REPORT
The Enrollment Strategic
Assessment
Findings from an Assessment of Colorado's
Eligibility and Enrollment Systems
March 2011
1
Enrollment Strategic Assessment
HealthCoverage
Table of Contents
Section 1: Introduction......................................................................................................................................................................................4
Section 2: The Impact of Federal Reform................................................................................................................................................9
Section 3: Understanding Colorado’s Current Position................................................................................................................. 14
Section 4: Enrollment Strategic Assessment Strategic Options............................................................................................... 20
2
Enrollment Strategic Assessment
About This Report
The Colorado Health Foundation’s vision is to make Colorado the healthiest state in the nation. Key to achieving
this vision is ensuring that all Coloradans have adequate and affordable health coverage.
Reform is dramatically changing health care in Colorado and throughout the country. Along with making health
insurance available to more Coloradans through Medicaid and Child Health Plan Plus (CHP+), new policies will
transform the ways in which individuals will connect with public and private health insurance.
Though reform presents an unprecedented opportunity to provide coverage for the uninsured and underinsured,
it also presents challenges. Eligibility and enrollment systems in Colorado are already straining to meet demand.
And despite intense efforts by state and local governments and advocacy groups, tens of thousands of Coloradans
who are eligible for public insurance programs still are not enrolled.
The implementation of the Affordable Care Act will increase demands on eligibility and enrollment systems.
According to the Colorado Health Institute, 214,000 Coloradans who are currently uninsured will become
eligible for Medicaid or CHP+. At the same time, an estimated 328,000 individuals will be newly covered through
individual and employer-sponsored insurance. Many Coloradans will enroll in coverage through a health insurance
exchange—a critical component of the ACA that provides consumers with an easy-to-use, web-based marketplace
for obtaining health insurance that meets essential benefit standards. The exchange also will help individuals and
employers obtain subsidies or tax credits to defray the costs of health coverage
To better understand how the state can improve and streamline its current eligibility and enrollment systems and
processes, and meet future demands, the Colorado Health Foundation funded the Enrollment Strategic Assessment
(ESA) project. This document summarizes the key findings of the project. The report begins with an overview of
current eligibility and enrollment issues facing Colorado. The ESA project team examined current efforts at the state
and local levels as well as best practices from other states to identify strategic options for short- and long-term
investments, analyze projected returns on those investments and identify potential funding sources.
Moving forward on these issues will help build efficient and sustainable eligibility and enrollment systems that reduce
costs, expand access to coverage, improve customer service and align strategic planning and operational efforts to
enroll Coloradans in health coverage programs as well as social service programs for which they might be eligible.
The Colorado Health Foundation would like to thank the many people who contributed their time, expertise
and perspective to this project. Rebound Solutions Consulting Corporation and a team of subject matter experts
conducted the assessment. An advisory committee made up of representatives of Colorado's Department of Health
Care Policy and Financing, the Office of Information Technology, county leadership, the Governor’s Policy Office,
the Colorado Department of Human Services, Covering Kids and Families and the Colorado Health Foundation met
regularly throughout the project. A series of stakeholder workshops also produced important ideas and feedback.
We thank you for your valuable input on the project and look forward to working with you on this important issue.
Anne Warhover, President and CEO
The Colorado Health Foundation
3
Enrollment Strategic Assessment
Section 1: Introduction
State and federal health reforms require essential, sustainable changes to Colorado’s eligibility and enrollment
systems for health coverage programs. Current eligibility and enrollment systems and processes in Colorado are
straining to meet demand. Despite intense efforts by state and local governments and advocacy organizations,
tens of thousands of Coloradans are eligible for public insurance programs but are not enrolled. State and federal
reforms will bring about significant changes, including dramatic increases in the number of people eligible for
coverage, entirely new programs and systems, and a transformation in eligibility and enrollment requirements.
With state and local budgets under intense pressure, it is critical to realize as much efficiency as possible and
to leverage all available sources of funding, including federal funding and private support. Promising practices
have been identified in other states and some Colorado counties; additionally, recently released federal guidance
provides a long-term vision for transforming eligibility and enrollment.
Impact of the Affordable Care Act
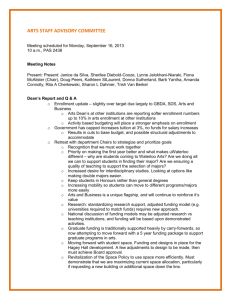
The Colorado Health Institute estimates that as a result of state and national health reform, 214,000 currently
uninsured Coloradans will be newly eligible for Medicaid or the Child Health Plan Plus (CHP+) program. Additionally,
328,000 individuals will be newly covered through individual and employer-sponsored insurance, and many of
these will enroll in coverage through the health insurance exchange. (See Figure 1.1.) The exchange is a web-based,
self-service marketplace for obtaining health care coverage including Medicaid and CHP+ programs. Additionally,
through the Patient Protection and Affordable Care Act (ACA) and subsequent guidance, the federal government
has established a new vision for eligibility and enrollment in health programs that is vastly different from what
exists in Colorado today.
The federal vision calls for systems that are client-centric, easy-to-use and web-based, with a self-service application
to provide users with a real-time eligibility determination. Additionally, enrollment must be seamless between
the health insurance exchange and Medicaid. Clients who seek to enroll in the exchange must first be screened
for Medicaid eligibility. Conversely, clients who apply for but are not eligible for Medicaid must be screened for
possible financial subsidies (as provided by the ACA) through the exchange. These changes will result in a better
client experience as well as efficiencies and financial savings for the system as a whole.
4
Enrollment Strategic Assessment
1
Figure 1.1: Impact of ACA
Estimates of how currently uninsured Coloradans will be covered after implementation of state
and national health reform.
10,000
adults
Uninsured before HR implementation
800,000
Uninsured after HR implementation
258,000
10,000
children
Insured after HR implementation
Medicaid/CHP+
214,000
Individual Purchase
153,000
Employer Sponsored Insurance
175,000
Source: Colorado Household Survey Issue Brief: Uninsured Coloradans: Who will be newly covered under health care reform?
Who will remain uninsured? Colorado Health Institute, January 2011.
Project Background
The Colorado Health Foundation funded the Enrollment Strategic Assessment (ESA) project to provide a
comprehensive view of Colorado’s current enrollment capabilities and identify potential strategic options that
could improve the foundational readiness to support these changes.
Several vendors were contracted to conduct portions of this assessment. Rebound Solutions Consulting
Corporation led the project. The following vendors contributed to the production of this report: The North
Highland Company, Deloitte Consulting, Infolink Consulting, Kone Consulting, National Academy for State Health
Policy and the Maxive Corporation. The participation of a particular vendor in this report does not constitute such
vendor's corroboration of the report as a whole.
This document provides a summary of the ESA. Specifically it includes:
••
••
••
••
5
An overview of the impact from the ACA.
A summary view of current enrollment issues facing Colorado.
Strategic options for investment (short and long term).
A summary of projected returns on these investments as well as funding sources.
Enrollment Strategic Assessment
Objective of the ESA
The ESA is timely and invaluable when considering options for modernizing Colorado’s current enrollment systems.
New federal guidance and resources for states’ information technology (IT) system development have been issued
to support states in achieving more streamlined and robust eligibility and enrollment functions. Colorado must
respond quickly to plan for the new system capacity thresholds required to address:
•• Significant increases in the number of people eligible for public insurance programs.
•• Integration requirements for a single streamlined and automated eligibility and enrollment process
between health insurance exchanges and Medicaid.
•• Revamping of eligibility rules and interfaces between health-related programs and agencies.
The overriding objective of this assessment is to understand how the state can streamline and improve its eligibility
and enrollment system and processes. The following critical questions were addressed:
••
••
••
••
••
••
What is the vision for an effective eligibility determination and enrollment system in Colorado?
What are the strategic investments with the highest return?
What are the short-term improvements and how do these align to the longer term reforms?
Can the current infrastructure scale and meet future demands and needs?
What are other state/federal leading practices that can be used in Colorado?
How does national reform influence and impact the longer term strategy?
ESA Outcomes
The project team identified and presented a wide range of options that could improve enrollment in Colorado. The
objectivity of the team and the mission to identify and evaluate options across the spectrum were critical to an
unbiased and effective assessment. This assessment resulted in thoroughly evaluated options for consideration by
state leadership. The option outcomes desired from this assessment are outlined below and summarized in Table 1.1:
1. While the assessment identifies short-term objectives, the primary focus is on the longer term options available
to Colorado to help ensure it is making wise investments given the changing federal landscape. This results in
options for policy leaders that identify:
••
••
••
••
••
••
Leading practices from other states.
Requirements established under new federal law.
Strategic concepts for leveraging national efforts within Colorado’s landscape.
Options for improving the existing system capabilities.
Viability of streamlined approaches for certain populations and programs.
Methods and concepts to implement valid options.
2. Many initiatives and programs currently under way are designed to improve enrollment. This assessment
validates and provides additional options to improve the chances for these initiatives to be deployed.
6
Enrollment Strategic Assessment
3. Critical business systems such as the Colorado Benefits Management System (CBMS), Medicaid Management
Information System (MMIS), the health insurance exchange and other business systems interact with the
eligibility and enrollment landscape. This assessment considers the bigger picture of the IT systems that affect
eligibility and enrollment.
4. The assessment provides options to improve the governance of the existing infrastructure and identifies ways
to improve the ability of the state to implement initiatives, investments and programs.
5. Working with key state, advocacy, county and national policymakers; technology experts; and other vital
stakeholders, the assessment captures wide-ranging input to assess the viability of every option produced.
ESA Questions and Findings
Table 1.1: Key ESA Questions and Findings
Key Question
ESA Findings
What is the vision for
an effective eligibility
determination and
enrollment system
in Colorado?
•• Colorado needs to improve the eligibility and enrollment systems (people,
process and technology components).
•• There are dramatic new federal functional and technical requirements (and
resources to support them) for eligibility and enrollment systems.
•• New eligibility and enrollment operations must support a “culture of
coverage”—everyone who is eligible is enrolled in a health insurance plan
ranging from full subsidy to no subsidy.
•• New technology means web-based, self-service user interface; real-time
eligibility determination and enrollment; automated verification; and
seamless integration across the health insurance exchange and medical and
human service programs.
What are the strategic
investments with the
highest return?
Within the key areas identified for improvement, the following are areas where
near- and mid-term improvements (called options) are possible and would yield
high impact:
••
••
••
••
••
••
••
••
Enterprise governance.
Administrative renewal processes.
Fraud reporting.
Rules engine upgrade.
MMIS claims.
Management interface improvements.
Improving and automating income and citizenship verification.
Client services business intelligence solution.
Additionally, longer term implementation of the exchange will provide a major
financial return for Colorado.
7
Enrollment Strategic Assessment
Table 1.1 (continued): Key ESA Questions and Findings
Key Question
ESA Findings
What are the short-term
improvements and how
do these align to the
longer term reforms?
Also included in the ESA options were areas where immediate investments
(starting this year) could provide high functional and financial return.
Improvements in these areas would dovetail seamlessly into the strategic
investments mentioned above. These areas include:
••
••
••
••
••
Client support clearinghouse.
Administrative renewal processes.
Improving and automating income and citizenship verification.
Learning academy.
Means-tested enrollment: Supplemental Nutritional Assistance Program
(SNAP) to Medicaid.
•• CBMS capacity upgrades.
Can the current
infrastructure scale and
meet future demands
and needs?
Based upon the ESA capacity assessment, CBMS requires upgrades to the
database servers. Other technical components are sufficient to manage the
current and near-term projected system loads. However, current infrastructure
does not meet future federal technical requirements.
What are other state/
federal leading practices
that can be used
in Colorado?
Several states have effectively implemented options that can be leveraged in
Colorado. These options include:
How does national reform
influence and impact the
longer term strategy?
8
••
••
••
••
••
••
••
Client support clearinghouse.
Administrative renewal processes.
Learning academy.
Streamlined income and citizenship verification.
Client services business intelligence solution.
Fraud reporting.
Means-tested enrollment: SNAP to Medicaid.
The longer term strategy identified in the ESA is based upon the implementation
of the health insurance exchange and other ACA components. For example, realtime enrollment and verification, self-directed web interface and interoperable
service-oriented architecture are reflective of federal guidance.
Enrollment Strategic Assessment
Section 2: The Impact of Federal Reform
National reform provides the foundational principles for the eligibility determination and enrollment systems of the
future. The major policy provisions under federal law establish a fundamental new paradigm under which states
will administer health insurance and eligibility and enrollment systems. Since ACA enactment, federal guidance
now establishes a set of policy, technology and procedural requirements that states need to consider.
Major policy provisions impact both insurance coverage and the health care delivery system. These provisions include:
•• Expansion of publicly subsidized coverage available under Medicaid and the Children’s Health Insurance
Program (CHIP) and via new tax subsidies for purchasing private coverage by low- and moderate-income
individuals.
•• Implementation of the health insurance exchange for making health coverage available to both individuals
and employers and providing real-time consumer-mediated eligibility and enrollment in health coverage.
•• Provisions to ensure real-time, automated, best-of-breed consumer experience in applying and being enrolled
in appropriate insurance coverage across a continuum of Medicaid, CHIP and private insurance products,
including the administration of low-income subsidies.
•• Provisions for enhanced health care delivery system performance based on quality and value, including
empowerment of accountable care organizations, payment reforms and other delivery system innovations.
Federal requirements and related guidance require states to address five key components for enhancing health
systems. Each is outlined in Figure 2.1 below.
Figure 2.1: ACA: System Reform Components
Culture of Coverage
Seamless access public-private
Collaborative Governance
HIE—Insurance—Medicaid
Cross Agency/Sector
Leadership & Managements
Client Centered
Easy navigation
Technology
Advanced Systems
Standardization
Automation
Business Models/Operations
Streamlined rules, functions,
shared services
This represents a major paradigm shift for states in managing eligibility and enrollment. The ACA calls for explicit
new system supports focused on streamlining processes for individuals obtaining coverage regardless of income
and employment status. With obvious impact for states and statewide eligibility and enrollment systems, these
changes include a continuum of policy and business process requirements enabled by emerging new technologies
and IT infrastructure.
9
Enrollment Strategic Assessment
General Guidance for Health Insurance Exchange and Medicaid IT Systems
In early November 2010, the Office of Consumer Information and Insurance Oversight (OCIIO) and the Centers for
Medicare & Medicaid Services (CMS) jointly issued a Notice of Proposed Federal Rulemaking and Federal Guidance
for Exchange and Medicaid Information Technology (IT) Systems (Guidance). The Guidance is intended for states
as they design, implement and operate technology and systems that support health reform implementation
across exchanges, Medicaid/CHIP coverage expansions and improvements, and in the administration of tax credits
and cost sharing. These standards are considered to set a new bar for efforts undertaken by states under health
insurance exchange grants, Medicaid health information technology (HIT) programs, Medicaid matching funds and
other cooperative agreement programs. According to OCIIO and CMS spokespersons, these standards will continue
to be expanded and enhanced on an iterative basis to articulate the evolving refinement of focus on achieving
broad interoperability across health care, human services, and eligibility and enrollment systems.
Ongoing Supports—Federal and State Partnership
While OCIIO and CMS intend to set a clear bar for states, they also intend to allow flexibility in how states will
migrate from current to future capacity and to provide supports to accelerate rapid learning and knowledge
transfer across states:
•• As states submit plans and resource requests for review, they will be expected to articulate a migration
pathway to meet ACA coverage, eligibility and enrollment objectives by 2015.
•• Early Adopter Grants to build exchange capabilities were recently awarded to the following entities1:
»» Kansas
»» Maryland
»» New York
»» Oklahoma
»» Oregon
»» Wisconsin
»» A consortium of New England states led by the University of Massachusetts Medical School
The Notice of Proposed Rulemaking provides yet additional direction for how guidance and resources will be
provided to support development of states’ IT and eligibility and enrollment infrastructure in response to ACA:
•• Adding to provisions already implemented in response to the Health Information Technology for
Economic and Clinical Health (HITECH) Act, ACA will make available enhanced Medicaid matching funds
(90 percent/10 percent) for Medicaid IT implementation—including eligibility and enrollment—through
December 31, 2015, followed by a 75 percent match rate for maintenance.
•• States must demonstrate seamless coordination/interoperability with health information exchange/public
health/Medicaid/insurance exchanges.
•• States should pursue modular/flexible approaches to system development to leverage IT development,
including integrating a Medicaid Information Technology Architecture roadmap and business rules across
the continuum of programs that are machine-readable.
•• States’ current stages of readiness and development are considered in setting deadlines for meeting the
OCIIO/CMS IT standards. States newly launching efforts are required to immediately use the IT guidance.
Projects under way are given a 12-month transition period. Those states in a steady-state are given a
36-month period in which to transition to new IT standards.
1 http://www.ihealthbeat.org/articles/2011/2/16/hhs-awards-early-innovator-grants-for-insurance-exchanges.aspx#ixzz1HurAISvA.
10
Enrollment Strategic Assessment
There are important Medicaid eligibility provisions that require states’ consideration. These include expanding income
eligibility to 133 percent of the federal poverty level (FPL)2 for all individuals and using a streamlined eligibility test that
includes the Modified Adjusted Gross Income (MAGI) test, which will enable states to receive increased federal match for
newly eligible beneficiaries. As states prepare for these and other eligibility transformations and work to align their existing
eligibility and claims systems to meet the increased need, technology and data have become extremely important.
Ensure a Client-Centered Approach
The ACA calls for states to provide a customer-friendly, client-centered approach to enroll and retain individuals in
the appropriate coverage—Medicaid, CHIP or health insurance exchange. To facilitate this goal, the ACA contains
provisions to streamline both eligibility and enrollment processes at the state level. Exchanges will be empowered
to make Medicaid and CHIP eligibility determinations, and Medicaid agencies will be able to make tax subsidy
determinations for private exchange coverage.
The streamlined enrollment process facilitated by the ACA simplifies enrollment in multiple ways. A single application
will be offered for Medicaid, CHIP and the exchange subsidy; enrollment and renewal will be determined through one
process for all of the health coverage programs; and a minimum documentation standard will require individuals to
provide additional documentation only if their application information contains inconsistencies with electronic data.
Clients must be able to apply for services through many different channels, including new Internet portals, in person,
by mail and by phone. In addition, a “no wrong door” policy will ensure that multiple state agencies and the state
exchanges will have the capacity to make an eligibility determination. The ACA will also expand state authority to
enroll individuals using presumptive eligibility.
Health Insurance Exchange
A health insurance exchange will play a new role in a statewide health insurance marketplace to make a range of
insurance plans available to all consumers (from Medicaid to private insurance). One function of the exchange will
be to provide a consumer-facing web portal for “one-stop,” real-time eligibility and enrollment functions, allowing
applicants to seamlessly identify available services, complete initial screening and enrollment checks, obtain electronic
verification of information from outside sources, process eligibility determinations, and store and reuse eligibility
information.
The ACA requires states to create exchange programs that will:
•• Develop streamlined, integrated application forms, processes and systems to support “no wrong door”
(i.e., phone, paper and online channels).
•• Align business processes, systems and branding strategy to support desired approach for targeting
subsidized and unsubsidized populations.
•• Integrate processes to enable screening, choice and coordination between Medicaid/CHIP and the
exchange.
•• Align policy, process and systems to support common health assessment, health plan selection and
premium management for exchange and Medicaid/CHIP.
•• Perform cost/benefit analysis to determine feasibility of creating a basic health plan.
2 A standard income disregard of 5 percent of income will effectively bring the upper limit to 138 percent FPL.
11
Enrollment Strategic Assessment
Figure 2.2 describes the federal government’s expectations about the basic use case of an exchange. It is important
to note that under the ACA, the exchange is obligated to ensure that a first step in eligibility and enrollment
determinations is screening for Medicaid and CHIP eligibility. Therefore, the exchange entity creates a new and
inherently collaborative relationship with the Medicaid agency and potentially other agencies also in the chain of
shared eligibility and enrollment processes.
Figure 2.2: Base Use Case of Health Insurance Exchange3
Medicaid MAGI, MA, Exchange, State systems
2
1
Initial Screening:
Applicant provides basic
demographic info
Check Current
Enrollment:
Check other systems for
existing coverage; first
match using single identifier,
probabilistic formula, or
other method; then obtain
enrollment info
3
Obtain Verification Info:
Electronically verify identity,
residency, citizenship,
household size, income, etc.
IEVS
VR
IRS
4b
4a
Enrollment
Notification
to Portal
DHS
Portal
makes
eligibility
decision
Portal
sends
eligibility
packet to
program
Program
makes
eligibility
decision
4
Determine Eligibility:
Method will depend on
system capabilities
5
Send eligibility info
to other programs
(human services, etc.)
6
Send enrollment
information to plans
3 U.S. Department of Health and Human Services 2010.
12
Enrollment Strategic Assessment
DMV
Key ACA Implementation Dates
As illustrated in Figure 2.3, there are a significant number of milestones for ACA implementation. As states prepare to launch health insurance exchanges and
expand their Medicaid programs by January 1, 2014, they must be aware of a number of significant milestones for health care reform implementation.
Figure 2.3: ACA Implementation Timelines4
2010
2011
2012
2013
Medical malpractice
demo grants awarded
Eliminate lifetime
limits and restrict
annual limits
Begin new Medicaid
state options for
additional coverage
Prohibit denial of
coverage to children
with pre-existing
conditions
Extend dependent
coverage to age 26
Within 90 days:
Create temporary
reinsurance program
& high risk insurance
pool
Begin state HIE & HIT
implementation and
planning grants
Begin quality
reporting/financial
disclosure
Develop National
Quality Improvement
Strategy
Medicaid State
Balancing Incentive
Program for enhanced
federal matching
payments
Creation of
Medicaid state plan
option permitting
designating health
homes
Creation of Medicaid
demonstration
projects to pay
bundled payments for
episodes of care with
hospitalizations
Begin multi-year
Administrative
Simplification phase in
Begin annual fee on
Pharmacy sector
Creation of CO-OPs
Begin mandatory use
of HIPAA version 5010
Begin mandatory use
of ICD-10 codes
Establish Medical
Community First
Choice Option
2015
Reduction of Medicaid
Disproportionate
Share Hospitals
allotments
Medicaid newly eligible
enrollment ends
Launch American
Health Benefit
Exchanges and Small
Business Health
Options Program
Exchanges
Permit states to merge
individual and small
group markets
Expand Medicaid
eligibility to 133% FPL:
Maintain CHIP
Phase-in tax penalties
for both individuals
and employers
Begin CMS
acceptance of Version
5010 claims
Allow states to create
a Basic Health Plan
for certain uninsured
with incomes between
133–200% FPL
State and State
Designated Entities
must match HIE grant
awards
Provide premium
credits/subsidies
to those between
133–400% FPL
Meaningful Use
incentives for EHR
begin
4 Deloitte Consulting: Timelines for ACA Implementation.
13
Begin increase in
Medicaid primary
care rates with 100%
federal funding
2014
Enrollment Strategic Assessment
2016
2017 and on
Begin increase in
private health insurance
company fees
Temporary reinsurance
& high risk pool ends
Reduction in Medicare
payments for hospital
acquired conditions
by 1%
Primary care payment
bonus ends
Meaningful Use
penalties begin
Permit states to form
health care choice
compacts and allow
insurers to sell in any
participating state
Close Medicare donut
hole by 2020
Begin excise tax on
high cost health
insurance plans in 2018
Meaningful Use
incentives end in 2021
Section 3: Understanding Colorado’s Current Position
The current eligibility determination and enrollment system is the critical front door for clients across Colorado.
While there is a combination of unprecedented client demand combined with significant budgetary pressures,
more applications are being processed than any other time in Colorado history. However, Colorado is not where
it could and should be in serving clients efficiently and effectively. There are major opportunities to increase
efficiencies, reduce costs, improve services, positively retool county caseworker roles and improve health
system performance and outcomes. To capitalize on enhanced federal funds and timelines, Colorado needs to
immediately organize planning and implementation efforts to align funding, people and programs. Other states
are implementing successful solutions which Colorado can build upon to transform current operational conditions.
Colorado has been a leader in designing new policies and programs to expand services to new populations over
the past four years. Colorado has been able to design innovative legislation such as the Health Care Affordability
Act (as authorized by House Bill 09-1293) and has been successful in obtaining federal financial support for
automating and improving the eligibility and enrollment systems. The foundation in Colorado has been firmly
established for transforming these systems through highly effective governance and operational execution.
However, the state faces significant barriers to improving operations:
•• Financial and budgetary constraints from the current economic environment. Colorado, like many states,
will be making significant cuts in the next fiscal year. These cuts have a direct impact on the state’s ability
to fund projects, necessary operational staff and other operational components.
•• Colorado’s centralized benefits management system, which is shared between the Colorado Department
of Health Care Policy and Financing (HCPF) and the Colorado Department of Human Services (CDHS). The
current architecture does not allow for flexibility in making individual program changes. A human services
program change can significantly impact a health program change. Changes to this rigid architecture will
be required to allow more aggressive and necessary changes to the programs in the near term.
•• Geographically distributed client base (across 64 counties). This creates challenges in outreach to inform
clients about programs as well as expand coverage.
•• Dilution of key resources by a significant number of strategic programs and demands. Better strategic
alignment of these priorities is critical for more effective implementation. This is especially relevant with the
impact from national health care reform efforts.
•• Ineffective internal state business processes such as procurement and contracting. These systems delay
implementation of key initiatives and programs.
14
Enrollment Strategic Assessment
The current systems in Colorado were evaluated against the following core components, which are outlined in
Table 3.1.
Table 3.1: Current State Core Component Summary Findings
Component
Summary Findings
Governance
•• The existing governance model is not optimal for the scale and complexity
required to manage and steer the required transformation.
•• The current structure does not meet federal guidelines for
effective coordination.
•• There is a gap around strategic planning and operational delivery.
•• Roles and responsibilities are not clearly defined or qualified.
Funding Alignment
•• While the state is securing federal and private funding, it is not being
managed from an enterprise position.
•• The state is not minimizing operational funding silos.
Strategic Alignment
•• The state is not effectively aligning strategic plans across the enterprise
and reducing silo operational programs.
Client Service and
Outreach
••
••
••
••
Self-Service
•• There is no option for self-service application submission.
•• Self-service only exists for screening and for clients who wish to check
their existing benefits.
Seamless Process
•• Processes are not efficient or consistent.
•• The process is not seamless between health and human service programs.
Effective Use of Data
•• Capacity and capabilities are limited for performance
management reporting.
•• Best practices for reporting are not being implemented.
Real-Time Enrollment
•• There is no real-time enrollment function today.
Automated Verification
•• Citizenship verification is being piloted but is not automated.
Effective Caseworker
Support
•• Caseworkers are not being effectively trained.
•• Infrastructure, curriculum and other core elements for effective training are
not being provided by the state.
15
Enrollment Strategic Assessment
Client support is neither consistent nor cost-effective.
Clients struggle to find relevant information and support.
Outreach efforts are not effectively coordinated.
Client correspondence is a major problem as it remains unclear
and confusing.
The components are further expanded in Figure 3.1, which subjectively illustrates the view of core operational functions.
Figure 3.1: Current State Findings
Highly Effective
Components
Governance
Funding Alignment
Target
Strategic Alignment
Client Support/Outreach
Effectiveness
Self Service
F
S
ES
I
E
R
Interoperability
G
Effective Use of Data
Real Time Enrollment
Automated Verification
SS
C
SP
A
Ineffective and
Not Aligned
Seamless Process
Alignment to Federal Reform
Effective Caseworker
Support
Aligned
This illustration indicates that there is work to be done in the future to move Colorado forward to address federal
reform. Even without federal reform efforts, moving forward on these components will reduce costs, improve
customer service, expand access and benefits, and align strategic planning and operational efforts.
16
Enrollment Strategic Assessment
The Client Perspective
Irrespective of federal reform mandates, the client perspective of the systems is still not optimal despite recent
improvements as outlined in Table 3.2.
Table 3.2: Key Client Concerns and Progress in the Past 2 Years
Key Client Concerns
Progress in Past 2 Years
There is a lack of clear and concise
information about programs for which
clients may be eligible.
•• The web portal (PEAK) was released in October 2009 and
provides a basic summary of programs and can be used for
eligibility screening.
•• Modernization efforts for the CHP+ program have improved
Interactive Voice Response (IVR) capabilities for customer
support.
Clients are generally confused by
notices and correspondence.
•• Despite changes made to reduce the volume and amount
of client correspondence, clients report that information
remains confusing.
Clients experience difficulty in
effectively locating resources to help
with the application process.
•• PEAK was released in October 2009 and provides a basic
summary of programs and can be used for eligibility screening.
•• Modernization efforts for the CHP+ program have improved
IVR capabilities for customer support.
There are too many disparities in the
process. Clients get different answers
depending upon who they ask.
•• The state started the business process learning collaborative to
improve business operations.
•• CBMS Web (formerly IDE) will be deployed to streamline the
client interface for eligibility caseworkers.
Clients are unable to apply for benefits
through the web.
•• PEAK Phase 2 is scheduled for a limited release in April 2011
to allow online application submission.
Clients do not receive benefits in a
timely fashion.
•• The state started the learning collaborative to improve
business processes.
•• CBMS Web will be deployed to streamline the client interface
for eligibility caseworkers.
•• The state is testing electronic verification interface with Vital
Statistics.
17
Enrollment Strategic Assessment
Table 3.2 (continued): Key Client Concerns and Progress in the Past 2 Years
Key Client Concerns
Progress in Past 2 Years
Clients struggle to find expert
resources for assistance.
•• The state started the learning collaborative to improve
business processes.
•• CBMS Web will be deployed to streamline the client interface
for eligibility caseworkers.
•• Modernization efforts for the CHP+ program have improved
IVR capabilities for customer support.
Program redetermination requirements,
timelines and processes are not
clearly understood.
•• There have been efforts to align program
redetermination cycles.
Clients don’t like to make multiple
trips or visit multiple locations to
complete the process.
•• The state is testing electronic verification interface
with Vital Statistics.
•• PEAK Phase 2 is scheduled for a limited release in
April 2011 to allow online application submission.
In addition to these client sentiments, statistics on performance also cause concern. Across the human services and
health programs, Colorado continues to trail other states. Conclusively, despite efforts to improve health enrollment
services and processes for clients, Colorado must further:
1. Reduce the paper-based bureaucratic process for clients. The dependency upon a paper-driven application
process is not a client-centric approach.
2 Focus more on streamlined enrollment and other means to reduce client over-the-counter or paper-based
application submissions.
3. Modernize other access points, not simply CHP+, in terms of providing better customer service,
access and support.
4. Improve client correspondence. There should be a concerted effort to move clients to electronic
benefit management through PEAK.
5. Launch PEAK Phase 2 to offer both clients and advocacy groups the ability to submit applications via the web.
6. Consolidate and modernize client support channels. In addition to phone lines, better support over
the web is required.
7. Continue efforts to improve the eligibility caseworker user interface to reduce application processing times.
8. Leverage resources, such as electronic document management, across the enterprise.
9. Automate key interfaces, such as vital statistics, to improve citizen and identity verification processes.
10. Continue efforts to streamline and build consistent business processes across the eligibility determination sites.
18
Enrollment Strategic Assessment
Although ACA amplifies the need for improvement, the crux of the need arises from Colorado’s eligibility
determination and enrollment systems and processes that are costly, inefficient, unwieldy to maintain and lagging
enhanced practices already proven by other states. There are opportunities to achieve significant cost savings,
improve application processing speeds and improve client support functions while also providing Colorado with
a much greater chance of successfully implementing the federally required components.
The intersection of the current Colorado eligibility and enrollment ecosystem and the impending national reforms
gives rise to a much-needed transformation—one characterized by a steep climb over a very short duration,
as shown in Figure 3.2. This ascent will require a sophisticated approach that allows leaders and teams to work
together effectively to best leverage limited financial and human capital resources.
Figure 3.2: Colorado’s Transformation through 2014
Colorado in 2014
•• Coordinated Governance
•• Electronic Submission—Minimal Paper Apps
•• High Self Service = Lower Cost/Transaction
Colorado in 2011
•• Operational Silos
•• Paper Based
•• High Cost/Transaction
•• Caseworker Centric
•• Manual Verification
•• Legacy Architecture
•• Inadequate Reporting
•• Caseworkers Focused on Higher Value Functions
•• Automated/Real Time Verification
•• Service Oriented Architecture
•• Robust Business Intelligence
•• Federally Compliant
•• Processing Times Measured in Minutes
•• Full Self-Service
•• Electronic Correspondence
•• Federal Compliance Issues
•• Processing Times
•• Measured in Weeks
•• No Self-Service
•• Cumbersome Correspondence
2011
2014
Although the climb is steep, the potential benefits are substantial as outlined in the next section. The ESA provides
both short- and long-term options for moving Colorado forward to realize these benefits.
19
Enrollment Strategic Assessment
Section 4: ESA Strategic Options
Strategic options were identified from multiple sources including evaluation of other states, review of federal directives and guidance, interviews with key
stakeholders in Colorado and assessment of current projects by ESA subject-matter experts. These options are described in the table below.
Table 4.1: Strategic Option Descriptions
Strategic Option
Description
Enterprise Governance Model
This option provides an outline of the governance model with a set of core features to build a reliable structure and processes for formal
collaboration and shared decision making across the gamut of infrastructure partners. This also outlines the roles and responsibilities
across the enterprise with the intent to maximize financial, human capital and system assets. This includes an overview of current
governance structures in Colorado and areas for changing the governance model. Specifically this option calls for:
••
••
••
Implementing an agency-neutral leader to ensure development of coordinated legislative policy collaborative outputs across
agencies, gathering stakeholder input and creating transparency.
Increasing the capabilities and role of the HIT coordinator to provide the necessary operational and technical leadership.
Creating an operations council responsible for implementation of the strategic plans and policies required for improving eligibility
and enrollment capabilities.
This option was created after reviewing other successful state governance models.
20
Enhanced Strategic Planning
This option outlines how to improve prioritization of initiatives and projects across and beyond the eligibility and enrollment landscape,
taking into account the broader strategic context for health reform implementation. This option is designed to prevent a silo approach
to projects and programs and ensure better enterprise coordination of financial and human capital assets. This option primarily focuses
on improving the operational capacity of the departments through the hiring of a chief operating officer who can provide operational
leadership by determining priorities and effectively executing programs.
Streamlining Procurement
This option outlines suggestions for improving both procurement and contracting functions within the state. Existing procurement
and contracting could be more effective by implementing key functional improvements. This is not just procurement and contracting
related to CBMS, but applies to MMIS, the future health insurance exchange, MAXIMUS and other related contracts. The current
procedures delay procurement and contracting in a way that hinders functional and technical improvements to core business systems,
rather than preventing unwise investment decisions and increasing stewardship over public funds. These delays impact more than large
system implementations—they also impede business process improvement studies, audits, language translation and other business
services. This option presents concepts that could streamline procurement while ensuring the appropriate level of fiscal controls.
Enrollment Strategic Assessment
Table 4.1 (continued): Strategic Option Descriptions
Strategic Option
Description
Improve Operational
Capacity
This option reviews necessary business functions and core competencies for the state workforce and identified key areas for
improvement—specifically within business analysis and project management. This option focuses on assessing and improving project
management capabilities within the state. The option suggests an organizational assessment of departments against the strategic
planning efforts. It also includes the option of certifying OIT Business Analysis (an effort currently underway) to improve system
development capabilities.
Client Support
Clearinghouse
Functional models of this option exist today in other states and establish a foundational “no wrong door” model for customer access
and support. Through a concerted marketing effort, the goal is to funnel clients to this clearinghouse to reduce the workload on
existing eligibility workers. This will also reduce county website management costs and other costs associated with providing support
and outreach to clients. Specifically, the clearinghouse can be designed to provide the following services:
1. Centralized customer support for clients, providing the following:
a. PEAK web-based customer support, integrated with chat and other on-line customer support functions.
b. Single point of contact / call center management with single toll-free number
c. Standard customer support from 7 am to 8 pm.
d. Ability to direct clients to county and external entities for application processing.
2. Single entity to manage all program-related web content to ensure all web content is accessible and current. Specialized
administrative services, including:
a. Ability to manage administrative renewal processes.
b. Processing pending cases that require citizenship and income verification.
c. Ability to process PEAK inbound cases (overflow) as needed.
3. Marketing and outreach services for clients, advocacy groups and the state. Services would include promotion of new
services and programs, facilitation of client focus groups and client surveys, and general communication services.
4. Centralized communication services for the state and caseworker community—including production of newsletters, outage
communication, events and training opportunities, release updates and other critical information for caseworkers.
21
Enrollment Strategic Assessment
Table 4.1 (continued): Strategic Option Descriptions
Strategic Option
Description
Learning Academy
This option is designed to improve learning systems and training for eligibility caseworkers, clients and other external users (advocacy
groups). The current training delivery for eligibility caseworkers is not highly effective and does not result in the best return on
investment. This option specifically focuses on the training for CBMS and related programs, although other enterprise systems
could benefit from this option as well. The Learning Academy will consolidate training assets with the intention of producing best
practice training solutions across the landscape. This is already being done with the Child Welfare training in Colorado. Counties in
particular have suggested this model as it provides much more effective training, provides certification programs and evaluates the
effectiveness of this training. The Learning Academy could:
1. Increase effectiveness of policy-focused training for eligibility workers.
2. Work with counties to develop training that focuses on new responsibilities beyond traditional data entry and application
processing responsibilities.
3. Design and maintain instructional content and curriculum and Learning Management Systems to ensure curriculum version
control, user registration, user certification, logistical certification and other necessary training support functions.
4. Allow for the collection and sharing of best practice training methods and materials from counties and other sites.
5. Ensure the training environment is secured, has appropriate training data, is updated with the most recent software releases
and has appropriate backup and recovery controls.
6. Deliver and deploy highly effective training through multiple channels, including instructor-led classroom, instructormoderated webinars, self-service webinars and other training methods.
7. Coordinate general professional service offerings for state and county staff. This may include business analysis, quality
assurance, project management and other core competencies.
8. Assess, monitor and maintain training curriculum and the overall effectiveness of training programs.
9. Develop role-based certification mechanisms (assessment) for eligibility workers and master trainers.
10. Deliver self-service training content for clients and advocacy groups for PEAK and other self-service applications.
22
Enrollment Strategic Assessment
Table 4.1 (continued): Strategic Option Descriptions
Strategic Option
Description
Means Tested Enrollment:
SNAP to Medicaid
This option assesses the ability for the state to expedite eligibility determination for public health insurance programs through existing
data from other means-tested programs (in this case, SNAP). Medicaid and CHIP (CHP+ in Colorado) now have the option to borrow
eligibility findings from other programs to determine eligibility and/or conduct renewals. Public Law No. 111-3 (Children’s Health
Insurance Program Reauthorization Act of 2009, or CHIPRA) gives states the option to rely on a finding from another means-tested
program to satisfy one or more eligibility components, even where the other program uses a different budget unit, disregard, deeming,
or other methodology to make its finding. This provision is referred to as Express Lane Eligibility (ELE). The use of existing data from
trusted sources to make eligibility determinations for Medicaid and CHIP is also supported within the ACA.
ELE strategies could help enroll many uninsured children and parents into Medicaid and CHP+. According to data from the 2002 National
Survey of America’s Families, more than two-thirds (71 percent) of uninsured children with family incomes at or below 200 percent of
the FPL live in families that participate in the National School Lunch Program (NSLP); the Special Supplemental Nutrition Program for
Women, Infants, and Children (WIC); or SNAP. Since most states extend Medicaid and CHIP to children with family incomes at or below
200 percent of the FPL, providing health coverage to uninsured children based on their families’ participation in these nutrition programs
could reach most low-income children who qualify for Medicaid or CHIP but are not yet enrolled. Adopting ELE using SNAP eligibility
determinations for Medicaid and CHP+ is a particularly good fit because the programs have similar income, resource, citizenship,
immigration and residency tests and requires similar documentation verification for each criterion. Because SNAP generally has more
stringent rules, most everyone who has been determined eligible for SNAP is likely eligible for, and should be enrolled in, health
insurance.
This option summarizes next steps for implementing SNAP to Medicaid ELE through policy and system changes.
Means-Tested Enrollment:
NSLP to Medicaid/CHP+
This option assesses the ability for the state to expedite eligibility determination through existing data (means-tested). This option
specifically focuses on using NSLP for children receiving free and reduced lunch as a basis to predetermine eligibility for health programs.
As described in the Means-Tested Enrollment: SNAP to Medicaid/CHP+ option, Medicaid and CHIP (CHP+ in Colorado) are now allowed
to borrow eligibility findings from other programs to determine eligibility and/or conduct renewals. Public Law No. 111-3 (Children’s
Health Insurance Program Reauthorization Act of 2009, or CHIPRA) gives states the option to rely on a finding from another means-tested
program to satisfy one or more eligibility components, even where the other program uses a different budget unit, disregard, deeming
or other methodology to make its finding. This is the ELE provision.
While there are potential benefits in using NSLP data to identify uninsured children, implementing ELE is complicated using this data,
as noted by other states, and the difficulty of aggregating data from 178 school districts must be considered. Rather, Colorado should
first focus on implementing ELE from SNAP. As noted in the Means-Tested Enrollment: SNAP to Medicaid/CHP+ option, this could be
implemented fairly easily since data from both SNAP and health coverage programs are housed in CBMS. NSLP should be focused as an
avenue for outreach in the short term and potentially modeled after SNAP ELE in the future.
23
Enrollment Strategic Assessment
Table 4.1 (continued): Strategic Option Descriptions
Strategic Option
Description
Income Verification
This option assesses the ability for the state to expedite eligibility determination for Medicaid and CHP+ through electronic sources
of income verification. This option specifically focuses on using third-party income data with the objective of reducing barriers for
clients and streamlining application and renewal processing requirements for eligibility workers by automating the lengthy process of
gathering needed client documentation.
Specifically, the near-term options are to obtain a gopher system that would improve the management of electronic verification and
streamline the process for staff and clients and to negotiate a statewide contract with the TALX Work Number™ or other similar service to
enhance the availability of electronic income verification. Colorado health programs already have considerable access to data showing
household income. Federal law requires that Medicaid programs and certain other public assistance programs operate the Income
Eligibility Verification System (IEVS), which matches client identity to income data housed by the Internal Revenue Service, the Social
Security Administration (SSA), and quarterly earnings and new hires data that employers report to the Colorado Department of Labor
and Employment.
Administrative Renewal
Administrative renewal is the practice of using sources already available to verify circumstances and renew a client’s enrollment in
Medicaid or CHP+. The Children’s Health Insurance Program Reauthorization Act (CHIPRA) of 2009 explicitly calls for states to utilize
administrative or paperless verification at renewal to help eliminate enrollment roadblocks for eligible children. Administrative renewal
may be performed though ex parte reviews, in which a state uses information available to it through other databases to verify ongoing
eligibility, or through prepopulated renewal forms. With either approach, administrative renewal eliminates the need for a client to
resubmit information already provided at the time of initial enrollment or already available through other programs and databases,
unless there has been a change in circumstances. This option calls for the alignment of program redetermination dates, system changes
and changes to manual processes, all of which could significantly reduce operational costs and improve application processing rates.
Improving and Automating
Citizenship Verification
Improving and automating citizenship verification refers to utilizing state and federal databases to satisfy U.S. citizenship requirements
electronically for a client’s enrollment in Medicaid and CHIP. The Deficit Reduction Act of 2005 required Medicaid clients to provide proof of
U.S. citizenship and identity when enrolling or renewing Medicaid benefits. In Colorado, this translates to a client having to provide a birth
certificate (or other official paper documentation) to the eligibility site to satisfy the U.S. citizenship requirement. Oftentimes this requires a
client to purchase a certified copy of his/her birth certificate, which can be cost-prohibitive for many low-income families.
This option includes automating or improving access to key interfaces such as vital statistics, SSA and Systematic Alien Verification for
Entitlements to enable eligibility caseworkers to confirm documentation. This streamlines the enrollment process and reduces demands
for clients to identify, bring and potentially purchase documentation that exists electronically and free of charge in resident state and
federal databases.
24
Enrollment Strategic Assessment
Table 4.1 (continued): Strategic Option Descriptions
Strategic Option
Description
MAXe Case Management
Interface
This tactical option evaluates how to improve the CBMS interface for the MAXIMUS caseworkers by either extending PEAK/CBMS Web or
by integrating the case management application, MAXe, into CBMS. MAXIMUS is the eligibility modernization vendor that provides case
maintenance for new clients and renewal clients for Medicaid and CHP+ who enter through their doors. MAXIMUS does not provide case
maintenance for combination cases or other human services programs. Currently MAXIMUS is using a customized application, MAXe, for
case management.
When a new client application is received, the application is scanned into MAXe through Optical Character Recognition and Intelligent
Character Recognition technologies. This streamlines the processing as a caseworker does not have to manually enter in the client data
from the application. However, in order for the information to be entered in CBMS, a caseworker must manually enter the data populated
in MAXe into CBMS, resulting in a dual entry process. MAXIMUS estimates that this process takes approximately 25 percent of the total
application processing time and therefore would be a significant process improvement if this manual entry step was eliminated.
This option outlines short-term technical steps that can be taken to eliminate this manual data entry.
Program Separation
This option explores removal or separation of programs within CBMS to improve system performance or program performance for
clients. The option focuses on identification of programs that are not best suited for the centralized eligibility determination or programs
that require additional or specialized functionality. Using a service-oriented architecture, these systems would share data and a common
interface with other public assistance programs. This option does not support an isolation of these programs and systems but rather
more highly integrated systems that better support the existing populations and associated eligibility workers.
The team identified two programs (Adult Protective Services and Long Term Care) that should be considered for separation as they likely
can be better supported by other architectural solutions.
25
MMIS Interface
Improvement
This option explores the feasibility of interface improvements achieved by remedying a specific issue currently preventing effective
interfacing—vanishing “med spans.” The CBMS Medical Eligibility Span (med spans) Interface is intended to provide new and updated
client and case medical benefit eligibility information to MMIS, which uses this information to determine medical services for which
the individual is eligible and processes resulting payments for the services on behalf of clients. MMIS interface improvements must be
considered as current CBMS functionality enables county and MA site workers to change data such that a current existing med span can
be eliminated retroactively without an audit trail or even a record of the original med span. Addressing this issue is critical in terms of
financial cost avoidance and recovery.
New Medical Program
Eligibility and Enrollment
System
This option evaluates the feasibility of implementing a new eligibility and enrollment system for medical programs (CHP+ and Medicaid).
This simplified future state would require system integration between CBMS and the new system. This option outlines benefits
for implementing a new system for Medicaid and CHP+ that will provide more flexibility and capabilities to support the eligibility,
enrollment and verification functions. This would include data conversion activities to ensure client data integrity between both systems.
The state would have to modify existing systems and develop new interfaces to both state and federal systems. This would naturally
include the development of new production and testing environments and would result in a new system to operate in Colorado. This
option assumes CBMS will continue to be used to provide eligibility and enrollment services for human services programs.
Enrollment Strategic Assessment
Table 4.1 (continued): Strategic Option Descriptions
Strategic Option
Description
CBMS Rules Engine
Modernization
This option evaluates the feasibility of implementing a new rules engine architecture that allows more flexibility in CBMS while lowering
development costs for program changes. The CBMS Rules Engine or EDBC subsystem houses the eligibility and benefit calculation rules for
the various assistance programs such as Food Assistance, Colorado Works, Family Medicaid and CHP+, and applies those rules for every case
(and individuals in that case). Clients’ benefits are calculated based on the rules of the each program. The option explored investing in new
rules engine capabilities that provide a more robust and flexible systems architecture.
The ESA team concluded that this is likely a necessary investment, regardless of the state’s long-term architectural decisions regarding
eligibility and enrollment systems.
Consolidated MMIS
Eligibility Determination
The basis for this option is to build CHP+ and Medicaid eligibility determination into the claims management system. HCPF currently
manages a contract to provide automated Medicaid claim processing that is currently managed by ACS which acts as the Medicaid fiscal
agent. This system, the MMIS, operates in a client-server environment with the server operating similarly to a mainframe and providing data
to a decision support system. Currently there is a point-of-sale pharmacy system that also interfaces with the MMIS. HCPF is currently in the
planning stages to upgrade MMIS under a revised contract. It is expected this procurement will start in 2011.
This option concludes that while this option may be possible, there are better ways to implement this type of system functionality without
impacting claims management.
26
Client Services Business
Intelligence Solution
This option explores building a best-of-breed data warehouse for the CBMS system specifically to improve reporting capability and capacity.
This option also provides an opportunity for improving client correspondence within the CBMS system. Client correspondence is nothing
more than a report with specific information within a limited and often confusing format. Currently client correspondence is produced
from within the transactional system. Moving client correspondence pieces to a data warehouse will allow for significant improvements
in formatting and control and decimation of content. Normalization of data with better business intelligence reporting could significantly
improve client correspondence through creation of clear and concise reports. More importantly, this functionality could empower
electronic correspondence or self-service reporting capabilities from within PEAK or the health insurance exchange.
Centralized Business
Intelligence and Analytics
This option explores outsourcing data analytics and reporting capabilities to a third party. This is an extension of the Client Services Business
Intelligence (BI) Solution. A centralized BI solution will serve many stakeholders across the state. Ad hoc, parameterized and static reporting
will allow agencies to create comprehensive views of performance and progress as well as the success of the client across all assistance
programs such as Low Income Energy Assistance Program (LEAP), Colorado Works, NSLP, CDHS’s Food Distribution Program, CHP+ and all
other Health and Human Service (HHS) programs.
Improved Fraud Reporting
Using Predictive Analysis
This option assesses how the state could improve fraud reporting capabilities. This option explores improving the existing reporting system
to proactively detect potential provider fraud activity and provide investigation tools with preaggregated data so cases may turn quickly,
thus reducing the cost of operation and increasing the damages recouped due to fraudulent uses of state funds. This option presents a
solution rooted in the creation of a centralized business intelligence system, provides end-to-end capabilities for detecting and preventing
fraud using a combination of business rules and analysis methods, and leverages report distribution and alerting techniques designed to
identify suspicious activities across the state’s systems.
Enrollment Strategic Assessment
Feasibility Summary
Each option was assessed against multiple factors. Table 4.2 summarizes these key feasibility criteria.
Table 4.2: Option Criteria Definitions
Criteria
Description
and Details
Criteria Definitions
Overall Feasibility
Provides an overall
assessment of the
option in terms of
feasibility
HIGH: The option is feasible and should be considered for
implementation.
MODERATE: The option may have a weaker business case, require
significant investment or be highly complex to implement..
LOW: The option is not feasible. It offers little to no return.
Demonstrated In
Others States
Has this
option been
demonstrated in
other states?
YES: The option has been implemented and used in other states.
Financial Cost
What is the
financial cost
of the option?
NO: The option has not been identified as currently being
used by other states
PARTIAL: States may be implementing something similar
to the proposed option.
VERY HIGH: The option will cost more than $5M.
HIGH: The option will cost more than $1M but less than $5M.
MODERATE: The option will cost less than $1M but
greater than $250K.
LOW: The option will cost less than $250K.
Financial Return
on Investment
Is there a financial
return on
investing on
this option?
STRONG: The option will provide a return up to 150 percent of
the value of the investment.
MODERATE: The option will provide a low financial return
but likely not fully return the investment.
LOW: This option does not include a tangible financial
return on investment.
Overall Benefits
Does the option
provide other
benefits?
HIGH: The option provides five or more tangible, nonfinancial
operational improvements. May include improving client
experience, caseworker capabilities or application processing,
or providing better information. The implementation would
significantly improve the client experience.
MODERATE: The option provides up to three tangible, nonfinancial
operational improvements. May include improving client
experience, caseworker capabilities or application processing, or
providing better information. The implementation would improve
the client experience.
LOW: The option provides only minor operational, nonfinancial
improvements, May include improving client experience, caseworker
capabilities or application processing, or providing better
information. The implementation does not impact the client.
Using these assessment criteria, the option score card outlines the overall feasibility of the options proposed in
the ESA and is shown in Figure 4.1.
27
Enrollment Strategic Assessment
Figure 4.1: Option Feasibility Scoring
Feasibility
Summary
Demonstrated
in Other States
Financial
Cost
Financial
ROI
Enterprise Governance Model
High
Yes
Low
Strong
High
Enhanced Strategic Planning
High
Yes
Low
Strong
High
Streamlining Procurement
High
Yes
Low
Moderate
Low
Improve Operational Capacity
High
Yes
Low
Strong
High
Client Support Clearinghouse
High
Yes
Moderate
Moderate
High
Learning Academy
Moderate
Yes
Moderate
Moderate
High
Means Tested Enrollment: SNAP
Moderate
Yes
Moderate
Moderate
High
Means Tested Enrollment:
National School Lunch Program
Low
Partial
Moderate
Moderate
Moderate
Income Verification
High
Yes
Moderate
Strong
High
Improving and Automating
Citizenship Verification
High
Yes
Moderate
Strong
High
Administrative Renewal
High
Yes
Low
Strong
High
MAXe Case Management
Interface
Moderate
No
Low
Strong
Moderate
Program Separation
Moderate
No
High
Strong
High
MMIS Interface Improvement
Moderate
No
Moderate
Strong
High
New Medical Program Eligibility
and Enrollment System
High
Yes
Very High
Moderate
High
CBMS Rules Engine
Modernization
High
Partial
High
Strong
High
Consolidated MMIS Eligibility
Determination
Low
No
High
Moderate
High
Client Services Business
Intelligence Solution
High
Yes
High
Strong
High
Centralized Business
Intelligence and Analytics
Moderate
No
Very High
Strong
High
Improved Fraud Reporting
using Predictive Analysis
High
Yes
Moderate
Strong
High
Option
28
Enrollment Strategic Assessment
Overall
Benefits
Option Benefits
There are major benefits to implementing the options identified in the ESA; these are summarized in Figure 4.2.
Figure 4.2: Potential Option Benefits
Save Money
Speed Application
Processing
Improve Client Support
Improve Program
Delivery
Significant long-term
savings from digital vs.
paper application
Real-time enrollment
capabilities through
self-service (web)
Clients empowered
through access to
self-service functions
Coordinated decision
making across
departments and
entities
Administrative
cost savings in
correspondence,
application processing
timelines, and reduction
of churn
Automated verification
of income and
citizenship
Consistent support for
clients, caseworkers,
and community-based
organizations
Better availability to
meet federal timelines
Conservative estimates
of annual savings
ranging from $10M to
$25M
Better program
retention rates reducing
churn
Improved training for
caseworkers
Improves coordination
of limited funding
sources and human
capital
Improvements to overall
system processing
capabilities
Clear, concise and
accessible client
correspondence
Clearly defined
authorities will
empower project teams
Improved reporting
capabilities to improve
performance
Better reporting
analytics for policy
makers and leadership
Reduction of key
integration risks across
major systems and
programs.
Change is clearly possible and necessary. Other states have consistently demonstrated that significant
improvements in eligibility and enrollment can be realized with an approach that centers on a robust
accountability and oversight model.
The expected benefits from implementing the needed improvements are substantial and total in excess of an
estimated $20 million in annual cost savings. (See Table 4.2 below for further details on savings, investments
and funding sources.)
29
Enrollment Strategic Assessment
Table 4.3: Summary Benefits, Projected Investment and Funding Sources5 by Track and Option
Option
Functional Benefits
Financial Benefits
Potential
Funding
Source(s)
Projected
Investment
Funding
Timeline
Accountability and Oversight
Enterprise
Governance
Model
•• Improves execution and operational effectiveness.
•• Enhances risk management, accountability and
oversight.
•• Maximizes financial investments and reduces
implementation costs.
•• Results in more effective resource allocation.
•• Optimizes procurement processes.
•• Ensures longer term strategic coordination.
•• Ensures better data integration between core systems.
•• Delivers much more effective communication and
outreach.
•• Allows for better stakeholder involvement and
participation.
•• Provides better evaluation metrics and capabilities.
Effective governance
models can produce
8% to 10% in program
efficiencies.
No new
investment
Provided through
staffing vacancy
and reallocations
N/A
Technical Architecture Planning and Short-Term Operational Improvements
Means-Tested
Enrollment:
SNAP to
Medicaid
•• Expands eligibility to children currently uninsured.
•• Reduces “churn” and pending application work.
Financial benefit not
projected
$50K to $100K
•• CMS 90/10
FFP/MMIS
•• CHIPRA
Performance
Bonus
•• Spring 2011 to 2015.
•• 2010 funds
awarded; annual
redetermination
through 2013.
Income
Verification
•• Allows workers to process cases more quickly.
•• Reduces burden for clients.
•• Reduces pending cases, which is one of the most
common reasons for issues with processing timeliness
and customer service.
$15K to $848K annually
in improving efficiencies
from 3% to 12%.
Variable – $500K
to $1M annual
cost
•• CMS 90/10
FFP/MMIS
•• CHIPRA
Performance
Bonus
•• Administrative
cost savings
•• Spring 2011 to 2015.
•• 2010 funds
awarded; annual
redetermination
through 2013.
•• Ongoing.
5 $19 million CHIPRA performance bonus 2010—available for unrestricted use by the state. CMS-enhanced FFP—available upon rulemaking expected Spring 2011, contingent upon CMS approval of state’s IAPD.
30
Enrollment Strategic Assessment
Table 4.3 (continued): Summary Benefits, Projected Investment and Funding Sources by Track and Option.
Option
Functional Benefits
Projected
Investment
Financial Benefits
Potential
Funding
Source(s)
Funding
Timeline
Technical Architecture Planning and Short-Term Operational Improvements (continued)
Improving and
Automating
Citizenship
Verification
•• Reduces cases pending due to citizenship verification
requirements.
•• Increases speed at which clients are able to receive their
benefits.
•• Reduces administrative time for caseworkers to
process a case.
•• Eliminates need to purchase birth certificate(s) in order
to receive medical assistance benefits.
•• Increases efficiency in the overall enrollment process.
•• Builds the foundation for the future of ELE and the
exchange, which call for a paperless process, including
for citizenship verification.
$157K to $848K annually
in improving efficiencies
from 3% to 12%.
$50K to
$100K for
implementation
•• CMS 90/10
FFP/MMIS.
•• CHIPRA
Performance
Bonus.
•• Administrative
cost savings.
•• Spring 2011 to
2015.
•• Current
plus annual
redetermination.
•• Ongoing.
•• General Fund
for Adult
Protective
Services.
•• Federal/General
Fund for Long
Term Care.
•• July 2011 funding
identified.
•• CMS 90/10
FFP/MMIS.
•• Potentially
realignment
and HRSA
Funding.
•• Administrative
cost savings.
•• Spring 2011 to
2015.
Technical Architecture Planning (additions)
Program
Separation
CBMS Rules
Engine
Modernization
31
•• Adult Protective Services: Allows this program to be
more effectively managed by eligibility caseworkers.
•• Long Term Care: Allows Colorado to meet federal
program requirements. Reduces transactional volumes
from CBMS.
Financial benefit not
projected.
•• Allows faster and more efficient eligibility determination.
•• Provides more flexibility for changes realigning the
workflows.
•• Expedites development and release of any emergency
changes due to changes in the program rules and
regulations.
•• Simplifies application and enhances efficiency of the
rule engine by eliminating unused processes.
Reduction in development
costs expected in the
range of $250K to $500K in
annual savings.
Enrollment Strategic Assessment
$500K for Adult
Protective
Services
$3M to $4M for
Long Term Care
$1.5M to $2M
Table 4.3 (continued): Summary Benefits, Projected Investment and Funding Sources by Track and Option.
Option
Functional Benefits
Financial Benefits
Projected
Investment
Potential
Funding
Source(s)
Funding
Timeline
Technical Architecture Planning (additions continued))
New Medical
Program
Eligibility and
Enrollment
System
•• Provides faster and more efficient eligibility
determination.
•• Allows more flexibility for changes realigning the
workflows in Medicaid and CHP+ programs.
•• Ensures higher chance of integration with external
systems and interfaces.
•• Modernizes core architectural components and
business rule structure.
•• Could be potentially funded through multiple sources.
With real-time integration,
projected to save $1M
in annual development
costs and more than
$10M in operational and
administrative costs.
$35M to $50M
•• CMS 90/10
FFP/MMIS.
•• CHIPRA
Performance
Bonus.
•• Administrative
cost savings.
•• Spring 2011 to
2015.
Consolidated
MMIS Eligibility
Determination
•• Provides faster, more efficient eligibility determination.
•• Eliminates integration issues with the MMIS system.
•• Allows more flexibility for changes realigning the
workflows in Medicaid and CHP+ programs.
•• Ensures higher chance of integration with external
systems and interfaces.
•• Modernizes core architectural components and
business rule structure.
•• Could be potentially funded through multiple sources.
With real-time integration,
projected to save $1M
in annual development
costs and more than
$10M in operational and
administrative costs.
$35M to $50M
•• CMS 90/10
FFP/MMIS.
•• CHIPRA
Performance
Bonus.
•• Administrative
cost savings.
•• Spring 2011 to
2015.
32
Enrollment Strategic Assessment
Table 4.3 (continued): Summary Benefits, Projected Investment and Funding Sources by Track and Option.
Option
Functional Benefits
Financial Benefits
Projected
Investment
Potential
Funding
Source(s)
Funding
Timeline
Short-Term Operational Improvements (additions)
MAXe Case
Management
Interface
•• Improves the speed of transactional processing for
CHP+ applications into CBMS.
Projected at 15% to 20%
case management savings
at $250K in annual savings.
$70K to $150K
•• General Fund
•• July 2011 funding
identified.
Administrative
Renewal
•• Allows for continuous coverage of eligible clients and
reduces the number of eligible clients dropped from
coverage for procedural reasons.
$750K: Client
correspondence
reductions through
reducing the production
and mailing of
redetermination packets.
$50K to $65K
for CBMS
modification
•• CMS 90/10
FFP/MMIS.
•• CHIPRA
Performance
Bonus.
•• Administrative
cost savings.
•• Spring 2011 to
2015.
•• 2010 funds
awarded; annual
redetermination
through 2013.
$1.3M: Administrative
processing—18%
reduction in administrative
time to renew, then
re-enroll a client.
Significant financial
savings are also projected
from providers in claim
processing.
33
Enrollment Strategic Assessment
Table 4.3 (continued): Summary Benefits, Projected Investment and Funding Sources by Track and Option.
Option
Functional Benefits
Financial Benefits
Projected
Investment
Potential
Funding
Source(s)
Funding
Timeline
Short-Term Operational Improvements (additions continued)
Learning
Academy
34
•• Reduces operational costs through improved
application processing time and reduction in processing
errors.
•• Allows a better understanding of policy and program
information.
•• Reduces help desk tickets, work around solutions and
other high-cost process impacts that are largely due to
inadequate training.
•• Reduces county investments to train its eligibility
workers.
•• Allows new caseworkers to be onboarded more
effectively. This would reduce new caseworker turnover
as well as improve the rate for new caseworkers to have
a positive impact.
•• Ensures training content is better maintained, more
accessible and delivered in a more effective manner.
•• Provides self-service training modules for advocacy
groups and clients, which will produce better results for
the PEAK (self-service) application.
Enrollment Strategic Assessment
Estimated to improve
processing metrics by
minimum of 5% or $157K
in annual savings.
Estimated error reduction
also by 5% or savings of
$157K annually.
$250K to $500K
annual cost
can potentially
be funded
by existing
allocations.
•• Provided
through
staffing
vacancy and
reallocations.
•• Could be
funded as a
percentage
of functional
development
costs.
•• Summer 2011
Table 4.3 (continued): Summary Benefits, Projected Investment and Funding Sources by Track and Option.
Option
Functional Benefits
Financial Benefits
Projected
Investment
Potential
Funding
Source(s)
Funding
Timeline
Short-Term Operational Improvements (additions continued)
MMIS Interface
Improvement
•• Reduces processing delays, speeding the
delivery of information.
Cost avoidance will be
achieved as eligibility
workers will no longer
spend time trying to
reconcile data or gather
missing information.
Estimates put this expense
at least at $18K per year.
$350K to $400K
•• CMS 50/50 FFP.
•• CMS 90/10
FFP/MMIS.
•• CHIPRA
Performance
Bonus.
•• Current.
•• Spring 2011
to 2015.
•• Annual
through 2013.
$750K to $1.5M
•• CMS 90/10
FFP/MMIS.
•• Spring 2011
to 2015.
Cost recuperation will be
achieved as the state will
recoup benefits payments
for clients that were
deemed ineligible but
are actually eligible. Cost
recuperation would be on
the order of $5M to $8M in
additional funds per year.
Data Management & Report Planning
Client Services
Business
Intelligence
Solution
35
•• Capitalizes on state-of-the-art solution for reporting and
analysis.
•• Improves client correspondence.
•• Reduces transactional load on core operational systems.
•• Follows state initiatives in enterprise architecture, data
and security management.
Enrollment Strategic Assessment
Expected 10% to 15%
reduction in client
correspondence costs or
$500K annually.
Table 4.3 (continued): Summary Benefits, Projected Investment and Funding Sources by Track and Option.
Option
Functional Benefits
Financial Benefits
Projected
Investment
Potential
Funding
Source(s)
Funding
Timeline
Data Management & Report Planning (continued)
Centralized
Business
Intelligence
and Analytics
Improved
Fraud
Reporting
Using
Predictive
Analysis
36
•• Minimizes demand on state resources, relies on state
resources for business knowledge and direction but
relies on expert services in all aspects of technical
design and development.
•• Capitalizes on state-of-the-art cloud computing for a
flexible information platform.
•• Gathers and integrates data from all data sources over
time.
•• Ties records together—same person, same family
(identity resolution while capable of keeping data
anonymous when necessary).
•• Follows state initiatives in enterprise architecture, data
and security management.
•• Provides data as a service to those who need it.
•• Supports longitudinal analysis, for example, tracking an
individual from K-20 education through human services.
Expected 10% to 15%
reduction in client
correspondence costs or
$500K annually.
•• Allows for reduction of provider fraud and provides the
state with a high return on investment.
Estimate at $15M to
$30M annual return on
preventing and identifying
provider-based fraud.
Enrollment Strategic Assessment
$2M to $4M
•• CMS 90/10
FFP/MMIS.
•• Spring 2011 to
2015.
$1M initial costs;
$200K ongoing
annual licensing
costs
•• CMS 50/50 FFP.
•• CMS 90/10
FFP/MMIS.
•• Current.
•• Spring 2011 to
2015.
Reduction of FTE
associated with reporting
functions, estimated at
$450K in annual savings.
www.ColoradoHealth.org
501 South Cherry Street, Suite 1100 º Denver, Colorado 80246 -1325
TEL: 303.953.3600 º FREE: 877.225.0839
Together, we will make Colorado the healthiest state in the nation.
© 2011 The Colorado Health Foundation. All rights reserved.
The Colorado Health Foundation is proud to be an equal opportunity employer.
37
Enrollment Strategic Assessment