Legal Aspects - Minnesota Department of Human Services
advertisement

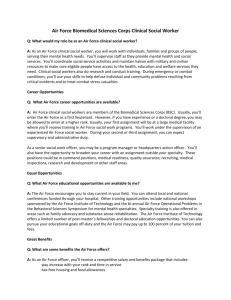
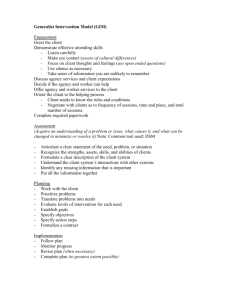
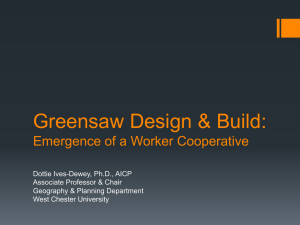
Handout Reference List Rule 79 Children’s Mental Health 405 – INTERVENTION # 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 TITLE Agenda Learning Objectives Intervention Services & Legal Aspects Core Competencies Idea Catcher Intervention Services PowerPoint Cultural Competence Self Assessment Samples of Age Appropriate Assessment Tools Individual Family Community Support Plan Family Systems Theory Rules to Build a Genogram Pacer Projects Family Strengths Assessment Scales Reframing Exercise Worksheet Case Study-Grandma's Child Observation Strategies for Indicators of Family Violence Decision Tree for IEP and 504 Highlights of Federal Education Programs for Children with Mental Health Problems MNDOE – Individual Agency Intervention Plan IIIP MNDOE – Section 504 of the Rehab Act MNDOE – MN State Interagency Coordination (MnSIC) MNDOE – Emotional and Behavioral Disabilities MNDOE – Mental Health MNDOE – Special Education MNDOE – Secondary Transition Major Components of IFCSP Project C3 Connecting Youth to Communities and Careers Independent Living Skills [ILS] Competencies 406 – Legal Aspects # 28 29 30 31 32 33 34 35 36 37 38 TITLE Legal Aspects PowerPoint Presentation Authorization for the Release and Exchange of Information (Sample: Olmsted County) Elements of Minnesota Data Privacy Ethics and Professional Practice and Professional Boundaries (Sample: Hennepin County) Scenario for Discussion Informed Consent and Client Confidentiality IV E Reimbursement Child Protection Mandatory Reporting Office of the Ombudsman for Mental Health and Mental Retardation Medical Review Subcommittee Serious Injury Report Action Plan Evaluation 400C – Rule 79 Children’s Mental Health: Intervention & Legal Aspects Revised 06/27/06 Page 1 of 1 AGENDA CHILDREN’S MENTAL HEALTH CORE SERIES CORE 405 – INTERVENTION SERVICES & CORE 406 – LEGAL ASPECTS TRAINING DAY 1 09 9:00 CORE 405: INTERVENTION SERVICES Introductions and Orientation Opening Exercise Idea Catcher 09 9:30 Review Collaboration Model For Intervention Services 10:30 Collecting Family Data and Building Trust Noon Lunch 01 1:00 Culturally Competent Interventions 02 2:30 04 4:00 Developing and Implementing Individualized Interagency Intervention Plan & Individualized Family Community Support Plan Adjourn TRAINING DAY 2 09 9:00 Welcome and Review of Previous Day’s Activities 09 9:30 Understanding P.L. 94-142 and IDEA 10:15 Individual Education Plans and Plans To Refer Child To Adult Services 11:15 11:45 Noon Features of Family Systems Theory and Family Group Decision Making Wrap-Up Lunch CORE 406: LEGAL ASPECTS 01 1:00 Legal Issues In CMH Case Management 01 1:20 Release of Information and Data Privacy 02 2:00 Ethics and Professional Boundaries 02 2:30 Group Exercise/Break 03 3:15 Child Protection Processes 03 3:45 Course Evaluations 04 4:00 Adjourn 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 1 Learning Objectives CORE 405 – INTERVENTION SERVICES Participants will be able to: 1. Collaborate with other practitioners to provide client assessment, case planning and delivery 2. Select services which incorporate cultural strengths and are compatible with the culture of the children and their families 3. Use a variety of age appropriate methods to elicit and transmit information and build trust with children 4. Recognize the indicators of family violence and assess risk to family members 5. Locate day treatment and residential treatment programs which meet the needs of the child and are the least restrictive 6. Write an action plan six months prior to the child’s 18th birthday which refers the child to adult case management services 7. Understand the intent of P.L. 94-142 and IDEA 8. Describe the process for developing at Individualized Interagency Intervention Plan (IIIP) 9. Apply the principles of family systems theory to the child’s needs, family assessment, case management planning and service delivery 10. Implement an Individualized Family Community Support Plan including referrals to other service providers 11. Empathize with families who have a child with a specific concern or disorder including severe psychiatric disorders 12. Apply the principles of the wraparound model of service to meet the needs of children and their families CORE 406 – LEGAL ASPECTS Participants will be able to: 1. Describe the legal issue that affect the practice of children’s mental health practice and knows how to implement legal requirements. This includes confidentiality, Tennessen Warning and HIPPA. 2. Provide clients with information about the Office of Ombudsman for Mental Health and Mental Retardation. 3. File a mandatory report of abuse under both their county’s process and the tribal process. 4. Meet the legal requirements of IV-E, Medical Assistance and third party payers when placing a child in an out-of-home placement. 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 Page 1 of 1 CORE 405 & 406 COMPETENCIES INTERVENTION SERVICES 405-1 405-2 405-3 405-4 405-5 405-6 405-7 405-8 405-9 405-10 405-11 405-12 405-13 405-14 405-15 405-16 405-17 405-18 405-19 The worker can collaborate with practitioners in other agencies and service disciplines in a team approach to provide client assessment, case planning and delivery. The worker will have knowledge of and be sensitive to cultural strengths and differences and be able to implement services that incorporate cultural strengths. The worker will demonstrate their cultural sensitivity in their interactions and use interventions that are compatible with the culture of children and their families. The worker can communicate with and interview children using a variety of age-appropriate methods and strategies to elicit and transmit information and build trust. The worker recognizes the indicators of family violence; understands the dynamics of family violence; and can assess the family situation to determine risk to family members. The worker can promote delivery of effective services for families through case management; referral to community resources; utilization of community support systems; including nontraditional and neighborhood resources; utilization and expansion of family support; and the direct provision of supportive and rehabilitative services. The worker knows how to seek out resource information to address the needs of the family and child as identified in the individual family community support plan. The worker understands the role and responsibilities of the children’s service agency, juvenile court, county prosecutor, law enforcement agency, hospital, schools, mental health and chemical health systems, and other community agencies involved in the identification, assessment and treatment of mental health. The worker understands the day treatment and residential treatment programs including assessment, eligibility determination and on-going services and can identify the least restrictive setting to meet the child’s treatment needs. The worker can identify education and preventive services. The worker can prepare a plan of action with parents/caregivers six months prior to the child’s 18th birthday for making a referral to adult case management services and other necessary services, e.g. housing, vocational and medical. The worker knows the importance of the Individual Education Plan and how to ensure that the mental needs of the child are included in the document and that they are carried out in the least restrictive setting. The worker knows the intent of P.L. 94-142 and IDEA; knows the available alternatives to traditional education, and can advocate for special services and programs for children and youth, including: the IEP (Individual Educational Plan), IIIP (Individual Interagency Intervention Plan), 504 Plan work and vocational programs, Severe Emotional Disturbance (SED), Learning Disabled (LD), adult education and GED preparation. The worker has the knowledge of the development of the family centered Individualized Interagency Intervention Plan (IIIP) for children and youth (birth through 21). The worker knows how to develop and implement an individual family community support plan. The worker can determine when a child or the family should be referred to other services. The worker understands the principles of family systems theory (the whole family moving forward not just individual members) and knows how to apply these principles to the child’s needs and family assessment, case management planning and service delivery. The worker will be familiar with the experiences and needs of families that have a child with a specific concern or disorder, including severe psychiatric disorders. The worker understands the wraparound model of service delivery and knows how to apply the principles to the child’s needs and family assessment, case management planning and service delivery. LEGAL ASPECTS 406-1 406-2 406-3 406-4 406-5 406-6 The worker understands the legal issues that affect the practice of children’s mental health practice and knows how to implement legal requirements. This includes confidentiality; mental health data practices and HIPPA. The worker will be aware of specific risks to children – biological, psychological and socio-culturaland be able to identify the severity of these risks with specific families and children. The worker understands the services provided by the Office of the Ombudsman for Mental Health and Mental Retardation The worker can outline the Minnesota guidelines for mandated reporting of abuse. The worker is aware of the county/tribal reporting processes. The worker knows the county/tribal policies and protocol for out-of-home placements. 400C – Children’s Mental Health Formatted 06/27/06 Page 1 of 1 Idea Catcher DON’T LET A GOOD IDEA GET AWAY! Research shows that people remember 20% of what they hear, 30% of what they see, 70% of what they say and 90% of what they do! If you use an idea within 24 hours of learning it, you’re more likely to integrate it permanently. If you hear or think of an idea or concept you want to use back on your job – WRITE IT DOWN. __________________________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ (Use the back of paper if necessary) 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 Adapted from the Idea Catcher developed by the Ohio Welfare Training Program Page 1 of 1 MCWTS • Leeann Jorgensen, Trainer CORE 405 Intervention Services • Mary Jo Verschay • Sue Stoterau • Lorna Wiens Objectives • Collaborate • Incorporate cultural strengths • Age appropriate • Family Safety • Placement Resources • Secondary transition Action Plan • PL 94-192 and IDEA, OHI • • • • IEP & IIIP Family Systems Empathy Wraparound Process Values and Principles • Collaboration Model Agenda • Welcome and Introductions • Family Systems Theory • Pacer Video • Case Management Steps • Collecting Family Information • • • • Family Safety Placement Resources PL 94-192, IEP Transition Planning Ball Toss • What learning have you applied from previous sessions? • How did it work? 400C - Rule 79 Children's Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 5 Expectations • Given the objectives for the day, what would you be most interested in learning, practicing, discussing? Other premises Family Systems • • • • • • Interrelated structure Patterns Boundaries Composition law Norms Subsystems Genogram Review • Homeostasis • Handout • Roles • Genogram changes with stress and illness • Decision-making Genogram • Draw your family genogram with positions, then identify a stressor or illness, describe how the communication, roles, decisionmaking changed with that stressor in small group. • PACER Video. What is the experience for families?? • Share themes in large group 400C - Rule 79 Children's Mental Health Formatted 06/27/06 405 - Intervention Services Page 2 of 5 Family Group DecisionMaking Process • Referral for meeting • Preparation • Meeting – Family Group Process – Family Unity – Hybrid Family • Post conference Best Practice: What are good ideas for families with 0-1 year old 2-3 year olds 4-5 year olds 6-8 year olds 9-12 year olds 13-16 year olds Over 16 Reminder: Children w/ sed often have developmtl skills a yr or more behind their peers. Family Strengths • Questions looking for strengths • Reframing Exercise Worksheet • Simple questions for family strengths inventory Steps in Case Management Process • • • • • • • • • 1. Request 2. County Response 3. Review Eligibility 4. Determine Eligibility 5. Case Manager Assigned 6. Complete functional assessment 7. Complete IFCSP 8. 90 IFCSP Review 9. Ongoing Review 400C - Rule 79 Children's Mental Health Formatted 06/27/06 Placement Resources • Consider all possibilities of community and inhome services prior to placement – don’t forget to check about the family’s insurance coverage. • Check with your supervisor regarding your county’s placement process and agency contacts • For additional placement resources contact the MN-DHS Licensing Division for a list of licensed facilities #651-296-3971 405 - Intervention Services Page 3 of 5 Family Trust • Open and honest Observation Strategies for Indicators of Family Violence • Review the handout, add those that experience have taught you • Clear in explanations • Listen with your eyes, ears and physical sense • Protecting Families Involved in Domestic Violence • Case Study Review • What do you see that would indicate trouble or not trouble? Services for Children • IDEA • PL 94-192 • MNDOE Handouts – Mental Health – Emotional and Behavioral Disorders – Current Topics 400C - Rule 79 Children's Mental Health Formatted 06/27/06 IDEA PL 94142 • 1975 – Ensured FAPE for children with disabilities – Outlined Due Process – IEP • 1983 – Transition Models – Outcomes 405 - Intervention Services Page 4 of 5 IDEA • 1990 – Transition and post school • 1997 – Family determination in planning – Short and long term goals – Transitional Planning expanded IIIP Document • • • • ISP CAC CADI TBI IEP IFSCP IFSP ICSP Multi-agency care Section 504 IIIP • MNDOE Handout Section 504 • Forms • MNDOE Handout Decision Tree • Guidebook • Overview Transition Planning • Regulations • Resource Planning 400C - Rule 79 Children's Mental Health Formatted 06/27/06 Review your case study • What would be focus of IEP/IFCSP with present age? • Fast forward to 16, how would transition planning start? 405 - Intervention Services Page 5 of 5 Reflecting On Our Cultural Competence Cultural Competence Self Assessment (1 = Strongly Agree; 5= Strongly Disagree) 1 2 3 4 5 6 7 8 9 10 11 12 The differences in how people of various cultures go about meeting their common basic needs as important as the similarities. Each culture finds some behaviors, interactions, or values more important or desirable than others. In the helping process, awareness and acceptance of differences in communication, life view and the definition of family are critical to successful outcomes. To fully appreciate cultural differences, workers must recognize the influence of their own culture on how they think and act. Minority families may exhibit behaviors, which are adjustment reactions to dealing with a hostile environment. When a worker of one culture interacts with a family from another culture, both will bring to the interaction the influence of current political or power relationships between the two groups. Knowing how primary support networks are configured in a family’s culture adds a critical dimension to the helping process. Because of the diversity within groups, the average worker cannot achieve comprehensive knowledge. More important than knowing all of the details about a child’s cultural or ethnic group is knowing where or how to obtain the necessary detailed information for use in specific cases. One way the case manager can adapt or adjust the helping process is to incorporate alternative culturally-enriching experiences. It is important to be sensitive to the fact that we are delving into other lives – their private spaces. The majority culture often assumes that some behaviors, interactions and values are shared by everyone. 400C – Rule 79 Children's Mental Health Formatted 06/27/06 1 2 3 4 5 405 – Intervention Services Page 1 of 1 Samples of Age Appropriate Assessment Tools 1. PECFAS: Preschool and Early Childhood Functional Assessment Scale (designed for use with children from the ages of 4 through 7). Latest version: 1994. Copy Righted. 2. CAFAS: Child and Adolescent Functional Assessment Scale, Latest version (designed for use with children from ages 7 through 17). Latest version: 1997. Copy Righted. http://www.mhsip.org/library/pdfFiles/CHILDANDADOLESCENTFUNCTIONALASSESSMENTSC ALE.pdf 3. CBCL: Child Behavior Checklist (AKA: the Achenbach) (for ages 6-18). Latest Edition: 2001. Copy Righted. www.ASEBA.org 4. CASII: Child and Adolescent Service Intensity Instrument. Free downloadable. http://www.aacap.org/clinical/CASII/ 5. SDC: Strengths and Difficulties Questionnaire. Downloadable in 50 languages. http://www.sdqinfo.com/ 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 1 Sample Individual Family Community Support Plan (IFCSP) CHILDREN’S MENTAL HEALTH CASE MANAGEMENT SAMPLE Individual Family Community Support Plan Imma Cool CMH-Rule 79 Client Name: Workgroup Current Diagnostic Assessment Date: Client ID # #### 10.15.04 Minimum 1x face to face per month Contact Frequency Date Case Manager 11.30.04 Stacy Bro Dates CAFAS Completed 1) 3) 5) 11.27.04 2) 4) 6) Current Diagnosis Axis I: Major Depression, ADHD Axis II: Deferred Axis III: No active medical problems Axis IV: Psychos social stressors related to family, school and social Axis V: 60 Initial CAFAS YOUTH’S FUNCTIONING School Performance: Home Performance: Community Performance: Behavior Towards Others: Moods / Emotions: Self-harmful Behavior: Substance use: Thinking: 8 Scale Scores Total of Scales: 90 Current CAFAS CAFAS 8 Scale Scores 20 10 20 20 10 0 10 0 Initial CAFAS Current CAFAS Enter “Yes” if this area was scored on CAFAS YOUTH RISK BEHAVIORS Suicidal / Attempted: (119, 144) Harmful to Self or Others: (142 – 145) Aggression: (3, 4, 43, 68, 89) Sexual Behavior: (69, 77, 90) Firesetting: (71, 78) Psychotic or Organic Symptoms: (182- 186) no no yes no no no no no no no no no 0 CLIENT’S RIGHTS Tennessen Warning has been given verbally and in writing and signed by client. Client’s rights under rule 79 pertaining to case management services have been explained or reviewed annually. Client’s right to appeal has been explained or reviewed annually or as requested. The following signatures indicate participation in the development and content of this interagency plan. Child/Youth: IFCSP Date Initials IFCSP Review Date Initials Parent: Parent: Case Manager: Supervisor: Mental Health Professional: Other: Other: Other: 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 2 Client Name: Imma Cool Needs/Outcomes Goals Imma will have a successful school year Imma will learn personal safety skills Imma will be active at home and with peers using age appropriate behaviors Strategies/Activities/Services Who By When? (How will you know goal is met?) Imma will attend school daily with no unexcused absences Case Management Stacy Bro Review in 6 mos. There will be no incidents of Imma hurting someone else or himself at school Anger management skills and social skills training Individual therapy addressing how Imma views and manages his relationships with adults Ralph Gruhlke Immediately Imma will improve his academic performance evident by better grades and positive teacher reports. Family therapy will address the relationship between Imma and his family with intent of developing family rules and discipline procedure which better meets Imma’s needs. Gina Dilly Current Imma will respect adults at school. This will be measured by no “notes” or phone calls home to his mother regarding negative interaction. Medication management Jane Buffie On-going Dr. Hennessey On-going Case management will assist Imma in developing relationship with fire personnel that can impart knowledge regarding fire safety and chemical safety. Stacy Bro Immediately Imma will understand the harmful effects of playing with fire and the ramifications of such. Imma will not use other household chemicals to play with. Anger management skills and social skills training Ralph Gruhlke On-going Individual therapy addressing personal safety and self – esteem issues. Gina Dilly On-going Imma will know and understand the potential harmful side effects of using such items Imma will decrease the amount of time he isolates. Medication monitoring Dr. Hennessey On-going Case management will actively participate in family therapy sessions as necessary. Stacy Bro As requested or necessary Imma will initiate and respond proactively to communication with his family and pro-social peers. Family therapy will address the communication within the family in order to assist Imma in developing appropriate communication skills as well as other family members. Jane Buffie On-going Imma will continue to be involved in sports such as football and hockey. Case manager will develop communication with the sports coach in order to monitor progress, attendance and assist with problem solving if necessary. Stacy Bro On-going Imma’s oppositional behavior with teachers will decrease. This will be measured by the teacher being able to manage his behavior with suggestions and reminders. Imma will not play with fire. This includes having possession of matches or lighters 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 Status 405 - Intervention Services Page 2 of 2 Family Systems Theory Structural Components of Family Systems Theory Subsystems This theory emerged from General Systems Theory by scholars who found it had many applications to families and other social systems. Any system is defined as a bounded set of interrelated elements exhibiting coherent behavior as a trait. (Constantine, 1986). Another definition is an assemblage of objects related to each other by some regular interaction or interdependence (Webster). Families are considered systems because they are made up of interrelated elements or objectives, they exhibit coherent behaviors, they have regular interactions, and they are interdependent on one another. The Components of Family Systems Theory are as follows: Family Systems… Have interrelated elements and structure. The elements of a system are the members of the family. Each element has characteristics; there are relationships between the elements; the relationships function in an interdependent manner. All of these create a structure, or the sum total of the interrelationships among the elements, including membership in a system and the boundary between the system and its environment. Interact in patterns. There are predictable patterns of interaction that emerge in a Family system. These repetitive cycles help maintain the family’s equilibrium and Provide clues to the elements about how they should function. Have boundaries and can be viewed on a continuum from open to closed. Every system has ways of including and excluding elements so that the line between those within the system and those outside of the system is clear to all. If a family is permeable and vague boundaries it is considered “open.” An open boundary system allows elements and situations outside the family to influence it. It may even welcome external influences. A closed boundary system isolates its members from the environment and seems isolated and self-contained. No family system is completely closed or completely open. Function by the Composition Law: the Whole is More than the Sum of Its Parts. Every family system, even though it is made up of individual elements, results in an organic whole. Overall family images and themes are reflected in this holistic quality. Unique behaviors may be ascribed to the entire system that does not appropriately describe individual elements. Use messages and rules to shape members. Messages and rules are relationships agreements which prescribe and limit a family members’ behavior over time. They are repetitive and redundant. They are rarely, if ever, explicit or written down. They give power; they induce guilt; they control or limit behaviors; and they perpetuate themselves and reproduce. Most messages and rules can be stated in one or a few words. For example, More is good, Be responsible, and Be Perfect are all examples of messages/rules. Have subsystems. Every family system contains a number of small groups usually made up of 2-3 people. The relationships between these people are known as subsystems, coalitions, or alliances. Each subsystem has its own rules, boundaries, and unique characteristics. Membership in subsystems can change over time. 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 1 Rules to Build Genograms Although there is general agreement on the basic genogram structure and symbols, there are some variations from one author to another. Some authors do reuse the same symbol for different situations while others have ignored such special cases. Basic Genogram Symbols The male is noted by a square and the female by a circle. A family is shown by a horizontal line connecting the two. The children are placed below the family line from the oldest to the youngest, left to right. Although this may sound obvious, it will be very important to remember these rules when the situation becomes a bit more complex. The following case is a husband with three spouses. The husband had three children with the first wife, and then divorced. The husband married the second wife, had one child and separated. The husband currently lives with another woman. As you can see, the oldest child is at the left, and the youngest child, "Half Sister", is at the right of her family, as she is the unique child of the husband and the second wife. A husband with multiple spouses Reversing the scenario where the wife had multiple husbands, we get the following genogram: A wife with multiple husbands 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 1 PACER Center Parent Advocacy Coalition for Educational Rights PACER Center E-mail Directory Projects Related to Transition FEATURED RESOURCES National Standards for Secondary Education and Transition for All Youth National organizations and experts representing general education, special education, workforce development, youth development, and families have developed a set of national standards of effective practice and quality indicators to improve secondary education and transition for all youth. The result, National Standards for Secondary Education and Transition for All Youth, is now available on the NCSET Web site: • • HOME WHO WE ARE LINKS National Standards in PDF http://www.ncset.org/teleconferences/docs/NASETFramework.pdf (350k, 13pgs) National Standards in MS Word http://www.ncset.org/teleconferences/docs/NASETFramework.doc (68k, 14pgs) THE FAMILY AS A CRITICAL PARTNER IN THE ACHIEVEMENT OF A SUCCESSFUL EMPLOYMENT OUTCOME. Check out new Parent Briefs developed by PACER in collaboration with the National Center on Secondary Education and Transition (NCSET) on Postsecondary Education, Supplemental Security Income, and other transition issues! PUBLICATIONS CONTACT US TRANSLATED MATERIAL PACER Projects Focusing on Transition National Technical Assistance Projects • NATIONAL INFORMATION • IDEA 1997 GUEST BOOK • TATRA (Technical Assistance on Transition and the Rehabilitation Act) This national project provides training, information and materials to parent center staff across the country who are helping the families of youth with disabilities learn about transition, independent living and vocational rehabilitation services. The National Center on Secondary Education and Transition PACER works with this national technical assistance project headquartered at the University of Minnesota to connect parents and youth with disabilities to information and resources. PACER manages a listserv and develops material for parents as part of the Center's technical assistance activities. National Post-School Outcomes Center PACER works with this national technical assistance project headquartered at the University of Oregon to inform parent centers and family advocates how post-school outcomes studies can be used to help shape more effective transition programs that better prepare youth for further education, employment and independent living. 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 2 For Minnesota Families • • • • Connecting Youth to Communities and Careers (Project C3) is an exciting collaborative project with the Minnesota Department of Employment and Economic Development to demonstrate how innovative partnerships with community organizations can improve local transition services and outcomes for youth with disabilities. As a key partner, PACER's role is to: o provide Minnesota families with training and information to help transition-age youth with disabilities prepare for and find meaningful, gainful employment o provide training to help Minnesota youth programs funded by the Workforce Investment Act to better serve youth with disabilities o facilitate state planning, communication and collaboration efforts across funding streams and agencies o develop a comprehensive Resource Map of Minnesota's youth service delivery infrastructure to inform Minnesota families, professionals and policymakers PACER's Parents Helping Parents Program provides workshops, one-on-one training and information to Minnesota families on a range of special education and other related topics, including transition. PACER's Perkins Project provides training and information to families and professionals focusing on improving transition outcomes for Minnesota youth with emotional behavioral disabilities and youth with disabilities in the state's juvenile justice system. Project PRIDE (PACER's Rehabilitation Act Information & Disability Education) provides information and training for Minnesota youth with disabilities, their families, and professionals about the Rehabilitation Act. Additional PACER Projects Inclusive of Transition Topics National Technical Assistance Projects • • The Alliance (Technical Assistance Alliance for Parent Centers) PACER is the national coordinating office for consultation and technical assistance on special education and related disability issues for 100 federally funded parent centers across the country. The Families and Advocates Partnership for Education (FAPE) PACER serves as the national coordinating office for a federally funded partnership linking families and advocates with researchers and policymakers. Its focus is the implementation of IDEA '07 Amendments, including its transition requirements. For Minnesota Families • • • • The Simon Technology Center introduces youth with special needs, their parents and teachers to educational software and special equipment to make computers accessible tools for communication, learning, employment, and independent living. It includes a software lending library. PACER's Health Information and Advocacy Center provides information about the health care system, resources, and advocacy to families of Minnesota youth with special health needs and disabilities. The Juvenile Justice Training Program trains professionals to identify the needs of youths whose disabilities may place them at risk for involvement with the justice system. The Project for Parents of Children with Emotional / Behavioral Disorders (EBD) offers assistance on education, social services, mental health or corrections issues for parents of youth with EBD in Minnesota. http://www.pacer.org/tatra/ 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 2 of 2 Family Strengths Assessment Scales A review of the family strengths literature identified four instruments that measure a subset of or all of the qualities of strong families listed above. Each of these scales is briefly described next. The use of self-report family strengths scales as part of family-centered assessment and intervention practices is described in a subsequent section of the article. Family Strengths Inventory (Stinnett & DeFrain, 1985b). This scale includes 13 items that measure six major qualities of strong families and a number of aspects of the interpersonal relationships among family members. The six qualities include commitment of family members to promoting each other's welfare and happiness, appreciation for each other on a frequent basis, communication skills used by family members, spending time together doing things important to the family, a sense of spiritual wellness that gives the family strength and purpose, and the ability to cope with stress and crisis in a way that provides the family an opportunity to grow. Other scale items assess the degree of closeness, happiness, confidence, and worthiness in the relationships among family members. Each item is rated on a five-point rating scale, based on the degree to which the quality or characteristic is present in the respondent's family. The scale yields a total score that provides a basis for determining the overall presence of family strengths. However, it is the individual responses to the 13 scale items that are most useful for determining family functioning style (see below). Family Strengths Scale (Olson, Larsen, & McCubbin, 1983). This scale includes 12 items that assess two dimensions of family functioning: family pride (loyalty, optimism, and trust in the family) and family accord (ability to accomplish tasks, deal with problems, and get along together). For each item, the respondent indicates the extent to which the quality is present in his or her family. The scale items measure many of the qualities of the two dimensions described above, and provide a basis for establishing which qualities are characteristic of the respondent's family. Family Hardiness Index (McCubbin, McCubbin, & Thompson, 1987). This scale includes 20 items that assess the internal strengths of families and how those strengths are used to both control life events and hardships and produce positive changes and growth in the family unit. Each item is rated on a four-point rating scale in terms of the degree to which each statement is true for the family. The items are organized into four subscales: coordinated commitment (internal strengths, dependability, and ability to work together); confidence (family's sense of being able to plan ahead and of being appreciated for individual efforts, and the ability to endure hardships); challenge (efforts to be innovative, be active, and to experience new learning opportunities); and control (being able to control important aspects of life). Family Functioning Style Scale (Deal, Trivette, & Dunst, 1988). This scale includes 26 items and was designed to assess all 12 qualities of strong families listed above. The instrument was developed as part of a family-centered assessment and intervention model (Dunst, Trivette, & Deal, 1988) that evolved from efforts to intervene in ways that support and strengthen family functioning. The scale assesses the extent to which an individual family member, or two or more family members, believes her or his family is characterized by different strengths and capabilities. Each item is rated on a fivepoint rating scale by noting the degree to which the 26 statements are "Not-At-All-Like My Family" to "Almost-Always-Like My Family". (The items on the scale are listed in Table 1.) Of the four family strengths scales, the Family Functioning Style Scale is the most comprehensive in terms of the range of qualities it attempts to measure. The scale was specifically developed to tap positive aspects of family functioning consistent with the five themes described above. Evidence regarding the reliability and validity of the scale is described next. 400C – Rule 79 Children's Mental Health Formatted 06/27/06 405 – Intervention Services Page 1 of 1 Reframing Exercise Worksheet Deficiency Chaotic family, few rules Reframe Energetic family who could benefit from structure and focus Grandma is authoritarian Respect for elders Missing or late Learning schedules, appointments, using written reminders uncooperative could improve the follow through for this family The children run the A child focused family. show. Parents could improve child experience with parenting classes and attitude Your examples: 400C – Rule 79 Children's Mental Health Formatted 06/27/06 Family Response Hopelessness Curiosity 405 – Intervention Services Page 1 of 1 Grandma’s Child Tanya, age 4, was seen for assessment in a clinic at the request of her grandparents. Tanya was the only child of parents who were longtime heroin users. Several months ago, not having seen Tanya or her parents for several years, the grandparents were called by child protection in another state and informed that Tanya's parents had been arrested and she had been placed in foster care. Soon thereafter, when Tanya came to live with them, the grandparents noticed that she did not have the verbal skills of a normal four-year-old child. She had marked problems with social interaction. She often seemed oblivious to ordinary invitations to hug or play with her grandparents and other relatives. She also exhibited a rapidly alternating mixture of responses in which sometimes she seemed to want to get very close to people, and otter times would push them away. The grandparents later learned that since she was an infant, Tanya had often been left with various friends of her parents, man of whom were themselves heavy drug users and often they were minimally attentive to her. On examination, Tanya was found to have mild language delays and marked problems in social interaction. She tended to avoid interaction or when it could not be avoided, became very anxious and disorganized. Spitzer, R., Givvon, M., Skodeol, A., Williams, J., First, M., (1994). DSM IV Casebook. Washington DC, American Psychiatric Press. 400C - Rule 79 Children's Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 1 Observation Strategies for Indicators of Family Violence (From: Reporting Child Abuse and Neglect: A Resource Guide For Mandated Reporters by Child Safety and Permanency Division, Minnesota Department of Human Services, October, 2004) The parents of an abused or neglected child may exhibit some of the following behaviors or characteristics: • They seem isolated from family supports such as friends, relatives, neighbors and community groups • They discourage social contacts or consistently fail to keep appointments or participate in school activities or events • They seem to trust no one • They may have been abused or neglected as children • They are often reluctant to give information about the child’s injuries or condition • When questioned, they offer an explanation that is inconsistent with the injury or offer contradictory explanations for the injury or are unable to explain the injuries • They respond inappropriately to the seriousness of the child’s condition either by overreacting, seeming hostile or antagonistic when questioned, or showing little concern or awareness of the child’s condition • They may refuse to consent to a medical evaluation • They may delay or fail to take the child for medical care, including routine checkups • In taking an injured child for medical care, they may choose different hospitals or doctors to prevent the injuries from being recognized as a pattern of abuse • They may be too critical of the child and seldom, if ever, discuss the child in positive terms • They may have unrealistic expectations of the child, expecting or demanding behavior that is beyond the child’s age or ability • They may believe in the necessity of harsh punishment for children • They seldom touch or look at the child, ignore the child’s crying, or react with impatience • They sometimes keep the child confined for long periods of time in a crib or playpen • They may lack understanding of the child’s physical, emotional, and psychological needs • They may misuse alcohol or drugs • They appear to lack self control or fear losing control over the family. 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 1 Does the student have an IEP and/or 504 Plan? See A Quick Reference for Accommodations available to all students No Yes Consider the instructional accommodations that the student receives in class and the accommodations for statewide assessments that have been written into the student's IEP Several options may apply for statewide testing No accommodation required 400C – Rule 79 Children's Mental Health Formatted 06/27/06 Special order accommodations that apply, including: • Math script or CD • 18/24 pt. font • Braille Arrange for any additional accommodations that apply If accommodation doesn't appear on A Quick Reference for Accommodations, e-mail mde.testing@state.mn.us for guidance. Student takes alternate assessment – see Flowchart for Decisions: IEP & 504 Teams 405 - Intervention Services Page 1 of 1 Highlights of Federal Education Programs For Children With Mental Health Problems Individualized Education Program – For children age 3 through high school, school districts use the Individualized Educational Program (IEP) as a tailor-made program which fits each child’s needs and abilities. The IEP is drawn up at a special IEP conference or staffing. The IEP is a based on an evaluation of the child. Individuals With Disabilities Education Act (IDEA) – This act raises academic expectations and accountability for children disabilities, increases parent involvement in the education of their children, and ensured that regular education teachers are involved in planning assessing children’s progress. Section 504 – For children with a physical or mental impairment, schools have a responsibility to provide a free, appropriate public education to persons with disabilities. The school needs to made reasonable accommodations to programs and facilities to make the education happen. Vocational and adult education programs – Each school district offers a variety of vocational and adult education programs for persons with disabilities. Check with your local school district. 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 1 http://education.state.mn.us/mde/Accountability_Programs/Compliance_and_Assistance/Special_Education_Monitoring/Monitoring_Resources/Individual_Interagency_Intervention_Plan_(IIIP)/index.html 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 1 http://education.state.mn.us/mde/Accountability_Programs/Compliance_and_Assistance/Section_504_of_the_Rehabilitation_Act/index.html 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 1 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 2 http://education.state.mn.us/mde/Learning_Support/Special_Education/Birth_to_Age_21_Programs_Services/MN_State_Interagency_Coord_MnSIC/index.html 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 2 of 2 http://education.state.mn.us/mde/Learning_Support/Special_Education/Categorical_Disability_Information/Emotional_and_Behavioral_Disabilities/index.html 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 1 http://education.state.mn.us/mde/Learning_Support/Special_Education/Birth_to_Age_21_Programs_Services/Mental_Health/index.html 400C – Rule 79 Children’s Mental Health Formatted 06/27/06 405 - Intervention Services Page 1 of 1 http://education.state.mn.us/mde/Learning_Support/Special_Education/index.html 400C – Children’s Mental Health Formatted 06/27/2006 405 - Intervention Services Page 1 of 1 http://education.state.mn.us/mde/Learning_Support/Special_Education/Birth_to_Age_21_Programs_Services/Secondary_Transition/index.html ________________________________________________________________ Table of contents for Chapter 245 245.4875 Local service delivery system. Subd. 8. Transition services. The county board may continue to provide mental health services as defined in sections 245.487 to 245.4887 to persons over 18 years of age, but under 21 years of age, if the person was receiving case management or family community support services prior to age 18, and if one of the following conditions is met: (1) the person is receiving special education services through the local school district; or (2) it is in the best interest of the person to continue services defined in sections 245.487 to 245.4887. HIST: 1989 c 282 art 4 s 42; 1990 c 568 art 5 s 14,34; 1991 c 94 s 7,24; 1991 c 292 art 6 s 58 subd 1; 1995 c 207 art 8 s 7,8; 1999 c 86 art 1 s 58; 1Sp2001 c 9 art 9 s 13; 2002 c 379 art 1 s 113; 1Sp2003 c 14 art 11 s 11; 2005 c 10 art 1 s 43; 2005 c 98 art 3 s 12,13 http://www.revisor.leg.state.mn.us/stats/245/4875.html 400C – Rule 79 Children’s Mental Health Formatted 06/27/2006 405 - Intervention Services Page 1 of 1 Major Components of IFCSP Signatures On Plan, Copies Provided To. . . Goals, Objectives, Tasks/Strategies Who Does What, How Often, Expected Outcome Demographic Information of Child, Family, Providers Individual Family Community Support Plan Time lines &results of Diagnostic Assessment & Functional Assessment Strengths Resources Assets (CAFAS, CBCL) Problems Needs Safety Stabilization Crisis Plan 400C – Rule 79 Children’s Mental Health Formatted 06/27/2006 Concerns Service Providers Names, address, telephone 405 - Intervention Services Page 1 of 1 http://www.c3mn.org/ 400C – Rule 79 Children’s Mental Health Formatted 06/27/2006 405 - Intervention Services Page 1 of 1 Independent Living Skills Competencies Assessment 1. The worker can engage youth in assessing their readiness for transitioning from care to living independently. 2. The worker is able to assess the adolescent’s level of ability in critical skills needed for independent living including problems that may interfere with their transition from out of home placement to living independently. 3. The worker knows the stages, processes of normal physical, cognitive, social, emotional, and spiritual development of adolescence. 4. The worker understands the impact abuse and trauma on normal development and knows the signs and indicators of special needs such as mental retardation, autism, learning disabilities (all types), attention deficit disorder, etc., and is able to assess the developmental needs of the adolescent. 5. The worker can utilize data from psychological or developmental assessments, youth self-assessments, clinical interviews, direct observations, and personal interactions to determine a youth’s strengths, areas of potential vulnerability, mental health, and independent learning needs. 6. The worker is able to use knowledge of the youth’s culture in a sensitive manner to help develop relationships, to stimulate development, to manage behavior appropriately and to promote and integrate the cultural heritage of the youth into their independent living plan. 7. The worker is constantly aware of their personal expectation for the youth and ensures that this is congruent with the youth’s potentially skill level. Role Identification 8. The worker is able to engage parents by using strength based approach to assist in the development of an independent living plan for their adolescent foster child. 9. The worker is able to engage parents as a team member and support their efforts to get their youth ready to live independently. 10. When working with parents, the worker models appropriate behavior in how to engage adolescents. 11. The worker understands the importance of being honest with youth about their current living situation and assisting the youth with the transition from being institutionalized or dependent on others to feeling independent. Community Supports 12. The worker is able to identify and connect youth with informal resources within their community. 13. The worker is knowledgeable about community resources such as Workforce centers, Section 8 housing, Property Management Companies, CAP agencies, various church groups etc., and has established relationships with these agencies to assist youth in connecting with their community. 14. The worker is aware of community resources such as the Department of Rehabilitation Services (DRS) that can assist adolescents with special needs. 15. The worker can help youth identify the types of relationships they want with significant people in their lives, including birth family, foster family, extended family, and friends. 16. The worker understands the importance of support systems for the emancipating youth, and can use a variety of techniques to help the youth build those support systems. Intervention Strategies 17. The worker can engage youth in developing a high quality Independent Living Skills plan and evaluate his / her progress in completing goals. 18. The worker is able to set realistic and achievable goals and objectives, identify learning activities and teaching strategies, set time frames for completion of activities, and formulate an individualized independence plan for a youth. 19. The worker can use techniques such as teaching, modeling, coaching, and positive reinforcement to help youth prepare for independent living. 20. The worker knows the importance of using daily situations as teachable moments in the process of teaching independent living skills. 21. The worker understands that developmentally adolescents have the mind set of only living for today and the value of teaching skills by letting youth feel the natural consequences for their behavior. 22. The worker understands that youth’s self-esteem improves when they have learned a new skill or mastered an existing one. 23. The worker will assist youth in creating a file of important documents that they will need when leaving care. These can include Social Security Card, Driver’s License, Insurance Cards, Foster Care paperwork etc. 400C – Rule 79 Children's Mental Health Formatted 06/27/2006 405 - Intervention Services Page 1 of 2 24. The worker understands the Workforce Investment Act – WIA and the services that could benefit youth preparing to transition from care. 25. The worker is knowledgeable about Support and Emancipation for Living Functionally (SELF) funding and the basic guidelines and procedures for accessing funds. Skills • • • • • • • • • • • • • • • • • • • • • How to engage youth in plans How to write quality plan: include youth in process, making it fun Engaging parents in entire process ¾ Support parents ¾ Strengths based ¾ Their role on team ¾ Expectations ¾ Modeling ¾ How they can help Connecting youth with formal and informal resources – “Team” Assessments for youth ¾ Needs ¾ Developmental Level ¾ MH ¾ Have kids demonstrate skills Teaching kids follow through, not only living for today Teaching kids to withhold judgment Understand workers personal expectations of where youth can go Create important document folder (SS card, driver’s license, insurance card, foster care paperwork) Let kids suffer the consequences Strengths based and skill assessments Honesty Identifying the teachable moment and know what to do (ex. pick up what foster parent is missing or not willing to do) Integrating life skills through time with child – even at a younger age Integrate worker skills with community resources Make a personal connection with needed resources in the community Need workers to understand where the youth is at and be at their level – make no assumptions o developmentally (assessments, interview skills, checklists) o emotionally o view of the world – living for today Time frame: process is on-going and personal – it will take time. Youth’s timeline Overcoming institutionalization, dependency, sense of entitlement Awareness of how kids learn: lecture vs hands on/experiential. Kids can to do it themselves – with some help. Workers can set this up. Kids self-esteem improves with mastery or understanding new skills Knowledge • • • • • • • • Know resources available – workforce centers, etc. Build relationships with these agencies Basic knowledge of specific populations – or at least familiar with resources (Department of Rehabilitation Services – DRS) ¾ Developmental disabilities ¾ Mental health ¾ Learning disabilities Awareness of waiting lists Workforce Investment Act – WIA Federal Funds Funding available and procedures involved to utilize (Darcy) Knowledge/info about SELF funding and process – basic guidelines and procedures 400C – Rule 79 Children's Mental Health Formatted 06/27/2006 405 - Intervention Services Page 2 of 2