Genetic Testing: Psychological Aspects and Implications

Journal of Consulting and Clinical Psychology
2002, Vol. 70, No. 3, 784 –797
Copyright 2002 by the American Psychological Association, Inc.
0022-006X/02/$5.00
DOI: 10.1037//0022-006X.70.3.784
Genetic Testing: Psychological Aspects and Implications
Caryn Lerman
University of Pennsylvania
Kenneth P. Tercyak
Georgetown University Medical Center
Robert T. Croyle
National Cancer Institute
Heidi Hamann
University of Utah
As the number of genes associated with inherited disease continues to grow, researchers and practitioners in behavioral medicine will encounter complex psychological issues faced by individuals at risk for these diseases. A review of the literature concerning prenatal, carrier, and predictive genetic testing suggests that the severity of psychological risks posed by research-based genetic testing is not great. However, subgroups of individuals with particular psychological traits may be more vulnerable to adverse effects.
Available data do not provide evidence that genetic testing promotes changes in health-related behaviors.
Thus, although there may be less of a role for mental health professionals in the psychological counseling of genetic testing participants, there is a need for research and practice to facilitate health protective behaviors in response to genetic risk information.
The number of inherited disorders and risk factors that can be detected through genetic testing is increasing rapidly, and genetic testing may soon become a common component of routine medical care. Is behavioral medicine ready? For the first time, a sophisticated understanding of gene-environment interactions as manifested in the interactions among an individual’s genetic predispositions, behavior, and environment seems within reach. Rather than diminishing the role of behavioral science, advances in molecular medicine highlight the centrality of behavior both in disease etiology and in the translation of science into practice.
The subset of psychological issues and processes that are most salient within the clinical genetics context has evolved alongside advances in biotechnology. Prenatal testing and carrier testing were among the first services offered, affording an opportunity for individuals to learn whether they had transmitted an altered gene to their offspring. As these tests provided information about the risk to the fetus, the focus of counseling tended to be on reproductive decision making. More recently, genetic testing is being applied to detect personal susceptibility to disease, shifting the focus of counseling to personal risk reduction. The hope is that awareness of genetic risk will enhance informed medical decision making by physicians and patients alike. However, there may also be psychological and social risks of genetic testing that should be considered, regardless of the potential medical benefits provided by testing. It is in this consideration of the entire breadth of the potential costs and benefits that psychologists can play a critical role. Both researchers and clinicians can assist patients, families, physicians, and policymakers as they grapple with the complex task of integrating genetic information into their professional practice and everyday lives.
In this article, we review the behavioral science literature concerning genetic testing in the following three primary domains: prenatal testing, carrier testing, and predictive testing. Although it is impossible to provide an exhaustive review of this vast literature, several studies are described to illustrate issues of relevance to the field of clinical psychology. The greatest attention has been devoted to predictive testing, because this research area is the most active and has generated a relatively greater number of controlled quantitative studies. Within each domain, we consider the following questions, based on available data: (a) What factors have been shown to influence whether a person decides to have a genetic test? (b) What are the psychological and behavioral outcomes of genetic testing? (c) What interventions have been used to enhance the outcomes of testing? The final section of the article considers emerging themes, future research needs, and the implications for training and practice.
Caryn Lerman, Cancer Center, University of Pennsylvania; Robert T.
Croyle, Division of Cancer Control and Population Sciences, National
Cancer Institute, Bethesda, Maryland; Kenneth P. Tercyak, Lombardi
Cancer Center, Georgetown University Medical Center; Heidi Hamann,
Department of Psychology, University of Utah.
Preparation of this article was supported by grants from the National
Cancer Institute and National Human Genome Research Institute, CA/
HG74861 and HG01846.
Correspondence concerning this article should be addressed to Caryn
Lerman, Cancer Center, University of Pennsylvania, 3535 Market Street,
Suite 4100, Philadelphia, Pennsylvania 19104 – 4283. E-mail: clerman@ mail.med.upenn.edu
784
Prenatal Testing
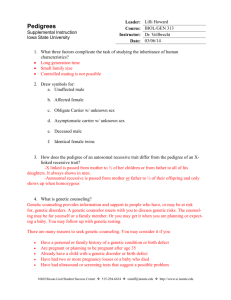
Several procedures are available to obtain prenatal genetic information, with amniocentesis and chorionic villus sampling
(CVS) being the most common and widely used (see Table 1).
Clinical indications for prenatal testing include advanced maternal age (35 and older), family history of a genetic defect or inborn metabolic error, parent or family member known to be a carrier of a genetic anomaly, ethnicity, or membership in a high-risk group
(American Academy of Pediatrics/American College of Obstetricians and Gynecologists, 1997). These procedures may also be recommended for women with abnormal ultrasounds, multiple
SPECIAL ISSUE: GENETIC TESTING
Table 1
Prenatal Diagnostic Test Procedures
Procedure Technique a Sample
Chorionic villus sampling Needle inserted through mother’s abdomen or catheter through
Early amniocentesis cervix
Needle inserted through mother’s
Amniocentesis
Placental biopsy abdomen into amniotic sac
Needle inserted through mother’s abdomen into amniotic sac
Needle inserted through mother’s
Cordocentesis
Fetoscopy with fetal skin biopsy abdomen into placenta
Needle inserted through mother’s abdomen into fetal umbilical vein
Needle inserted through mother’s abdomen, camera used to facilitate biopsy
Chorionic villus
Amniotic fluid and/or amniocytes
Amniotic fluid and/or amniocytes
Placental tissue
Fetal blood
Fetal skin
Gestational age at procedure
(in weeks)
10–12
⬍
15
15–20
⬎
12
⬎
18
⬎
18
Note.
Used by permission of GeneTests: Genetic Testing Resource for republication from the GeneTests Web site (http://www.genetests.org). Copyright 1999 by Children’s Health Care System, Seattle, WA. Further a copying or republication is prohibited.
Ultrasound guided.
785 marker screens, or elevated levels of maternal serum alpha fetoprotein (MSAFP), which is suggestive of chromosomal or neural tube defects (Thompson, McInnes, & Willard, 1991).
The relative benefit of the diagnostic information acquired in this manner is balanced against the risk posed by obtaining it.
Specifically, pregnancy loss rates following amniocentesis are typically around 1:200, though estimates range from 1:100 to
1:300 (Chescheir & Hansen, 1999; Romero, Ghidini, & Santolaya,
1992). Fetal loss rates for CVS for a group of women 35 to 39 years old are estimated to be from 2.6% to 6.3% (Brambati, 1992).
Because of the risk to maternal–fetal health, these forms of prenatal testing are unique among the genetic tests currently available.
Thus, psychological responses to amniocentesis may relate both to concerns about positive test results as well as to the stressprovoking effects of the procedures themselves (Astbury &
Walters, 1979; Marteau, Kidd, et al., 1992).
Decision Making About Prenatal Testing
As the implications of prenatal genetic testing for maternal and fetal health are substantial, comprehension of information about the potential risks and benefits are important aspects of the decision-making process. However, patient knowledge and actual risk figures have generally not been shown to be strong predictors of test use among persons eligible for testing (French, Kurczynski,
Weaver, & Pituch, 1992; Marteau et al., 1991). Rather, perceptions of increased risk (i.e., higher subjective risk estimates) may be a more important determinant of test uptake than actual risk (Marteau et al., 1991; Shiloh & Saxe, 1989). There are many likely reasons for this finding, including that some statistical figures
(e.g., risk ratios) commonly used during genetic counseling are puzzling for many individuals to comprehend (Statham & Green,
1993). Further, perceptions of risk following genetic counseling are also influenced by how information is presented during the session. For example, d’Ydewalle and Evers-Kiebooms (1987) found that knowledge about genetic risk probabilities was influenced by whether information regarding the emotional consequences of testing was presented. Specifically, discussing future childbearing decisions and the potential psychological outcomes of testing led to greater knowledge than if only one, or neither, of these issues had been raised.
Psychological Effects of Prenatal Testing
The potential effects of amniocentesis on short-term disruptions in women’s psychological well-being have been explored by several prospective studies. For example, Astbury and Walters (1979) reported significant reductions in pre- to post-amniocentesis state anxiety scores, though all scores remained within normal limits. In another study, Beeson and Golbus (1979) followed women who were at high risk because of either advanced age or having an affected child during a previous pregnancy. Participants’ anxiety levels were highest prior to amniocentesis and peaked again prior to test-result notification. Women with a previous affected child had more marked elevations in anxiety than women at risk due to advanced age. However, notification of normal test results produced relief to nonclinical anxiety levels in both groups.
Phipps and Zinn (1986a) assessed mood changes in women referred for amniocentesis for maternal age-related concerns and an age-matched control group of women seen for routine obstetric visits. No significant differences were detected between the amniocentesis and control groups on mood or pregnancy attachment measures before testing or after notification (months 3 and 5).
Relatively greater anxiety was found in the amniocentesis group only at month 4; however, reductions on most mood state scales were observed following test result notification. More recent studies suggest that the anxiety that women experience prior to amniocentesis tends to dissipate following successful completion of the procedure (e.g., Tercyak, Johnson, Roberts, & Cruz, 2001).
In an effort to elucidate further the role of age-related risks on women’s anxiety levels, Tabor and Jonsson (1987) examined anxiety levels in younger and older women undergoing amniocen-
786 LERMAN, CROYLE, TERCYAK, AND HAMANN tesis to young women receiving an ultrasound (controls). Although pretest anxiety levels were equivalent for all women, the level of anxiety for younger ( ⬍ 35 years) women (amniocentesis and control groups) significantly decreased from pretest to posttest, and from pretest to 23 weeks. For women over age 35, a significant decrease in anxiety was not seen until 23 weeks (after test results were communicated). Thus, older women experienced relief only after receiving their results, whereas younger women were relieved after having successfully completed the procedure.
Fava et al. (1982, 1983) also evaluated the psychological reactions of high-risk women referred for amniocentesis and a matched control sample of healthy pregnant women who did not receive the procedure. Prior to amniocentesis, women receiving the procedure reported higher levels of hostility and less somatic well-being than did the control group. However, those differences disappeared after the procedure. In addition, anxiety and depression decreased significantly in both groups. Thus, reductions in psychological distress observed among women receiving amniocentesis may reflect normal psychological changes that occur during pregnancy, rather than being a direct effect of testing itself.
Some investigators have also evaluated the relative impact of the various procedures for prenatal testing. Spencer and Cox
(1987) randomized women to either amniocentesis or CVS.
Women in the CVS condition experienced reductions in anxiety and depression (as self-reported on an adjective checklist) earlier than women in the amniocentesis condition. Other researchers have found similar anxiety reductions among CVS and amniocentesis participants (G. E. Robinson et al., 1988; Tunis et al., 1990).
The above studies primarily examined women who had knowledge of their risk of giving birth to a child with a genetic abnormality, for example, women over age 35. For these women, who initiate their pregnancy with some degree of concern, amniocentesis may be reassuring or at least neutral because the vast majority will receive normal results. However, this may not be the case for women who are referred to testing after the discovery of abnormal
MSAFP levels (most of which are false positives), because many of these women initiate their pregnancies unaware of their increased risk. Marteau, Cook, et al. (1992) addressed this question in a study of two groups of women less than 38 years of age: (a) those with initially abnormal MSAFP results who went on to have normal results on subsequent testing and (b) those with initial
MSAFP results within the normal range. Women who received abnormal results were more anxious, held more negative attitudes toward their pregnancies and the baby, and were less certain about their baby’s health than women who received normal results; these effects persisted up to 3 weeks following subsequent normal results. The data are similar to those reported for women aged 38 and older (Marteau et al., 1988). In a similar study, J. O. Robinson,
Hibbard, and Laurence (1984) prospectively examined women at risk for having a baby with a neural tube defect (i.e., anencephaly or spina bifida) and referred them for further testing (ultrasound or amniocentesis). Immediately prior to the amniocentesis, anxiety was greatest, but there was a significant post-result decline to normal levels (see also Tabor & Jonsson, 1987).
A study by Phipps and Zinn (1986b) also indicates that women’s responses to testing may be influenced by their personality or coping style. Among women receiving amniocentesis, those who had information-seeking coping styles had higher levels of anxiety and depression at all timepoints. However, in the control group, coping style was unrelated to psychological distress. Given that more recent work has not reported an effect of coping style on the psychological well-being of women undergoing prenatal testing
(Tercyak et al., 2001), the role of potential moderators merits further study.
Interventions in Prenatal Testing
Intervention research on patient decision making and psychological outcomes in prenatal genetic testing is limited. However, within the field of genetic counseling, a few studies have focused on the most effective ways to communicate risk information and educate patients. For example, d’Ydewalle and Evers-Kiebooms
(1987) demonstrated that persons who used decision-making devices (such as decision trees) to aid them in their evaluation of the risks of prenatal testing tended to reach different conclusions about testing than those not using such a tool. Ormond, Pergament, and
Fine (1996) provided the following one of three educational interventions for expectant mothers presenting for multiple marker serum screening: (a) genetic counselor and physician, (b) pamphlet and physician, and (c) physician only. Patients in the genetic counselor and pamphlet conditions scored significantly higher on posttest scores of knowledge than did women in the physician only condition. With respect to anxiety, all three groups were within normal limits and remained relatively stable throughout; however, the sample sizes in this study were very small.
Summary and Critique of Prenatal Testing Studies
Despite that prenatal testing is widespread, research on decision making is quite limited. Only a few studies have been reported, and these studies tended to rely on patients’ qualitative descriptions about reasons for testing, rather than on validated instruments and hypothesis-driven study designs. Although some of the earlier studies are notable in their use of decision-making theory to guide study methodology (d’Ydewalle & Evers-Kiebooms, 1987), there has been limited attention to this topic in recent years. The available, mostly qualitative, data do suggest that both cognitive factors
(e.g., perceived benefits) and emotional factors (e.g., expected psychological impact of testing, feelings about termination) are integral to the decision-making process.
The literature on the psychological impact of prenatal testing is relatively more informative than that on decision making. Although generally not theory driven per se, many of these studies use validated measures of psychological distress and repeated measures study designs. Whereas earlier studies lacked control groups (Beeson & Golbus, 1979; Astbury & Walters, 1979), most other studies used control groups of women seen for routine visits or for other procedures (e.g., ultrasound). Studies in the literature have tended to focus on the effects of testing in the context of normal results, as abnormal results are relatively rare in the population. Although clinicians should be cognizant of the anticipatory anxiety experienced by patients undergoing testing, these studies provide no evidence for sustained or clinically significant psychological distress. However, subgroups of women who may be more vulnerable to adverse effects of prenatal testing include those with information-seeking coping styles. The absence of significant psychological effects may explain the dearth of intervention studies to improve the outcomes of testing.
Carrier Testing
SPECIAL ISSUE: GENETIC TESTING
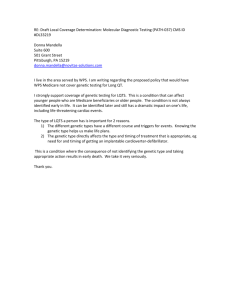
Carrier testing is used to identify gene mutations inherited in an autosomal recessive fashion (i.e., inheritance of two altered gene copies, one from each parent, is required for the offspring to develop the disease). This form of genetic testing is unique because testing takes place in couples or in a two-step fashion, with one member of the couple tested first, followed by the other.
Further, mutation carriers are generally unaffected by the disease themselves, though their offspring may develop the disease
(Thompson et al., 1991; see Table 2).
787 fibrosis, per se), and 2% felt they could not refuse the test (i.e., did not perceive a choice). In a similar study, Levenkron, Loader, and
Rowley (1997) found that 57% of women accepted cystic fibrosis testing. Compared with women who declined testing, test acceptors were more likely to perceive having a child with cystic fibrosis as a more serious health threat, had significantly higher risk perceptions, had more knowledge about cystic fibrosis, and had more favorable attitudes toward abortion of an affected fetus than the decliner individuals.
Decision Making About Carrier Testing
The decision to participate in carrier testing for three relatively common genetic conditions (Tay-Sachs disease, cystic fibrosis, and Gaucher disease; see Table 2 for description) was examined among 1,000 Ashkenazi Jewish patients, 80% of whom were pregnant or partners of pregnant women (Kronn, Jansen, & Ostrer,
1998). In this population, 23% chose testing for Tay-Sachs disease only, 26% elected cystic fibrosis and Gaucher disease carrier testing, and 42% wanted to undergo full testing. In a similar study of Ashkenazi Jewish individuals who had received Tay-Sachs screening, only 3% of persons tested for Tay-Sachs disease declined additional testing for cystic fibrosis and 5% declined testing for Gaucher disease (Eng et al., 1997). In both studies, the diseases in question, their potential severity, and the ability to treat the conditions were all important considerations in the decisionmaking process.
The above studies offered testing to couples primarily at risk for
Tay-Sachs disease because of their ethnic origin. However, factors influencing decision making may be different when testing is nonselect and offered as part of routine medical care. Such was the case in an English study of cystic fibrosis carrier testing conducted by Hartley et al. (1997). Eighty-five percent of the women accepted cystic fibrosis testing. Eighty-one percent reported that their decisions were related to the disease (e.g., to determine their carrier status, to avoid having an affected child), 16% felt that all tests offered during pregnancy were important (regardless of cystic
Psychological Effects of Carrier Testing
In one of the earliest reports of the impact of carrier testing,
Stamatoyannopoulus (1974) studied the implementation of a sickle-cell disease carrier screening program in a community where 23% of the population were gene carriers and about 1% of infants were born with sickle-cell disease. The community’s custom of arranging marriages provided the opportunity to offer counseling aimed at avoiding matings between carriers. A 7-year follow-up descriptive evaluation indicated that notification of carrier status resulted in anxiety, embarrassment, and an inferior social status, particularly among women. In fact, 20% of parents reported that they requested that their noncarrier children not marry a carrier, even though such an arrangement would not result in any offspring with the disease. In a related study by Wooldridge and Murray (1988), carriers and noncarriers did not report differences in self-image. However, noncarriers were found to have more negative attitudes about sickle-cell carrier status than carriers, suggesting the potential for social stigmatization.
A more recent qualitative study by Williams and Schutte (1997) examined adults’ experiences with carrier testing for four disorders: cystic fibrosis, Tay-Sachs disease, Duchenne muscular dystrophy, and Fragile X syndrome. Results suggested that noncarriers experienced relief and a general sense of well-being toward their future childbearing. However, carriers reported feelings of hopelessness regarding the health of their offspring.
As is evident from this brief review, few studies of carrier testing have used validated tools for assessing psychological out-
Table 2
Carrier Testing Information for Commonly Screened Medical Conditions
Condition Characteristics
Approximate carrier frequency
Cystic fibrosis Endocrine gland dysfunction resulting in excessively thick mucus that obstructs pulmonary functioning and disturbs normal digestion
X-linked painless degenerative childhood condition of Duchenne muscular dystrophy weakening muscles
Fragile X syndrome X-linked form of moderate developmental delay
Gaucher disease
Sickle cell disease
Tay–Sachs disease
1/2,000
1/3,000–1/3,500 males
Lysosomal storage disorder
Hematologic condition resulting in abnormally shaped red blood cells often resulting in vasoocclusive pain
1/1,500 males, 1/2,000–
1/3,000 females
1/500 Ashkenazi Jews
1/400 African Americans crises
Neurological degenerative disorder beginning in infancy 1/3,000 Ashkenazi Jews
Note.
From Thompson & Thompson: Genetics in Medicine (5th ed.) (pp. 5–7), M. W. Thompson, R. R.
McInnes, and H. F. Willard, 1991, Philadelphia: W. B. Saunders. Copyright 1991 by W. B. Saunders. Reprinted with permission.
788 LERMAN, CROYLE, TERCYAK, AND HAMANN comes. However, in a prospective study of general-population cystic fibrosis screening in Great Britain, Watson, Mayall, Lamb,
Chapple, and Williamson (1992) compared carriers and noncarriers in terms of anxiety levels (as measured by the State–Trait
Anxiety Inventory [STAI]). Carriers reported small but statistically significant increases in anxiety immediately following testing.
Although most carriers did not report sustained anxiety, those who still intended to have children reported some anxiety at 6-month follow-up. Levenkron et al. (1997) also reported on the psychological status of cystic fibrosis mutation carriers. A modified version of the STAI administered after genetic counseling did not reveal differences in anxiety between carriers and a matched control sample of test decliners.
With regard to the psychological effects of carrier testing, descriptive studies provided initial evidence for social stigmatization; however, this has yet to be replicated in studies that use standardized assessments. Although some participants in carrier testing do report psychological distress, there is no evidence for long-term negative sequelae of testing in carriers. However, additional studies that use a wider range of psychological instruments are needed to draw a firm conclusion. Videotapes, Web sites, home testing, and other methods to increase access to testing are promising in this context, particularly because the risk of significant adverse psychological consequences appears to be small.
Interventions in Carrier Testing
In a novel study, Sorenson et al. (1997) compared the acceptability of free home-based versus free clinic-based education and carrier testing for cystic fibrosis. Participants were relatives of cystic fibrosis patients, all of whom had a 1:4 chance of being a gene carrier. The home-based pretest intervention consisted of written education materials and a mail-in buccal swab kit. The clinic intervention consisted of pretest education provided by a certified genetic counselor. Among those offered clinic-based education and testing, 44% accepted compared with 67% offered home-based education. No statistically significant differences were noted between the two intervention groups in terms of cystic fibrosis knowledge, anxiety, or mood; while either awaiting test results or following test-result disclosure (Cheuvront, Sorenson,
Callanan, Stearns, & DeVellis, 1998).
Other studies have focused on the use of video programs to provide standardized information to patients in a nondirective manner. Compared with patient education and patient-centered genetic counseling, video programs have been found to result in comparable levels of learning, information recall, and psychosocial well-being (Lipkin, Fisher, Rowley, Loader, & Iker, 1986).
When this form of intervention is accompanied by examples of appropriate responses to carrier information (e.g., cognitive and affective responses), as well as opportunities to receive adjunct counseling, increased patient knowledge has also been demonstrated (Loader, Sutera, Walden, Kozyra, & Rowley, 1991).
Summary and Critique of Carrier Testing Studies
Although the literature on carrier testing suffers from most of the same methodological limitations as that on prenatal testing, some tentative conclusions can be drawn. With regard to decision making, uptake of carrier testing tends to be high, especially when made accessible and recommended by a physician. Individuals appear to be especially motivated to pursue testing for conditions that are incompatible with life or are life threatening. Conditions for which treatment is available may also be associated with more favorable attitudes about the benefits of testing and with higher rates of test use. As these observations are based primarily on descriptive or qualitative analysis, studies that use decisionmaking theory and standardized assessments could perhaps shed more light on testing determinants. Further, the studies reviewed generally do not include data on emotional factors that might influence the decision-making process.
Predictive Testing
Although prenatal and carrier testing are primarily used to determine the risk of disease for one’s children, predictive genetic testing focuses on one’s own risk for developing disease later in life. The information provided by predictive testing is not uniform across diseases. For some late-onset diseases, such as Huntington’s disease (HD; a progressive neurodegenerative disorder), a genetic mutation in the HD gene is associated with a relatively certain lifetime chance of a disease for which there are no proven treatments or cures (GeneClinics, 1999). Because a mutation in an HD gene is required for disease onset, an individual who does not inherit the mutated HD gene is virtually guaranteed to never get the disease. In the case of other diseases such as breast, ovarian, and colon cancer, a positive genetic test is rarely associated with a
100% chance of disease, because most cancer susceptibility genes have reduced penetrance (Offit, 1998). Additional genetic and environmental factors are likely needed for cancer susceptibility genes to be expressed and associated with disease. Lifetime cancer probabilities for individuals who inherit alterations in major cancer susceptibility genes (e.g., BRCA1/2, hMSH2) range from about
55% to 85% (Easton, Bishop, Ford, & Crockford, 1993; Ford,
Easton, Bishop, Narod, & Goldgar, 1994; Lynch & Smyrk, 1998;
Lynch, Smyrk, & Lynch, 1997; Struewing et al., 1997). Because most cancers have no known genetic cause, a negative test result does not rule out the possible onset of cancer for an individual.
Another difference between genetic testing for HD and for cancer is that there are promising approaches for the early detection of cancer and for risk reduction. Examples of genes identified through predictive testing and the diseases associated with each can be found in Table 3.
Decision Making About Predictive Testing
Huntington’s disease.
In a series of studies conducted before
HD testing was widely available, approximately 56% to 81% of surveyed at-risk individuals expressed interest in HD testing
(Evers-Kiebooms, Swerts, Cassiman, & Van den Berghe, 1989;
Kessler, Field, Worth, & Mosbarger, 1987; Koller & Davenport,
1984; Markel, Young, & Penney, 1987; Mastromauro, Myers, &
Berkman, 1987; Meissen & Berchek, 1987; Tyler & Harper,
1983). The most prevalent reasons given for testing included reducing uncertainty and making decisions for the future. However, subsequent research on HD test uptake revealed significant discrepancies between genetic-testing intentions and actual decision making. Such studies reported that only 10% to 20% of at-risk individuals had been tested (Babul et al., 1993; Craufurd, Dodge,
Table 3
Examples of Genes and Associated Diseases Identified by
Predictive Genetic Testing
Gene
BRCA1, BRCA2 hMSH2, hMLH1, hPMS1, hPMS2
APC
HD p53
ApoE4
CYP2D6
ADPKD1
Primary associated diseases
Breast cancer, ovarian cancer
Colon cancer
Childhood polyposis leading primarily to colon cancer
Huntington disease
Childhood sarcomas, breast, and other cancers
Alzheimer disease
Lung cancer
Polycystic kidney disease
Note.
The table is based in part on data adapted from Clinical Cancer
Genetics: Risk Counseling and Management (p. 6), by K. Offit, 1998, New
York: Wiley. Copyright 1998 by Wiley. Adapted with permission. It is also based in part on data from GeneTests (1999).
Kerzin-Storrar, & Harris, 1989; Quaid & Morris, 1993). In general, the data suggest that individuals are more interested in a potentially available predictive test than one that is immediately available (Jacopini, D’Amico, Frontali, & Vivona, 1992; Quaid,
Brandt, Faden, & Folstein, 1989).
To better understand the determinants of HD test use, Codori,
Hanson, and Brandt (1994) administered questionnaires to 44 individuals who had contacted the testing program but were not tested and 66 individuals who had undergone HD testing. Test acceptors were less likely to endorse concerns about potential emotional reactions than members of the untested group. In a second study, van der
Steenstraten, Tibben, Roos, van de Kamp, and Niermeijer (1994) compared precounseling responses of persons who had received test results to those of nontested respondents. Results of the study indicated that the test decliners reported a more pessimistic outlook for the future prior to counseling (as defined by higher Beck Hopelessness
Scale [BHS] scores) than the tested group.
Cancer susceptibility testing.
In the domain of cancer susceptibility, surveys of the general population (unselected for disease risk) have reported very high levels of interest in predictive genetic testing. For example, in a random digit-dialing survey of Utah residents, over 80% of respondents said they would be “somewhat” or “very” interested in predictive genetic testing for colon cancer (Croyle & Lerman, 1993; see also Smith & Croyle, 1995).
Perceived risk of colon cancer was positively correlated with interest in testing. In a study of HMO enrollees, 69% of those surveyed said they would be interested in being tested for a breast cancer susceptibility gene. Women who believed that regular mammograms could benefit their families and give them control over their health were more likely to endorse testing (Tambor,
Rimer, & Strigo, 1997). Croyle, Dutson, Tran, and Sun (1995) found that women high in need for certainty were more interested in testing but were less interested if explicitly informed about the residual risk for noncarriers.
Studies that focused on high-risk individuals have also reported high levels of interest in genetic testing (Jacobsen, Valdimarsdottier, Brown, & Offit, 1997). Struewing, Lerman, Kase, Giambarressi, and Tucker (1995) found that 95% of members of hereditary
SPECIAL ISSUE: GENETIC TESTING 789 breast cancer families indicated that they would either “definitely” or “probably” want to be tested. Although estimated true probability of having a mutation did not predict interest in testing, those with higher perceived risk were more likely to definitely want testing. In a study of Caucasian, Japanese, and Hawaiian relatives of colon cancer patients, Glanz, Grove, Lerman, Gotay, and Le
Marchand (1999) found that almost three fourths of the study participants indicated they would “probably” or “definitely” be interested in taking a genetic test. In this study, both actual risk and perceived risk correlated with intentions. However, other studies have found that interest in genetic testing for cancer is influenced less by participants’ actual risk status than by their perceived risk and cancer concerns (Lipkus, Iden, Terrenoire, & Feaganes, 1999;
Petersen et al., 1999). Further, there is a tendency for participants in these studies to overestimate their personal risks of cancer, raising concerns that decision making may not be optimally informed (Bluman et al., 1999; Croyle & Lerman, 1999).
Initial reports have indicated that actual uptake of genetic testing for cancer susceptibility has been higher than in the case of HD testing, although not as high as predicted based on studies of testing interest (Bowen, Patenaude, & Vernon, 1999). In a study of members of a large kindred with a known family mutation in
BRCA1, the overall uptake rate was 35% (Nash et al., 1999). A study of members of hereditary breast cancer families (Lerman et al., 1996) found that 43% of eligible family members elected to receive their test results. Those who requested test results were more likely to be female, affected by cancer, have higher levels of education, and have health insurance. In addition, test uptake was positively correlated with more knowledge about BRCA1 testing, perceptions of the benefits of testing as important, and higher levels of pretest cancer worry and distress (Lerman et al., 1996;
Lerman, Schwartz, et al., 1997). In a recent study of colon cancer gene testing among members of families with hereditary colon cancer families, 43% of individuals received genetic test results
(Lerman, Hughes, Trock, et al., 1999). In this study, test acceptors were more likely to be educated and to have participated in a previous genetic linkage study. The presence of depressive symptoms (based on the Center for Epidemiological Studies Depression
Scale; CES–D) was associated with lower rates of test use, particularly among females.
Although these initial studies focused on research families, more recent studies are examining the use of genetic testing in the clinical setting. In one study of high-risk breast cancer patients who selfreferred for genetic counseling, 82% opted for testing (Schwartz et al.,
2000). Among women who perceived themselves as having a low risk of recurrence, those with higher levels of spiritual faith were significantly less likely to be tested. However, among those with high levels of perceived risk, rates of test use were high regardless of spirituality.
Perceived risk was also found to be an important predictor of genetic testing for colon cancer among relatives of colon cancer patients
(Codori et al., 1999). Armstrong et al. (2000) reported that 50% of their clinic participants utilized BRCA1/2 testing, with higher rates among women who were less concerned about job and insurance discrimination. It should be noted that the studies of research families included all eligible patients in the denominator to determine uptake.
However, clinic-based studies such as Schwartz et al. (2000) included only women presenting for counseling. Thus, the higher uptake rates in the clinic-based studies are likely because of the self-selected nature of the study sample.
790 LERMAN, CROYLE, TERCYAK, AND HAMANN
Other predictive tests.
There are a handful of studies that have explored attitudes toward testing in other predictive testing domains. In a study of interest in testing for a primarily adult onset disease, autosomal dominant polycystic kidney disease (ADPKD),
Sujansky et al. (1990) found that 97% of at-risk individuals indicated that they would use genetic testing. Although there is currently no genetic testing available for susceptibility to bipolar disorder, a study of 45 individuals with bipolar disorder indicated that 85.4% would definitely be interested in a future genetic test, and the rest (14.6%) of the study participants reported probable interest (Trippitelli, Jamison, Folstein, Bartko, & DePaulo, 1998).
Psychological Effects of Predictive Testing
Huntington’s disease.
The first longitudinal study of HD testing was initiated in British Columbia in 1986. The results indicated that immediately after learning test results (7–10 days), the increased risk group reported decreased scores on the General Well-
Being Scale, but little change on measures of distress (General
Severity Index from the Symptom Checklist 90) and depressive symptoms (Beck Depression Inventory [BDI]) from baseline.
Those who had a decreased risk reported increases on the General
Well-Being Scale, along with reductions in the General Severity
Index and the BDI. By 6 months posttest, the difference between groups was limited to scores on the General Well-Being Scale, and at the 1-year posttest measurement the groups did not differ significantly on any of the three measures (Wiggins et al., 1992).
This study also followed 40 individuals who did not receive risk-altering information. A subset (n ⫽ 23) of these individuals declined testing, whereas the others (n
⫽
17) were told that testing would not be informative for them. By the 1-year follow-up, this group had higher levels of depressive symptoms and lower wellbeing scores than the increased or decreased risk groups.
Studies of testing for HD have also examined predictors of psychological responses to testing. Tibben et al. (1993) reported data from carriers and noncarriers approximately 6 months after receiving genetic test results. Precounseling HD-related stress symptoms (based on the Impact of Event Scale [IES]) predicted poorer adjustment. Codori, Slavney, Young, Miglioretti, and
Brandt (1997) evaluated participants in an HD testing program using the BDI and the BHS. Baseline distress scores were the best predictor of postcounseling distress, and genetic status was only marginally predictive.
Cancer susceptibility.
A few large-scale longitudinal studies have begun to yield data on the psychological effects of genetic testing for cancer susceptibility. In a study of members of hereditary breast cancer families, noncarriers of BRCA1 mutations reported significant reductions in depressive symptoms (as defined by the CES–D scale) and functional impairment (as measured by two scales from the Medical Outcomes Study), compared with carriers and those who chose not to be tested. However, carriers did not show overall increases from baseline to follow-up in measures of depressive symptoms and functional impairment (Lerman et al., 1996). In another study of BRCA1 testing, carriers reported higher levels of test-related distress (as measured by the
IES) than noncarriers approximately 1–2 weeks after learning test results. Similar to the Lerman et al. (1996) study, carriers did not exhibit increases in anxiety (as defined by scores on the STAI) from baseline to follow-up (Croyle, Smith, Botkin, Baty, & Nash,
1997). In this study, carrier women who had never experienced cancer or cancer-related surgery reported higher levels of testrelated distress.
Although these studies did not provide evidence for adverse effects of testing, analyses have been conducted to identify subgroups of individuals that might be more psychologically vulnerable. Lerman, Hughes, et al. (1998) classified their hereditary breast cancer family members into low-moderate (two lowest tertiles) and high-stress (highest tertile) categories based on their scores on the Intrusion subscale of the IES. The highest levels of depression symptoms 1 month after testing (based on CES–D scores) were reported by individuals with high stress at baseline who decided not to get tested. In this subgroup, 26% reported symptoms consistent with depression at baseline, and by 1 month, this number had increased to 47%. More recently, Dorval et al.
(2000) reported that testing participants who underestimated the emotional impact of testing were more likely to experience distress 6 months after receiving their results.
A study by Codori, Petersen, Boyd, Brandt, and Giardiello
(1996) addressed the psychological effects of genetic testing for familial adenomatous polyposis, a form of colon cancer first characterized by the formation of hundreds of polyps in adolescence and early adulthood. Codori et al. (1996) surveyed tested children and their parents before and 3 months after testing using the
Children’s Depression Inventory or the Reynolds Adolescent Depression Scale and Children’s Manifest Anxiety Scale. Children’s depression levels remained in normal ranges after testing. However, mutation-positive children with affected mothers had significantly higher follow-up depression scores. Further, all children with affected mothers had increased anxiety scores.
Behavioral Outcomes of Predictive Testing
Although initial studies suggest that genetic-testing decisions were motivated by the desire to gain information about surveillance options (Patenaude et al., 1996), little is known about the actual ways in which genetic testing influences behavior. In one longitudinal study, none of the 41 BRCA1/2 carriers reported having a prophylactic mastectomy by 1-year follow-up, but 17% were considering it. It is interesting to note that 43% of the eligible carriers reported having had an oophorectomy within the year since learning their test results, with most of the other carriers considering it (Botkin et al., 2000). There were no differences in reported mammography use between carriers and noncarriers among women over 40 years old (81% of carriers and 73% of noncarriers reported a mammogram within the year). However, younger carriers (aged 25–39) were more likely than younger noncarriers to have reported a mammogram within the year (45% vs. 17%, respectively). A second study of women followed for 1 year after BRCA1/2 testing found that only 1 of 29 (3%) unaffected female carriers had a prophylactic mastectomy within 1 year after receiving genetic test results and 13% had a prophylactic oophorectomy (Lerman et al., 2000). Sixty-eight percent of carriers reported an annual mammogram at the 1-year follow-up, compared with 44% of the noncarriers. Women over 40 were more likely to have had an annual mammogram than women between 25 and 39 years old. Of greater concern was the finding that less than
15% of BRCA1/2 carriers had the recommended ovarian cancer screening.
One concern about genetic testing for cancer risk has been the possibility that testing-related distress would deter adherence to cancer screening. Although there has been some support for this association in studies of high-risk women (e.g., Kash, Holland,
Halper, & Miller, 1992), this phenomenon has not been demonstrated among individuals who have been tested. In the Botkin et al. (2000) study, there was no correlation between immediate posttest scores on the STAI and IES and 1 year posttest mammography adherence. Lerman et al. (2000) reported a positive univariate association between IES scores 1 month posttest and 1 year mammography adherence, but this relationship was not significant in the multivariate analysis. One study of women 4 – 6 months after receiving test results reported a positive correlation between breast self-examination frequency and IES scores among carriers, but no association among noncarriers (Hamann, Croyle, Smith, Smith, &
Botkin, 2000).
A related line of research has focused on genetic testing for lung cancer susceptibility. Lerman, Gold, et al. (1997) randomized smokers to receive a minimal contact smoking cessation counseling session only, counseling plus carbon monoxide feedback, or counseling plus carbon monoxide feedback and CYP2D6 genotyping. The CYP2D6 gene is associated with metabolism of carcinogens in tobacco; individuals with a genotype associated with extensive metabolizing may be more susceptible to lung cancer.
Smokers who received genetic-testing feedback reported increased levels of perceived risk, perceived benefits of quitting smoking, and fear arousal compared with the other two groups immediately after the intervention. However, at a 2-month and 12-month follow-up, there were no significant differences between groups in quit rates (Audrain et al., 1997; Lerman, Gold, et al., 1997). The genetic feedback group reported higher levels of depressive symptoms (as measured by the CES–D) at 2-month follow-up, but there were no differences by 12-month follow-up.
Interventions in Predictive Testing
Intervention studies in the field of predictive genetic testing are relatively limited, and the majority of such studies have been in the domain of breast– ovarian cancer susceptibility. Because the first breast– ovarian cancer susceptibility gene (BRCA1) was not isolated until 1994 (Miki et al., 1994) and testing has only recently become more widely available, most such intervention studies have addressed cancer risk counseling without genetic testing.
It has consistently been found, both in surveys of the general population and in studies of persons with significant family cancer histories, that individuals often overestimate their personal cancer risks (Andrykowski, Munn, & Studts, 1996; Croyle & Lerman,
1999; Struewing, Lerman, et al., 1995). Therefore, studies initiated before the availability of genetic testing often focused on reducing exaggerated risk perceptions. Lerman et al. (1995) studied women with at least one first-degree relative with breast cancer. Women were randomized to a risk-counseling condition that provided individualized breast cancer risk estimates based on the Gail model
(Gail et al., 1989) or to a control condition that provided general health information. Women who received risk counseling were 3.5
times more likely to improve their risk comprehension at a
3-month follow-up. Breast cancer risk counseling was more effective for African American women and women who reported less breast cancer preoccupation (as defined by lower scores on the
SPECIAL ISSUE: GENETIC TESTING 791
Intrusion subscale of the IES). Although the counseling intervention was effective overall, it should be noted that approximately two thirds of the women in the risk-counseling condition continued to overestimate their risk substantially 3 months after the individualized session (i.e., they perceived their risk to be higher than the highest possible score for a woman with all possible risk factors).
Other studies have incorporated educational interventions into risk notification (Alexander, Ross, Sumner, Nease, & Littenberg,
1996). After rating their perceived risk of breast cancer, the women participated in a 90-min educational session, during which the patient’s objective breast cancer risk (calculated by the Gail model) was presented visually and verbally. Perceived risk was reassessed after the education session and 3 to 11 months later. The median breast cancer risk was 15% before age 80. Participants’ perceived risk of breast cancer fell from a preintervention level of
50% to 25% after the intervention. Although postintervention perceived risk estimates were more consistent with the calculated measures, participants continued to significantly overestimate their actual risks.
Cull et al. (1998) reported on the use of videotaped information about cancer and genetics for 128 women referred to Scottish cancer clinics. Participants were randomized to watch the video before or after genetic counseling consultations with a geneticist and breast surgeon. The video included information about the role of genetic factors in the development of breast cancer, genetic risk assessment based on family history, risk reduction and cancer surveillance, and genetic counseling and testing. Results indicated that the video before group spent significantly less time with the breast surgeon, but their time with the geneticist was not significantly different than that of the other group. Both groups reported more accurate risk assessments postvideo than they had at baseline, and the two groups were not significantly different in their accuracy of breast cancer perceived risk immediately after counseling. However, the use of the video before counseling was associated with higher levels of self-reported and objective understanding of breast cancer genetic risk information immediately after counseling (but not at the 1-month follow-up). There were no differences between groups in psychological distress (as measured by the Spielberger STAI and the General Health Questionnaire) at any timepoint.
As cancer susceptibility genetic testing became a viable option but was still limited in use, a second generation of intervention studies focused not only on risk perceptions but also on interest in genetic testing. One study of women with at least one first-degree relative with breast or ovarian cancer compared a counseling approach, educational approach, and a wait-list control condition
(Lerman, Biesecker, et al., 1997). The education intervention focused on individual risk factors, benefits and limitations of testing, and surveillance options. Women in the counseling approach received the same information plus psychosocial counseling, including discussion of experiences of cancer in the family and anticipated emotional reactions to genetic testing. Both the counseling and educational approaches were associated with increases in knowledge compared with the wait-list condition at the 1-month follow-up. Only the counseling approach was associated with increases in the perceived limitations of testing and decreases in the perceived benefits at the follow-up interval. However, neither intervention was associated with overall changes in the intentions to have BRCA1 testing (Lerman, Biesecker, et al., 1997). A second
792 LERMAN, CROYLE, TERCYAK, AND HAMANN report showed that the counseling approach was associated with greater increases in the desire to be tested among African American women than was the educational approach (Lerman, Hughes,
Benkendorf, et al., 1999).
Summary and Critique of Predictive Testing Research
Initial studies in the predictive testing area used hypothetical vignettes to assess interest in testing and correlates of interest. The greatest limitation of this approach is that assessments of intentions were made following review of brief, relatively uninformative statements about the test. Because many of these studies were conducted prior to the availability of testing, data on the predictive validity of the test was not available (and remains limited). Further, these studies provided very limited information to participants about the potential risks of testing, such as insurance discrimination, adverse psychological effects, and stigmatization.
Thus, it is not surprising that levels of testing intentions greatly exceeded actual uptake of testing among individuals who participated in pretest genetic counseling sessions. It is interesting to note that although these studies showed comparable levels of interest in testing for HD and cancer, uptake of cancer gene testing has been substantially higher than that for HD.
With regard to the outcomes of genetic testing, there is limited support for adverse psychological effects. The few longitudinal studies that have been conducted show reductions in distress among noncarriers and minimal changes in distress among carriers. This may be a result of the specific genetic-testing research protocols that included comprehensive genetics education and counseling. The results of these studies may underestimate rates of psychological distress in clinical settings and among participants who are self-referred and naive to genetic testing, rather than members of research registries. Although data on behavior change following genetic testing are limited, initial results do not support substantial effects (see also Marteau & Lerman, 2001). In the next section, we consider these and other issues in greater detail, and we identify critical needs for research in this area.
Discussion and Research Needs
Decision Making About Genetic Testing
Across all genetic-testing domains, a common theme is that participants’ decisions about testing are influenced less by their actual risk status than by subjective risk and emotional factors.
Within the predictive-testing domain, there are interesting contrasts in the role of emotional factors in decision making about HD testing versus cancer gene testing. Studies suggest that cancer worries and cancer-specific distress can motivate test use (Durfy,
Bowen, McTiernan, Sporleder, & Burke, 1999; Lerman, Schwartz, et al., 1997; Vernon et al., 1999), whereas disease-specific distress appears to deter testing for HD (van der Steenstraten et al., 1994).
This is not surprising when one considers that there are no options available for preventing or treating HD, while the potential for cancer risk reduction exists. Thus, one tentative conclusion would be that the use of genetic testing is a coping response that may be facilitated by disease-specific distress, if this action is perceived as leading to increased control over disease outcomes. On the other hand, general distress appears to reduce the likelihood of testing for cancer (Lerman, Hughes, Trock, et al., 1999). Thus, even when risk reduction is possible, global distress symptoms may promote feelings of fatalism that interfere with health protective behaviors.
Although these studies shed some light on predictors of genetic test use, little is known about the mechanisms by which risk perceptions and emotional factors influence the decision-making process. On the basis of data showing an inverse relationship between anxiety and cancer risk comprehension, it has been suggested that distress interferes with information processing (Lerman et al., 1995). According to Janis and Mann (1977), stress interferes with one’s ability to process key aspects of a risk message and to weigh the advantages and disadvantages of a course of action. The effects of stress on decision-making processes have been examined systematically in laboratory settings (e.g., Keinan, 1987); however, these experimental models have yet to be applied to risk perception and decision making in the genetic-testing context. As discussed elsewhere (Croyle & Lerman, 1999), a critical need for this research is the development and validation of better measures of risk perception.
On the basis of the current literature, it is therefore not possible to determine whether use of genetic testing is an informed adaptive coping response to disease-specific concerns or whether many individuals are driven to testing without carefully considering the consequences of this action. Although not yet studied systematically, anecdotal evidence suggests that most individuals commit to a decision about genetic testing long before they participate in genetic counseling. That is, those who decide not to pursue testing generally do not avail themselves to genetic counseling, whereas the majority of persons who participate in a counseling session opt to be tested (Nash et al., 1999). Thus, it appears that genetic-testing decisions are often made without the full benefit of counseling or other sources of information. To better understand decision making about genetic testing, researchers should track decision-making processes over time, including precounseling and postcounseling assessments of distress, disease representations, comprehension, and testing motivation. These studies should aim to include all at-risk members of families, rather than self-selected counseling attenders.
Finally, decision making must be considered in the context of the family, a feature often overlooked in the literature. Initial data suggest that genetic testing for cancer susceptibility is motived, in part, by the desire to help family members (Vernon et al., 1999;
Geller, Doksum, Bernhardt, & Metz, 1999) and by family support
(Glanz et al., 1999). Individuals with positive beliefs about genetic testing may be more likely to encourage family members to undergo genetic testing (Patenaude et al., 1996). Gender of family members also appears to play an important role. In a study of women who attended cancer genetic-counseling sessions, participants were more likely to talk with female relatives about genetic counseling (Green, Richards, Murton, Statham, & Hallowell,
1997). With regard to communication of test results, 81% of
BRCA1/2 carriers and 87% of noncarriers told a sister about their test results, whereas only 61% of carriers and 68% of noncarriers communicated their results to a brother (Hughes et al., 1999).
In an effort to gain more information about the communication process, it may be helpful for future research to use well-validated measures of interpersonal communication that have been used in other domains. Self-report measures such as Benjamin’s (1983)
Intrex questionnaire and the Impact Message Inventory developed
SPECIAL ISSUE: GENETIC TESTING by Kiesler and Schmidt (1993) allow scoring based on interpersonal circumplex models. Direct observational coding systems such as the Martial Interaction Coding System (Weiss & Summers,
1983; see also Heyman, Weiss, & Eddy, 1995), the Living in
Familial Environments coding system (Hops et al., 1990), and the
Structural Analysis of Social Behavior (Benjamin, 1974) could provide rich information about genetic-testing communication among couples and other family members.
793
In the context of genetic testing for cancer susceptibility, behavior change is a key outcome, as intensive surveillance may lead to earlier detection and improved health outcomes. Despite this potential, initial studies do not provide evidence for substantial effects on cancer screening behavior. Although earlier studies of high-risk individuals suggested that distress may lead to avoidance of screening (Kash et al., 1992), this has not been shown in the genetic-testing domain (Hamann et al., 2000; Lerman et al., 2000).
More detailed process data from counseling are needed to elucidate specific cognitive and emotional barriers to adoption of medical recommendations. Interactive communication methods (e.g.,
Web based, CD-ROM) and other promising approaches to facilitate decision making and promote adherence should be evaluated in this context.
Psychological and Behavioral Outcomes of Genetic
Testing
Overall, this body of research is consistent in the finding that genetic test results have less influence on emotional distress than initially anticipated. Although some studies report initial increases in anxiety following prenatal, carrier, or predictive testing, these effects tend to be transient and not clinically significant. However, there are several important caveats. For example, most research studies have used optimal models of genetic counseling that may have more beneficial outcomes than more minimal approaches used in some clinical settings. In addition, standardized measures of distress may not be sensitive enough to detect more subtle changes in functioning that are specific to genetic testing. Some of these effects are reported anecdotally as occurring in persons who test negative, such as survivor guilt and difficulties adjusting expectations based on “good” news from testing (Bloch, Adam,
Wiggins, Huggins, & Hayden, 1992; Huggins et al., 1992).
Another caveat is that analyses of differences between groups of tested individuals (i.e., carriers, noncarriers, decliners) do not reveal within-group variation in adverse psychological effects.
With few exceptions (e.g., Lodder et al., 2001; Phipps & Zinn,
1986b), the interactions between personality and dispositional factors with test results have been largely ignored. More sophisticated theoretical models and analytic strategies should be applied to identify possible subgroups of participants that may be more psychologically vulnerable. In this regard, Baum, Friedman, and
Zakowski (1997) proposed a novel model to shape research on stress and genetic testing for disease risk. A unique feature of this model is the focus on uncertainty as a stressor characteristic and ambiguity in the appraisal process. Individual differences in tolerance for uncertainty or need for information may be important moderators of the impact of genetic test results on psychological functioning (Croyle et al., 1995; Miller, 1995; Shoda et al., 1998).
Also understudied is the effect of genetic testing on the family.
One study of HD showed that partners’ responses to testing are qualitatively similar to tested individuals (Tibben, Timman, Bannick, & Duivenvoorden, 1997). In a study of BRCA1/2 testing,
Smith, West, Croyle, and Botkin (1999) found the highest levels of distress among female carriers who had siblings who tested negative. However, distress also was elevated in male noncarriers when siblings’ test results were positive. A similar effect of siblings’ test results on female noncarriers was reported by Lodder et al. (2001). The complexity of the family interactions responsible for these findings is unlikely to be captured by ignoring interaction effects or relying on standardized measures of family environment.
New measures and analytic strategies specific to these and other issues in genetic testing are needed to tap the richness of family responses and to create a more complete picture of the effects of genetic testing.
Conclusion
By reviewing the evidence concerning psychological issues in genetic testing, we have attempted to highlight the kinds of concerns, decisions, and emotional sequelae that clinicians may encounter in patients who are members of families with inherited disease. Through collaborations with genetic counselors and medical geneticists, clinical psychologists can ensure that comprehensive programs include adequate and valid assessment, intervention, and follow-up to address the full range of issues presented. We are also versed in the conduct of research on health behavior and health outcomes—two key ingredients in successful genetictesting programs. Although the literature reviewed here does not provide evidence for significant adverse psychological effects of genetic testing, psychologists can make an important contribution toward improving risk comprehension and facilitating informed decision making regarding medical management.
Awareness of the issues, however, is only a first step toward ensuring the appropriate and effective involvement of psychologists in the new medical genetics. The design of geneticcounseling programs and provision of effective counseling and support to individuals at risk for inherited disease also requires a level of knowledge of genetics and genetic testing that today’s clinical psychologist does not have. Training programs must address this knowledge gap, with realistic expectations concerning the depth of expertise attainable within an already crowded behavioral medicine curriculum. In addition, a critical barrier to engagement is an attitude that portrays molecular biology and genetics as a rival to a holistic biobehavioral model of health and wellness.
Instead, we strongly encourage our colleagues to integrate the science and practice of genetics into an expanded model of behavioral medicine that is truly transdisciplinary and multilevel. At its best, the highly specific information provided by genetic testing can empower both clinicians and patients to target their efforts on behavioral strategies that will have the greatest impact on reducing disease morbidity and mortality.
References
Alexander, N. E., Ross, J., Summer, W., Nease, R. F., Jr., & Littenberg, B.
(1996). The effect of an educational intervention on the perceived risk of breast cancer. Journal of General Internal Medicine, 11, 92–97.
American Academy of Pediatrics/American College of Obstetricians and
Gynecologists. (1997). Guidelines for perinatal care (4th ed.). Washington, DC: Author.
794 LERMAN, CROYLE, TERCYAK, AND HAMANN
Andrykowski, M. A., Munn, R. K., & Studts, J. L. (1996). Interest in learning of personal genetic risk for cancer: A general population survey.
Preventive Medicine, 25, 527–536.
Armstrong, K., Calzone K., Stopfer J., Fitzgerald G., Coyne J., & Weber
B. (2000). Factors associated with decisions about clinical BRCA1/2 testing. Cancer Epidemiol Biomarkers Prevention, 9, 1251–1254.
Astbury, J., & Walters, W. A. (1979). Amniocentesis in the early second trimester of pregnancy and maternal anxiety. Australian Family Physi-
cian, 8, 595–599.
Audrain, J., Boyd, N. R., Roth, J., Main, D., Caporaso, N. E., & Lerman,
C. (1997). Genetic susceptibility testing in smoking-cessation treatment:
One-year outcomes of a randomized trial. Addictive Behaviors, 22,
741–751.
Babul, R., Adam, S., Kremer, B., Dufrasne, S., Wiggins, S., Huggins, M.,
Theilmann, J., Bloch, M., & Hayden, M. R. (1993). Attitudes toward direct predictive testing for the Huntington disease gene. Relevance for other adult-onset disorders. The Canadian Collaborative Group on Predictive Testing for Huntington Disease. Journal of the American Med-
ical Association, 270, 2321–2325.
Baum, A., Friedman, A. L., & Zakowski, S. G. (1997). Stress and genetic testing for disease risk. Health Psychology, 16, 8 –19.
Beeson, D., & Golbus, M. S. (1979). Anxiety engendered by amniocentesis. Birth Defects: Original Article Series, 15, 191–197.
Benjamin, L. S. (1974). Structural analysis of social behavior. Psycholog-
ical Review, 81, 392– 425.
Benjamin, L. S. (1983). The Intrex user’s manual: Parts I and II. Salt Lake
City, UT: Department of Psychology, University of Utah.
Bloch, M., Adam, S., Wiggins, S., Huggins, M., & Hayden, M. R. (1992).
Predictive testing for Huntington disease in Canada: The experience of those receiving an increased risk. American Journal of Medical Genet-
ics, 42, 499 –507.
Bluman, L. G., Rimer, B. K., Berry, D. A., Borstelmann, N., Iglehart, J. D.,
Regan, K., Schildkraut, J., & Winer, E. P. (1999). Attitudes, knowledge, and risk perceptions of women with breast and/or ovarian cancer considering testing for BRCA1 and BRCA2. Journal of Clinical Oncol-
ogy, 17, 1040 –1046.
Botkin, J. R., Smith, K. R., Croyle, R. T., Baty, B. J., Nash, J. E., Dutson,
D., Chan, A., Hamann, H. A., Lerman, C., McDonald, J., Venne, V.,
Ward, J. H., Goldgar, D. E., & Lyon, E. (2000). Genetic testing for a
BRCA1 mutation in a large kindred: Screening behavior and prophy-
lactic surgery in women 1 year post testing. Unpublished manuscript.
Bowen, D. J., Patenaude, A. F., & Vernon, S. W. (1999). Psychosocial issues in cancer genetics: From the laboratory to the public. Cancer
Epidemiology, Biomarkers & Prevention, 8, 326 –328.
Brambati, B. (1992). Prenatal genetic diagnosis through chorionic villus sampling. In A. Milunsky (Ed.), Genetic disorders and the fetus: Diag-
nosis, prevention, and treatment (3rd ed., pp. 123–153). Baltimore:
Johns Hopkins University Press.
Chescheir, N. C., & Hansen, W. F. (1999). What’s new in perinatology.
Pediatrics in Review, 20, 57– 63.
Cheuvront, B., Sorensen, J. R., Callanan, N. P., Stearns, S. C., & DeVellis,
B. M. (1998). Psychosocial and educational outcomes associated with home- and clinic-based pretest education and cystic fibrosis carrier testing among a population of at-risk relatives. American Journal of
Medical Genetics, 75, 461– 468.
Codori, A. M, Hanson, R., & Brandt, J. (1994). Self-selection in predictive testing for Huntington’s disease. American Journal of Medical Genet-
ics, 54, 167–173.
Codori, A. M, Petersen, G. M., Boyd, P. A., Brandt, J., & Giardiello, F. M.
(1996). Genetic testing for cancer in children. Short-term psychological effect. Archives of Pediatric and Adolescent Medicine, 150, 1131–1138.
Codori, A. M., Petersen, G. M., Miglioretti, D. L., Larkin, E. K., Bushey,
M. T., Young, C., Brensinger, J. D., Johnson, K., Bacon, J. A., &
Booker, S. V. (1999). Attitudes toward colon cancer gene testing:
Factors predicting test uptake. Cancer Epidemiology, Biomarkers &
Prevention, 8, 345–351.
Codori, A. M., Slavney, P. R., Young, C., Miglioretti, D. L., & Brandt, J.
(1997). Predictors of psychological adjustment to genetic testing for
Huntington’s disease. Health Psychology, 16, 36 –50.
Craufurd, D., Dodge, A., Kerzin-Storrar, L., & Harris, R. (1989). Uptake of presymptomatic predictive testing for Huntington’s disease. Lancet, 2,
603– 605.
Croyle, R. T., Dutson, D. S., Tran, V. T., & Sun, Y. C. (1995). Need for certainty and interest in genetic testing. Womens Health, 1, 329 –339.
Croyle, R. T., & Lerman, C. (1993). Interest in genetic testing for colon cancer susceptibility: Cognitive and emotional correlates. Preventive
Medicine, 22, 284 –292.
Croyle, R. T., & Lerman, C. (1999). Risk communication in genetic testing for cancer susceptibility. Journal of the National Cancer Institute Mono-
graphs, 25, 59 – 66.
Croyle, R. T., Smith, K. R., Botkin, J. R., Baty, B., & Nash, J. (1997).
Psychological responses to BRCA1 mutation testing: Preliminary findings. Health Psychology, 16, 63–72.
Cull, A., Miller, H., Porterfield, T., Mackay, J., Anderson, E. D., Steel,
C. M., & Elton, R. A. (1998). The use of videotaped information in cancer genetic counselling: A randomized evaluation study. British
Journal of Cancer, 77, 830 – 837.
Dorval, M., Patenaude, A. F., Schneider, K. A., Kieffer, S. A., DiGianni,
L., Kalkbrenner, K. J., Bromberg, J. I., Basili, L. A., Calzone, K.,
Stopfer, J., Weber, B. L., & Garber, J. E. (2000). Anticipated versus actual emotional reactions to disclosure of results of genetic tests for cancer susceptibility: Findings from p53 and BRCA1 testing programs.
Journal of Clinical Oncology, 18, 2135–2142.
Durfy, S. J., Bowen, D. J., McTiernan, A., Sporleder, J., & Burke, W.
(1999). Attitudes and interest in genetic testing for breast and ovarian cancer susceptibility to diverse groups of women in western Washington. Cancer Epidemiology, Biomarkers & Prevention, 8, 369 –375.
d’Ydewalle, G., & Evers-Kiebooms, G. (1987). Experiments on genetic risk perception and decision making: Explorative studies. Birth Defects:
Original Article Series, 23, 209 –225.
Easton, D. F., Bishop, D. T., Ford, D., & Crockford, G. P. (1993). Genetic linkage analysis in familial breast and ovarian cancer: Results from 214 families. The Breast Cancer Linkage Consortium. American Journal of
Human Genetics, 52, 678 –701.
Eng, C. M., Schechter, C., Robinowitz, J., Fulop, G., Burgert, T., Levy, B.,
Zinberg, R., & Desnick, R. J. (1997). Prenatal genetic carrier testing using triple disease screening. Journal of the American Medical Asso-
ciation, 278, 1268 –1272.
Evers-Kiebooms, G., Swerts, A., Cassiman, J. J., & Van den Berghe, H.
(1989). The motivation of at-risk individuals and their partners in deciding for or against predictive testing for Huntington’s disease. Clinical
Genetics, 35, 29 – 40.
Fava, G. A., Kellner, R., Michelacci, L., Trombini, G., Pathak, D., Orlandi,
C., & Bovicelli, L. (1982). Psychological reactions to amniocentesis: A controlled study. American Journal of Obstetrics and Gynecology, 143,
509 –513.
Fava, G. A., Trombini, G., Michelacci, L., Linder, J. R., Pathak, D., &
Bovicelli, L. (1983). Hostility in women before and after amniocentesis.
The Journal of Reproductive Medicine, 28, 29 –34.
Ford, D., Easton, D. F., Bishop, D. T., Narod, S. A., & Goldgar, D. E.
(1994). Risks of cancer in BRCA1-mutation carriers. The Breast Cancer
Linkage Consortium. Lancet, 343, 692– 695.
French, B. N., Kurczynski, T. W., Weaver, M. T., & Pituch, M. J. (1992).
Evaluation of the Health Belief Model and decision making regarding amniocentesis in women of advanced maternal age. Health Education
Quarterly, 19, 177–186.
Gail, M. H., Brinton, L. A., Byar, D. P., Corle, D. K., Green, S. B.,
Schairer, C., & Mulvihill, J. J. (1989). Projecting individualized proba-
bilities of developing breast cancer for White females who are being examined annually. Journal of the National Cancer Institute, 81, 1879 –
1886.
Geller, G., Doksum, T., Bernhardt, B. A., & Metz, S. A. (1999). Participation in breast cancer susceptibility testing protocols: Influence of recruitment source, altruism, and family involvement on women’s decisions. Cancer Epidemiology, Biomarkers & Prevention, 8, 377–383.
GeneTests. (1999). Gene tests. Retrieved December 12, 1999, from http:// www.genetests.org
Glanz, K., Grove, J., Lerman, C., Gotay, C., & Le Marchand, L. (1999).
Correlates of intentions to obtain genetic counseling and colorectal cancer gene testing among at-risk relatives from three ethnic groups.
Cancer Epidemiology, Biomarkers & Prevention, 8, 329 –336.
Green, J. M. (1990). Calming or harming? A critical review of psycholog-
ical effects of fetal diagnosis on pregnant women (Occasional Papers,
2nd Series No. 2). London: The Galton Institute.
Green, J., Richards, M., Murton, F., Statham, H., & Hallowell, N. (1997).
Family communication and genetic counseling: The case of hereditary breast and ovarian cancer. Journal of Genetic Counseling, 6, 45– 60.
Hamann, H. A., Croyle, R. T., Smith, T. W., Smith, K. R., & Botkin, J. R.
(2000, April). Predictors of breast self-examination frequency among
women tested for a BRCA1 mutation. Poster session presented at the 21st annual meeting of the Society of Behavioral Medicine, Nashville, TN.
Hartley, N. E., Scotcher, D., Harris, H., Williamson, P., Wallace, A.,
Craufurd, D., & Harris, R. (1997). The uptake and acceptability to patients of cystic fibrosis carrier testing offered in pregnancy by the GP.
Journal of Medical Genetics, 34, 459 – 464.
Heyman, R. E., Weiss, R. L., & Eddy, J. M. (1995). Marital Interaction
Coding System: Revision and empirical evaluation. Behaviour Research
and Therapy, 33, 737–746.
Hops, H., Biglan, A., Tolman, A., Sherman, L., Arthur, J., Warner, P., Romano, J., Turner, J., Friedman, L., Bulcroft, R., Holcomb, C., Oostenink,
N., & Osteen, V. (1990). Living in familial environments (LIFE) coding
system: Training/procedures and reference manual for coders (Rev.
ed.). Eugene: Oregon Research Institute.
Huggins, M., Bloch, M., Wiggins, S., Adam, S., Suchowersky, O., Trew,
M., Klimek, M., Greenberg, C. R., Eleff, M., Thompson, L. P., Knight,
J., MacLeod, P., Girard, K., Theilmann, J., Hedrick, A., & Hayden,
M. R. (1992). Predictive testing for Huntington disease in Canada:
Adverse effects and unexpected results in those receiving a decreased risk. American Journal of Medical Genetics, 42, 508 –515.
Hughes, C., Lynch, H., Durham, C., Snyder, C., Lemon, S., Narod, S.,
Fulmore, C., Main, D., & Lerman, C. (1999). Communication of
BRCA1/2 test results in hereditary breast cancer families. Cancer Re-
search Therapy and Control, 8, 51–59.
Jacobsen, P. B., Valdimarsdottier, H. B., Brown, K. L, & Offit, K. (1997).
Decision-making about genetic testing among women at familial risk for breast cancer. Psychosomatic Medicine, 59, 459 – 466.
Jacopini, G. A., D’Amico, R., Frontali, M., & Vivona, G. (1992). Attitudes of persons at risk and their partners toward predictive testing. Birth
Defects Original Articles Series, 28, 113–117.
Janis, I. L., & Mann, L. (1977). Decision making: A psychological analysis
of conflict, choice, and commitment. New York: Free Press.
Kash, K. M., Holland, J. C., Halper, M. S., & Miller, D. G. (1992).
Psychological distress and surveillance behaviors of women with a family history of breast cancer. Journal of the National Cancer Insti-
tute, 84, 24 –30.
Keinan, G. (1987). Decision making under stress: Scanning of alternatives under controllable and uncontrollable threats. Journal of Personality and
Social Psychology, 52, 639 – 644.
Kessler, S., Field, T., Worth, L., & Mosbarger, H. (1987). Attitudes of persons at risk for Huntington disease toward predictive testing. Amer-
ican Journal of Medical Genetics, 26, 259 –270.
Kiesler, D. J., & Schmidt, J. A. (1993). The Impact Message Inventory:
SPECIAL ISSUE: GENETIC TESTING 795
Form IIA Octant Scale Version. Palo Alto, CA: Mind Garden (Consulting Psychologists Press).
Koller, W. C., & Davenport, J. (1984). Genetic testing in Huntington’s disease. Annals of Neurology, 16, 511–513.
Kronn, D., Jansen, V., & Ostrer, H. (1998). Carrier screening for cystic fibrosis, Gaucher disease, and Tay-Sachs disease in the Ashkenazi
Jewish population: The first 1000 cases at New York University Medical
Center, New York, NY. Archives of Internal Medicine, 158, 777–781.
Lerman, C., Biesecker, B., Benkendorf, J. L., Kerner, J., Gomez-Caminero,
A., Hughes, C., & Reed, M. M. (1997). Controlled trial of pretest education approaches to enhance informed decision-making for BRCA1 gene testing. Journal of the National Cancer Institute, 89, 148 –157.
Lerman, C., Gold, K., Audrain, J., Lin, T. H., Boyd, N. R., Orleans, C. T.,
Wilfond, B., Louben, G., & Caporaso, N. (1997). Incorporating biomarkers of exposure and genetic susceptibility into smoking cessation treatment: Effects on smoking-related cognitions, emotions, and behavior change. Health Psychology, 16, 87–99.
Lerman, C., Hughes, C., Benkendorf, J. L., Biesecker, B., Kerner, J.,
Willison, J., Eads, N., Hadley, D., & Lynch, J. (1999). Racial differences in testing motivation and psychological distress following pretest education for BRCA1 gene testing. Cancer Epidemiology, Biomarkers &
Prevention, 8, 361–367.
Lerman, C., Hughes, C., Croyle, R. T., Main, D., Durham, C., Snyder, C.,
Bonney, A., Lynch, J. F., Narod, S. A., & Lynch, H. T. (2000). Prophylactic surgery decisions and surveillance practices one year following BRCA1/2 testing. Preventive Medicine, 31, 75– 80.
Lerman, C., Hughes, C., Lemon, S. J., Main, D., Snyder, C., Durham, C.,
Narod, S., & Lynch, H. T. (1998). What you don’t know can hurt you:
Adverse psychologic effects in members of BRCA1-linked and BRCA2linked families who decline genetic testing. Journal of Clinical Oncol-
ogy, 16, 1650 –1654.
Lerman, C., Hughes, C., Trock, B. J., Myers, R. E., Main, D., Bonney, A.,
Abbaszadegan, M. R., Harty, A. E., Franklin, B. A., Lynch, J. F., &
Lynch, H. T. (1999). Genetic testing in families with hereditary nonpolyposis colon cancer. Journal of the American Medical Association, 281,
1618 –1622.
Lerman, C., Lustbader, E., Rimer, B., Daly, M., Miller, S., Sands, C., &
Balshem, A. (1995). Effects of individualized breast cancer risk counseling: A randomized trial. Journal of the National Cancer Institute, 87,
286 –292.
Lerman, C., Narod, S., Schulman, K., Hughes, C., Gomez-Caminero, A.,
Bonney, G., Gold, K., Trock, B., Main, D., Lynch, J., Fulmore, C.,
Snyder, C., Lemon, S. J., Conway, T., Tonin, P., Lenoir, G., & Lynch,
H. (1996). BRCA1 testing in families with hereditary breast-ovarian cancer: A prospective study of patient decision making and outcomes.
Journal of the American Medical Association, 275, 1885–1892.
Lerman, C., Schwartz, M. D., Narod, S., Lin, T. H., Hughes, C., & Lynch,
H. T. (1997). The influence of psychological distress on use of genetic testing for cancer risk. Journal of Consulting and Clinical Psychol-
ogy, 65, 414 – 420.
Levenkron, J. C., Loader, S., & Rowley, P. T. (1997). Carrier screening for cystic fibrosis: Test acceptance and one year follow-up. American Jour-
nal of Medical Genetics, 73, 378 –386.
Lipkin, M., Jr., Fisher, L., Rowley, P. T., Loader, S., & Iker, H. P. (1986).
Genetic counseling of asymptomatic carriers in a primary care setting:
The effectiveness of screening and counseling for beta-thalassemia trait.
Annals of Internal Medicine, 105, 115–123.
Lipkus, I. M., Iden, D., Terrenoire, J., & Feaganes, J. R. (1999). Relationships among breast cancer concern, risk perceptions, and interest in genetic testing for breast cancer susceptibility among African-American women with and without a family history of breast cancer. Cancer
Epidemiology, Biomarkers & Prevention, 8, 533–539.
Loader, S., Sutera, C. J., Walden, M., Kozyra, A., & Rowley, P. T. (1991).
796 LERMAN, CROYLE, TERCYAK, AND HAMANN
Prenatal screening for hemoglobinopathies: II. Evaluation of counseling.
American Journal of Medical Genetics, 48, 447– 451.
Lodder, L., Frets, P. G., Trijsburg, R. W., Meijers-Heijboer, E. J., Klijn,
J. G., Duivenvoorden, H. J., Tibben, A., Wagner, A., van der Meer,
C. A., van den Ouweland, A. M., & Niermeijer, M. F. (2001). Psychological impact of receiving a BRCA1/BRCA2 test result. American
Journal of Medical Genetics, 98, 15–24.
Lynch, H. T., & Smyrk, T. (1998). An update on Lynch syndrome. Current
Opinions in Oncology, 10, 349 –356.
Lynch, H. T., Smyrk, T., & Lynch, J. (1997). An update of HNPCC (Lynch syndrome). Cancer Genetics and Cytogenetics, 93, 84 –99.
Markel, D. S., Young, A. B., & Penney, J. B. (1987). At-risk persons’ attitudes toward presymptomatic and prenatal testing of Huntington disease in Michigan. American Journal of Medical Genetics, 26, 295–
305.
Marteau, T. M., Cook, R., Kidd, J., Michie, S., Johnston, M., Slack, J., &
Shaw, R. W. (1992). The psychological effects of false-positive results in prenatal screening for fetal abnormality: A prospective study. Prena-
tal Diagnosis, 12, 205–214.
Marteau, T. M., Kidd, J., Cook, R., Johnston, M., Michie, S., Shaw, R. W.,
& Slack, J. (1988). Screening for Down’s syndrome. British Medical
Journal, 297, 1469.
Marteau, T. M., Kidd, J., Cook, R., Michie, S., Johnston, M., Slack, J., &
Shaw, R. W. (1991). Perceived risk not actual risk predicts uptake of amniocentesis. British Journal of Obstetrics and Gynaecology, 98, 282–
286.
Marteau, T. M., Kidd, J., Cook, R., Michie, S., Johnston, M., Slack, J., &
Shaw, R. W. (1992). Psychological effects of having amniocentesis: Are these due to the procedure, the risk or the behaviour? Journal of
Psychosomatic Research, 36, 395– 402.
Marteau, T., & Lerman, C. (2001). Genetic risk and behaviour change.
British Medical Journal, 322 (7293), 1056 –1059.
Massarik, F., & Kaback, M. M. (1981). Genetic disease control: a social
psychological approach. Beverly Hills, CA: Sage.
Mastromauro, C., Myers, R. H., & Berkman, B. (1987). Attitudes toward presymptomatic testing in Huntington disease. American Journal of
Medical Genetics, 26, 271–282.
McConkie-Rosell, A., Spiridigliozzi, G. A., Rounds, K., Dawson, D. V.,
Sullivan, J. A., Burgess, D., & Lachiewicz, A. M. (1999). Parental attitudes regarding carrier testing in children at risk for fragile X syndrome. American Journal of Medical Genetics, 82, 206 –211.
Meissen, G. J., & Berchek, R. L. (1987). Intended use of predictive testing by those at risk for Huntington disease. American Journal of Medical
Genetics, 26, 283–293.
Miki, Y., Swensen, J., Shattuck-Eidens, D., Futreal, P. A., Harshman, K.,
Tavtigian, S., Liu, Q., Cochran, C., Bennett, L. M., Ding, W., Bell, R.,
Rosenthal, J., Hussey, C., Tanh, T., McClure, M., Frye, C., Hattier, T.,
Phelps, R., Haugen-Strano, A., Katcher, H., Yakumo, K., Gholami, Z.,
Shaffer, D., Stone, S., Bayer, S., Wray, C., Bogden, R., Dayanath, P.,
Ward, J., Tonin, P., Narod, S., Bristow, P. K., Norris, F. H., Helvering,
L., Morrison, P., Rosteck, P., Lai, M., Barrett, J. C., Lewis, C., Neuhausen, S., Cannon-Albright, L., Goldgar, D., Wiseman, R., Kamb, A.,
& Skolnick, M. H. (1994, October 7). A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science, 266, 66 –71.
Miller, S. M. (1995). Monitoring versus blunting styles of coping with cancer influence the information patients want and need about their disease. Cancer, 76, 167–177.
Nash, J., Dutson, D., Croyle, R. T., Smith, K. R., Baty, B. J., & Botkin,
J. R. (1999). BRCA1 testing uptake in a large kindred. Unpublished manuscript.
Offit, K. (1998). Clinical cancer genetics: Risk counseling and manage-
ment. New York: Wiley.
Ormond, K. E., Pergament, E., & Fine, B. A. (1996). Pre-screening education in multiple marker screening programs: The effect on patient anxiety and knowledge. Journal of Genetic Counseling, 5, 69 – 80.
Patenaude, A. F., Schneider, K. A., Kieffer, S. A., Calzone, K. A., Stopfer,
J. E., Basili, L. A., Weber, B. L., & Garber, J. E. (1996). Acceptance of invitations for p53 and BRCA1 predisposition testing: Factors influencing potential utilization of cancer genetic testing. Psycho-Oncology, 5,
241–250.
Petersen, G. M., Larkin, E., Codori, A. M., Wang, C. Y., Booker, S. V.,
Bacon, J., Giardiello, F. M., & Boyd, P. A. (1999). Attitudes toward colon cancer gene testing: Survey of relatives of colon cancer patients.
Cancer Epidemiology, Biomarkers & Prevention, 8, 337–344.
Phipps, S., & Zinn, A. B. (1986a). Psychological response to amniocentesis: I. Mood state and adaptation to pregnancy. American Journal of
Medical Genetics, 25, 131–142.
Phipps, S., & Zinn, A. B. (1986b). Psychological response to amniocentesis: II. Effects of coping style. American Journal of Medical Genet-
ics, 25, 143–148.
Quaid, K. A., Brandt, J., Faden, R. R., & Folstein, S. E. (1989). Knowledge, attitude, and the decision to be tested for Huntington’s disease.
Clinical Genetics, 36, 431– 438.
Quaid, K. A., & Morris, M. (1993). Reluctance to undergo predictive testing: The case of Huntington disease. American Journal of Medical
Genetics, 45, 41– 45.
Robinson, G. E., Garner, D. M., Olmsted, M. P., Shime, J., Hutton, E. M.,
& Crawford, B. M. (1988). Anxiety reduction after chorionic villus sampling and genetic amniocentesis. American Journal of Obstetrics
and Gynecology, 159, 953–956.
Robinson, J. O., Hibbard, B. M., & Laurence, K. M. (1984). Anxiety during a crisis: Emotional effects of screening for neural tube defects.
Journal of Psychosomatic Research, 28, 163–169.
Romero, R., Ghidini, A., & Santolaya, J. (1992). Fetal blood sampling. In
A. Milunsky (Ed.), Genetic disorders and the fetus: Diagnosis, preven-
tion, and treatment (3rd ed., pp. 649 – 682). Baltimore: Johns Hopkins
University Press.
Schwartz, M. D., Hughes, C., Roth, J., Main, D., Peshkin, B. N., Isaacs, C.,
Kavanagh, C., & Lerman, C. (2000). Spiritual faith and genetic testing decisions among high risk breast cancer probands. Cancer Epidemiol-
ogy, Biomarkers & Prevention, 7, 55– 68.
Shiloh, S., & Saxe, L. (1989). Perception of risk in genetic counseling.
Psychology and Health, 3, 45– 61.
Shoda, M., Mischel, W., Miller, S. M., Diefenbach, M., Daly, M. B., &
Engstrom, P. F. (1998). Psychological interventions and genetic testing:
Facilitating informed decisions about BRCA1/2 cancer susceptibility.
Journal of Clinical Psychology in Medical Settings, 5, 3–17.
Smith, K. R., & Croyle, R. T. (1995). Attitudes toward genetic testing for colon cancer risk. American Journal of Public Health, 85, 1435–1438.
Smith, K. R., West, J. A., Croyle, R. T., & Botkin, J. R. (1999). Familial context of genetic testing for cancer susceptibility: Moderating effect of siblings’ test results on psychological distress one to two weeks after
BRCA1 mutation testing. Cancer Epidemiology, Biomarkers & Preven-
tion, 8, 385–392.
Sorenson, J. R., Cheuvront, B., DeVellis, B., Callanan, N., Silverman, L.,
Koch, G., Sharp, T., & Fernald, G. (1997). Acceptance of home and clinic-based cystic fibrosis carrier education and testing by first, second, and third degree relatives of cystic fibrosis patients. American Journal of
Medical Genetics, 70, 121–129.
Spencer, J. W., & Cox, D. N. (1987). Emotional responses of pregnant women to chorionic villi sampling or amniocentesis. American Journal
of Obstetrics and Gynecology, 157, 1155–1160.
Stamatoyannopoulus, G. (1974). Problems of screening and counseling in the hemoglobinopathies. In A. G. Motulsky & W. Lenz (Eds.), Birth defects: Proceedings of the 4th international conference, Vienna, Austria (September 2– 8, 1973).
Statham, H., & Green, J. (1993). Serum screening for Down’s syndrome:
Some women’s experiences. British Medical Journal, 307, 174 –176.
Struewing, J. P., Hartge, P., Wacholder, S., Baker, S. M., Berlin, M.,
McAdams, M., Timmerman, M. M., Brody, L. C., & Tucker, M. A.
(1997). The risk of cancer associated with specific mutations of BRCA1 and BRCA2 among Ashkenazi Jews. The New England Journal of
Medicine, 336, 1401–1408.
Struewing, J. P., Lerman, C., Kase, R. G., Giambarresi, T. R., & Tucker,
M. A. (1995). Anticipated uptake and impact of genetic testing in hereditary breast and ovarian cancer families. Cancer Epidemiology,
Biomarkers & Prevention, 4, 169 –173.
Sujansky, E., Kreutzer, S. B., Johnson, A. M., Lezotte, D. C., Schrier,
R. W., & Gabow, P. A. (1990). Attitudes of at-risk and affected individuals regarding presymptomatic testing for autosomal dominant polycystic kidney disease. American Journal of Medical Genetics, 35, 510 –
515.
Tabor, A., & Jonsson, M. H. (1987). Psychological impact of amniocentesis on low-risk women. Prenatal Diagnosis, 7, 443– 449.
Tambor, E. S., Rimer, B. K., & Strigo, T. S. (1997). Genetic testing for breast cancer susceptibility: Awareness and interest among women in the general population. American Journal of Medical Genetics, 68,
43– 49.
Tercyak, K. P., Johnson, S. B., Roberts, S. F., & Cruz, A. C. (2001).
Psychological response to prenatal genetic counseling and amniocentesis. Patient Education and Counseling, 43, 73– 84.
Thompson, M. W., McInnes, R. R., & Willard, H. F. (1991). Thompson
& Thompson: Genetics in medicine (5th ed.). Philadelphia: W. B.
Saunders.
Tibben, A., Duivenvoorden, H. J., Vegter-van der Vlis, M., Niermeijer,
M. F., Frets, P. G., van de Kamp, J. J., Roos, R. A., Rooijmans, H. G.,
& Verhage, F. (1993). Presymptomatic DNA testing for Huntington disease: Identifying the need for psychological intervention. American
Journal of Medical Genetics, 48, 137–144.
Tibben, A., Timman, R., Bannink, E. C., & Duivenvoorden, H. J. (1997).
Three-year follow-up after presymptomatic testing for Huntington’s disease in tested individuals and partners. Health Psychology, 16, 20 –
35.
Trippitelli, C. L., Jamison, K. R., Folstein, M. F., Bartko, J. J., & DePaulo,
SPECIAL ISSUE: GENETIC TESTING 797
J. R. (1998). Pilot study on patients’ and spouses’ attitudes toward potential genetic testing for bipolar disorder. American Journal of Psy-
chiatry, 155, 899 –904.
Tunis, S. L., Golbus, M. S., Copeland, K. L., Fine, B. A., Rosinsky, B. J.,
& Seely, L. (1990). Patterns of mood states in pregnant women undergoing chorionic villus sampling or amniocentesis. American Journal of
Medical Genetics, 37, 191–199.
Tyler, A., & Harper, P. S. (1983). Attitudes of subjects at risk and their relatives towards genetic counselling in Huntington’s chorea. Journal of
Medical Genetics, 20, 179 –188.
van der Steenstraten, I. M., Tibben, A., Roos, R. A., van de Kamp, J. J., &
Niermeijer, M. F. (1994). Predictive testing for Huntington disease:
Nonparticipants compared with participants in the Dutch program.
American Journal of Human Genetics, 55, 618 – 625.
Vernon, S. W., Gritz, E. R., Peterson, S. K., Perz, C. A., Marani, S., Amos,
C. I., & Baile, W. F. (1999). Intention to learn results of genetic testing for hereditary colon cancer. Cancer Epidemiology, Biomarkers & Pre-
vention, 8, 353–360.
Watson, E. K., Mayall, E. S., Lamb, J., Chapple, J., & Williamson, R.
(1992). Psychological and social consequences of community carrier screening programme for cystic fibrosis. The Lancet, 340, 217–220.
Weiss, R. L., & Summers, K. J. (1983). Martial Interaction Coding System—III. In E. Filsinger (Ed.), Marriage and family assessment (pp.
85–115). Beverly Hills, CA: Sage.
Wiggins, S., Whyte, P., Huggins, M., Adam, S., Theilmann, J., Bloch, M.,
Sheps, S. B., Schechter, M. T., & Hayden, M. R. (1992). The psychological consequences of predictive testing for Huntington’s disease.
Canadian Collaborative Study of Predictive Testing. The New England
Journal of Medicine, 327, 1401–1405.
Williams, J. K., & Schutte, D. L. (1997). Benefits and burdens of genetic carrier identification. Western Journal of Nursing Research, 19, 71– 81.
Wooldridge, E. Q., & Murray, R. F., Jr. (1988). The Health Orientation
Scale: A measure of feelings about sickle cell trait. Social Biology, 35,
123–136.
Received February 18, 2001
Revision received August 10, 2001
Accepted August 10, 2001 䡲