Physical Therapy Clinical Note Form for CH and BD Update.xlsx
advertisement

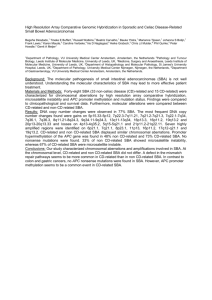
Physical Therapy Clinical Note Pt Name/#: Significant Subjective Observations: Subunit: Date: HOMEBOUND STATUS ‐ Mark all that apply 6 ‐ Bed‐bound 7 ‐ Wheelchair bound 8 ‐ Needs assistance with equipment 9 ‐ Other (specify) ______________________________________ 1 ‐ Limited ambulation ________ ft. 2 ‐ Unsteady gait/poor balance 3 ‐ SOB with minimal exertion 4 ‐ Mental confusion 5 ‐ Fear of, or refuses, to leave home ASSESSMENT ‐ Report significant findings to subunit and document contact below BP: __________ P: ______ R:______ (before rx)/BP: __________ P: ______ R:______ (after rx) Vital signs Location: Intensity (0‐10) _______________________ Pain Pain Intervention Mental status Unchanged Changed (specify) YES NO NA (Report significant changes & document contact below) Diabetes: Any s/s of hypo/hyperglycemia? Diabetes: Does patient have foot ulcers? CHF: Any edema, weight gain, SOB? Skin Integrity: Any redness/breakdown/pressure areas? Medications review: List any new medications Falls: Any falls since last visit? Assessment Notes: CARE COORDINATION Yes Location No If Yes, Who Re: MX Maximum assist KEY: IN Independent SBA Stand by assistance TD Total dependence MI Minimal assistance N/A Not applicable MO Moderate assistance Mark specific activity/activities performed in the following interventions. If no interventions provided in a section, mark entire section as NA. MOBILITY/FUNCTIONAL INTERVENTIONS N/A (No Interventions provided) BED MOBILITY Roll (left to right) IN SBA MI Roll (right to left) IN SBA MI IN SBA MI Sit to supine Supine to sit IN SBA MI Assessment: MO MO MO MO MX MX MX MX TD TD TD TD HBS116‐srw Pt Name/#: Subunit: BALANCE N/A (No Interventions provided) Static sitting IN SBA MI Static standing IN SBA MI Dynamic sitting IN SBA MI Dynamic standing IN SBA MI Assessment: TRANSFERS N/A (No Interventions provided) IN SBA MI Sit to stand Stand to sit IN SBA MI Bed to chair/wheelchair IN SBA MI Chair/wheelchair to bed IN SBA MI MI Bed to commode IN SBA Shower/tub IN SBA MI Toilet IN SBA MI Floor (Up/Down) IN SBA MI Into car IN SBA MI IN SBA MI Out of car Adaptive Equipment Required: Assessment: Date: MO MO MO MO MX MX MX MX TD TD TD TD MO MO MO MO MO MO MO MO MO MO MX MX MX MX MX MX MX MX MX MX TD TD TD TD TD TD TD TD TD TD GAIT TRAINING N/A (No Interventions provided) Weight Bearing Status __________________Gait Distance _________________________ Level Surface IN SBA MI MO MX TD Uneven Surface IN SBA MI MO MX TD Outdoor surfaces IN SBA MI MO MX TD Step/stairs IN SBA MI MO MX TD Device: Cane (SPC) Quad cane Gait Deficits None Initiating gait Stopping Steppage Shuffling Assessment: Wheeled walker Walker Crutches Other (specify): Cadence Posture Balance Scissoring Turning Hip stability Festinating Circumducting FALL PREVENTION INTERVENTIONS Fall Risk Assessment No Compliance with Fall Precautions Assessment: Yes Yes TUG _____Tinetti No N/A Step length Ataxic Trendelenburg Antalgic Other: _____________________ HBS116‐srw Pt Name/#: Subunit: Date: THERAPEUTIC EXERCISE N/A (No Interventions provided) Passive Active Assistive Active Resistive Specific Exercise(s)/Assessment: Objective ROM/Strength Measurements: WHEELCHAIR MOBILITY Interventions/Assessment: N/A (No Interventions provided) HOME PROGRAM: Instructions provided to Instructions provided/response Patient Caregiver SKILLED INTERVENTIONS TO BE PROVIDED NEXT VISIT: SUPERVISORY VISIT N/A PTA Present Not Present If assistant not present, date contacted re POC CARE COORDINATION Yes No If Yes, Who Re: DISCHARGE VISIT Yes No (If yes, complete PT Discharge Below) Status at time of referral Care provided Goal status at D/C Disposition at D/C Functional Scores at D/C M1830 M1850 M1860 Signatures: Patient/Caregiver Therapist HBS116‐srw