP group and 11.7 hours in controls. Overall, the rate of delayed graft function was reduced in MP transplanted kidneys
(11.5%) compared to controls (20.7%). When kidneys were stratified according to their quality, the incidence of delayed graft function in kidneys obtained from standard criteria
DCD donors was significantly reduced in the machine perfused group compared to controls
(0% vs 21.4%, p =0.046). There was no difference in rates of acute rejection and 1-year graft
survival between the two groups.
37 An abstract from the 2012 International Congress of the
Transplantation Society reported on the outcomes of kidneys donated from DCD donors treated with the LifePort device. Although those kidneys preserved with MP experienced a significantly longer cold ischaemic time compared to controls (13.6 vs 10.0 hours, p =0.001), there was no difference in the rate of delayed graft function. In the MP group (n=30) there was no correlation between cold ischaemic time and either delayed graft function or onemonth estimated glomerular filtration rate. In the controls (n=27) there was a negative correlation between cold ischaemic time and one-month estimated glomerular filtration rate (-0.765), however this was non-significant ( p
The benefits of MP for the preservation of kidneys from extended criteria donors remains unclear as Sedigh et al reported no difference in the rate of delayed graft function between
MP and controls for kidneys donated from extended criteria donors d
(16.7% vs 20.3%, p =0.658), which contradicts the results reported by the high-quality RCT by Moers et al
(2012) above. A retrospective analysis of 88 patients who received kidneys from extended criteria donors was reported at the 2012 International Congress of the Transplantation d Expanded criteria donors are donors aged >60 years, or those aged >50 years with either a history of hypertension, death due to cerebrovascular causes, serum creatinine >150 μmol/L before removal of the kidney
New and emerging organ perfusion systems: July 2014 19
Society and compared to matched historical controls (level III-3 intervention evidence).
Mean cold ischaemic time was similar in both groups (15 hours for LifePort MP and 16 hours for SCS kidneys). The rate of delayed graft function was reduced in the MP recipients compared to controls (17% vs 24%, significance not stated), however the 1-year graft
survival rate was similar in both groups (97.7% vs 96.6%).
Of interest is the Eurotransplant Senior Programme RCT, which utilised extended criteria
DCD kidneys from donors aged ≥65 years transplanted into recipients aged ≥65 years (level
Out of the 132 potential donors, 85 kidney pairs from donors
with a median age of 70 years (range 65-83 years) were randomised to MP with LifePort or
SCS (control). There were no differences in baseline characteristics between the control and intervention recipients, with a median age of 66 years (range 37-79 and 39-79, respectively) in both groups. The median cold ischaemic time was 11.0 hours in the MP treated kidneys compared to 10.5 hours for controls. Although more patients in the MP group were undergoing a re-transplantation procedure (20/85 = 23.5%) compared to controls (12/85 =
14.1%), this was not significant ( p =0.3).
The primary and secondary outcomes of this RCT are summarised in Table 7. There was no
difference in the development of delayed graft function between the two groups, which may be due to the relatively short cold ischaemic times. Primary non-function was significantly reduced in MP kidneys (3.5%) compared to controls (12.9%). A logistic regression analysis found that only length of cold ischaemic time (OR 1.2, p <0.0001) and retransplantation (OR 3.99, p =0.007) were significantly associated with the development of delayed graft function. The overall 1-year patient and graft survival rates were similar in both groups (94% vs 95% and 89% vs 81%, p >0.05, respectively). However, in patients with delayed graft function, 1-year graft survival was significantly better in recipients of MP kidneys compared to that in controls (84% vs 48%, p =0.01).
Table 7
Primary and secondary outcome results from the Eurotransplant Senior Programme 40
Machine perfusion Cold storage p value
DGF (%) 29.4 34.1 0.58
Duration of DGF (days, range)
Functional DGF (%)
Primary non-function (%)
Calcineurin inhibitor toxicity (%)
Acute rejection (%)
12.5 (3-31)
18.8
3.5
8.2
22.5
13.0 (3-92)
23.5
12.9
7.06
16.5
0.33
0.84
0.02
0.61
0.25
Another area of interest is the use of perfusion parameters during MP, such as flow, resistance and pressure, as predictive or prognostic indicators of long-term kidney transplant function and success, allowing for early therapeutic intervention. Patel et al
New and emerging organ perfusion systems: July 2014 20
(2012) discussed the advantages of waiting until these perfusion parameters improved prior to transplantation, which may result in long cold ischaemic times and a possible decrease in graft function (level IV intervention evidence). Although 190 kidneys underwent MP, outcome data in this retrospective case series were only available on 165. The status of donors was not clearly stated (DBD vs DCD vs extended criteria). For all kidneys at 2-hours, the average flow increased markedly from baseline whereas the average resistance decreased. Flow and resistance were measured again at 4- and 6-hours but did not differ from rates measured at 2-hours. However these average figures were a result of 82 kidneys improving in function and 83 that remained static or declined in function with continued perfusion. Although the discard rate was higher in the static group, for those kidneys that were transplanted, the rate of delayed graft function was higher in the improved flow group
(Table 8). A logistic regression analysis found that resistance at 2, 4 and 6-hours was
predictive of delayed graft function, as was donor anoxia and cerebrovascular accident.
Flow parameters and cold ischaemic time were not predictive of delayed graft function.
Table 8
Outcomes after continuous MP based on an improvement in flow from baseline 41
Improved flow Static or decline in flow p value
Discard kidneys
Delayed graft function
1-year graft loss
17/82 (20%)
27/42 (64%)
4/42 (9.5%)
29/83 (34%)
13/33 (39%)
3/33 (9.1%)
0.04
0.03
0.94
Economic evaluation of the LifePort Kidney Transporter
The UK’s National Institute for Health and Clinical Excellence completed a cost-effectiveness analysis as part of its 2009 technology appraisal guidance on the use of MP for kidneys from
deceased donors. 42 This analysis is likely to be applicable to Australia and New Zealand due
to the similarities of the respective health systems. The first part of this assessment reported on the cost-effectiveness analysis by Bond et al (2009), which was included in the original 2009 HealthPACT assessment. Markov modelling was used to simulate posttransplantation outcomes using data obtained from two RCTs that compared cold storage to preservation with the LifePort device. The donor populations used in the two, at the time ongoing studies, differed e
and therefore both populations were modelled separately. Cost data for MP were annualised and the lifespan of the LifePort device was assumed to be 10years. Costs when using data from the European MP trial were based on preserving 61 kidneys per year obtained from DCD donors. This resulted in a cost per kidney stored of
£544. MP with the LifePort was found to be cheaper (£139,100 vs £142,805) and generated slightly more QALYs f
(9.79 vs 9.58) when compared to SCS. Probabilistic sensitivity analyses e The European MP trial used mainly DBD with some DCD donors and the UK pulsatile perfusion trial used all f
DCD donors.
QALYs = quality-adjusted life-years
New and emerging organ perfusion systems: July 2014 21
predicted that over a range of willingness-to-pay levels (£0–£100,000) the probability of
LifePort being cost effective was 80 per cent. However, when the model was populated with data from the UK trial, the number of kidneys stored per year was only 16, all from DCD donors, which resulted in a cost per kidney stored of £737. MP with the LifePort was found to be slightly more expensive (£141,319 vs £139,205) and generated slightly less QALYs
(9.13 vs 9.19) when compared to SCS. Probabilistic sensitivity analyses predicted that over a range of willingness-to-pay levels (£0–£100,000) the probability of LifePort being cost effective was about 40 per cent. This difference may be accounted for in the difference in
It should be noted that the UK study used in this analysis
has since been completed and is summarised above. The study by Watson et al (2010) found no difference in 1-year post-transplant outcomes in patients who received a kidney
Two other economic evaluations of the LifePort Kidney Transporter were identified for inclusion in this assessment; however the results of these may not be generalisable to the
Australian Health System as they were conducted in the United States.
Gomez et al (2012) developed a probabilistic decision tree model using patient outcome data obtained from the European MPT trial for the MP arm and historic data for the SCS arm. However, it should be noted that only kidneys donated from extended criteria DBD donors with a mean age of 72.9 ± 7.3 years. The analysis was conducted from the perspective of a tertiary hospital, using 2010 US dollar prices. It was assumed that each transplant centre would require two LifePort devices to preserve a pair of kidneys, at an initial purchase price of US$6,060 each, and a life-span of 10-years. The total costs per kidney transplant, including training and consumables, were calculated to be US$1,395 for
MP and $185 for SCS. The analysis considered three patient outcomes post-kidney
transplant: immediate graft function, delayed graft function and primary non-function.
Resources consumed for each outcome are summarised in
Table 9. A major part of the costs for each outcome was hospital stay (41.5-53.9%), followed
by graft explantation (20.2%) and the need for dialysis in recipients who experience primary non-function (16.0%). The budget impact per patient for the introduction of MP was $505.
However, when the incremental cost-effectiveness ratio (ICER) was calculated taking into account the number of cases of delayed graft function and primary non-function avoided by the use of the LifePort, machine perfusion was found to have a negative ICER of $3,369.
That is, machine perfusion is cost-effective in terms of savings for delayed graft function and primary non-function when kidneys obtained from extended criteria donors are
New and emerging organ perfusion systems: July 2014 22
Table 9
Results
Differences between average expected costs for MP and SCS (US$) 45
Costs Probability Costs x probability
MP with LifePort Kidney
Transporter
IGF
DGF
SCS
PNF
Expected costs
$9,522
$12,228
$27,297
0.71
0.26
0.03
IGF $8,159
$10,865
0.56
0.38
$25,933
Difference in costs: MP-SCS
IGF = immediate graft function, DGF = delayed graft function, PNF = primary non-function
0.06
$6,761
$3,179
$819
$10,759
$4,569
$4,128
$1,556
$10,254
$505
The earlier cost-effectiveness analysis conducted by Garfield et al (2009) supported these findings for both standard and extended criteria donors, which is not surprising as the model was constructed using estimates from the European MP trial. The perspective for this model, however, was from that of the US health care system, comparing reimbursement
(payment) on behalf of health care payers and the associated patient outcomes (utility) dependent of whether the donated kidney was preserved with MP with the LifePort or SCS.
The different perspective may explain the difference in ICERs.
As with the study by Gomez et al, the patient outcomes considered were immediate graft function, delayed graft function and primary non-function, with the first two outcomes modelled out to 1-year post-transplant. At 1-year post-transplant, MP was more costeffective than SCS when used for kidneys obtained from either standard (US$92,561 vs
US$104,118) or extended criteria donors (US$106,012 vs US$114,530). It should be noted that these results indicate that the least cost-effective option was using SCS for extended criteria donors (US$114,530), with MP of standard criteria donors being the most cost-
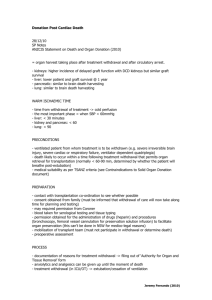
RM3® and Waves
Waters Medical Systems have two hypothermic kidney MP devices on the market: the RM3® and the Waves. The RM3® is a non-portable system, with a wet weight of 30.7 kg, which is
capable of preserving two kidneys simultaneously (Figure 5). The RM3® uses the Waters
MOX pulsatile pump as described in the early studies included in the above systematic reviews. The RM3 has been described as a flow-driven device as opposed to the LifePort
New and emerging organ perfusion systems: July 2014 23
which is a pressure-driven device.
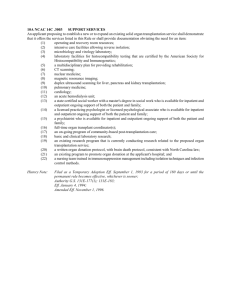
The Waves device is a portable single kidney MP device
with a 24-hour battery life and is comprised of three parts: a control unit, a disposable
cassette and perfusion circuit, and remote monitoring software (Figure 6). The entire system
is relatively compact with dimensions of 648mm x 413mm x 337mm, with a fully loaded weight of 26 kgs. Neither device is currently in use in Australia or New Zealand (personal communication Waters Medical Systems).
Figure 5 The RM3 ®
device perfusing 2 kidneys simultaneously 48
Biopsy/sample tubes Disposable cassette
Control unit
Figure 6 The Waves portable MP device. When lids are closed the device is in transport mode, when open the device is in perfusion mode (personal communication Waters Medical Systems).
Cost of the WAVES and RM3® devices
The current purchase price of the RM3® is US$37,669. The cost of a single kidney disposable sterile cassette for the RM3 is US$848, with a dual kidney cassette costing US$990. Either cassette requires one litre of Waters perfusate solution at a cost of US$197/litre. In addition, the costs of sterile cannulas range from US$45 to $85 each.
The basic list price for the Waves device is US$25,625. To perfuse one kidney, the cost of the disposable cassette and perfusate is US$1,538 and US$197/litre, respectively. Training is
New and emerging organ perfusion systems: July 2014 24
included in the list price of the device, however depending on location consumers may be required to share the cost of the trainer’s travel (personal communication Waters Medical
Systems).
Safety and effectiveness of the Waves and RM3® devices
No clinical studies describing the use of the Waves device could be identified. Several studies, circa 1980s, describing the use of the RM3® (Waters MOX pump) were included in the systematic reviews summarised above.
A large retrospective case series (n=339) describing the pooled results of three studies using
kidneys transplanted after MP using the RM3® system (level IV intervention evidence).
The initial aim of these three studies was to assess the effectiveness of various immunosuppression regimens. All transplanted kidneys were placed in static cold storage at time of retrieval for transportation, and then placed on MP using the RM3 until time of transplantation. The majority of kidneys came from DBD donors with 3.5 per cent from DCD donors and 10.9 per cent from ECD donors (criteria not defined in paper). The mean SCS time was 6.6 ± 4.5 hours, with a mean MP time of 26.7 ± 8.4 hours and a mean cold ischaemia time of 33.2 ± 8.4 hours.
Five patients developed graft failure during the first two weeks post-transplantation due to primary non-function (n=3), renal vein thrombosis (n=1) and ruptured kidney (nonimmunological) (n=1). A total of 15 patients (4.4%) developed delayed graft function and 41 patients had slow graft function. Receiving a DCD kidney was the only factor associated with the development of delayed graft function with an odds ratio of 8.8 (95% CI [2.1, 36.5], p <
0.001). There was a trend towards a reduced rate of delayed graft function in those patients who received a kidney that had been treated with <24 hours MP compared to those with kidneys treated with 24-29 hours of MP (5.2% vs 7.3%, not significant). Pre-transplant diabetes and having a non-Caucasian racial origin were two factors associated with the development of slow graft function. Rates of biopsy proven acute rejection were 5.6, 9.1 and 18.3 per cent at six and 12 months, and at any time post-transplant, respectively. A univariate analysis found that biopsy proven acute rejection was associated with the development of delayed graft function (p=0.002) and with recipient age being less than 50
At median follow-up of 47 months (range 24-93 months) 274 patients were still alive with a functioning graft (80.8%), with 65 patients experiencing graft loss. Actuarial graft survival (± standard error) was 94 ± 1, 86 ± 2, 77 ± 3 and 72 ± 3 per cent at one, three, five and seven years, respectively. Death censored graft survival at the same time points was 97 ± 1, 92 ± 2,
86 ± 2 and 83 3 per cent, respectively.
New and emerging organ perfusion systems: July 2014 25
Conclusions as to the effectiveness of machine perfusion using the RM3® cannot be drawn due to the non-comparative nature of this study. In addition it should be noted that partial salary funding for the completion of this study was provided by Waters Medical.
Ciancio et al (2012) retrospectively compared the impact of different perfusion factors
(flow, pressure) on outcomes in patients who were recipients of kidneys from the same DCD donor, perfused using the RM3 device (level III-2 intervention evidence). There were 66 donor-matched pairs of DCD recipients who were followed up for a minimum of 2-years. As a group, there was no difference in the baseline characteristics of the recipients (age, sex, pre-existing diabetes) who received the first kidney of the matching pair when compared to the group who received the second kidney, apart from a higher number of African-
Americans being present in the second group (35% vs 20%). Mean pump and cold ischaemic
times were significantly longer in the group that received the second kidney (Table 10).
However, there was no significant effect of pump or ischaemic time on the development of
delayed graft function, or graft or patient survival.
Table 10
Characteristics of matched donor kidneys 50
p value
Pump time (hrs)
Cold ischaemic time (hrs)
Clinical outcome
Graft failure
Group received 1 st kidney
22.7 ± 7.3
27.6 ± 7.7
8
Group received 2 nd kidney
31.2 ± 7.9
36.0 ± 8.3
7
<0.001
<0.001
0.85
Graft survival
Patient survival
15
8
13
5
0.76
0.39
An abstract presented to the 2011 American Transplant Congress reported the longest follow-up data with the 4-year outcomes of patients from a series of 66 kidneys obtained from expanded criteria DCD donors (ECD) and perfused with either the RM3® or the LifePort device. The outcomes from these patients were compared to 92 age-matched historical controls that underwent transplantation with ECD kidneys preserved by SCS (level III-3 intervention evidence). There was no significant difference in either the donor or recipient characteristics between the MP and SCS groups. However, kidneys that underwent MP experienced a significantly longer cold ischaemic time (31.1 ± 9.8 vs 24.7 ± 7.8 hours, p <0.001). Patient survival at 4-years was better in the MP group (89.7% vs 72%, p =0.02).
Delayed graft function tended to be reduced in the MP group, however this did not reach significance (24.2% vs 29.3%, p=0.59). Similarly, graft survival at 4-years was higher in the
MP recipients compared to the SCS group, but again did not reach significance (70.5% vs
57.7%, p
New and emerging organ perfusion systems: July 2014 26
The one recent, albeit small, RCT compared two MP devices: the RM3® (flow-driven or FD) and the LifePort (pressure-driven or PD) (level III-3 intervention evidence). A total of 50 kidneys were obtained and randomised to either device. Approximately half of the kidneys were obtained from expanded criteria donors (n=24) with the remaining being from DCD donors. There was no difference in the baseline characteristics between the FD and PD recipients, or the mean cold ischaemic time the organs underwent.
Results from this study are summarised in Table 11. Renal flow, renal resistance and
perfusion pressure were all lower in the PD group compared to the FD group. Overall 1-year graft survival was 88 per cent. When stratified by donor, graft survival was higher in kidneys retrieved from standard criteria donors (96%) compared to those from expanded criteria donors (79%, no significance stated). There was no difference in the rate of delayed graft function between kidneys preserved with PD or FD MP. Although there appeared to be a benefit in 1-year graft survival for those patients who received a kidney preserved by PD
MP compared to the FD group this did not reach significance.
Table 11
Outcomes of kidneys preserved with either pressure or flow driven MP 47
LifePort PD group RM3 ® FD group p value
Renal flow
Renal resistance at 18 hrs
Perfusion pressure at 4 hrs
Delayed graft function
130 ml/min
0.17 ml/min
22 mmHg
8/25 (32%)
150 ml/min
0.24 ml/min
31 mmHg
8/25 (32%)
Mean number of haemodialysis sessions required post-transplant in patients with
DGF
2.65 ± 1.5 4.66 ± 0.91
1-year graft survival
DCD + ECD
ECD donors only
24/25 (96%)
11/12 (92%)
20/25 (80%)
8/12 (66%)
NS = not significant, PD = pressure driven, FD = flow driven, ECD = expanded criteria donors, DGF = delayed graft function
NS
0.001
<0.01
NS
0.004
0.07
0.09
Economic evaluation of the WAVES and RM3® devices
No economic analyses on the Waves or RM3® devices could be identified.
Airdrive™ hypothermic kidney perfusion transport system
The Airdrive™ is a disposable sterile, hypothermic organ perfusion kidney transport system, with a transport range of at least 12-hours. The system including perfusion fluids and an oxygen bottle weighs approximately 11 kg, and the control unit records organ pressure, flow
and temperature throughout transport.
The system is based on an oxygen-driven, positive displacement pump that allows pressure controlled pulsatile perfusion and oxygenation of the perfusate. Medical grade oxygen is
provided by a 2-L pressurised cylinder containing that is carried on board (Figure 7). The gas
New and emerging organ perfusion systems: July 2014 27
valves and pressure feedback systems are powered by a 12-volt, non-rechargeable battery.
All components are embedded in polystyrene to provide optimal isolation and four precooled packs (-20°C) are placed underneath the organ chamber inside the transporter box to
The price for the system is approximately €3,600, which includes an oxygen bottle. As this is a disposable kit, this price represents the cost per transplant, with no maintenance required. Training is provided by the company at the cost of €1,200 per day. The company have begun pre-clinical trials in Europe using discarded human livers and pre-clinical trials for kidneys will follow in late 2014 (personal communication Portable Organ Perfusion).
Figure 7
Only the preliminary results from three animal studies that used the Airdrive™ perfusion
system could be identified, and were therefore not included for assessment.
Sherpa Pak™
Although Paragonix announced that they had filed a submission for regulatory approval of
the Sherpa Pak™ for kidney transportation to the FDA in December 2013
only describes the Sherpa Pak™ for cardiac perfusion. No studies could be identified describing the use of the Sherpa Pak™ for the perfusion of kidneys.
Kidney Assist
The Kidney Assist provides hypothermic oxygenated perfusion in a transportable unit that
has a battery life of 24-hours (Figure 8). No studies that assessed the clinical use of the
Kidney Assist could be identified. The only papers that could be identified were those that
described the advantages of oxygenated hypothermic perfusion.
contacted for information in respect to regulatory status, diffusion and cost but no information was supplied.
New and emerging organ perfusion systems: July 2014 28
Figure 8 The Kidney Assist, showing the transportable unit and the organ holder that is submerged in
preservation solution during perfusion 57
Ongoing research
Only one ongoing clinical trial assessing the use of machine perfusion for kidney transplantation was identified.
The ‘Pulsatile Perfusion Preservation in Kidney Transplantation From Expanded Criteria
Donors (IMPULSION)’ open label RCT commenced in 2010, is still recruiting and expects to enrol 300 patients (Lyon, France NCT01170910 ). Eligible patients will be randomised to either SCS (control) or preservation with the Waters Medical® pulsatile perfusion machine
(RM 3). Machine perfused kidneys are placed in the perfusion machine within 2-hours and maintained for at least 6-8 hours before being transplanted. This RCT expects to assess the viability of organs from donors using expanded donor criteria including older donors (>60 years) and donors with pre-existing medical conditions including diabetes, hypertension, serum creatinine levels >1.5 mg/dL and death by stroke (haemorrhagic or thrombotic). The primary outcome measure is the rate of delayed graft function, with secondary measures including graft survival and reversion to dialysis.
New and emerging organ perfusion systems: July 2014 29
Summary
A total of seven machine perfusion systems for kidneys were identified. Of these, only the
LifePort® is listed on the ARTG. Of the remaining six systems, two are approved by the FDA
(Waters’ Waves and RM3), two are seeking FDA approval (Airdrive™ and Sherpa Perfusion), one is CE marked (Kidney Assist) and one is still investigational.
As of the end of 2012, there were 1,190 Australian and New Zealand patients on the kidney transplant waiting list. In that same year, a total of 661 kidneys were transplanted.
The evidence base for machine perfusion of kidneys is the most mature of all organs.
Several systematic reviews were identified, however, there was a great deal of heterogeneity between studies included in these reviews due to the age of the studies, small numbers of patients, variation in perfusion systems and variations in clinical practice. Two reviews assessed outcomes in recipients who received organs from DCD and DBD donors.
When only RCTs were considered, the overall relative risk of delayed graft function (DGF) was significantly reduced with MP compared to SCS (RR= 0.81-0.83), with no difference in outcomes when stratified by DCD or DBD organs. Mixed results were reported for graft survival but there was no difference in the rate of primary non-function (PNF) between MP and SCS treated kidneys. Two systematic reviews assessed outcomes in recipients who received organs from only DCD donors. When only RCTs were considered, MP significantly reduced the odds of DGF (OR= 0.56) compared to SCS, however, as before, there was no difference in the rate of PNF between MP and SCS treated kidneys. One-year graft and patient survival tended towards favouring MP but did not reach significance. These results indicate that the use of DCD donors may result in good outcomes for patients.
Of the seven MP devices identified, only two hypothermic devices (LifePort® and the RM3) had published peer-reviewed clinical studies.
New and emerging organ perfusion systems: July 2014 30
Summary continued
LifePort® device
Level II intervention evidence
Level III-3 intervention evidence
Level IV intervention evidence
4
2
1
The largest RCT to date included DCD and DBD donors (n=672). Overall, the odds of DGF were lower and the 1-year graft survival was higher in recipients who received MP kidneys compared to SCS treated kidneys. Graft survival remained superior at 3-years in the MP group. When stratified to donor type, graft survival was poor in MP kidneys from DCD donors but superior in MP kidneys from DBD or extended criteria donors. These results were supported by another RCT (n=82), however a small (n=45) RCT by Watson et al found no difference in any outcomes between MP and SCS treated kidneys.
Mixed results were reported when only extended criteria kidneys were transplanted. Of the two good quality RCTs, one reported reductions in DGF and PNF with organs obtained from
DBD extended criteria donors. The other study reported on transplants with organs obtained from DCD extended criteria donors and found no difference between MP and SCS in the rate of development of DGF.
Three economic analyses were identified that compared costs and outcomes using the
LifePort®. The most relevant of these to the Australian and New Zealand health systems was conducted by NICE in the United Kingdom. Cost-effectiveness varied depending on the data used to populate the model. Using the data from the largest RCT, MP was cost-effective compared to SCS, however when using data from the small Watson RCT, SCS was more costeffective.
RM3
Level III-2 intervention evidence
Level III-3 intervention evidence
Level IV intervention evidence
1
2
1
The evidence base for the RM3 device was poor. Two studies compared the use of the RM3 to the LifePort® device, in extended criteria and DCD donors. One study found that 4-year patient and graft survival was greater in recipients of MP kidneys compared to matched historical controls, and that DGF tended to be reduced in MP recipients. No conclusions regarding the effectiveness of the RM3® could be drawn from the large case series.
New and emerging organ perfusion systems: July 2014 31
Lung
One of the main problems associated with the transplantation of lungs is not only the shortage of organs, but a low utilisation of those made available due to sub-optimal gas exchange function or damage to the donor lung from intubation/aspiration, poor donor management or the presence of high levels of inflammatory cytokines. Using marginal lungs may be associated with an increased risk of chronic graft dysfunction. When lungs are preserved using hypothermic methods cellular metabolism is slowed, making it difficult to assess function. During ex-vivo lung perfusion (EVLP) the lungs are often preserved cooled, but then warmed up to normothermic temperatures during the reconditioning phase, which
allows the viability of donated lungs to be evaluated prior to transplantation.
addition, lungs may undergo treatment such as the administration of antimicrobial therapy to reduce bacterial load or thrombolytics to prevent pulmonary emboli. It is hoped that gene and mesenchymal stem cell therapy prior to transplantation may improve future
The aim of EVLP is to reproduce the in-vivo environment of the donor lung, using ventilation and perfusion. Three EVLP protocols have been developed: the Toronto technique used by
XVIVO, the Scandinavian protocol used by Vivoline, and the Organ Care System, which is designed for the transport of healthy organs in normothermic conditions. These protocols vary slightly, e.g. the fraction of inspired oxygen used, the type of pump (centrifugal, roller or pulsatile), perfusion start rate, etc. Unlike the other two protocols, the Toronto protocol uses an acellular perfusion solution, a closed circuit with a positive left-atrial pressure, and low pulmonary artery flow (40% of estimated cardiac output), and is designed for perfusion between to 3 to 4 hours. The Toronto and Scandinavian protocols use the Steen™ preservation solution (XVIVO, Vitrolife), a buffered dextran solution with an optimised colloid osmotic pressure developed specifically for EVLP. Both the Organ Care and
Scandinavian protocols use a perfusate with 10-15 per cent red blood cells added.
Although the Scandinavian protocol is cited as being designed for short-term perfusion of up to 2 hours to evaluate pulmonary responses at normal blood flows with an open atrium, local experience states that this protocol is suitable for much longer perfusion times of up to six hours (personal correspondence Prince Charles Hospital, Brisbane). The Organ Care
protocol is designed for the duration of transportation.
XVIVO™ and XPS lung perfusion systems
The XVIVO provides normothermic EVLP to “recondition” marginal lungs from DCD or expanded criteria donors, or other sub-optimal /marginal lungs currently rejected for use, in
a bid to expand the available pool of donor lungs.
XVIVO Perfusion offers two different
EVLP methods: the XVIVO Perfusion System (XPS) and the manual XVIVO system, both of which can utilise either the Lund or Toronto protocols (personal communication XVIVO
New and emerging organ perfusion systems: July 2014 32
Perfusion AB). A short video demonstrating the use of the XVIVO™ system can be viewed via this link .
The XPS™ (Figure 9) is an integrated cardiac bypass system which includes the following
components;
MAQUET CardioHelp centrifugal pump (includes pressure, temperature, level, bubble and flow sensors);
heater/cooler (15-39°C);
Hamilton C2 ICU ventilator;
perfusate Gas Monitor, Terumo CDI-500;
STEEN Solution™ pumps;
organ Chamber platform;
100% medical O
2
gas cylinder or high pressure wall line for ventilator;
deoxygenator;
temperature/pressure and flow/bubble monitoring; and
EVLP cart (personal communication Xvivo Perfusion AB).
Figure 9
Hardware for the manual system is generally off-the-shelf standard cardiac bypass equipment and requires a:
centrifugal pump and flow sensor;
heater-cooler unit;
ventilator;
gas analyser; and
New and emerging organ perfusion systems: July 2014 33
gas cylinder (s) depending on protocol in use (personal communication Xvivo
Perfusion AB).
During XVIVO EVLP, 500 ml of perfusate is removed every hour and replenished with 500 ml of fresh solution. Donor lungs are placed in the XVIVO™ chamber and the left atrial cannula
is connected to the circuit (Figure 10). Flow was initiated slowly in a retrograde fashion to
remove air through the pulmonary artery cannula, which is then connected to the circuit.
Anterograde flow is started at 150 ml/min with the perfusate at room temperature and the temperature is then gradually increased to 37°C. Ventilation of the lungs is commenced when the temperature reaches 32°C. After four hours of EVLP, the lung block is cooled down in the circuit to 10°C and perfusion and ventilation are halted. The trachea is then clamped to maintain the lungs in an inflated state and the lungs are then preserved at 4°C in
Perfadex® until transplantation. Lungs are considered suitable for transplantation if the partial pressure of oxygen to the fraction of inspired oxygen (PO
2
:FiO
2
) is ≥ 350 mmHg. In addition, lungs are deemed suitable if pulmonary vascular resistance, dynamic compliance and peak inspiratory pressure deteriorates less than 15 per cent from baseline levels during
Figure 10
A simplified schematic of the XVIVO system perfusing donated lung. 58
PV= pulmonary vein, PA = pulmonary artery
Cost of the XVIVO system
The current list price in Europe for the XPS is €150,000 and the disposable kit is €15,000. The products that XVIVO Perfusion supplies for the set-up of the manual system per donation are:
STEEN Solution, 1 x 500ml
XVIVO Organ Chamber
XVIVO Lung Cannula Set
AUD $1,032
AUD $563
AUD $241.
New and emerging organ perfusion systems: July 2014 34
It should be noted that priming the circuit may require 2-2.5 litres of Steen solution, and that the circulating solution may be changed during perfusion (personal communication
Xvivo Perfusion AB).
Safety and effectiveness of the XVIVO system
Cypel et al (2011) reported on their experience using the XVIVO system for lungs from 23
donors identified as high-risk for transplantation.
58 In 2012, the same research group
reported on the results of the first 50 consecutive ex-vivo lung perfusions on marginal lungs, which included the results of the 2011 study, therefore only results from the 2012 study are
During the 39 month study period, a total of 317 lung transplantations were performed in the University of Toronto. When patients on extracorporeal life support as a bridge to transplantation were excluded, a total of 253 patients underwent a conventional transplantation (controls) and 50 transplants were performed following EVLP with the
XVIVO system using the acellular Toronto protocol (level III-2 intervention evidence). A further eight lungs underwent EVLP, however, they did not meet the functional criteria required and were rejected for transplantation. Of the 50 EVLP lungs, 22 were obtained from category III controlled DCD donors and 28 came from DBD donors. There were
significant differences in the characteristics between EVLP and control donor lungs (Table
Table 12
Characteristics of donated lungs 59
Donor variable EVLP (n=50) Controls (n=253) p value
Mean age (years)
DCD (%)
Best PO
2
:FiO
2 mmHg
Chest x-ray abnormalities (%)
Positive bronchoalveolar lavage culture (%)
45
44
334
67
70
45
5.1
452
45
55
0.52
0.001
0.001
0.001
0.05
After 1-hour of EVLP, the median PO
2
:FiO
2 ratio improved from 334 to 478 mmHg, and again improved to 513 mmHg after 4-hours of EVLP (p=0.001). Post-transplant outcomes are
summarised in Table 13. There was no difference in any of the reported outcomes between
EVLP treated lungs and controls. Although EVLP tended to have less primary graft dysfunction, this was not significant. It may be expected that outcomes in the EVLP group may be poorer for lungs obtained from DCD compared to DBD donors, however when results were stratified by donor type there was no difference in outcomes. . In addition, there was no difference in survival in EVLP recipients who were transplanted with donor lungs with a PO
2
:FiO
2
less than 300 mmHg compared to those donor lungs with a higher
New and emerging organ perfusion systems: July 2014 35
PO
2
:FiO
2
(>300 mmHg). The authors stated that although numbers of DBD donors had decreased over time, the number of lung transplants performed in their centre had remained stable with the use of EVLP, which accounted for 10-15 per cent of the transplant program. The authors also acknowledged that these results need to be replicated in an
Table 13 Post-transplant outcomes comparing EVLP and controls
EVLP (n=50) Controls (n=253) p value
Primary graft dysfunction at 72 hours (%)
Extracorporeal life support (%)
Median mechanical ventilation (days)
2
2
2 (1-101)
8.5
2.7
2.2 (1-43)
0.14
1.0
0.30
Median ICU stay (days)
Median hospital stay (days)
30-day mortality (%)
1-year survival (%)
3-year survival (%)
4 (1-100)
20 (7-156)
4
87
70
4.5 (1-257)
23 (1-299)
3.5
86
72
0.32
0.11
1.0
1.0
0.86
Anastomotic stricture requiring intervention (%) 4 4 1.0
A small study conducted in Austria by Aigner et al (2012) using DBD donors , whilst not explicitly stating that they used the XVIVO system, reported on the use of the Toronto protocol to recondition 13 lungs considered unacceptable for transplantation. Outcomes from these transplanted lungs were compared to 119 standard lungs transplanted during the same period (level III-2 intervention evidence). The Toronto protocol was followed, with a period of warming, followed by ventilation once normothermia had been reached and functional assessment was conducted after 15 minutes at a FiO
2
All donated marginal lungs had a PO
2
:FiO
2
less than 300 mmHg (median 216 mmHg), compared to a median value of 447 mmHg for the standard donated lungs. Donor cause of death, age, duration of intubation and length of ICU stay in EVLP donated lungs were comparable to standard lungs. Median total ischaemic time was 577 minutes (range 486-
678 minutes). EVLP was performed for 2-4 hours on all lungs. EVLP was discontinued on four lungs, which were discarded, due to deterioration or poor gas exchange with the
In the nine transplanted lungs, PO
2
:FiO
2
improved to a median of 466 mmHg (range 434 to
525 mmHg). The rejected lungs had a median PO
2
:FiO
2
of 372 mmHg. One patient with
New and emerging organ perfusion systems: July 2014 36
secondary pulmonary hypertension was placed on prolonged ECMO g
post-operatively. Of the remaining eight patients, seven had a primary graft dysfunction score of zero and one patient had a score of one at both 24 and 72 hours. Median duration of ventilation was two days and median ICU and hospital stay was 5.5 (range 3-18 days) and 20 (range 14-59 days) days, respectively. Although no patients died in the 30-day post-operative period, one patient died during their stay in a rehabilitation centre at day 54 due to sudden cardiac death and another patient died at 280 days due to sepsis. There were no significant differences in the outcomes of these EVLP transplanted lungs when compared to the
Another UK study by Zych et al (2012) compared the outcomes of 13 consecutive EVLP transplanted lungs to those of 86 standard lung transplantations (level III-2 intervention evidence). The majority of the donated lungs came from DBD donors; however, three were from DCD donors. Interestingly, nine donors were current or past smokers. Mean PO
2
:FiO
2 was 318 ± 110 mmHg, with four donors having a PO
2
:FiO
2
<300 mmHg. Prior to donation,
the average duration of mechanical ventilation was 102.6 ± 91.92 hours.
Of the 13 lungs, only six proceeded to transplantation with seven being considered unacceptable for transplantation due to various reasons including excessive pulmonary oedema and an atrial cuff considered too short to perform an anastomosis. Of the six transplanted lungs, two were from DCD donors. The average ischaemic and EVLP time was
448.8 ± 161 and 127 ± 16 minutes, respectively. Median length of ICU stay was considerably longer in the EVLP patients compared to the standard transplant patients (20.5 versus 7 days), however length of hospital stay was similar in both groups (38 and 37 days). The difference in median length of ICU stay was mainly due to one patient who underwent complex cardiac surgery prior to the lung transplant procedure. This patient was placed on
ECMO upon arrival in ICU. The mean PO
2
:FiO
2
of the remaining five patients upon arrival in
ICU was 291.2 ± 56.5 mmHg, with two patients being below 300 mmHg (195 and 285 mmHg). At 3-months all patients were alive; however one patient died at 203 days posttransplant due to a resistant Ralstonia pickettii chest infection. No primary graft dysfunction
These two small studies demonstrated that EVLP using the XVIVO/Toronto method is feasible and that not all lungs can be “reconditioned” to appropriate physiological parameters for transplantation.
Economic evaluation of the XVIVO system
No economic analyses on XVIVO system could be identified. g ECMO = extracorporeal membrane oxygenation
New and emerging organ perfusion systems: July 2014 37
Vivoline® LS1
The Vivoline® LS1 is based on the original normothermic lung perfusion research conducted
by Steen and first published in 2001.
65 The system contains two main parts: an evaluation
unit and a disposable lung chamber. The evaluation unit has a roller pump, a heater cooler unit, a gas system and software. The system is run from the monitor where the desired pressure, flow and temperature are set. The disposable lung chamber, which is provided sterile and pre-assembled, contains a lung box, an oxygenator, tubes, temperature probes,
pressure measurement and a leukocyte filter (Figure 11).
As with the XVIVO, Vivoline® LS1
is intended for the reconditioning, evaluation and preservation of lungs ex-vivo, after donation and prior to transplantation. The system is primed with 2 litres of Steen solution
containing washed red cells (haematocrit 10-15%).
The pulmonary artery of the cold lung is cannulated and the trachea is connected with a tube. The lung is gradually warmed to normothermia (reconditioning phase) and ventilation is started at approximately 32 C. Once normothermia is reached the lung is assessed and may be improved with ventilation/circulation, depending on the condition of the organ.
During the reconditioning phase oxygen is provided to the circulation. Once the lung has improved function, the system is switched into the evaluation phase and oxygen is only provided via ventilation. At this point blood gases and cardiac output are assessed. The circulating perfusate does not need to be exchanged due to the presence of the red blood cells. If the lungs satisfy transplantation criteria they are cooled to < 10 C and may be stored
in the system for up to 22 hours (Figure 12) (personal correspondence Vivoline Medical).
The Vivoline LS1 is currently being trialled at The Prince Charles Hospital in Brisbane and a
summary of their experience can be found in Appendix 1.
Figure 11 The Vivoline ®
LS1 lung perfusion system, showing the disposable lung chamber 66
New and emerging organ perfusion systems: July 2014 38
Figure 12 The phases and settings of EVLP using the Vivoline ®
Cost of the Vivoline® LS1
The price of the system is approximately €99,000 h with the cost of disposables averaging
€9,500, however this will vary depending on the volume ordered. Both wet lab and on-site training is included in the purchase price, with refresher training provided free of charge.
Vivoline’s maintenance agreement may provide an extra system free of charge for research purposes (marked not for clinical use). In addition, systems may be upgraded to the latest version every fourth year (personal correspondence Vivoline Medical).
Safety and effectiveness of the Vivoline® LS1
A number of feasibility studies describing the development of the Vivoline® system dating from the early 2000s were identified, however due to their age, these studies were not included in this overview. Wallinder et al (2012) reported on the results of six pairs of DBD donor lungs that were considered marginal and unsuitable for transplantation (level IV intervention evidence). The majority of the lungs had inferior blood gases and one had advanced bilateral infiltrates visible on chest x-ray. These lungs underwent reconditioning with the Vivoline® system. The mean transportation time from cold flush to commencement of EVLP was 221 ± 64 minutes. Mean PO
2
:FiO
2 of the donor lungs was 180 ± 90 mmHg.
During the reconditioning phase the system was primed with 2.0 litres of Steen Solution mixed with red blood cells to a haematocrit level of 10-15 per cent. Perfusion was initiated at a low level until the lungs reached a normothermic temperature. During the evaluation phase the perfusate was deoxygenated. After evaluation the lungs were cooled to 12°C with
h On 16 th July 2014, €99,000 = $143,434 and €9,500 = $13,764
New and emerging organ perfusion systems: July 2014 39
Two pairs of lungs had oedema and low PO
2
:FiO
2 ratios, therefore two patients underwent single lung transplantation, with the remaining patients undergoing a double. Mean EVLP time was 231.8 ± 95.6 minutes, with the two sets of lungs with oedema taking markedly longer (305 and 393 minutes). Almost half of this time was the time taken for reconditioning
The mean PO
2
:FiO
2 ratio post-EVLP was 430.4 ± 82.5 mmHg. The time to extubation ranged from 3 to 7 hours with the exception of one patient. This patient received one of the single lungs, which once transplanted showed immediate signs of dysfunction. The patient developed grade 2 primary graft dysfunction at 36 hours and remained on ventilation in ICU for 24 days. Excluding this patient, the average stay in ICU was 72 hours. Two other patients developed grade 1 primary graft dysfunction at 72 hours. All patients survived to 30-days
and were discharged from hospital.
The results from the initial experience of The Prince Charles Hospital (as described in
Appendix 1) were presented at the 2013 International Society for Heart and Lung
Transplantation conference. Due to the brief nature of the abstract, limited information was provided. Although EVLP was indicated for 16 donor lungs, only four lungs reconditioned by
EVLP were transplanted. Mean EVLP time was 140 ± 32 minutes which resulted in a mean
PO
2
:FiO
2 of 458 ± 37 mmHg, an improvement over the mean donor PO
2
:FiO
2 of 189 ± 96 mmHg. EVLP patient outcomes were compared to 25 standard lung transplantations. There was no difference between the two groups in time to extubation, length of ICU or hospital stay or incidence of acute rejection. No EVLP patients developed primary graft dysfunction compared to three in the standard transplantation group and all EVLP patients had survived
Organ Care System™
TransMedics manufactures the Organ Care System™, a portable normothermic perfusion system that is designed to perfuse and allow continuous functional, biochemical and metabolic assessment of lungs and hearts (see below) from the time of donation to the time
of transplantation (Figure 13).
Refer to page 49 below for cost details.
New and emerging organ perfusion systems: July 2014 40
Figure 13
The Organ Care System™ perfusing donated lungs and schematic of the system 69
As with the XVIVO, the Organ Care System™ is designed to “recondition” marginal lungs and to assess the viability of perfused lungs prior to transplantation. Oxygenated blood (15-25% red blood cells) is circulated through the lung via a pulsatile pump, using a proprietary
perfusate that contains nutrients and other substrates.
The OCS protocol is designed for
normothermic transportation of lungs.
The company was contacted for information in respect to regulatory status, diffusion and costing, however no response was received.
Only one study could be identified that reported on the use of the Organ Care System™ in a small pilot study (n=12), which was conducted by the lead author of the ongoing INSPIRE
RCT (described below) (level IV intervention evidence).
transplanted within the same centre and lungs were all obtained from DBD donors bar one category I DCD donor. Donor lungs were ranked according to a lung quality score, with factors including increased age, impaired oxygenation capacity or evidence of abnormalities, such as pneumonia, increasing the score. Those scoring less than nine were considered ideal lungs for transplantation, however, six of the donated lungs scored seven or six out of nine.
Donated lungs were required to have a PO
2
:FiO
2
>300 mmHg, with the mean reported ratio at time of donation of 463.9 ± 91.4 mmHg.
The mean perfusion time was 303 ± 105 minutes (range 188-622 mins), with no donor lungs being lost. The mean PO
2
:FiO
2
after perfusion was 471.6 ± 127.9 mmHg, which was not significantly different from the mean baseline measure ( p =0.72). At time of follow-up, 11/12 patients had survived, with survival time post-transplant ranging from 414 to 529 days. The one remaining patient died on day 140 post-transplant due to cardiomyopathy of unknown origin. Two recipients required an extended period of mechanical ventilation (117 and 456
New and emerging organ perfusion systems: July 2014 41
hours) both of whom received extended criteria lungs and one recipient receiving lungs that were substantially size mismatched. When these two patients were excluded, mechanical ventilation time ranged from 16.5 to 36 hours. ICU stay ranged from 30 to 742 hours (mean
314 hours). At 72 hours post-transplant, no patient had a primary graft dysfunction grade 3 score. The mean best forced expiratory volume as a per cent if predicted measured at 1year post-transplant was 87 ± 21 per cent.
Although this study is limited by its size and the lack of a control group, it does appear that assessing the viability of organs with the Organ Care System™ is feasible. The results of the
INSPIRE RCT, along with a cost analysis, would better inform clinical practice.
Ongoing research
A number of ongoing clinical trials assessing the use of machine perfusion for lung transplantation were identified.
The ‘ Phase 2 Study of Ex-vivo Perfusion and Ventilation of Lungs to Assess Transplant
Suitability ’ was being conducted by the University of North Carolina and sponsored by
Vitrolife and XVIVO Perfusion. This non-randomised study commenced in 2010, however recruitment was suspended in 2013 with no reason stated ( NCT01241942 ). The purpose of this study was to assess the safety of transplanting ventilated lungs (XVIVO lung perfusion machine) and perfused with a lung perfusion solution (Steen solution™). The same research group is, however, currently recruiting recipients (n=10) for the ‘ Ex-vivo Perfusion and
Ventilation of Lungs Recovered From Non-Heart-Beating Donors to Assess Transplant
Suitability ’ non-randomised study ( NCT01615484 ). This study commenced in 2013 and expects to be finalised by 2017. Outcomes from patients transplanted with DCD lungs will be compared to outcomes in patients transplanted with lungs from conventional brain-dead organ donors. Primary outcome measures are 30-day mortality, graft survival and primary lung graft dysfunction. Secondary outcome measures include length of ICU stay, day 7 ventilator/ECMO status, recipient mortality at 12-months and bronchiolitis obliterans syndrome.
A large, non-randomised multi-centre comparative study is currently being conducted by the University of Colorado, sponsored by XVIVO Perfusion ( NCT01365429 ). This study began in 2011 and expects to recruit 104 recipients by May 2014. Human donor lungs that do not meet the standard clinical criteria for donor lung utilisation but fit into the study inclusion criteria will be retrieved from donors. Donor lungs will be prepared using ex vivo perfusion with Steen solution with the addition of methylprednisolone, heparin and antibiotics.
Criteria for donor lungs include: a delta pO2 (Δ pO2 = Pulmonary vein pO2 - pulmonary artery pO2) during ex vivo perfusion assessment > 350mmHg and good lung compliance.
XVIVO prepared lungs will be compared to recipient lung transplant patients that receive donor lungs via conventional transplant. The primary outcome measure will be 30-day mortality. Secondary outcome measures include length of ICU stay, day 7 ventilator/ECMO
New and emerging organ perfusion systems: July 2014 42
status, recipient mortality at 12-months and primary lung graft dysfunction scores at 0,
24,and 72 hours.
The DEVELOP-UK study (Donor Ex-vivo Lung Perfusion in UK Lung Transplantation,
ISRCTN44922411 ) is a non-randomised, non-inferiority multi-centre comparative study that intends to evaluate the clinical and cost effectiveness of lungs transplanted after EVLP reconditioning with the Vivoline® LS1 system. The study is aiming to recruit 306 and 102 adult patients with advanced lung disease to the standard and EVLP arms, respectively. The
90-day and 12-month mean cost of undertaking lung transplant using EVLP lungs and standard donor lungs will be assessed. The study is designed to demonstrate non-inferiority of EVLP in terms of 12 month survival. Quality of life will also be determined at 3- and 12months post-transplant. This study commenced in January 2012 and expects to have results published by April 2016.
The INSPIRE Trial is an international multicentre RCT, FDA pivotal trial comparing preservation of donor lungs using the Organ Care System™ OCSTM device to SCS. A total of
264 primary lung transplant recipients will be randomised into the trial. Donor inclusion criteria: age < 65 years, normal gas exchange at time of final acceptance of donor lung, and no active primary pulmonary disease. Primary endpoints include patient and graft survival at
30-days post-transplantation, and rate of primary graft dysfunction at 72 hours post-
transplantation. To date, 60 patients have been transplanted in the trial. 71
New and emerging organ perfusion systems: July 2014 43
Summary
A total of three machine perfusion systems for lungs were identified. Of these, two are listed on the ARTG, the XVIVO and the Organ Care System, however the OCS listing does not specifically state whet her it is for OCS™ HEART or OCS™ LUNG . The remaining system, Lung
Assist is CE marked.
As of the end of 2012, there were 107 Australian and New Zealand patients on the lung transplant waiting list. In that same year, a total of 157 lung and four heart-lung transplants were performed.
The majority of XVIVO published peer-reviewed clinical studies describes the reconditioning of marginal lungs using the XVIVO system. No economic analysis could be identified.
XVIVO
Three non-randomised studies were identified that reported on outcomes of ex-vivo lung perfusion (EVLP) with the XVIVO system compared to controls. In the largest study (n=50), there was no difference between the EVLP group and controls in any of the outcomes measured. Unlike the studies conducted in kidneys, equivalent results between EVLP and control lungs can be considered in a favourable light as these reconditioned EVLP lungs would otherwise have been rejected for transplant.
Vivoline® system
There was limited recent published evidence available describing the Vivoline® system. The results from these preliminary studies demonstrate that the system is feasible for the reconditioning of marginal lungs.
Organ Care System™ - OCS™ LUNG
Only one small case series describing the outcome in patients transplanted with EVLP treated lungs all obtained from DBD donors. No conclusions as to the effectiveness of this system can be made due to the non-comparative nature of the study, however the system appears safe with survival time post-transplant ranging from 414 to 529 days.
New and emerging organ perfusion systems: July 2014 44
Liver
Renal machine perfusion protocols must be adapted for use in livers due to important differences in organ structure and anatomy including flow competition between the hepatic and portal systems, the susceptibility of damage to hepatic sinusoidal endothelial cells, high liver metabolism, the MP effect on preventing biliary tree injury, and Kupffer cell activation.
It is unclear at this current time whether or not normothermic or hypothermic MP would be
ideal for the treatment of livers.
Immediately after restoration of blood flow during reperfusion, mitochondria consume oxygen, resulting in the release of reactive oxygen species due to excessive mitochondrial electron leakage within the electron transport chain. Cells unable to cope with the resulting mitochondrial release of hydrogen peroxide, then release factors into the circulation, which in turn activate Kupffer cells. The Kupffer cells then produce large amounts of reactive oxygen species. In addition, cytokines and chemokines are released that trigger platelet and neutrophil adhesion, resulting in the release of more reactive oxygen species. Low pressure, hypothermic oxygenated perfusion would protect the liver from mitochondrial injury,
nuclear injury, Kupffer cell activation and endothelial injury.
It is hoped that the ability of MP to assess the viability of “marginal” organs via the measurement of markers such as aspartate transaminase (AST) and alanine transaminase
(ALT) prior to transplantation would increase the number of organs made available. Several other viability markers have been investigated including markers of hepatic damage such as liver fatty acid-binding protein (L-FABP), glutamate dehydrogenase (GLDH), α-glutathione-S-
transferase (α-GST), hyaluronic acid, and β-galactosidase.
donor pool by reconditioning marginal livers from DCD donors or steatotic liver grafts. DCD liver grafts are associated with increased reperfusion injury, post-transplant morbidity and graft loss. It is thought that poor outcomes are due to the ischaemic injury to the graft that occurs at time of cardiac death, which results in the development of late bile duct
A preliminary study by Guarrera et al (2010) used a non-commercial, experimental hypothermic perfusion system. Adult patients scheduled for orthotopic liver transplantation who had a MELD score i
<35 were eligible. The portal vein and hepatic artery were cannulated and perfusion was performed for between 3-7 hours, keeping the total cold ischaemic time to under 12-hours. Twenty recipients who received hypothermic perfused livers were compared to a matched group of controls who were transplanted with livers preserved by SCS (level III-3 intervention evidence). Although a statistical analysis of donor i MELD = model for end-stage liver disease, a scoring system for assessing the severity of chronic liver disease and uses values for serum bilirubin, serum creatinine, and the international normalised ratio for prothrombin time (INR) to predict survival. The higher the score, the lower the likelihood of survival. Scores of >40 associated with 71% mortality, 30-39 = 53% mortality, 20-29 = 20% mortality.
New and emerging organ perfusion systems: July 2014 45
characteristics was not performed, the intervention and control groups appeared to be similar apart from baseline measurements of AST (peak AST MP = 213.9 ± 92.8 vs controls
70.4 ± 11.2 IU/ml). Donor type was not stated. 74
The results from this preliminary study are summarised in Table 14. There was no significant
difference on any of the outcomes apart from the length of hospital stay, which was significantly lower in the MP intervention group. In addition, peak serum levels of markers of liver injury and renal function were significantly lower in the intervention group after MP compared to the control group apart from the INR. These results indicated that MP was
potentially of value prior to transplantation.
Table 14
Patient outcomes from initial hypothermic MP study in livers 74
MP (n=20) Controls (n=20) p value
Primary non-function
Early allograft dysfunction
Vascular complications
Hepatic artery stenosis
Biliary complications
Early bile leak
Hospital length of stay (days)
Graft and patient survival
0
1/20 (5%)
0
0
2
1
10.9 ± 4.7
18/20 (90%)
0
5/20 (25%)
1
1
4
1
15.3 ± 4.9
18/20 (90%) p=0.08 p=0.006
Death with functional grafts at 12-months 2 2
Liver Assist- Hypothermic Oxygenated PErfusion - HOPE
Organ Assist manufactures the ECOPS® device for the in-situ hypothermic oxygenated perfusion of livers, with the aim of reconditioning marginal organs and allowing evaluation
of parameters during perfusion (Figure 14). The company was contacted for information in
respect to regulatory status, diffusion and cost but no information was supplied.
Two studies were identified by the literature search, both published by the same research group, the developers of the technology. The first was an abstract presented to the 2013
International Congress of the International Liver Transplantation Society, reporting on the
first five recipients of ECOPS® perfused livers.
Since that time, Dutkowski et al (2013) have
published further results of eight patients, which include those described previously, therefore only the results from this study are presented.
All livers were obtained from category III DCD donors. Transplantation results in these recipients were compared to the historical results from matched DBD donors (level III-3 intervention evidence). There was no significant difference in any of the baseline
New and emerging organ perfusion systems: July 2014 46
characteristics of the DCD and DBD donors apart from the median donor risk index score, which was significantly higher in the DCD recipients (2.22 vs 1.47, p =0.007).
Organs experienced a median of 38 minutes (range 26-43 minutes) warm ischaemic time.
Median cold storage time prior to machine perfusion was 2.4 hours. Each liver was connected to the ECOPS® device and perfused through the portal vein alone with cool
(10°C) and oxygenated perfusate for a median of 2-hours (range 1.7-2.7 hours).
There was no difference in either the mean length of ICU stay (DCD 2 vs DBD 4.5 days, p =0.137) or hospital stay (DCD 16.5 vs DBD 18 days, p =0.341). At 6-months follow-up there was no difference between the two groups in bilirubin, alkaline phosphatase, γglutamyltransferase or creatinine levels, however glomerular filtration rate was significantly higher in the DCD recipients ( p =0.002). Graft and patient survival outcomes were not reported. Results from this initial study appear promising, however, the results from the
randomised controlled trial comparing ECOPS® outcomes to SCS would be of interest.
Figure 14 The ECOPS system, Organ Assist
OrganOx metra™
No clinical studies could be identified that described the use of the OrganOx metra™ device.
Only preliminary animal studies and studies describing the advantages of normothermic perfusion for donated livers were identified. In addition, the company was contacted for information in respect to regulatory status, diffusion and costing of the OrganOx metra™ device, however no response was received. The company’s web site states that the system will be commercially available in 2014.
New and emerging organ perfusion systems: July 2014 47
Ongoing research
Two clinical trials assessing the use of machine perfusion for liver transplantation were identified.
The ‘ Hypothermic Oxygenated Perfusion (HOPE) of Human Liver Grafts ’ double blind RCT conducted by the University of Zurich commenced recruitment in 2011 (expected n=70) and expects to be completed by September 2014 ( NCT01317342 ). Eligible patients will be randomised to either the HOPE perfusion or control group. Standard liver procurement will be performed at the site of organ donation, and the cold stored organ will be transported to the research centre. Following back table preparation, short term hypothermic oxygenated perfusion (HOPE group) for one hour will be performed vs continued cold storage (control).
The primary endpoint will be major post-operative complications (Grade ≥ III) according to the established Clavien classification. Secondary endpoints are postoperative peak ALT levels in the serum, duration of hospital and ICU stay, costs, and recipient and graft survival.
Additionally, we will assess liver graft biopsies taken at the end of liver transplantation for markers revealing inflammatory response and reperfusion injury.
A study investigating the safety and performance of the OrganOx Metra, for normothermic perfusion of livers, prior to transplantation was recently completed in the United Kingdom
( ISRCTN14355416 ). Results have yet to be published. Twenty patients were transplanted with livers perfused with the OrganOx system and the primary outcome of graft survival at
30-days was compared to a historical control group.
New and emerging organ perfusion systems: July 2014 48
Heart
Cardiac donor conversion rates even from standard criteria donors may be less than 50 per cent. A recent abstract presented to the International Society for Heart and Lung
Transplantation evaluated the quality of hearts rejected for transplantation and assessed their suitability for transplantation. The most common reasons for rejection were donor age, the quality and size of the organ and the social history of the donor. Hearts donated from 33 donors underwent functional evaluation. Of these 16 hearts were considered acceptable for transplantation, however only seven were offered for transplantation. This indicates that a large proportion of donated organs are considered marginal and are not
being transplanted, some of which may benefit from perfusion technology.
SCS of cardiac grafts are associated with anaerobic metabolism and requires short intervals between graft harvesting and transplant. In addition, prolonged ischaemia time is associated with poor 1-year survival with primary graft failure being a leading cause of death within the first month of transplant. MP may preserve myocardial trans-membrane ionic gradients, prevent lactate and adenosine build-up, allow for reparative processes in the ischaemic myocardium, and promoting excretion of toxic metabolites. MP perfusion heart transplantation studies conducted in animals reported increased levels of myocardial oedema which may be mediated by MP-dependent hydrostatic pressure and the lack of
lymphatic flow to the arrested heart.
Organ Care System™- OCS™ HEART
The Transmedics OCS™ HEART is a sterile portable pulsatile perfusion system that allows for organ preservation by pumping warm, nutrient- and oxygen-rich blood through the organ
3 No clinical studies could be identified that used the OCS™ HEART device. The
company was contacted for information in respect to regulatory status, diffusion and costing, however no response was received.
The OCS™ HEART device costs approximately US $200,000.
In Western Australia, a joint funding arrangement between the Heart and Lung Transplant
Foundation of WA Inc. (HLTF) and the Department of Health’s Office of the Chief Medical
Officer (OCMO) facilitated the purchase of the OCS™ HEART technology for heart transplant patients at the Royal Perth Hospital. The HLTF has funded the purchase of the OCS portable platform and backup unit (approximately US$360,000) and donated this equipment to WA
Health. In addition, the HLTF also funded the training of essential WA clinical staff in the use of the technology including a cardiac transplant surgeon, perfusionist and anaesthetist.
Departmental support included funding for three single-use heart perfusion modules per year (approximately $35,000/module) for two years and further clinical staff training
(personal communication Western Australia Department of Health).
New and emerging organ perfusion systems: July 2014 49
The OCS™ technology was identified as a technology with the potential to significantly reduce ischaemic time (European data reporting a total ischaemic time of 81 minutes), reduce post-transplant complications such as primary graft failure and to improve organ availability and utilisation. The OCS™ HEART technology allows for the ex-vivo treatment, optimisation and functional evaluation of donated hearts. This is of importance in a state such as Western Australia where a flight time of 5-6 hours precluded WA from accessing organs from the east coast, reducing the number of potential donors significantly.
Approximately 4-13 cardiac transplants are performed in WA each year, however the number of patients on the WA cardiac transplant waiting list is increasing. It is hoped that the OCS™ technology will allow potential access to a significantly expanded donor pool. In
July 2012 the OCS™ HEART technology was first used by the Royal Perth Hospital for the successful transplantation of a locally retrieved heart. As of November 2013, the Royal Perth
Hospital has used the OCS™ HEART technology to successfully support three WA heart transplant patients, with two transplants using organs obtained from interstate. This is fewer than the forecast number 3-6 patients per year, derived partly from a number of implementation issues including staffing implications posed by the OCS. With previous transport modes (cold storage), perfusionists were not required to attend to a donor organ during transport following retrieval. However, perfusionists are integral to support the donor heart during transport with the OCS™. It was necessary to address the costs associated with the on-call rostering of perfusionists, plus the staffing implications
(additional work demands) associated with the use of this technology (personal communication Western Australia Department of Health).
Other implementations issues include:
• Training: training of transplant teams (surgeon, perfusionist and anaesthetist) capable of using the machine successfully is an important, but costly, requirement. One team received training in the USA, while training of further Royal Perth Hospital cardiac transplant staff was undertaken at the University of Western Australia’s Clinical Training &
Evaluation Centre. This training used animal (pig) hearts to simulate retrieval, support and transport of human hearts using the OCS. There are learning curve challenges and implications for maintenance of skills for a complex but infrequently used piece of equipment with costly consumables.
• Air transport: the existing aircraft transport arrangements used for transport of a donor hearts retrieved from South Australia were not suitable for transporting the OCS™.
Additional staff, including a perfusionist and nurse are required to attend a donor heart retrieval that uses the OCS™, and the OCS™ machine dimensions exceeded the size of the door of the aircraft previously used for donor heart retrieval flights. The flights to retrieve donor hearts also potentially go a lot further than distances previously limited by organ
New and emerging organ perfusion systems: July 2014 50
ischaemic time. Costs for flights for appropriate aircraft range from $40,000-$80,000 depending on the distance (eg NT/Qld).
Organ access: there are implications for national rotational referral lists for heart and lung as previously WA was only on SA list due to ischaemic time limitations (personal communication Western Australia Department of Health).
The OCS™ HEART device is also being trialled at St Vincent’s Hospital, Sydney. The trial is comparing the OCS device to cold storage especially in extended criteria or marginal donors.
Current experience with the OCS™ HEART is that the device fits into a standard retrieval aircraft (personal communication NSW Ministry of Health).
Figure 15
A schematic describing the use of the OCS™ HEART 78 and the perfusion module
Transmedics cites benefits of the OCS™ HEART include health system cost-savings from reductions in waiting list costs, such as the need for left ventricular assist devices, ICU usage and multiple hospital admissions, and reductions in post-transplant costs due to reduced complications.
LifeCradle® HR
The LifeCradle® is a lightweight, portable device that is capable of extending the preservation time to more than 12 hours. The donated heart is placed into the temperaturecontrolled LifeCradle® capsule and after connection, an oxygenated, hypothermic perfusate
is pumped through the organ (Figure 16).
The company was contacted for information in
respect to regulatory status, diffusion and costing, however no response was received.
Apart from one abstract presented to the 2009 Society for Heart and Lung Transplantation conference, only animal studies could be identified. The abstract by Cobert et al described the performance of the LifeCradle® device when used to perfuse donated hearts that were
New and emerging organ perfusion systems: July 2014 51
considered unsuitable for transplantation. Perfused hearts were not intended to be transplanted. The results of this study demonstrated that the LifeCradle® supported
myocardial metabolism in the absence of myocardial oedema.
Figure 16 The LifeCradle ®
Sherpa Pak™
The Sherpa Perfusion ™ Cardiac Transport System is a fully disposable oxygenated perfusion
system (Figure 17), capable of extending ischaemic time to 12-hours, designed specifically
for the transportation of donor hearts.
Figure 17 The Sherpa Perfusion™ Cardiac Transport System
In June 2013, Paragonix announced that an abstract titled ‘An Innovative, Novel
Hypothermic Storage System For Donor Hearts’, describing the use of the Sherpa Pak™ for cardiac transport was presented to the 16th Congress of the European Society for Organ
Transplantation. This abstract could not be identified from the conference abstracts. Other
literature identified described the principles of the technology, 81 that is, the use of
oxygenated hypothermic perfusion. No human clinical studies could be identified. Although the company was contacted to supply information in respect to regulatory status, diffusion and costing, no reply was received.
New and emerging organ perfusion systems: July 2014 52
Ongoing research
Although the TransMedics sponsored ‘Organ Care System Cardiac for Preservation of
Donated Hearts for Eventual Transplantation’ multi-centre RCT ( NCT00855712 ) was due to be completed in September 2013, it is still recruiting patients (n=128). The OCS maintains organ viability by providing near-normal physiological conditions, continuously perfusing the donated heart with warm, oxygenated blood. The OCS preserves and monitors the organ's perfusion and metabolic state after explantation from a donor and connection to the device, during transportation to the recipient site, and until disconnection from the device. The primary outcome measure is 30-day patient survival.
New and emerging organ perfusion systems: July 2014 53
Summary of findings
A total of 10 different perfusion systems were identified, some of which are designed for multiple organ types. Many of these systems are still in a development stage.
The most mature evidence base to date is that for the hypothermic perfusion of kidneys using the LifePort Kidney Transporter, with several well conducted RCTs published. Results from these studies are mixed, however, when the largest study is considered the odds of delayed graft function were lower and the rate of 1-year graft survival was higher in those recipients who were transplanted with a MP kidney compared to SCS controls. When these results were used in a cost-effectiveness analysis, MP was cost-effective compared to SCS.
Origin of donor organs (DCD or DBD or extended criteria) varied greatly between the studies and made direct comparisons of outcomes difficult.
The evidence base for the normothermic reconditioning of marginal lungs is poor, however from initial results there appears to be no difference in outcomes in patients who received
EVLP lungs compared to controls. Unlike the studies conducted in kidneys, equivalent results between EVP and control lungs can be considered in a favourable light as these reconditioned EVLP lungs would otherwise have been rejected for transplant. Anecdotal accounts from Australian researchers report favourable outcomes with the use of the XVIVO system, with an increase in the number of viable organs able to be transplanted.
There is little published evidence describing the use of perfusion systems for liver or heart transplantation.
There is a great variation in the price of systems, with some designed to be wholly disposable.
It is clear that more randomised controlled trials are required. Several of the systems identified are currently conducting RCTs, and the results of these studies will greatly inform decision making. Studies using single donor origin (DCD or DBD or extended criteria donors) would be helpful.
HealthPACT assessment
Organ perfusion technologies may have the potential to significantly impact on health care in Australia and New Zealand. The most mature evidence base regarding the use of perfusion systems for the preservation of kidneys indicates reduced rates of delayed graft function, which may represent significant savings to the health system. It is too early in the development phase to make conclusions in respect to cardiac and lung perfusion systems as the evidence base is still maturing, however lung perfusion may result in an increased number of organs able to be transplanted.
Some jurisdictions, where distance and remote locations are an issue, may choose to invest in this technology, whilst others may not. In Australia, organ procurement by some states
New and emerging organ perfusion systems: July 2014 54
currently operates under limitations imposed by distance. The introduction of technologies which may extend ischaemic time may lead to a requirement to review policy and procedures around organ donation, collection and distribution.
Number of studies included
All evidence included for assessment in this Technology Brief has been assessed according to the revised NHMRC levels of evidence. A document summarising these levels may be accessed via the HealthPACT web site .
Search criteria to be used (MeSH terms)
Search terms: (machine perfusion AND (transplantation OR preservation OR perfusion OR storage) AND (heart OR lung OR liver OR kidney OR pancreas OR small bowel)) AND Humans
[Mesh] AND English language.
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
Organ Transport Systems Inc (2012). Our Technology. Available from: http://organtransportsystems.com/OurTechnology.html
[Accessed 4th February
2014].
Wight, J. P., Chilcott, J. B.et al (2003). 'Pulsatile machine perfusion vs. cold storage of kidneys for transplantation: a rapid and systematic review'. Clinical transplantation ,
17 (4), 293-307.
Balfoussia, D., Yerrakalva, D.et al (2012). 'Advances in machine perfusion graft viability assessment in kidney, liver, pancreas, lung, and heart transplant'.
Experimental and clinical transplantation : official journal of the Middle East Society for Organ Transplantation , 10 (2), 87-100.
Van Raemdonck, D., Neyrinck, A.et al (2013). 'Machine perfusion in organ transplantation: a tool for ex-vivo graft conditioning with mesenchymal stem cells?'.
Current opinion in organ transplantation , 18 (1), 24-33.
Lam, V. W., Laurence, J. M.et al (2013). 'Hypothermic machine perfusion in deceased donor kidney transplantation: a systematic review'. The Journal of surgical research ,
180 (1), 176-82.
Neyrinck, A., Van Raemdonck, D.& Monbaliu, D. (2013). 'Donation after circulatory death: current status'. Current opinion in anaesthesiology , 26 (3), 382-90.
NHMRC (2010). National Protocol for Donation after Cardiac Death , Australian Organ and Tissue Donation and Transplantation Authority, Canberra http://www.donatelife.gov.au/Media/docs/DCD%20protocol%20020311-0e4e2c3d-
2ef5-4dff-b7ef-af63d0bf6a8a-1.PDF
.
Hosgood, S. A., Nicholson, H. F.& Nicholson, M. L. (2012). 'Oxygenated kidney preservation techniques'. Transplantation , 93 (5), 455-9. van Smaalen, T. C., Hoogland, E. R.& van Heurn, L. W. (2013). 'Machine perfusion viability testing'. Current opinion in organ transplantation , 18 (2), 168-73.
New and emerging organ perfusion systems: July 2014 55
10. Bon, D., Chatauret, N.et al (2012). 'New strategies to optimize kidney recovery and preservation in transplantation'. Nature reviews Nephrology , 8 (6), 339-47.
11. Catena, F., Coccolini, F.et al (2013). 'Kidney preservation: Review of present and future perspective'. Transplantation proceedings , 45 (9), 3170-7.
12. AIHW (2005). Chronic kidney disease in Australia , Australian Institute of Health and
Welfare, Canberra http://www.aihw.gov.au/publications/phe/ckda05/ckda05.pdf
.
13. AIHW (2012). Australia’s health 2012 , Australian Institute of Health and Welfare,
Canberra http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=10737422169 .
14. Grace, B., Hurst, K.& McDonald, S. (2011). Stock and flow , Australia and New Zealand
Dialysis & Transplant Registry http://www.anzdata.org.au/anzdata/AnzdataReport/34thReport/2011c01_stockflo w_v1.2.pdf
.
15. AIHW (2011). Cardiovascular disease: Australian facts 2011 , Australian Institute of
Health and Welfare, Canberra http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=10737418530 .
16. Principal diagnosis data cubes [database on the Internet]. Australian Institute of
Health and Welfare. 2014 [cited 17th January 2014]. Available from: http://www.aihw.gov.au/principal-diagnosis-data-cubes/ .
17. Publicly Funded Hospital Discharges - 1 July 2010 to 30 June 2011 [database on the
Internet]2013 [cited 17th January 2014]. Available from: http://www.health.govt.nz/publication/publicly-funded-hospital-discharges-1-july-
2010-30-june-2011 .
18. Keogh, A., Williams, T.& Pettersson, R. (2012). Australia and New Zealand
Cardiothoracic Organ Transplant Registry 2012 Report , Australia and New Zealand
Cardiothoracic Organ Transplant Registry, Sydney http://www.anzcotr.org.au/uploadedFiles/1279001464281-56522.pdf
.
19. AIHW (2010). Asthma, chronic obstructive pulmonary disease and other respiratory diseases in Australia , Australian Institute of Health and Welfare, Canberra
20. Australian Health Survey: First Results, 2011–12 — Australia [database on the
Internet]. Australian Bureau of Statistics. 2012 [cited 20th January 2014]. Available from: http://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/4364.0.55.0012011-
12?OpenDocument
.
21. AIHW (2013). How many die from COPD? [Internet]. Australian Institute of Health and Welfare. Available from: http://www.aihw.gov.au/copd/mortality/ [Accessed
20th January 2014].
22. GESA (2013). The economic cost and health burden of liver diseases in Australia , The
Gastroenterological Society of Australia/Australian Liver Association, Melbourne http://www.gesa.org.au/files/editor_upload/File/GESA%20report%2028032013_we b.pdf
.
23. Henry, S. D.& Guarrera, J. V. (2012). 'Protective effects of hypothermic ex vivo perfusion on ischemia/reperfusion injury and transplant outcomes'. Transplantation reviews (Orlando, Fla) , 26 (2), 163-75.
New and emerging organ perfusion systems: July 2014 56
24. ANZOD (2013). 2013 ANZOD Annual Report Australia and New Zealand Organ
Donation (ANZOD) Registry, Adelaide, South Australia http://www.anzdata.org.au/anzod/v1/AR-2013.html
.
25. McAnulty, J. F. (2010). 'Hypothermic organ preservation by static storage methods:
Current status and a view to the future'. Cryobiology , 60 (3 Suppl), S13-9.
26. O'Callaghan, J. M., Morgan, R. D.et al (2013). 'Systematic review and meta-analysis of hypothermic machine perfusion versus static cold storage of kidney allografts on transplant outcomes'. The British journal of surgery , 100 (8), 991-1001.
27. Moers, C., Smits, J. M.et al (2009). 'Machine perfusion or cold storage in deceaseddonor kidney transplantation'. The New England journal of medicine , 360 (1), 7-19.
28. Bathini, V., McGregor, T.et al (2013). 'Renal perfusion pump vs cold storage for donation after cardiac death kidneys: a systematic review'. The Journal of urology ,
189 (6), 2214-20.
29. Deng, R., Gu, G.et al (2013). 'Machine perfusion versus cold storage of kidneys derived from donation after cardiac death: a meta-analysis'. PloS one , 8 (3), e56368.
30. Jochmans, I., Moers, C.et al (2010). 'Machine perfusion versus cold storage for the preservation of kidneys donated after cardiac death: a multicenter, randomized, controlled trial'. Annals of surgery , 252 (5), 756-64.
31. Watson, C. J., Wells, A. C.et al (2010). 'Cold machine perfusion versus static cold storage of kidneys donated after cardiac death: a UK multicenter randomized controlled trial'. American journal of transplantation : official journal of the American
Society of Transplantation and the American Society of Transplant Surgeons , 10 (9),
1991-9.
32. van der Vliet, J. A., Kievit, J. K.et al (2001). 'Preservation of non-heart-beating donor kidneys: a clinical prospective randomised case-control study of machine perfusion versus cold storage'. Transplantation proceedings , 33 (1-2), 847.
33. Matsuno, N., Sakurai, E.et al (1994). 'The effect of machine perfusion preservation versus cold storage on the function of kidneys from non-heart-beating donors'.
Transplantation , 57 (2), 293-4.
34. Organ Recovery Systems (2014). LifePort
®
Kidney Transporter 1.1 Brochure. Available from: http://www.organ-recovery.com/pdfs/Kidney-Transporter-1-
1/LifePort1.1_Brochure.pdf
[Accessed 23rd January 2014].
35. Moers, C., Pirenne, J.et al (2012). 'Machine perfusion or cold storage in deceaseddonor kidney transplantation'. The New England journal of medicine , 366 (8), 770-1.
36. Gallinat, A., Moers, C.et al (2013). 'Machine perfusion versus static cold storage in expanded criteria donor kidney transplantation: 3-year follow-up data'. Transplant international : official journal of the European Society for Organ Transplantation , 26
(6), E52-3.
37. Sedigh, A., Tufveson, G.et al (2013). 'Initial experience with hypothermic machine perfusion of kidneys from deceased donors in the Uppsala region in Sweden'.
Transplantation proceedings , 45 (3), 1168-71.
New and emerging organ perfusion systems: July 2014 57
38. Szabo, L., Bill, C.et al. Hypothermic machine perfusion improves outcomes in DCD kidneys with long cold ischemia time. 24th International Congress of the
Transplantation Society; 27 Sep; Berlin, Germany: Transplantation; 2012. p. 279.
39. Forde, J. C., Shields, W. P.et al. Single centre experience of hypothermic continuous machine perfusion of kidneys from extended criteria deceased heart-beating donors.
24th International Congress of the Transplantation Society; 27 Sep; Berlin, Germany:
Transplantation; 2012. p. 512.
40. Gallinat, A., Moers, C.et al (2012). 'Machine perfusion versus cold storage for the preservation of kidneys from donors >/= 65 years allocated in the Eurotransplant
Senior Programme'. Nephrology, dialysis, transplantation : official publication of the
European Dialysis and Transplant Association - European Renal Association , 27 (12),
4458-63.
41. Patel, S. K., Pankewycz, O. G.et al (2012). 'Prognostic utility of hypothermic machine perfusion in deceased donor renal transplantation'. Transplantation proceedings , 44
(7), 2207-12.
42. NICE (2009). Machine perfusion systems and cold static storage of kidneys from deceased donors , National Institute for Health and Clinical Excellence, London www.nice.org.uk/TA165 .
43. Bond, M., Pitt, M.et al (2009). 'The effectiveness and cost-effectiveness of methods of storing donated kidneys from deceased donors: a systematic review and economic model'. Health technology assessment (Winchester, England) , 13 (38), iii-iv, xi-xiv, 1-
156.
44. Garfield, S. S.& Evans, R. W. (2010). 'Machine perfusion cost-effectiveness versus cold storage has been demonstrated; limiting use to marginal donor kidneys unjustified'. Transplant international : official journal of the European Society for
Organ Transplantation , 23 (11), e67-8.
45. Gomez, V., Galeano, C.et al (2012). 'Economic impact of the introduction of machine perfusion preservation in a kidney transplantation program in the expanded donor era: cost-effectiveness assessment'. Transplantation proceedings , 44 (9), 2521-4.
46. Garfield, S. S., Poret, A. W.& Evans, R. W. (2009). 'The cost-effectiveness of organ preservation methods in renal transplantation: US projections based on the machine preservation trial'. Transplantation proceedings , 41 (9), 3531-6.
47. Wszola, M., Kwiatkowski, A.et al (2013). 'One-year results of a prospective, randomized trial comparing two machine perfusion devices used for kidney preservation'. Transplant International , 26 (11), 1088-96.
48. Waters Medical Systems (2008). RM3. Available from: http://www.wtrs.com/transplant.html
[Accessed 30th January 2014].
49. Ciancio, G., Gaynor, J. J.et al (2010). 'Favorable outcomes with machine perfusion and longer pump times in kidney transplantation: a single-center, observational study'. Transplantation , 90 (8), 882-90.
50. Ciancio, G., Gaynor, J. J.et al (2012). 'Machine perfusion following static cold storage preservation in kidney transplantation: donor-matched pair analysis of the prognostic impact of longer pump time'. Transplant international : official journal of the European Society for Organ Transplantation , 25 (1), 34-40.
New and emerging organ perfusion systems: July 2014 58
51. Basu, A., McMichael, J.et al (2011). 'Kidney transplantation from expanded criteria donors following machine perfusion: Four-year outcomes'. American Journal of
Transplantation , Conference: 11th American Transplant Congress, 11, 228-9.
52. Portable Organ Perfusion (2010). Portable Organ Perfusion. Available from: http://www.portableorganperfusion.com/ [Accessed 24th January 2014].
53. Dirkes, M. C., Post, I. C. J. H.et al (2013). 'A novel oxygenated machine perfusion system for preservation of the liver'. Artificial organs , 37 (8), 719-24.
54. Hosgood, S. A., Mohamed, I. H.et al (2011). 'Hypothermic machine perfusion after static cold storage does not improve the preservation condition in an experimental porcine kidney model'. The British journal of surgery , 98 (7), 943-50.
55. Doorschodt, B. M., Schreinemachers, M. C. J. M.et al (2009). 'Evaluation of a novel system for hypothermic oxygenated pulsatile perfusion preservation'. International
Journal of Artificial Organs , 32 (10), 728-38.
56. BusinessWire (2013). Available from: http://www.businesswire.com/news/home/20131217005181/en#.UuHLTax_V_M
[Accessed 24th January 2014].
57. Organ Assist (2011). Kidney Assist. Available from: http://www.organassist.nl/images/Products/brochure/kidneyassistinfo.jpg
[Accessed 31st January
2014].
58. Cypel, M., Yeung, J. C.et al (2011). 'Normothermic ex vivo lung perfusion in clinical lung transplantation'. The New England journal of medicine , 364 (15), 1431-40.
59. Cypel, M., Yeung, J. C.et al (2012). 'Experience with the first 50 ex vivo lung perfusions in clinical transplantation'. The Journal of thoracic and cardiovascular surgery , 144 (5), 1200-6.
60. Munshi, L., Keshavjee, S.& Cypel, M. (2013). 'Donor management and lung preservation for lung transplantation'. The Lancet Respiratory Medicine , 1 (4), 318-
28.
61. Sanchez, P. G., Bittle, G. J.et al (2012). 'State of art: clinical ex vivo lung perfusion: rationale, current status, and future directions'. The Journal of heart and lung transplantation : the official publication of the International Society for Heart
Transplantation , 31 (4), 339-48.
62. XVIVO Perfusion AB (2014). XPS - XVIVO Perfusion System. Available from: http://www.xvivoperfusion.com/products/normothermic-perfusion/xps-xvivoperfusion-system/ [Accessed 3rd February 2014].
63. Aigner, C., Slama, A.et al (2012). 'Clinical ex vivo lung perfusion--pushing the limits'.
American journal of transplantation : official journal of the American Society of
Transplantation and the American Society of Transplant Surgeons , 12 (7), 1839-47.
64. Zych, B., Popov, A. F.et al (2012). 'Early outcomes of bilateral sequential single lung transplantation after ex-vivo lung evaluation and reconditioning'. The Journal of heart and lung transplantation : the official publication of the International Society for Heart Transplantation , 31 (3), 274-81.
65. Steen, S., Sjoberg, T.et al (2001). 'Transplantation of lungs from a non-heart-beating donor'. Lancet , 357 (9259), 825-9.
New and emerging organ perfusion systems: July 2014 59
66. Vivoline Medical AB (2013). Vivoline LS1. Available from: http://www.vivoline.se/en/clinical/ [Accessed 26th February 2014].
67. Wallinder, A., Ricksten, S. E.et al (2012). 'Transplantation of initially rejected donor lungs after ex vivo lung perfusion'. The Journal of thoracic and cardiovascular surgery , 144 (5), 1222-8.
68. Hopkins, P. M., Chambers, D. C.et al. Australia’s Experience with Ex-Vivo Lung
Perfusion of Highly Marginal Donors. The International Society for Heart and Lung
Transplantation; Montreal, Canada: Journal of Heart and Lung Transplantation; 2013. p. S154-S.
69. Warnecke, G., Moradiellos, J.et al (2012). 'Normothermic perfusion of donor lungs for preservation and assessment with the Organ Care System Lung before bilateral transplantation: A pilot study of 12 patients'. The Lancet , 380 (9856), 1851-8.
70. TransMedics, I. (2014). OCS™ LUNG. Available from: http://www.transmedics.com/wt/page/ocslungintro_med [Accessed 3rd February
2014].
71. Warnecke, G., Weigmann, B.et al. The inspire international lung trial with the organ care system technology (OCS). International Society for Heart and Lung
Transplantation; Montreal, Canada: Journal of Heart and Lung Transplantation; 2013. p. S16.
72. Schlegel, A., Rougemont, O.et al (2013). 'Protective mechanisms of end-ischemic cold machine perfusion in DCD liver grafts'. Journal of hepatology , 58 (2), 278-86.
73. Dutkowski, P., Schlegel, A.et al (2013). 'HOPE for Human Liver Grafts obtained from
Donors after Cardiac Death'. Journal of hepatology .
74. Guarrera, J. V., Henry, S. D.et al (2010). 'Hypothermic machine preservation in human liver transplantation: the first clinical series'. American journal of transplantation : official journal of the American Society of Transplantation and the
American Society of Transplant Surgeons , 10 (2), 372-81.
75. Dutkowski, P., Schlegel, A. A.et al. First results on end-ischemic hypothermic oxygenated machine perfusion (HOPE) of human liver grafts donated after cardiac arrest. 19th Annual International Congress of the International Liver Transplantation
Society; Sydney, Australia: Liver Transplantation; 2013. p. S108-S9.
76. Organ Assist (2014). HOPE for liver. Available from: http://www.hopeliver.com/technology/ [Accessed 4th February 2014].
77. DiMaio, J. M., Morse, M.et al. Donor hearts not offered or rejected for transplantation - A lost opportunity? International Society for Heart and Lung
Transplantation; Montreal, Canada: Journal of Heart and Lung Transplantation; 2013. p. S156.
78. Suchetka, D. 2012), "'Heart in a box' invention allows transplant hearts to remain outside the body for 12 hours." Clevelandcom, Northeast Ohio Media Group LLC,
Cleveland, Ohio. Available from: http://www.cleveland.com/healthfit/index.ssf/2012/08/heart_in_a_box_invention_t o_ex.html
[Accessed 3rd February 2014].
79. Cobert, M. L., Peltz, M.et al. Maintenance of Human Heart Oxidative Metabolism after 12 Hour Perfusion Preservation. International Society for Heart and Lung
New and emerging organ perfusion systems: July 2014 60
Transplantation; Paris, France: Journal of Heart and Lung Transplantation; 2009. p.
Page S126.
80. Paragonix Technologies Inc (2013). Sherpa Perfusion™ Cardiac Transport System.
Available from: http://paragonixtechnologies.com/?page_id=31 [Accessed 24th
January 2014].
81. Bunegin, L., Tolstykh, G. P.et al (2013). 'Oxygen consumption during oxygenated hypothermic perfusion as a measure of donor organ viability'. ASAIO journal
(American Society for Artificial Internal Organs : 1992) , 59 (4), 427-32.
New and emerging organ perfusion systems: July 2014 61
Appendix 1
Report for Clinical Access and Re‐Design Unit (CARU) for the New Technology Funding and
Evaluation Program (NTFEP), Queensland Health.
An overview of the ex-vivo lung perfusion technology (EVLP) that was acquired in October
2011 as a result of funding from the Queensland Policy and Advisory Committee for New
Technology.
Purpose and Objectives
The objective of EVLP is to recondition non-viable or marginal donor lungs to enhance overall numbers of lung transplant operations in Queensland each year and directly save lives. The conventional approach to organ donation currently involves out dated preservation techniques with the lungs cooled after harvesting which inhibits their metabolic and cellular functions and poses risk of further injury. Donor lungs are then transported back to the transplant hospital fully inflated with this hyperinflation during transfer adding further insult to an already fragile organ. The Vivoline® lung perfusion system is able to keep a pair of human lungs slowly breathing inside a fibreglass dome attached to a standard ventilator pump and filters. The lungs are maintained at normal body temperature of 36‐37⁰C and perfused with a combination of nutrients, proteins and oxygen.
The organs are kept alive in that machine developed by Vivolife for up to 12 hours while both physicians and surgeons assess function and initiate appropriate therapeutic manoeuvres. This enables normothermic ex-vivo evaluation of donor organs to be performed.
New and emerging organ perfusion systems: February 2014 62
Sterile chamber
Connection for ventilator
Oxygenator
Sampling ports
Extracorporeal pump
Figure 18 The Vivoline ® Lung Perfusion System
The Vivoline® system allows for an unprecedented period up to 12 hours of observation and treatment of marginal donated lungs once removed from the deceased to assess and improve function prior to transplantation. It is estimated that since 1989‐2011 there have been 848 potential lung donors in Queensland of which 460 or 54 per cent have not resulted in transplantation. Common reasons for organs not being utilised for transplantation include poor gas exchange, infection, age of the donor, trauma to the organ and logistical concerns.
With the Vivoline® ex-vivo system, organs are retrieved in the usual manner and then transferred to a protective transparent bubble like chamber in theatre 11 at The Prince
Charles Hospital, ventilated and perfused with an acellular solution called Steen solution whilst gas exchange is assessed. The temperature is incrementally increased until it reaches
37⁰C over approximately 30 minutes. Various therapeutic manoeuvres can be performed whilst regularly evaluating lung function with key indicators including oxygenation, airway pressure and lung compliance. Therapeutic manoeuvres consist of recruitment manoeuvres on the ventilator, airway toilet with bronchoscopy, administration of antibiotics and careful titration of pulmonary flow to avoid injury to the lung parenchyma.
The overall aims of EVLP are to:
1.
Minimise ischaemia reperfusion injury by improving solutions used for extracorporeal preservation of organs and tissues;
2.
Extend the safe extracorporeal preservation time for organs prior to transplantation; and
New and emerging organ perfusion systems: February 2014 63
3.
Increase organ availability and transplantation success rates by reassessing and optimising function of injured donor lungs that otherwise would not be used prior to acquisition of this technology.
Figure 19 Donor lungs connected to the
Vivoline® circuit
Population Need
The intended donor organs for application of this EVLP technology have been lung donors with potentially reversible pathology that may be improved with ex-vivo resuscitation.
Guidelines for ex-vivo donor lung eligibility criteria were as follows:
Last donor PaO2 < or equal to 300 mm Hg on the FiO2 of 100 per cent MPEEP of 5;
Poor lung compliance or PEEP dependent donor lungs in the absence of mechanical trauma or significant structural lung disease;
Donor lungs with acceptable gas exchange but evidence of pneumonia, persistent purulent secretion on bronchoscopy or minor structural lung lesions – including localised bullous emphysema or focal nodularity requiring frozen section or definitive resection for histopathological assessment;
Lungs from donors aged > 45 years with a projected ischaemic time in excess of 6 hours (typically lung donors in Darwin or Perth);
Donors with potentially unfavourable parameters including disseminated intravascular coagulation, massive transfusion requirement (guide > or equal to 10 units of packed red blood cells), prolonged mechanical ventilation or pulmonary oedema detected on CXR, bronchoscopy or palpation of lungs; or
Recipients who have a predicted or actual difficult explant in order to limit impact of lengthy ischaemic time.
New and emerging organ perfusion systems: February 2014 64
Contraindications to ex-vivo lung perfusion include those lung donors where there is irreversible pathology or the presence of pre‐existing structural lung disease. It was estimated with the original submission that there would be a net increase per year of 6‐9 lung transplants. In Queensland a total of 8 referrals have been made for ex-vivo lung perfusion resuscitation since November 2011 to May 2013 inclusive. Six of 8 attempts at
EVLP perfusion resulted in clinical transplants resulting in a net increase of approximately 20 per cent in lung transplant numbers for the State of Queensland per year. The overall conversion rate to clinical transplantation from the time of referral is therefore six of eight cases or 75 per cent which was our target rate for clinical transplantation. The net increase in lung transplant numbers has also resulted from an increase in the donors per million of population in Queensland over the last 3‐4 years following the establishment of the
National Tissue Authority. There has been a dramatic reduction in mortality on the waiting list for lung transplantation with the advent of an increased donation rate and acquisition of
EVLP technology.
Guidelines for donor lung criteria for transplant suitability after EVLP include:
PaO2 >300 mmHg measured on FiO2 1.0 at two consecutive time points within the 4 hour maximum period of XVIVO perfusion.
Stability or improvement of other lung function parameters during XVIVO including pulmonary vascular resistance, compliance and airway pressures.
Achieving full flow in the circuit (70ml/kg/min) at normal pulmonary artery pressures
– ie low resistance (target PVR <500 dynes).
Normal collapse test (if performed, remember to first reduce flow to avoid tracheal oedema).
Surgeon clinically satisfied with lung evaluation.
The Technology
As stated above EVLP consists of a sterile chamber, a heating reservoir, closed circuits, temperature probes and pressure catheters along with a monitoring interface and external connections to a mechanical ventilator and a complex gas mixture of nitrogen and carbon dioxide. The marginal donated lung is placed in the sterile chamber and covered with a clear fibreglass dome. The initial temperature of lungs placed on the circuit is approximately 15⁰ and they are connected accordingly to their respective circuits including a pulmonary artery and tracheal connection. The temperature of the circuit is slowly increased with an open circuit perfusion of red blood cells mixed with Steen solution. Steen solution contains human serum albumin providing above normal oncotic pressure to prevent interstitial oedema. In addition, Steen solution contains dextran which is a mild oxygen scavenger which coats and protects endothelium from subsequent excessive leucocyte interaction and thrombogenesis. The electrolyte composition of the solution resembles the extracellular fluid with a low potassium content to reduce free radical generation and avoid vascular
New and emerging organ perfusion systems: February 2014 65
spasm under normothermic conditions. The temperature of the perfusate is slowly increased to normothermia or 36⁰C to restore normal cellular repair systems and metabolic pathways. At 32⁰C the donor lung is ventilated gently with a mechanical ventilator and once the reconditioning phase is complete the oxygen supply to the oxygenator is discontinued.
The donor lung is then ventilated with 100 per cent oxygen purely from the mechanical ventilator and arterial blood gases are sampled from the circuit to assess the level of oxygen or PaO2 emanating from the donor lung. Donor organs are inspected for any abnormalities whilst on the Vivoline® perfusion system and a range of parameters evaluated to assess their physiological function. This includes a continuous measurement of airway pressure, flow within the circuit, temperature recording and pulmonary vascular resistance. Lung compliance is also measured by way of recruitment manoeuvres performed whilst the lungs are ventilated.
Implementation of EVLP technology required the collaboration between perfusionists, anaesthetists, cardiac surgeons and transplant physicians. Six staff members from The
Prince Charles Hospital campus travelled to the University of Lund outside Copenhagen in order to undergo training in the ex-vivo perfusion technique. This was under the direction of
Professor Stig Steen from the University of Lund who first published a case report of success with EVLP technology in 2001. There are no comparator technologies with reference to exvivo lung perfusion. A number of centres around the world are contributing to a database of
EVLP outcomes including hospitals in Vienna Austria, Madrid Spain, Harefield UK, Newcastle
UK, Lund Sweden, Toronto Canada and Sal Paulo Brazil. It is estimated that approximately
120 lung transplants worldwide have been performed using the EVLP system and this number is increasing exponentially. There are now widespread and emerging case series of
EVLP that confirm it is safe and effective in donor organ evaluation and resuscitation. There is an ongoing clinical trial based in Europe, Australia, the US and Canada which is evaluating donor organs resuscitated with EVLP perfusion versus standard cold storage preservation
(the INSPIRE trial). The Toronto group under the leadership of Professor Shaf Keshavjee have published their data on outcome for the Toronto program over a 12 month period of evaluation. In the final analysis, 16 EVLP transplants were compared to 86 standard transplants with comparable 30 day mortality, need for ECMO, mean gas exchange in the first 12 hours post operatively, incidence of primary graft failure, ICU and hospital length of stay. There is emerging data that the incidence of primary graft failure is a major contributor to ICU length of stay post lung transplant and that this dramatically reduced with EVLP reconditioning. The reason for this is likely that EVLP dramatically reduces neurogenic pulmonary oedema in donated lungs and this leads to improved gas exchange in the early post-transplant period in the recipient. In summary, EVLP has now been acquired by numerous transplant programs around the world with The Prince Charles Hospital being the ninth hospital based transplant program to incorporate this technology into donor organ evaluation.
New and emerging organ perfusion systems: February 2014 66
Strategic Alignment
The Queensland Health Strategic Plan 2012‐2016 is a core planning document that strives to obtain quality health care that Queenslanders value. The EVLP system is aligned with the priorities and activities within Queensland Health by enabling a net increase in lung transplant numbers for the State of Queensland thereby improving health care to those patients afflicted with chronic lung disease. With an acceptance rate for clinical transplantation using EVLP target of 75 per cent we have proven that EVLP is both affordable and sustainable in terms of being incorporated into routine clinical assessment of marginal donor lungs. Initiatives from the National Tissue Authority has contributed to an increase organ donor rate per million of population from 2007‐2013 by approximately 50 per cent. For example, in the State of Queensland organ donor rates have increased from 10 per million to over 15 per million in this short timeframe. The addition of EVLP technology results in a higher proportion of lung donors being accepted as being suitable for clinical transplantation and has resulted in a net increase in lung transplant procedures. Last year was the first full calendar year that EVLP technology was available and we had a record year of lung transplant numbers totalling 26 for 2012. Already this year in 2013 there has been
18 transplants and we are on track to have yet another record year in lung transplantation.
EVLP has enabled our regional and rural patients awaiting lung transplant to remain in their home town, as donor organs can be placed on the system whilst recipients are travelling to
Prince Charles Hospital. In addition, the majority of EVLP transplants have occurred during normal business hours thereby reducing medical and nursing fatigue, as organs are placed onto the system in Cooling Phase for up to 12 hours of extended preservation.
Training
In terms of the training involved a total of six staff members – one anaesthetist, one perfusionist, two transplant physicians and two cardiac surgeons attended a training workshop just outside of Lund in Sweden for three days in August 2011. Following our attendance at the workshop a broader educational workshop was rolled out for additional
TPCH staff members who were unable to attend the workshop in Sweden. A total of over 10 perfusionists, one cardiac surgeon, two transplant physicians and six transplant retrieval staff were orientated to the EVLP system upon our return from the workshop. We were in a position to accept referrals of marginal donated lungs in October 2011 and shortly thereafter in November 2011 received our first referral for ex-vivo lung perfusion. Between
November 2011 and May 2013 a total of eight referrals have been received with six leading to clinical transplantation, an overall acceptance rate of 75 per cent.
Evaluation Design
A research project titled “Prospective Audit of Lung Transplant Outcomes After Different
Modes of Clinical Lung Donation – Traditional Brainstem Death, Donation after Cardiac
New and emerging organ perfusion systems: February 2014 67
Death and ex-vivo Lung Perfusion of Marginal Lungs” was lodged with the Human Resources and Ethics Committee in August 2011. The key performance indicators of EVLP included the following:
The primary outcome evaluated for the research study was recipient mortality at 30 days post-transplant.
Secondary outcome measures were as follows:
Incidence of primary lung graft dysfunction at 24 and 72 hours post-transplant;
ICU length of stay and time to hospital discharge;
day 7 ventilator or extracorporeal membrane oxygenator status (ECMO);
recipient mortality at 12 months;
bronchiolitis obliterans syndrome incidence at years 1, 2 and 5;
percentage of marginal lungs resuscitated using EVLP proceeding to lung transplantation;
parameters of pulmonary vascular resistance, lung compliance and pO2 of EVLP lungs during the Evaluation phase on the circuit;
significant clinical episodes of acute allograft rejection and infection (bacterial, fungal, viral or other);
demographic data of donor and recipient;
incidence of airway complications; and
organ retrieval parameters including cold ischaemic and warm ischaemic time.
A prospective database was developed by Associate Professor Peter Hopkins and maintained accordingly following each referral for EVLP. The results of the EVLP trial have been subjected to International peer review by way of presentation at the International
Society of Heart and Lung Transplant Annual Conference meeting Montreal, Canada April
21‐24 2013.
Results
A number of organisational and logistical challenges were experienced following the introduction of EVLP technology at TPCH. These issues were addressed essentially at the outset following careful consultation with members of the EVLP team, theatre staff and pharmacy personnel. The first issue was in reference to where the technology would reside.
A designated area in a theatre has been set aside for EVLP transplant evaluation. There is no clinical case load that impacts upon EVLP being undertaken in this theatre currently at TPCH
Campus. The next barrier was in reference to obtaining a medical grade gas mixture of 93 per cent nitrogen and seven per cent carbon dioxide. This was eventually manufactured by
BOC Medical of a sufficient standard to be recommended for use with human tissue. With reference to staff training we were able to internally run a workshop to educate other relevant staff members to the EVLP system and this responsibility was left with those who
New and emerging organ perfusion systems: February 2014 68
attended the original workshop in Sweden. The ordering process for consumables did prove somewhat cumbersome for the first 12 months. Ordering consumables is now straight forward and time efficient via a Vivolife company representative based in Melbourne,
Australia.
The net activity of EVLP has consisted of eight referrals over the last 18 months with a net increase in six lung transplant operations. It is anticipated that there would be a net increase in the order of 20‐25 per cent in transplant numbers for Queensland as a result of acquiring this new technology. Last year 26 transplants were performed in Queensland and four of these were the direct result of EVLP resuscitation of highly marginal donor lungs. This represents a net increase of 15 per cent and is approaching that net 20‐25 per cent target.
We are confident that with the increasing experience that is being developed as a result of our EVLP use, referrals will continue to be made and almost certainly increase towards the number first predicted with the new technology submission.
In terms of the outcome measures as detailed in the original submission, we have directly compared the outcome of a total of 35 lung transplant operations performed in Queensland from October 2011 to March 2013. During this evaluation period six were ex-vivo transplants and 29 standard donations from a total of 79 solid organ donors (an overall procurement rate of 44per cent). All ex-vivo lungs met at least two marginal criteria with a mean oxygen blood gas in the donor of 189 +/‐ 96 (range 117‐331). Two lungs referred for
EVLP during this evaluation period were deemed unsuitable despite four hours of reconditioning due to either persistent parenchymal oedema or evolution of pulmonary infarction respectively. Please see below tables which outline important ex-vivo donor demographics and outcome along with comparison of EVLP to standard transplantation.
Table 15 Donor characteristics of n=6 EVLP donor lungs
New and emerging organ perfusion systems: February 2014 69
The salient findings are that of the six ex-vivo transplants performed during this evaluation period the net 30 day mortality is 0 per cent for ex-vivo transplants along with 0 per cent for need for prolonged ventilation or ECMO support. The incidence of primary graft failure has been 17 per cent in ex-vivo lungs compared with 17 per cent for standard transplantation.
There have been no airway complications within the ex-vivo transplant group and a markedly lower acute rejection rate. The mean ICU and hospital length of stay are
equivalent to standard transplantation. Table 18 summarises the transplant times for ex-
vivo resuscitated lungs for our first 6 cases. One can see that the total ischaemic time for exvivo lungs in general is well beyond 8-hours and this therefore exceeds the traditional criteria of lung ischaemic time of less than 6‐8 hours. The ability to perfuse the lung at normothermia enables one to extend the time before organs are placed into the recipient and this is reflected in the table. Our first recipient was able to reside in her home town of
Mackay (despite a distance of 1000 kilometres from TPCH) as the donor lungs remained stable on the ex-vivo system. In summary, no specific adverse events in the 6 ex-vivo recipients have been detected to date. In terms of costs per procedure there are two main areas of costs associated with EVLP. The first is the lung chamber disposable kit which averages $12,445 per unit and the second, Steen solution at $3,000 per case. In addition to the consumables there is staff employment and over time if outside normal rostered hours, requiring one cardiac surgeon, one physician, one anaesthetist and one perfusionist for approximately 3‐4 hours each.
Table 16 Outcome data of EVLP recipients
Table 17 Comparison ex-vivo lung to standard transplantation
New and emerging organ perfusion systems: February 2014 70
Table 18 Transplant times for ex-vivo resuscitated lungs
In terms of continuation of this technology the Queensland Lung Transplant Service would consider this technology now part of our standard practice given the success of this pilot program. We are confident that marginal lung donors which we would otherwise reject can often now be referred for EVLP resuscitation and reconditioning. Our results indicate in this early assessment that the outcomes of our first 6 cases are at least equivalent and in many respects superior to standard transplantation. Given the reduced mortality we have experienced on the waiting list and the net increase in transplant numbers we believe the technology has been cost effective in providing greater access to lifesaving transplantation for Queenslanders with end stage respiratory failure. The Prince Charles Hospital is the only facility in Australia with the EVLP system and will continue to advocate for other transplant programs across the nation to adopt this technology.
Figure 20 An example of lungs not utilised for transplant post-EVLP showing pulmonary infarcts and persistent lower lobe oedema
Conclusions and Recommendations
The Queensland Lung Transplant Service would strongly recommend to Queensland Health and the Queensland Policy and Advisory Committee for New Technology that ex-vivo lung perfusion is now incorporated into standard clinical practice and reserved for those lung donor referrals considered to be of high risk or marginal in nature. The Director of the
New and emerging organ perfusion systems: February 2014 71
Queensland Lung Transplant Service will continue to prospectively evaluate EVLP outcomes according to the original Ethics submission and compare these outcome measures with standard organ transplantation. The Prince Charles Hospital transplant program will contribute to an international database which is being established by the International
Society of Heart and Lung Transplantation to evaluate EVLP lung transplant outcomes. The machine and service agreement are in place with any subsequent advances in technology automatically being acquired by the Queensland Lung Transplant Service as a result of the original agreement signed with Vivolife Medical. The one area requiring ongoing funding is the consumables consisting of the lung chamber disposable kit and Steen solution which is approximately $15,445 per case referred for EVLP resuscitation. Currently, ordering of consumables is occurring from operational funding with the approval of the Metro North
Executive. Given the reduced mortality on the waiting list, reduced time waiting for donor organ allocation and net increase in transplant numbers for those with respiratory failure we believe that it is both economically viable and fiscally responsible to continue with exvivo resuscitation.
New and emerging organ perfusion systems: February 2014 72