draft outline of autism proposal
advertisement

Autism Services Proposal
SJR 567
1
AUTISM SERVICES PROPOSAL for the Tennessee Legislature
12/20/2002
I. Executive Summary
As a response to Senate Joint Resolution 567, an interdepartmental work group met between
September and December 2002 to study the current service system for children with Autism
Spectrum Disorders (ASD) and their families, and to make recommendations regarding an
improved service system for Tennessee children with ASD. The workgroup met also with
parents and providers of children with ASD. The combined groups created a plan for
Tennessee that will:
Generate better outcomes for children with autism and their families
Reduce overall, long-term costs by providing effective services early and intensively
Minimize legal risk exposure for the state of Tennessee
Definition of Autism Spectrum Disorders
Autism Spectrum Disorders (ASD) are a group of five related neurobiological developmental
disorders that profoundly affect a person’s ability to communicate, form relationships with
others, and respond appropriately to the environment. The onset of autism occurs in early
childhood and impairments are evident throughout the person’s lifespan. Manifestations of the
disorder vary widely. For example, some persons are nonverbal while others have limited or
adequate speech. The majority of persons with ASD are mentally retarded. ASD presents
serious challenges to affected individuals and their families, as behavior is often highly
problematic (e.g., self-harm) and tends to require high levels of supervision.
Autism is the fastest-growing developmental disability (Autism Society of America, 2002).
The prevalence of ASD in the population is not known with certainty, with ranges from 2-6
per 1,000 reported in most studies. Research for this proposal led the workgroup to use a
prevalence estimate of 2-3 per 1,000. For Tennessee, this yields an estimate of 3,200 to 4,800
children ages 0-21. Incidence rates of reported autism are on the rise nationally and certainly
reflected in Tennessee school numbers. The number of Tennessee public school children
(ages 3-22) within Special Education with a primary autism diagnosis has risen almost fivefold from 1992 to 2002. This number is sure to continue to rise as Tennessee schools, as of
July 2002, now consider a child with any form of ASD (not just autism) as eligible for Special
Education.
Effective Intervention
Early intervention is the key to improving the conditions associated with autism (Guralnick,
1998; Lovaas, 1987; McEachin, Smith, & Lovaas, 1993). Children with ASD can improve
with appropriate early, intensive behavioral intervention that is consistent across the home and
Autism Services Proposal
SJR 567
2
school settings. Treatments such as speech and language therapy and occupational therapy
combine with intensive behavioral therapy to ameliorate the difficult symptoms of ASD, to
improve communication, and to advance some children to normative functioning. However,
the intervention must be early and intensive to be fully effective. Children cannot regain lost
developmental time. Early and intensive treatment is dependent on early, accurate screening
and diagnosis, a network of providers with autism expertise, accessibility to services, and
funding for services. Evidence-based behavioral intervention models and educational models
exist for treating children with autism and should always be the choice of intervention (e.g.,
Dawson & Osterling, 1997; McEachin, Smith, & Lovaas, 1993).
Tennessee’s Existing System
Tennessee’s existing system for ASD is inadequate. The areas of greatest concern are:
A limited network of trained professionals in the area of autism in:
• Primary care physicians
• Educators
• Mental health professionals
• Behavioral interventionists
• Health related professions such as speech/language and occupational therapy
Lack of insurance coverage for autism by both public and private insurance
• TennCare excludes ASD as a covered diagnosis for behavioral health
• Private insurance often excludes ASD for even routine medical care
Lack of family support services (e.g., respite care; home modifications)
Inadequate early intervention services
Inadequate educational services
Inadequate long term care options
A fragmented service delivery system
Costs
The cost associated with caring for persons with ASD is an estimated $4.5 million per person
over a lifetime (Jarbrink & Knapp, 2001); however, most of these costs are for adult services,
due partially to a lack of early, effective treatment. Costs are high due to the need for
intensive levels of supervision and the cost of specialty services often over many years.
Tennessee costs for children with severe ASD are heightened due to sending children to other
states for care, lack of a network for less expensive home-based treatment, and lawsuits
against the state related to care for children with autism. Researchers have speculated that,
with early intervention, cost avoidance could be as substantial as lifetime savings of
$656,000-$1,082,000 per person (Jacobson, Mulick, and Green, 1998).
Immediate Actions Needed
Tennessee must assure its families and children with ASD of appropriate services and
mechanisms to ensure those services. Tennessee must:
Autism Services Proposal
SJR 567
3
Assure early identification, accurate diagnosis and treatment planning capacity
across all regions by funding regional diagnostic/consultation centers
Create a coordinated system of autism-specific services with expert providers
Provide access to individualized home-based intensive behavioral intervention
Implement evidence-based, intensive early intervention strategies across all
Tennessee systems in order to capitalize on the benefits of early intervention for
children birth to age eight.
Ensure year round school options for all students, as appropriate to their needs
Ensure developmentally appropriate educational strategies and transition plans for
older children (ages 8-22) (See pp. 22-24 for appropriate educational components)
Assure that every school district receives training and support for educators and
related professionals
Establish statewide capacity to constantly improve knowledge, practice and costeffectiveness
Measure improved outcomes as defined by each child’s IEP
Create a clear oversight plan to ensure an effective system
Create a clear funding plan for ASD services
Proposed Solutions
The workgroup proposes that a new model for ASD service delivery be implemented in order
to reach these goals. See page 31 in this document for the organizational chart. The plan
builds upon many existing structures, making it cost effective and integrative. The model
includes:
A Tennessee Center for ASD
Five regional ASD Centers of Excellence
Eight regional education ASD teams
A plan for oversight of this system
A plan for an advisory council to this system
The Tennessee Center for ASD would uphold research, training, and information
dissemination functions. The Tennessee Center for ASD would build on the current Treatment
and Research Institute for Autism Spectrum Disorders (TRIAD) at Vanderbilt University.
The Tennessee Center for ASD would ensure the training of educational and health-related
providers statewide, as well as keeping the state abreast of current ASD knowledge and also
contributing to knowledge through research.
The five regional ASD Centers of Excellence would function as diagnostic and consultation
centers, as well as providing family resource services and service liaison at the local level.
Some direct services in addition to diagnostic evaluations (such as medication management)
would be offered at the COEs. The five COEs would also be extenders of the TRIAD training
efforts, particularly with health-related professionals. The five COEs would be housed in the
existing Centers of Excellence for Children in State Custody at five tertiary pediatric centers
across the state.
Autism Services Proposal
SJR 567
4
The eight education ASD teams would function out of the eight Department of Education
(DOE) regions at the local school levels as extenders of the TRIAD training, as well as
providing consultation in the schools regarding children’s educational plans. Team members
would be employees of the DOE and would be supervised administratively through the three
grand regional offices.
The Tennessee Center would be highly collaborative with the five COEs and the eight ASD
education teams in the area of training professionals. The COEs, with their health-related
expertise, and ASD education teams would work closely together around individual children’s
plans and would act together as liaisons in both the home and school settings. This system
would monitor quality of children’s plans and the Tennessee Center would research the
effectiveness of the delivery model.
The proposed system would be overseen at the State level by an interdepartmental unit with
executive authority that would sit above individual departments and report to the governor’s
office.
This proposed organizational model provides:
an integrated system of services
trained professionals
diagnostic centers
quality assurance around evidence based treatment and optimal outcomes for
individual children
liaison service coordinators to guide individual families through the system
information and referral resources
direct educational and clinical consultation and services
Proposed costs and financial considerations
North Carolina operates a statewide autism services plan (Division TEACCH) that
encompasses the regional diagnostic and consultative concepts like the proposed Tennessee
model, but does not include the more extensive training, dissemination, and research features
of the Tennessee Center, the regional educational teams, or service liaison functions. NC’s
Division TEACCH has been in operation since 1972 by legislation and is funded annually
through legislated funds. This year’s budget draws $4,655,479 from state funds; the rest of
the operation is funded through Medicaid.
A rough estimate of cost for the more inclusive Tennessee model is $6,571,500. A
spreadsheet is located in Appendix I.
Funding for ASD services is complex. Several financial issues must be considered. It is
recommended that Tennessee:
Create a clear delineation of available funding sources from state, federal, and
private entities and ensure that Tennessee is drawing down all available funds from
federal and other sources
Autism Services Proposal
SJR 567
5
Clearly designate a person or entity that is in charge of authorizing funding once a
funding plan is designed
Conduct a thorough lifespan cost-benefit analysis of treating ASD in Tennessee
Consult with experts from other states that have statewide ASD service delivery
(e.g., North Carolina)
Consider various funding strategies such as:
♦ Use blended funding (e.g., DOE, DCS, DMRS, TennCare, DOH)
♦ Write a demonstration waiver for long term solutions to serving this population
♦ Create a collaborative waiver model with Education as the primary source of
services and funding, but in partnership with other funding sources such as
private and public insurance. Such a model has been designed in other states
and requires that families who are not Medicaid eligible must cooperate by
using their private insurance as a supplemental form of payment for services
♦ Create a funding unit for children with special health care needs, much like the
model already operation under TennCare Select for children in state custody
♦ Direct funds to the Tennessee Respite Coalition for ASD specific respite care
Final recommendations
The original broad goals of this study included:
Generate better outcomes for children with autism and their families
Reduce overall, long-term costs by providing effective services early and intensively
Minimize legal risk exposure for the state of Tennessee
In order to reach these goals, the state must ensure that there are adequately funded
services that will reach families and children with ASD. By providing evidence-based
treatments early in development, the state can save money over the long run. By
providing the right kinds of services and helping families afford these services, the state
will be less vulnerable to lawsuits around ASD services. While this document contains
much of our current understanding of ASD and of the services needs in Tennessee, there
are several next steps that must occur in order to best implement this plan. These steps
include:
Create a subgroup that examines more closely the financial aspects of this plan
Create an implementation task force for the plan; use some of the same committee
members whohave contributed thus far to the plan; draw on the faculty at TRIAD
and the staff at the current COEs; draw on the Autism Society of America
members
Make funds available in the Tennessee state budget for the plan
Discern the governmental “home” for the oversight of the plan
Autism Services Proposal
SJR 567
6
II. Background
Senate Joint Resolution 567 (Appendix A) required an interdepartmental study to propose a
comprehensive statewide plan for coordinating services and maximizing their delivery to
children with autism and their families. It is important to state that many persons with autism
continue to require services throughout their lifespans, and while the current resolution
requests a plan for children, a lifespan perspective should be considered as a next step to the
children’s plan.
Similarly, it should be noted that children with autism and children with other developmental
disabilities share many of the same essential needs for services. Though the current proposal,
in response to SJR 567, is focused on children with autism, much of it is applicable to children
with other developmental disabilities. Implementation of improved services for children with
autism should lead to similar improvements for children with other developmental disabilities.
SJR 567 directed that the departments of Mental Health and Developmental Disabilities,
Education, Children’s Services, the TennCare Bureau, and the Tennessee Commission on
Children and Youth participate in the interdepartmental study. At the request of the
Tennessee Commission on Children and Youth, with the concurrence of the Commissioners’
EPSDT Task Force, the Children’s Health Initiative in the Office of Health Services was
designated as the lead agency to convene representatives of the departments of state
government and others to develop the proposal required by SJR 567.
An interdepartmental work group convened initially on September 11, 2002, and met
regularly from then through December 2002 to develop the proposal to submit to the special
committee of the legislature as required by SJR 567. In addition, the Children’s Health
Initiative convened three other groups, which met on a less frequent basis, to provide
additional information related to children with autism. These groups were: 1) a group of
parents of children with autism; 2) a group of providers of educational, psychological, and
medical services for children with autism; and 3) a group of developmental and psychological
experts at Vanderbilt University’s Kennedy Center. Individual consultants who are experts in
autism were also contacted for this effort (see Appendix B for the full list of participants).
The Tennessee Developmental Disabilities Expansion Plan (June 2002) was considered as a
major process of state government, which forms a context for proposals to improve services
for children with autism and their families. The current proposal includes plans for relating
the needs of children with autism to the recently developed Developmental Disabilities
Regional Planning Councils.
III. Overall Goal of the Proposal
The goal of this proposal is to bear light on the complexities involved in autism and
corresponding service needs, to summarize the current situation in Tennessee regarding
services for autism, and to propose some solutions to bringing appropriate services to children
with autism and their families in Tennessee. This proposal offers solutions that will:
Autism Services Proposal
SJR 567
•
•
•
7
Generate better outcomes for children with autism and their families
Reduce overall, long-term costs by providing effective services early and intensively
Minimize legal risk exposure for the state of Tennessee
IV. Definition of Autism Spectrum Disorders
Autism is one of the pervasive developmental disorders, as described in the Diagnostic and
Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV, American Psychiatric
Association, 2000). Autism is a neurobiological developmental disability characterized by
impairment in three major areas:
•
•
•
Impairment in social interaction
Impairment in communication
Restrictive, repetitive, and stereotyped patterns of behavior, interests, and activities
The onset of autism occurs in the first three years of life and the impairments are evident
throughout the person’s lifespan, though manifestations may vary depending on age and
developmental status as well as severity. For example, about 50% of persons with autism
remain non-verbal or minimally verbal throughout the lifespan (Minshew & Rattan, 1992);
others develop adequate, although unusual, communication and speech. In addition, there is a
range of behavioral problems associated with autism that include hyperactivity, short attention
span, impulsivity, aggressiveness, self-injurious behavior, unusual responses to sensory
stimuli (such as hypersensitivity to certain sounds, fascination with certain visual stimuli, and
the like), abnormalities in eating, disturbances of sleep, excessive fearfulness, and
abnormalities of mood. These features are highly variable, ranging from mild to severe.
Autism frequently co-occurs with mental retardation. Approximately 70-75% of individuals
with autism also have mental retardation. Individuals with autism often have cognitive
problems even when the problems are not severe enough to meet the criteria for mental
retardation. Despite the high co-occurrence of mental retardation with autism, individuals
with autism vary widely in their intellectual abilities with some individuals having very low
abilities and some very high abilities.
Each of the Autism Spectrum Disorders (ASD) defined below, presents serious challenges to
affected individuals and their families. While most involve some degree of mental retardation
and often severe cognitive problems, all involve significant impairments in behavior, which
can present difficult challenges to family coping. Without intervention, the behavior
problems of children with ASD tend to be chronic and to severely limit their vocational and
life opportunities. With intervention, especially intensive, early intervention, many of the
behavioral problems associated with ASD can be ameliorated and the prognosis improved
(Dawson & Osterling, 1997; Hurth, Shaw, Izeman & Whaley, & Rogers, 1999; Strain,
Wolery, & Izeman, 1998).
Autism Services Proposal
SJR 567
8
The Autism Spectrum Disorders include Autism, Asperger’s Disorder, and Pervasive
Developmental Disorder Not Otherwise Specified (PDDNOS). Two other disorders which
are part of the spectrum of pervasive developmental disorders are Childhood Disintegrative
Disorder and Rett’s Disorder. For purposes of the current proposal, all five disorders are
collectively referred to as autism spectrum disorders (ASD). These conditions are described
in detail in the DSM-IV. Brief definitions of each are as follows.
•
Autism – impairments in social interaction, in communication, and in the range of
interests and activities; manifest by age 3.
•
Asperger’s Disorder – impairments in social interaction and in the range of
interests and activities but without a general delay in language; cognitive abilities
are not significantly delayed.
•
Pervasive Developmental Disorder Not Otherwise Specified (PDDNOS) –
includes "atypical autism", with late age of onset (after age 3), atypical symptoms,
or subthreshold symptoms with impairment in social interaction and either
impairment in communication or a restricted range of activities and interests.
•
Rett’s Disorder – a progressive disorder characterized by loss of early
developmental skills and loss of purposeful use of the hands and development of
stereotyped hand movements. This disorder has been found only in girls and is
quite rare.
•
Childhood Disintegrative Disorder – regression in multiple areas of development
after normal development in the first two years of life; this disorder is usually
associated with severe mental retardation, and is quite rare.
V. Prevalence
The prevalence of the autism spectrum disorders in the population is not known with
certainty. The Centers for Disease Control and Prevention (CDC) has been studying the
prevalence of autism spectrum disorders in a variety of locations, using several different
methods. Studies worldwide note the range of ASD to be from 2-6 persons in 1000. The
Metropolitan Atlanta Developmental Disabilities Surveillance Program has found that 2-3 of
every 1,000 children ages 3-10 have an ASD. Our work group adopted a prevalence estimate
of 2-3 per 1,000 based on the Atlanta study, which had the advantage of being in the southeast
U.S., appeared to be a well-done study, and concurred with several other estimates from other
studies with a wider population base.
Although this estimate of the prevalence of ASD is not definitive, it appears to be the estimate
most applicable to Tennessee, yielding an overall estimate for Tennessee of 3200 to 4800
children (ages 0-21) with ASD. Prevalence estimates based on 2-3 per 1,000 children have
been calculated for each Tennessee county (see Appendix C). These figures are only an
application of the prevalence estimate to the population numbers for each county – they are
not a count of children actually identified with ASD.
Autism Services Proposal
SJR 567
9
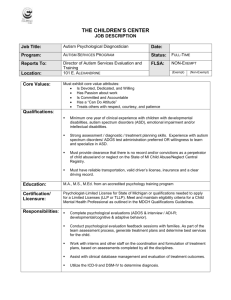
Rising Incidence
The incidence of reported autism is increasing. For example, reports from special education
across the nation and world indicate more numbers of children with autism enrolled in
schools. In Tennessee, the numbers of identified children with autism, ages 3-22, has
significantly increased from 1992 (n = 367) to 2002 (n = 1505). It should be noted that the
numbers in Figure 1 (below) are based only on children identified with autism rather than the
broader ASD category. In July 2002, the Department of Education broadened its definition to
include the ASD disorders in addition to autism, so the numbers of children in the 2002-2003
school year is expected to increase further1. Also, the numbers reported in the schools appear
to be an underestimate of the numbers of children with autism expected relative to the
prevalence estimates. This discrepancy may be due to multiple factors. Some children with
autism are classified in diagnostic categories other than autism (e.g., mental retardation,
speech and language impaired); some children are not counted due to attending home school,
private school, or being institutionalized; and some children, particularly younger children and
children with more mild manifestations of ASD, are not being diagnosed at all.
Figure 1. Number of Students with Autism Identified by Tennessee Schools
1600
1400
Number 1200
Of
Students 1000
800
Autism
600
400
200
91
-9
2
92
-9
3
93
-9
4
94
-9
5
95
-9
6
96
-9
7
97
-9
8
98
-9
9
99
-0
0
00
2 0 -0
01 1
-2
00
2
0
School Year
1
The numbers of young children, birth to age 3, identified by Tennessee’s Early Intervention System as
having autism are much smaller, reflecting the difficulty of diagnosing children with ASD early in life.
For the 2001-2002 school year, 153 children from birth to 3 years of age were identified as having
autism. Large numbers of children were identified with speech and language delays or with general
developmental delays. Many children from these classifications will later be found to have autism.
Autism Services Proposal
SJR 567
10
The cause of increased numbers of children being diagnosed with autism is not known.
Possible contributing factors to the rising incidence of reported autism and ASD are: 1) higher
numbers of children being diagnosed due to better diagnostic services and increased
awareness in the population about developmental disabilities and ASD, 2) numbers reflecting
the full spectrum of ASD, rather than autism only; 3) better data collection efforts, and 4) asyet-unrecognized environmental causes of ASD.
One careful study conducted in California2 in 1999 at legislative request concluded that the
unprecedented rise in reported cases of autism in California between 1987 and 1998 could not
be explained by a loosening in the diagnostic criteria, misclassification, nor in the issue of
children “migrating” to California for services. The study concluded that the increase was not
artificial, but could not explain the causes of the increase.
VI. Tennessee’s Existing System
Tennessee’s existing system for serving children with autism is inadequate. There is a broad
consensus from parent, provider, and state focus groups, a 2002 informal survey of 130
stakeholders across the state, and previous Tennessee autism task forces that children with
autism and their families are not receiving adequate services in education, health, behavioral
health, and family support services such as respite (see Appendix D for related documents). A
study of TennCare services (Ruble, Heflinger, Renfrew, & Robson, in press) found that the
rate of children with ASD served by TennCare between 1995-2000 for any kind of service
delivery in health and behavioral health services was 10 times less than the expected number
of enrollees. Furthermore, a reduction in services (most notably day treatment) was noted in
this time frame. Few children received autism-specific kinds of treatment like habilitative
services and speech and language therapy. The study identified gaps between the current
known standards of care for treating children with ASD and the local access and delivery of
behavioral health care services provided in Tennessee.
The inadequacies in the system include:
•
Limited network of trained professionals in the area of ASD
Professionals particularly needed to serve children with ASD include special educators,
primary care providers, mental health providers, speech and language pathologists,
occupational and physical therapists, and dental providers. The recent survey named
TRAINING as the most needed service across all areas of the state.
The Department of Education (Division of Special Education) has taken first steps to train
educators through a contract with the Treatment and Research Institute for Autism Spectrum
Disorders (TRIAD), however, the scope of the contract has some limitations, including: 1)
2
The conclusion: “Without evidence for an artificial increase in autism cases, we conclude that some, if
not all, of the observed increase represents a true increase in cases of autism in California, and the
number of cases presenting to the Regional Center system is not an overestimation of the number of
children with autism in California” (The Epidemiology of Autism in California, Executive Summary,
2002, p. 5).
Autism Services Proposal
SJR 567
11
until this year training has been for preschool only; 2) contract offers little opportunity for
follow-up to the trainees, and 3) the anticipated “train-the-trainer” model has not materialized
within some regions where special educators have been trained, due in part to lack of
resources and support to allow time off for new teachers to be trained. It is clear that, for the
training program to be successful, there must be more support for trainer development as well
as more resources for TRIAD staff to follow up with the trained teachers in the field.
More training is needed within secondary educational institutions. While there is some
training within the state such as the federally funded Leadership Training in
Neurodevelopmental and Related Disabilities (LEND) that teaches a section on autism to
interdisciplinary groups out of the UT-Boling Center and Vanderbilt’s Division of Child
Development, there clearly need to be more educational efforts. There are no state-funded
training initiatives at the professional level for training in autism.
•
Lack of insurance coverage for autism by both public and private insurance
Autism and mental retardation as primary diagnoses are specifically excluded in the contract
between TennCare and the BHO, as well as in most private insurance plans. In other words, if
the behavioral challenges appear to be “autism-related”, and not specific to a mental illness
(e.g., bipolar disorder), then the BHO declines payment responsibility and usually will not be
asked to pay upon appeal. Even if a child is served due to having a dually diagnosed mental
illness, the BHO does not have contracts with autism-specific service providers or service
delivery systems, once again highlighting the lack of specialists in the network (See Appendix
E for this contract language).
Services such as speech, occupational, and physical therapy are often needed for children with
autism. While these services, when medically necessary, fall under the auspices of covered
health benefits, the insurance plan reviewers often refuse to pay for children with autism,
stating that these specialized services should be delivered by the educational system. The
argument is that the services are “educationally related” rather than “medically necessary”.
Because children with autism often need such services intensively and early, there may be
both an educational and medical need. The lack of clarity gives room for debate between
systems. Children have been caught between systems as they try to obtain needed services,
often losing precious time and obtaining the “legal minimum” of a service rather than the
appropriate “dosage” of various services.
However, at least in the realm of public health coverage, c;aroty does exist, at least in writing,
that the MCOs and education have joint responsibility for services. TennCare Standard
Operating Procedure #019, dated January 1, 1994, addresses the subject of MCO
responsibility to provide medical treatment to children receiving special education services. It
states in part:
“in the case of a TennCare-eligible child identified as eligible for
special education as part of the Individuals with Disabilities
Education Act who is also identified as having “related services”
needs that must be met in order for the child to benefit from special
education, TennCare MCOs are required to provide TennCare
Autism Services Proposal
SJR 567
12
covered services for TennCare children despite the inclusion of such
services in the child’s individualized education program…” Services
such as occupational therapy, physical therapy, speech therapy and
any other TennCare covered services are the responsibility of the
MCO.”
Despite TSOP # 019, however, families continue to struggle to get covered services
for their children with autism.
•
Lack of Family Support Services
Tennessee’s existing system lacks important non-entitled services that have traditionally been
deemed as not medically necessary, and fall outside coverage from insurance companies, but
are often the kinds of services needed to maintain a child in the home. Respite services,
intensive in-home behavioral assistance, personal assistance, and home modifications are
currently non-entitled services that are not covered under Tennessee’s existing service
structure for children with autism. Families, providers, and other stakeholders, through the
recent statewide survey, indicated that respite, in-home personal care, intensive in-home
behavioral interventions, and home modifications were inadequate. See the following
percentages from 130 respondents from a recent informal survey that was answered by
statewide stakeholders such as parents and providers of children with autism:
•
•
•
•
Service
Deemed Inadequate in 2002 Survey
Respite
82%
Personal assistance/care
77%
Intensive behavioral intervention
77%
Home modifications
78%
Many families with children with ASD need in-home modifications for safety such as special
door locks, bed modifications, and alarm systems. The state should assure that there is a
mechanism to provide these services to families who cannot afford them. Families of children
with autism speak of the challenging and draining experience of day to day life with children
with severe autism. These families experience burnout and exhaustion and often require
respite to continue caring for their children in their homes. Locating respite providers to give
caregivers a break, or personal assistants to aid in the activities of daily living such as feeding
and bathing may be the key to keeping children in the home. Finding professional caregivers
with the special training to care for the unique demands of a child with ASD is problematic.
All families with children with ASD need periodic respite. The State should assure that there
is a statewide system of respite services available.
•
Current Status of Respite Services in Tennessee
Some children with autism who have a dual diagnosis of mental retardation have been able to
access limited respite services through auspices such as Tennessee Voices for Children with
funds through the Family Support Program (Division of Mental Retardation). Families who
have been fortunate enough to receive the Family Service Program funds and find appropriate
Autism Services Proposal
SJR 567
13
respite services have reported positive outcomes. There are few trained respite providers,
however, who can serve children with autism who also have serious behavioral challenges.
There is a need for autism-specific providers and for more respite funds. The FSP has a very
long waiting list for families.
Currently, there is a model respite services delivery vision through the Tennessee Respite
Coalition (TRC), housed in DMHDD. A federal grant funds a coordinator for the Tennessee
Respite Coalition, which has been in existence for several years. This group has a statewide
presence, with seven regional TRC groups, and has served as a collaborative, networking
entity, which advocates for respite services across lifespan and disability. All sectors with an
interest in respite are represented in this group.
The Coalition has developed a statewide model for lifespan respite services that cross all ages
and disabilities. The Tennessee Respite Coalition will be a 501(c) 3 (nonprofit) program
which will house an infrastructure which will train providers across the state in the specific
skills needed to deliver respite services, as well as doing information and referral service and
running a voucher program which would provide assistance to families unable to pay for
respite service. The respite services will be delivered in seven regionally based lifespan
respite programs. All lifespan respite programs will work with providers to deliver respite
services.
•
Inadequate Early Intervention Services
While there are federally mandated early intervention services delivered statewide through the
Tennessee Early Intervention Services for children birth to age three, the workgroup
consensus is that these services are greatly variable across the state in terms of adequacy; the
services often do not begin early enough for families and children to benefit; and transition
from the early intervention services to pre-school is always abrupt and usually uncoordinated.
Although research indicates that early intervention services for children with autism should
ideally be available for children up to age eight, the federal statute allows for these services to
go at least to age three but up to age five. Since children with autism are often not diagnosed
until age two or later, the current TEIS services are often too brief to be fully beneficial.
There needs to be a system where the types of services available for early intervention
services can be extended through the early elementary years. (See Appendix F for the federal
guidelines for early intervention and the TEIS guidelines). Section VIII details the
importance of effective early intervention.
•
Inadequate Educational Services
Educationally, many families report that their children with autism do not receive the types or
amounts of educational services that are most beneficial to children with autism. While there
is an overwhelming general consensus across the state that educational services are not
adequate, there are spotted reports of certain school districts or specific local school programs
that are addressing the needs of children and families adequately. Such school districts are
seeing an influx of families with children with autism moving into their districts. This
phenomenon is creating a capacity issue. Section XI details appropriate educational services.
Autism Services Proposal
SJR 567
14
The majority of families accept the school’s version of the Individualized Education Program
(IEP) which typically meets the minimum of legal requirements and is often not adequate to
meet the individual child’s needs. Parents have described many educational programs as
“babysitting”. Others have indicated that their child is getting the right services, but not
nearly enough to create progress toward IEP goals. Parents describe the relationship with the
IEP team as very strained, lacking collaboration. Parents with training in autism and due
process, or those with legal counsel or advocates, have sometimes successfully gained needed
services for their children. This often has come at great expense, such as expensive lawsuits
(for both parents and school districts), frustration and relationship tension, and lost time for
children. Most families express a great frustration when describing their attempts to gain
sufficient school services. Many families, however, report important progress in their
children once adequate services have been obtained.
Finally, although early intervention is seen as foundational for children with autism, another
very specific need emerges at the other end of the age range, that is, the transition from school
to work. Tennessee has virtually no specific system for training young people with autism in
the skills needed to work and live as independently as possible. Many young persons with
autism can be trained to contribute productively to the work force; however, the services for
these young persons need to be developed within the educational system and should be
autism-specific. Educational services are available for youngsters to age 22; there is a great
need to invest some resources in this transitional population. The specifics of these needs are
discussed in section XI.
•
Inadequate long term care options
Long-term care is a complex issue, but an important one for children with autism. While
ideally, most children who need long term care would best be served by home and community
supports, this would require a “waiver” service that would only be accessible by those who
meet eligibility and it would require a waiver that matches the service needs of children.
There is not such a waiver for children in Tennessee. Under the federal Early and Periodic
Screening, Diagnosis, and Treatment (EPSDT) statute, institutional long term care (ICFMR)
is a covered service for those who are Medicaid eligible and meet medical necessity criteria.
However, there are very few ICFMR placements in Tennessee and ICFMR services are rarely
the best treatment option for children. (Office of the Surgeon General, 1999). Thus, long term
care needs for children on both public and private insurance plans are not, at this time, readily
available in Tennessee. Although a few children have become eligible for long-term care
through the MR waiver, these few children have been considered “crisis exceptions”, due to
the risk of entering state custody without services. Once children have been accepted into the
long term care facilities, it is clear that the services are set up for adults, not for children.
Because most children with autism, by definition, require long term care at some level, there
is a clear need for a long term care program that is more accessible for children’s entry and for
services that better match children’s needs (e.g., home-based services).
Autism Services Proposal
SJR 567
15
VII. Costs
A recent estimate of the lifetime costs associated with autism is $4.5 million per person
(Jarbrink & Knapp, 2001). Costs for services for children with severe autism and behavioral
challenges are high due to:
• the need for intensive levels of supervision;
• the chronic and intense nature of the behavioral challenges;
• the need for a combination of specialty services (e.g., psychiatry, behavioral specialists,
speech/language, etc.).
In addition to these general reasons for high costs, greater expenses for Tennessee
children with autism occur due to:
• lack of specialists in a given area, creating the need for travel or for out of state
treatment;
• lack of integration of services leading to fragmentation of care so that behaviors
continue to be unnecessarily problematic;
• lack of less expensive home-based services available that specialize in serving
children with autism and their families , again leading to more costly out-of-home
placement;
• lawsuits against the state
Following are a few recent examples of children with autism from Tennessee, and the
costs associated with their care.
One family with a 9 year old boy with autism and profound
mental retardation was struggling with extremely challenging
behaviors from their son, including self injury and aggressive
outbursts. When they could not obtain appropriate services
through the TennCare channels, they successfully sued the
state. Their son was placed out of state in a residential
program. The state paid about $16,000 a month for 10 months.
This would amount to $192,200 per year. The treatment
providers in this facility did not think that this child could
return home, however, his parents wanted to give it a try.
Because the lawsuit was driving payment for the treatment, the
family was able to access good home-based behavioral
interventions for their child. Since May 2002, the care for this
child is costing approximately $3500 per month, or $42,000
per year, a savings of approximately $150,000 per year. With
appropriate services, there are better outcomes for the child
and family at a lower cost to the state.
----------------------------------------------------------------------A 14-year-old boy with autism and mental retardation was
having a difficult time remaining in the care of his
grandmother due to behavioral challenges. He was placed in
an adult psychiatric facility, paid for by the BHO (TennCare)
Autism Services Proposal
SJR 567
16
and the cost was $675 per day. He remained in this facility for
months, despite the fact that it was not appropriate to meet his
needs. The Implementation Team from the Department of
Health became involved and the child was placed in a
Professional Support Home (family-based care) with
behavioral support services at a cost of $355 per day. Since
there is not an entity that pays for these kinds of services for
children in Tennessee, state only funds are used to support this
child in the current plan. He is making progress in this
placement and the state is saving $320 dollars per day on his
care as compared to the psychiatric facility.
Creating a coordinated, intensive early intervention service system to which children have
adequate access can ameliorate the costs associated with autism. This effort would result in
decreasing symptomatology in children with autism, which in turn reduces human and dollar
costs. Compelling evidence exists that early intervention is effective; this will be briefly
reviewed in the next section. In terms of cost, however, a group of researchers from
Pennsylvania conducted a theoretical lifespan cost-benefit analysis associated with the
benefits of early intervention for persons with autism compared to persons with autism not
receiving early intervention services (Jacobson, Mulick, and Green, 1998). This speculative
study was based on costs of intervention for an average of three years per person and known
clinical benefits of early intervention. At varying rates of effectiveness and in constant
dollars, this study puts forth a model that estimates that cost savings would range from
$187,000 to $203,000 per person for ages 3-22 years and from $656,000 to $1,082,000 per
child for ages 3-55 years. This cost-benefit analysis suggests that the initial annual investment
of EIBI services ($33,000-$50,000 per child) would, again, theoretically, be worth the
savings. The analysis indicates that significant cost-aversion or cost-avoidance may be
possible with EIBI.
VIII. Effectiveness of Early Intervention
•
Early Intervention is a known key to improving the conditions associated with autism; the
benefits of early intervention cannot be regained at a later time.
Early intervention describes the provision of services, under federal mandate, to young
children with disabilities or at risk of developing disabilities. These services include the
evaluation, assessment and treatment of young children with disabilities from birth to three in
most states, but from birth to five in a few states that have extended the age limit. These
services are rendered in the hopes of lessening the effects of the child’s disability or condition.
In Tennessee, the Tennessee Early Intervention Services, known as TEIS, is the service
delivery mechanism for these federally mandated services. There are nine TEIS regions that
serve children, ages birth to three, who have a wide variety of developmental disabilities.
Early intervention is dependent on early and accurate diagnosis. One of the issues raised by
families and providers is that children often have limited access to early intervention services
because they are diagnosed too late to be eligible, or have a very short time in the early
intervention program
Autism Services Proposal
SJR 567
17
Early intervention for children with autism requires the development of an individualized
treatment plan, which includes both academic and non-academic goals. The goals and
objectives for a child with autism may include social skills, self help skills (dressing, toilet
training, feeding oneself, etc.), communication, behavior modification, as well as others as
appropriate. It is important to stress that no one program is appropriate for all children with
autism. A program should be designed to work with each child’s unique strengths and
challenges (see Appendix F for a list of services available for Early Intervention Services
through the 1990 Individuals with Disabilities Education Act (IDEA), Part C, as well as the
TEIS guidelines).
There is substantial evidence that children with a variety of developmental delays and
disorders have a greater chance for successful outcomes if interventions are started at an early
age (e.g., Guralnick, 1998). Thus, there has been an increased emphasis on programs for
“early intervention” in the past decade. Likewise, many experts agree that intervention at
early stages in a child’s development may have a greater chance for success for children with
autism (e.g., Lovaas, 1987; McEachin, Smith, & Lovaas, 1993). Over the past 25 years, a
small number of programs have worked intensively on researching interventions for young
children with autism and their families. These programs have published information about the
characteristics of children served, the methodologies used, and the child and family outcomes.
Although the programs vary in their philosophical approach and strategies, they include
several common elements detailed below.
Dawson and Osterling (1997) reviewed eight model early intervention programs for children
with autism. These studies meet good scientific standards and the results point to the
effectiveness of these eight model programs. The results of these studies have been adopted
as the standard for creating the early intervention guidelines for autism services in New York
State. The common elements that have been found to underpin successful programs for
children with autism include3:
•
•
•
•
3
Curriculum content. Five basic skill domains including: 1) to attend to elements of
the environment that are essential for learning, especially to social stimuli; 2) to
imitate others; 3) to comprehend and use language; 4) to play appropriately with
toys; and 5) to interact socially with others.
Highly supportive teaching environments and generalization strategies. The
programs first try to establish core skills in highly structured learning situations
and then work to generalize these skills to more natural environments.
Predictability and routine. Since the behavior of children with autism is easily
disrupted by changes in the environment and routine, the programs adopt strategies
to assist the child with transitions from one activity to another.
Functional approach to problem behaviors. To address problem behaviors, the
environment is structured to help avoid problems. When problems persist, a
functional approach is used that involves: 1) recording the behavior; 2) developing
These elements are taken from the Clinical Practice Guideline: Report of the Recommendations;
Autism/Pervasive Developmental Disorders, sponsored by the NY State Department of Health Early
Intervention Program (1999).
Autism Services Proposal
SJR 567
•
•
18
a hypothesis about the function that behavior serves for the child; 3) changing the
environment to support appropriate behavior which allows the child to cope
effectively with the situation; and 4) teaching appropriate behaviors to replace
problem behaviors.
Plans for transition from preschool classrooms. The programs teach “survival”
skills that children will need later on in order to function independently in
preschool or school classrooms.
Family involvement. The programs include parents as a critical component in the
intervention for young children with autism. Parents give insight into creating an
intervention plan, they add hours of intervention, and they can help with the
maintaining and generalization of skills.
Tennessee examples regarding early intervention
Consider the following examples about two Tennessee children with autism:
A situation with early intervention services
A child, currently age 5, was diagnosed with developmental
problems at age 15 months and referred to Tennessee Early
Intervention Services (TEIS). At age 20 months he began attending
a developmental preschool and receiving speech therapy. Soon
thereafter, he was diagnosed with mild to moderate autism. The
child received autism-specific intensive therapy with a program in
Applied Behavioral Analysis (ABA) for 12 hours a week for which
TEIS paid. Later, TEIS paid for speech and occupational therapy, as
well as 6 hours a week of the ABA. (Private insurance had been
contacted and had deemed the needs “educational”, refusing to pay
for speech and occupational therapy). At age 3, due to age limits,
the child was no longer eligible for TEIS, however, the local public
preschool program (through his IEP) agreed to continue the ABA
program with the same providers. Current evaluations at Vanderbilt
have determined that this child no longer falls in the autism range,
but is achieving at the average and above average level of skill. He
no longer qualifies for speech therapy. He is now mainstreamed in
regular education classes with no special supports. Due to early
intervention with autism-specific, evidenced based services, this
child has been able to succeed and the state no longer will pay for
special services.
A situation without early intervention services
A child with autism and mental retardation, currently age 10, was
adopted at age 5 after several failed foster placements. She had never
been diagnosed with autism, nor had she had any early intervention
services for severe behavioral challenges and developmental
Autism Services Proposal
SJR 567
19
problems. She was nonverbal when adopted. While her primary
care physician (PCP) tried to treat her symptoms with medications,
the PCP gave neither diagnosis nor referral for a specialized
assessment. Finally, at age seven, a provider in North Carolina
diagnosed this child with autism. The family still travels out of state
to a provider experienced in prescribing medications for autistic
children, after seeing a very reputable psychiatric provider in
Tennessee whose service was ineffective due to lack of knowledge
regarding autism.
The adoptive, single mother, herself a professional in the area of
social services, began a long struggle with the public education
system. Although her child was hearing impaired and making some
progress with sign language at the Tennessee School for the Deaf,
services were discontinued due to her behavioral issues related to
autism. Following, the county school district would not put her in a
program for hearing impaired children, placing her instead in a
Consolidated Developmental Classroom (special education
classroom) without an interpreter. Her mother had to go to due
process in order to obtain an interpreter.
Costs to this family have been enormous. The mother recently gave
up her full-time work due to the inaccessibility of after-school care
(child was ejected from after-school care) and assistance during
school breaks (e.g., holidays; summer). This mother’s income has
drastically decreased while expenses have drastically risen. She has
spent over $13,000 in due process hearings with Special Education,
has depleted her savings account, had to quit her job, and has found
the entire process exhausting. This mother has paid out of her
pocket for assistance in the home, for respite, and for occupational
and physical therapy. The mother has had difficulty acquiring respite
care (both in finding a provider trained in physical restraints and in
obtaining funding) but is currently getting some respite through
Tennessee Voices for Children (initially BHO funded; now ARC
funded). Likewise, she has been through a long, frustrating battle
between the BHO and MCO on coverage of needed services such as
in-home personal assistance.
Clearly, this child did not receive the benefits of early intervention that might have given her
the communication, behavioral, and social skills to have more success in daily living. Even
with a dedicated and informed parent advocating hard for her daughter, the services for this
child have been difficult to obtain.
These two cases obviously differ in the level of the children’s initial impairment. While the
first child was helped to achieve normal functioning, the second child’s potential has not been
realized. While it is improbable that she could have reached “normal” functioning, she would
Autism Services Proposal
SJR 567
20
likely have been able to achieve some behavioral control and some level of independence if
she had been afforded early intervention services. Her family life would have likely been
smoother; she would probably have been able to stay in after school programs with her peers.
However, she probably would have required some level of continued services across her
lifespan, no matter what the intervention. At this point, it is uncertain whether her mother will
be able to keep her in the home; the mother has been advised to move to a different state
where the educational services offer more autism-specific support.
IX. Immediate actions needed
There are several clear actions that Tennessee should take to ensure that children with autism
and their families are comprehensively served in order to maximize the effectiveness of
treatment for ASD. These include:
•
•
•
•
•
•
•
•
•
•
•
Assure early identification, accurate diagnosis and treatment planning capacity
across all regions by funding regional diagnostic/consultation centers
Create a coordinated system of autism-specific services with expert providers
Provide access to individualized home-based intensive behavioral intervention
Implement evidence-based, intensive early intervention strategies across all
Tennessee systems in order to capitalize on the benefits of early intervention for
children birth to age eight.
Ensure year round school options for all students, as appropriate to their needs
Ensure developmentally appropriate educational strategies and transition plans for
older children (ages 8-22)
Assure that every school district receives training and support for educators and
related professionals
Establish statewide capacity to constantly improve knowledge, practice and costeffectiveness
Measure improved outcomes as defined by each child’s IEP
Create a clear oversight plan to ensure an effective system
Create a clear funding plan for ASD services
These points will be elaborated in sections to follow, most notably in section XIII that outlines
a proposal for an organizational model for autism-specific resources. The following
paragraphs are designed to continue to discuss the specific needs of children with ASD.
X. Screening and Diagnosis
Periodic screening as part of routine child care
Early diagnosis of autism that results in appropriate and consistent interventions has been
shown to be associated with improved long-term outcome (Committee on Children with
Disabilities, American Academy of Pediatrics, 2001; Filipek et al., 2000). However, there is
considerable evidence that routine health care for children misses a significant proportion of
developmental and behavioral problems (Dworkin, 1989; Glascoe & Dworkin, 1993;
Autism Services Proposal
SJR 567
21
Majnemer, Rosenblatt, & 1994). In fact, one constant theme among the focus groups surveyed
for this report to the Tennessee legislature was that many children with autism are not being
identified or referred early by their primary care providers.
Use of validated developmental/behavioral screening instruments in well childcare improves
detection of developmental and behavioral problems (Committee on Children with
Disabilities, American Academy of Pediatrics, 2001). A 2001 American Academy of
Pediatrics (AAP) policy statement on autism stated that for pediatricians, "There must be a
high index of suspicion, especially when parents have concerns about their child's language
and social development...." (Committee on Children with Disabilities, AAP, 2001; p.107). The
recommendations further state that all children should be formally monitored and screened for
developmental progress at every well child visit with special vigilance when deficits are noted
in language or social skills development. Ideally, children who have abnormal screens,
especially in these areas, should have further screening specific for ASD with standardized,
well validated instruments (e.g., Modified Checklist for Autism in Toddlers (M-CHAT;
Robins, Fein Barton, & Green, 2001), or they should be referred to a specialist or
multidisciplinary team with expertise in autism. In Tennessee, however, such resources are
limited. Historically, there has been state funding for university-based diagnostic centers, but
the funding has decreased markedly in recent years.
A report by the American Academy of Neurology in their 2000 autism guidelines stated that
while as many as 25% of children in a typical primary care practice may have developmental
issues, fewer than 30% of primary care physicians conduct standardized screening tests at
well child visits. (Filipek et al., 2000).
In Tennessee, TennCare has recommended use of validated developmental/behavioral
screening instruments as part of Early and Periodic Screening, Diagnosis and Treatment
(EPSDT) well child screening. In July 2002, the Tennessee Health Department began use of
the recommended screening instruments in its EPSDT well child screenings but use of such
instruments in well child care in Tennessee is not widespread outside the Health Department.
The reasons for the lack of developmental screenings at well child visits are multifaceted and
include lower than desired reimbursement rates for a screening process that often leads to
more paperwork and triage, lack of PCP familiarity and comfort with the screening
instruments, lack of training and awareness by PCPs of the full range of developmental
disabilities, especially ASD, lack of personnel to conduct these time-consuming screens, and
inadequate referral resources for children with positive screens.
Implementation of widespread effective screening for early detection of ASD depends on:
• Ongoing, time-efficient educational programs to train PCPs to recognize the wide
spectrum of symptoms of ASD
• Reimbursement policies that allow adequate time to be spent in the use of the
screening tools and in the management and coordination of care in the context of
a medical home4 (AAP Committee on Children with Disabilities 2000-2001).
4
The American Academy of Pediatrics has a nationwide effort to establish “medical homes” for
children with special health care needs. The American Academy of Pediatrics (AAP) believes that
Autism Services Proposal
SJR 567
•
•
22
Persons within PCP offices with the time and expertise to conduct the screens and
follow up with triage (e.g., maybe “extenders” such as social workers)
An adequate number of behavioral specialists who accept referrals for diagnosis
of autism
School systems require information beyond screening from several sources in order to certify
that a child has a diagnosis of autism and is eligible for special education services. These
include:
•
•
•
•
•
•
Parent interviews
Behavior observations in two settings
Medical report of physical and neurological information from a physician,
pediatrician, or neurologist
Assessment by speech and language specialist
Assessment of cognitive, adaptive behavior, and social skills
Documentation of how autism adversely affects educational performance
Assessment information is then used by a multidisciplinary team, which includes the parents
of the child, to develop an Individualized Family Service Plan (IFSP) for children under 3 or
an Individualized Educational Program (IEP) for children from 3 to 22. The ISFP or IEP
should reflect the needs of the individual child, as documented in the assessment process, and
provide for services to address those needs. Details about services provided through IFSPs or
IEPs are discussed in the following section and also in Appendices F and G.
XI. Educational service needs for children with autism and their families
Federal and state definitional and eligibility criteria
Information gained through recent task forces and surveys clearly indicate that educational
services are the most important source of help for children with ASD. Because children with
ASD need intensive, consistent, behaviorally-based learning, the educational system bears the
primary responsibility for the developmental progress of children with ASD. The federal
IDEA law indicates that autism is a developmental disability that must be addressed through
special education. The State Board of Education Rule 0520-1-9-.01 states a definition for
autism that is consistent with the federal IDEA statute. The current task force endorses the
DOE state standards as they stand. The state’s definition of autism conforms to current
medical and behavioral health standards, and the addition of including eligibility for the entire
autism spectrum serves as an important inclusion. Likewise, the standards for determining
medical care should be accessible, continuous, comprehensive, family centered, coordinated,
compassionate, and culturally effective. Termed " medical home", this model provides for a primary
care physician to collaborate in partnership with the child and family to: 1) Interact with early
intervention programs, schools, early childhood education and child care programs, and other public and
private community agencies to be certain that the special needs of the child and family are addressed;
and 2) Provide care coordination services in which the family, the physician, and other service providers
work to implement a specific care plan as an organized team. ( AAP Policy Statement, Pediatrics
Volume 110, July 2002, pages 184-186). The Tennessee chapter of the American Academy of pediatrics
has endorsed this concept and worked diligently to promote this concept in the state.
Autism Services Proposal
SJR 567
23
eligibility are sound and use a multidisciplinary approach (See Appendix G for our state
definition, eligibility standards, evaluation procedures, and evaluation participants for autism.)
As a part of the IDEA guidelines, each child should have an IFSP (ages 0-3), or an IEP (ages
3-22) that is developed by a multi-disciplinary group of persons knowledgeable about autism
in partnership with parents in order to facilitate goals, objectives and outcomes for the child
and family. Although the current state definitions do indicate that a multidisciplinary team is
formed that includes parents, the current definitions do not indicate that persons on the task
force must have expertise in autism-specific services. IDEA posits that all states must:
“ensure that all children with disabilities have available to them a free appropriate public
education that emphasizes special education and related services designed to meet their unique
needs and prepare them for employment and independent living.” (34 CFR 300.1 (a))
Core educational components
The work group recommends that educational programs for children aged birth to 22 years old
with autism include several core components.
First, there is clear evidence that many children with autism need year round educational
services in order to maintain and continue educational gains. Many children without summer
educational programs lose ground that is difficult, if not impossible, to regain (Committee on
Children with Disabilities, AAP, 2001). The work group members concur that a year round
model must be a goal for Tennessee children as appropriate.
Services must be individualized for the child and family and based on the IFSP/IEP goals,
objectives and outcomes to address all areas of development, including, as appropriate:
•
•
•
•
•
•
•
Functional communication skills
Social skills and relationships
Cognitive developmental skills (including attending skills)
Fine and gross motor skills
Prevocational skills
Positive behavioral skills and adaptive skills
Family involvement and participation
The above general areas of development are supported through various, autism-specific
services including some or all of the following:
•
•
Behavioral intervention5 (very intensive in earlier years, e.g., ages 0-8)
Speech and language therapy
5
Behavioral intervention includes many possible techniques. The techniques included under the
umbrella of Applied Behavioral Analysis have passed research standards indicating their effectiveness.
Under the ABA umbrella, however, are a number of techniques such as discrete trial training and
incidental learning. See Appendix H for a fuller description of the ABA approach.
Autism Services Proposal
SJR 567
•
•
•
•
•
24
Audiology assessment and accommodations if needed (especially critical in early intervention
years)
Occupational therapy
Physical therapy
Parent training
Consistent use of data collection and monitoring
Depending on the nature of the child’s needs and the child’s specific learning style, a
combination of environments should be accessed to best serve that child in a least restrictive
and most educationally appropriate way. The amount of time spent in these environments
should be child specific and may change over time.
Inclusion is the philosophical idea that children with disabilities learn best when included in
environments with typically developing peers. The current task force emphasizes that special
education programs should facilitate inclusion with typically developing peers as appropriate,
with decisions made on the basis of an individual child's needs. A quote from the recent 2001
report, Educating Children with Autism, discusses inclusion as follows:
“… a child must receive sufficient individualized attention on a daily basis so that
individual objectives can be effectively implemented; individualized attention
should include individual therapies, developmentally appropriate small group
instruction, and direct one-to-one contact with teaching staff. … To the extent that
it leads to the specified goals (e.g., peer interaction skills, independent
participation in regular education), children should receive specialized instruction
in settings in which ongoing interactions occur with typically developing peers”.
A quote from a chapter regarding preschool services agrees that inclusion is important, but
emphasizes that the needs of the individual child are paramount as stated in the following
quote:
“The goal of integration into the typical school setting is unquestionably correct.
However, for some children a normalized setting, even with extensive support
services, may not be the least restrictive setting. Central to the issue is one’s
definition of “least restrictive.” For some children, a strategy of a continuum of
services, from an intense, focused, individualized, specialized setting to the more
typical classroom with required support services, is the most appropriate. This
allows for rapid acquisition of needed skills and for a choreographed approach to
habilitation …”6
Next, services should facilitate active engagement across settings, with children being actively
engaged for appropriate periods of time. Current national education standards recommend 2025 hours of active engagement as a target amount for children birth through age eight
6
Raymond Romanczyk, Linda Matey, and Stephanie B. Lockshin, (1994). In Preschool Programs for
Children with Autism by Sandra L. Harris and Jan S. Handleman (Pro-Ed: Austin), Ch. 10, The
Children’s Unit for Treatment and Evaluation.
Autism Services Proposal
SJR 567
25
(Committee on Educational Interventions for Children with Autism, 2001). Active
engagement is defined below.
“… the child is engaged in systematically planned, developmentally appropriate
educational activity aimed toward identified objectives. Where this activity takes place
and the content of the activity should be determined on an individual basis, depending
on the characteristics of both the child and the family” (Educating Children with
Autism, 2001 p.220)
One complaint in the current Tennessee system is that some children do receive the
appropriate hours of active engagement while in the early intervention system, but do not
continue to receive this engagement once they are age three and are in the regular educational
system. Often, children at the age 3-6 year old level continue to need many hours of active
engagement in the home as well as in the preschool and other settings. Sometimes, the homebased interventions abruptly end at age three, leaving children without the needed consistency
of program to generalize their learning across settings.
Another complaint is that the term “active engagement” can be misconstrued to mean “being
with typical peers”. Some children are put in “inclusive” settings and then are given services
that appear to be more like typical “childcare” rather than active autism-specific curriculum.
Thus, an aide may be involved all day with a child to ensure his/her safety, but the child is not
adequately stimulated and thus is not progressing.
Quality control/accountability
All services in the educational setting should be autism-specific and evidence-based. There
exist specific curricula for working with children with autism in the various service modalities
such as speech and language, occupational therapy, social and adaptive skills, behavioral
skills, and physical therapy, as well as the basic academic curricula and cognitive skills such
as learning how to learn and paying attention.
Furthermore, ongoing program evaluations based on appropriate data must occur to document
the child’s progress and to facilitate any needed adjustments in the IFSP/IEP. A main
component of Applied Behavioral Analysis is to collect consistent data and monitor the
child’s progress based on the data. So, if ABA principles are consistently utilized within the
educational curricula, data monitoring should be an integral part of the process (see Appendix
H for ABA defined).
Transition services
Transition services are a key component to adequately addressing the needs of persons with
developmental disabilities. The IDEA Public Law 105-17 mandates that all states ensure that
students with disabilities are “prepared for employment and independent living.” (34 CFR
300.1 (a))
Autism Services Proposal
SJR 567
26
It is essential that the transition between early intervention services and preschool services, as
well as between Pre-Kindergarten to Kindergarten be well coordinated in order for the child to
continue making consistent progress. It is also important that the option for autism services
continue to include in-home interventions if needed, as well as intensive classroom
interventions. If transition at these early stages is not handled well, children are at risk of
losing skills that may be difficult, and often impossible, to regain.
Transition services for high school students (ages 14-22) should include the kinds of services
and supports that allow students to learn independent working and living skills that will lead
to success following the school years. Integrated high school programs with specific living
and vocational skills that are geared toward young persons with autism must be stressed.
Families and students should be helped throughout development to think about goals for life
after high school and to develop long-range plans that can be addressed within the high school
curriculum. Note the following IDEA 1997 transition requirements:
(b)(1) For each student with a disability beginning at age 14 (or younger, if
determined appropriate by the IEP team), and updated annually, a statement of
transition service needs of the student under the applicable components of the
student’s IEP that focuses on the student’s courses of study (such as participation
in advanced placement courses or a vocation education program); and
(2) For each student beginning at age 16 (or younger, if determined appropriate by
the IEP team), a statement of needed transition services for the student, including,
if appropriate, a statement of the interagency responsibility or any needed
linkages.
The federal regulations that include interagency linkages must be strictly enforced for students
with autism. The law states that needed transition services:
“includes instruction, related services, community experiences, the development
of employment and other post-school adult living objectives, and if appropriate,
acquisition of daily living skills and functional vocational evaluation (34 CFR
300.29(a) (3)).”
Thus, it is important that eligible students gain the benefits of Vocational Rehabilitation
Services and other interagency services while still in high school that are, under IDEA, their
right. It is an eligible child’s right according to the Tennessee DOE Division of Special
Education manual that:
“A comprehensive vocational evaluation must be completed on every eligible
child by the child’s 14th birthday. It includes an assessment of the child’s interests
and aptitude” (Tennessee DOE Division of Special Education, IEP Procedural
Manual, p. 13).
Autism Services Proposal
SJR 567
27
Recommended components for an integrated transitional curriculum for this age group, as
individually appropriate, include:
•
•
•
•
•
•
•
•
•
•
•
Identifying most effective learning styles and job preferences
Introduction to structured community work experiences
Working with a job coach
Employer relations
Coworker relations
Use of transportation
Supervised management of money
Community skills training including communication
Identification of a conservator
Self-regulation and relaxation skills
Transitions in health care plans and insurance coverage
Transitional programs to follow the formal educational experience are also desperately
needed; however, such services go beyond the scope of this legislative proposal.
XII. Service Needs of Children with Autism and their Families
Barriers to care.
All of the work groups surveyed for this document have reported that acquiring services for
children with autism is difficult. Providers, advocates, and families report that they have
frequently encountered disagreements among various payment sources (e.g., insurance
companies, Managed Care Companies (MCOs), Behavioral Health Organizations (BHO),
Department of Education, Division of Mental Retardation Services) over responsibility for
payment and provision of services.
For families of children with ASD there is considerable variation in health insurance benefits
in amount, scope, duration, and provider of service. In addition, insurance coverage may
change with time. As families of children with ASD experience the demands of raising a child
with significant cognitive and behavioral problems, a parent may be forced to quit or change
jobs, and, thus, insurance coverage available through employers may change. In the private
sector, insurance companies may subcontract with a BHO for mental health care that is
limited in scope.
In Tennessee, behavioral and physical health needs of children on TennCare (Medicaid
eligible) have been divided into BHO and MCO services. When a child with autism has a
behavior that is clearly the result of a defined mental illness such as bipolar disorder, the BHO
will cover treatment related to that diagnosis. However, the current TennCare BHO contract
excludes autism if this is the only given diagnosis for a child’s behavioral problems. Many
private insurance companies also exclude coverage for primary autism. This makes it
problematic for a child with autism and disruptive or aggressive behaviors to get needed
mental health services. In addition, many private insurance companies exclude autism as a
billable diagnostic category for covered services.
Autism Services Proposal
SJR 567
28
In both private insurance and TennCare, respite services and long term care (discussed
previously in this proposal) are not covered. In addition, behavioral analysts and behavioral
specialists trained to assist in developing behavioral intervention plans for children with
autism are often not eligible for mental health licensure, thus currently rendering them
ineligible to be service providers through many BHOs, including TennCare.
Even beyond the issues of screening mentioned previously, recruiting physicians to participate
in the care of children with ASD has been hampered by low reimbursement rates relative to
the time required to coordinate care and deal with the special needs of these children and their
families. Such activities as phone consultations or visits to schools for IEP participation are
rarely reimbursed under private or public insurance plans. Likewise, psychologists and
behavioral interventionists are not able to bill for attending IEP meetings or travel time to a
family’s home to conduct intensive behavioral services. Some insurance companies will not
accept a child for even routine medical coverage if the child has a diagnosis of autism.
Another barrier to care reported by the focus groups is that many agencies have case
managers, leading sometimes to multiple case manages and a “diffusion of responsibility”
such that no one person is “steering the ship”. Also, sometimes federal and state regulations
preclude case managers from more than one agency being involved simultaneously. For
example, a community services agency (CSA) family support services (FSS) case manager
cannot continue to work with a family if a mental health case manager is assigned through a
community mental health center. The result is that children may have multiple case managers
or multiple sequential case managers with no single consistent person or agency directing care
over time.
The following list of services is based on an assumption that most children with ASDs will
have some type of insurance program (either public or private) that provides for physical
health coverage through a policy that relegates mental health coverage to a BHO through a
subcontract arrangement or through TennCare, where health services are divided between care
MCOs and BHOs. The following list is not intended to be inclusive.
Autism Specific Health Needs
•
Medications
Psychoactive medications do not address the core symptoms of autism but are frequently
helpful in addressing behavioral problems associated with ASD. Medications can
significantly improve behavior and the child’s ability to respond to educational and
behavioral interventions (Cohen & Volkmar, 1997). Though much more study is needed,
research has demonstrated the effectiveness of some medications in reducing aggressive
behavior (King, 2000), agitation, self-injurious behavior, stereotypic motor movements
(McDougle, Kresch, & Posey, 2000), perseverative behavior (Barnard, Young, Pearson,
Geddes, et al., 2002; Gordon, 2000), anxiety, irritability, hyperactivity (Aman &
Langworthy, 2000), and sleep problems. Research has also indicated side effects of many
medications and points to the complexity of using medications for children with ASD.
Management of medications for children with ASD is a sophisticated process and requires
Autism Services Proposal
SJR 567
29
trained child psychiatrists, developmental pediatricians, or pediatric neurologists to assure
safety and effectiveness of treatment. The co-occurrence of ASD with seizure disorders,
estimated at 25-30%, (Minshew & Rattan, 1992) means that a significant proportion of
children with ASD are treated with anti-seizure medications (Tuchman, 2000). Cooccurring ASD and seizure disorders present challenges in use of psychoactive
medications with children who require anti-seizure medications. There is a great need for
trained child psychiatrists, pediatric neurologists, and developmental pediatricians for
appropriate treatment of children with seizure disorders and ASD.
•
Evidence-Based Behavioral Interventions
Behavioral interventions are the cornerstone of effective treatments for children with ASD
and should be delivered in both the home and school setting. Because children with ASD
have unique behaviors, BHOs should be required to develop a network of trained
providers with autism expertise who can develop comprehensive, individualized
behavioral management programs. BHOs should be empowered to contract with trained
behavioral analysts and specialists so that Applied Behavioral Analysis services can be
offered to children with autism. Because needs of children with ASD and families change
with time, BHOs should be required to provide ongoing monitoring of the behavioral
programs with this same network of trained providers. Provisions should be in place to
assure that there is coordination with the school personnel to assure consistency between
in-home and in-school behavioral management plans.
•
Other Important Treatments/Services
Speech/ language therapy is usually a needed service for children with autism. Often,
occupational therapy and physical therapy are also indicated. Although these services are
provided through the schools, they are often not comprehensive enough to adequately
meet the child’s needs. MCOs should be required to cover these services to the extent that
the PCP feels that they are medically necessary to provide optimum benefit.
Personal assistance is an important service for children with autism who require intensive
assistance with activities of daily living and supervision to ensure safety from selfinjurious behaviors. MCOs should be required to offer personnel assistance as necessary.
Children with autism have a great need for care coordination due to the spanning of
multiple systems inherent to their condition. Coverage for enhanced case management
with an individual trained in ASD is essential to quality care. Such a model might be a
shared responsibility of the MCO and BHO when these are separate (e.g., TennCare) or a
part of the comprehensive package when the MCO covers behavioral health also (e.g.,
many private insurance companies).
•
Therapy for family groups and siblings, specific to dealing with having a family member
with autism, should be available.
•
Children with severely disturbed behaviors may occasionally require out-of-home
placement. This should be given in the least restrictive environment possible. The BHOs
Autism Services Proposal
SJR 567
30
should be required to have an adequate network of residential facilities. Ideally, the
emphasis should be on short- term, individualized, family-like programs such as
professional support homes7. Likewise, as children with ASD transition to adulthood,
some young adults may be able to transition to independent living while others may
require long term supportive living that cannot be provided in the home due to the
advancing age of the caregivers. The state must assure that there are adequate resources
for these persons.
•
Respite Services and in-home modifications, previously discussed in section VI are crucial
services for families with children with autism and have been funded traditionally outside
of the managed care companies.
In sum, because ASD spans a broad array of symptoms from mild to severe developmental
challenges, plans of care must be individually tailored and changed as necessary with time. To
achieve the goal of providing appropriate and consistent care for a child with ASD, insurance
companies should not be allowed to exclude autism from their list of covered services,
reimbursement to providers should be appropriate to assure an adequate network of both
primary care and specialty care providers in a medical home model, there should be clear
guidelines for state agencies (e.g., DOE and DMRS) relating to which services fall under their
purview, families should have a knowledgeable and consistent case manager, and treatment
should be family focused and evidence based.
XIII. Organizational Model for Autism-Specific Resources
This proposal endorses a new infrastructure for a statewide, comprehensive service
improvement plan for autism services. This plan builds upon many existing structures,
making it cost effective and integrative. See figure 2 (next page) for an organizational map of
this proposed plan. As can be seen, the plan includes a state-level oversight unit, a state
center for ASD, five regional diagnostic and consultative centers, and eight regional
educationally based autism teams. These entities are interconnected in important ways that are
detailed in the following paragraphs.
7
Professional Support Homes are homes are much like “therapeutic foster care” models, where
“professional” parents are trained to care for special needs children in their homes.
Autism Services Proposal
SJR 567
31
Governor’s Cabinet Oversight
Dept of Education
(DOE)
Tennessee Center
for Autism
Spectrum
Disorders
5 COE &
Autism
Spectrum
Disorder Units
8 DOE
Regional
Education Autism
Teams
CHILD/FAMILY
Providers
School
Autism Services Proposal
SJR 567
32
State-level leadership.
First, improvements in services to children with autism and their families will require
governmental leadership with:
•
•
•
Executive, interdepartmental authority in state government
Expertise in autism
Multi-agency involvement
The leadership entity should be a super-ordinate unit that reports directly to the governor’s
office. Due to the multi-agency services involved in autism, it is imperative that the
leadership unit is given the kind of executive authority that is above individual departmental
heads. Such an entity could be similar to a children’s cabinet model (as long as there is one
authorized decision-maker) or it could be a unit within an oversight agency for children’s
health related services. The new administration will likely make changes that cannot be
anticipated at this time, thus, there may be a “home” for an autism leadership unit that will
become apparent within a new structure.
Tennessee Center for Autism Spectrum Disorders
The proposed Tennessee Center for ASD would be the “mother ship” of current knowledge
and best practices in the area of ASD that would relate to the regions within Tennessee. The
Tennessee Center for ASD should ideally be located at Vanderbilt University, due to its
current resources and activities in the area of ASD. Vanderbilt houses several autism-specific
entities including: 1) the Treatment and Research Institute for Autism Spectrum Disorders
(TRIAD) located in the Division of Child Development, which is well-known for its
diagnostic clinic for developmental disabilities; 2) the Kennedy Center that studies
developmental disabilities and includes the Susan Gray School which includes children with
autism spectrum disorders in its developmental preschool program, 3) the Vanderbilt Bill
Wilkerson Center, which provides speech-language and other services to children with ASD.
The Tennessee Center might best be located under the umbrella of the Division of Child
Development in the Department of Pediatrics, which is the organizational home of TRIAD,
which has been the most significant research and training center on autism spectrum disorders
in the state.
The Tennessee Center for Autism Spectrum Disorders would have three main functions
including:
• Research
• Training
• Dissemination/information and referral.
Research. The Tennessee Center for ASD will conduct studies on the early identification of
autism spectrum disorders, incidence rates of ASD in Tennessee, best practices for ASD
intervention, and evaluation studies on this proposed statewide infrastructure. TRIAD’s
Autism Services Proposal
SJR 567
33
faculty has produced a body of research on screening and assessment of ASD. This research
will continue with the research support that TRIAD has obtained from federal sources. Some
additional research activity should be funded by the state of Tennessee to support
development and evaluation of services for children with ASD. In addition, the Tennessee
Center for ASD will pursue grants from federal and other sources for special projects as
needed.
Training. The Tennessee Center for ASD will assume the role of providing consultation,
training, and quality oversight to the five regional ASD Centers of Excellence (COEs) and to
Educational ASD Teams located in each of the eight regional offices of the Department of
Education (DOE). The Tennessee Center staff will ensure, through a certification process,
that all the professionals at the COEs have specific ASD expertise, and will train the DOE
staff to the level of expertise such that they could then replicate training for educators within
the eight DOE regions. Thus, the training function will be an extensive part of the Tennessee
Center’s responsibility. The Tennessee Center for ASD will also provide ongoing
consultation regarding identification, assessment, and intervention with children with ASD, as
well as dissemination of current research findings to keep the staff in these centers abreast of
advances in the field.
Other training functions of the Tennessee Center for ASD will be to provide training for
primary care providers on screening for ASD and work to support broader use of screening
instruments in primary care. In addition to training PCPs, the state center will coordinate
training through other parts of this system (e.g., regional centers) to mental health providers,
speech and language therapists, occupational therapists, physical therapists, institutions of
higher learning, and parents should also be part of the plan.
Finally, there should be an expanded continuation of the current contract with the Department
of Education in which educators are trained statewide by TRIAD. The five regional resource
ASD centers of excellence and the eight DOE teams should be trained to help extend the
TRIAD training.
Dissemination. Dissemination of best practices will be the third component of the Tennessee
Center. The Tennessee Center will work to create a state of the art, ASD information center
and will disseminate both electronically and otherwise the best practices and treatment
breakthroughs to providers and consumers within the state.
In the related area of information and referral, the Tennessee Center would connect with the
existing state-supported information and referral services for developmental disabilities at the
Kennedy Center at Vanderbilt (“Pathfinders”) in order to enhance the ASD referral
information within that system. While the information and referral system would be overseen
as is, the Dissemination unit of the Tennessee Center would collaborate closely with the
Kennedy Center to develop and maintain the ASD specific components of that network.
Regional Autism Spectrum Disorder Centers of Excellence
In addition to the Tennessee Center for ASD, autism expertise will be developed at five
Regional ASD Centers of Excellence (COEs). These COEs are essential to the coordinated
Autism Services Proposal
SJR 567
34
system of care called for in SJR 567. The regional COEs will be the “hub of the wheel” in
terms of ensuring that health-related autism-specific services reach the level of the individual
child. The primary functions of these COEs will be:
•
•
•
•
•
•
•
•
to conduct comprehensive, ASD specific, multidisciplinary evaluations
to facilitate care plans and provide ongoing consultation to providers within the
designated regions
to provide triage services for children with ASD
to provide enhanced care coordination to families within the regions
to provide training to providers and within institutions of higher learning
to disseminate information to providers and parents
To act as liaisons within the schools to ensure IEPs are adequate and goals are met
To act as liaisons to pull the required agencies together (per IDEA) to plan
transitional services for students aging out of high school
In order to build on an existing infrastructure, the COEs should be located as special units
within the already existing Centers of Excellence for Children in State Custody. These five
COEs, four of which are operational (one is still in contract negotiation), are in the following
locations:
•
•
•
•
•
University of Tennessee in Memphis at its Boling Center for Developmental
Disabilities (Memphis)
Vanderbilt University (Nashville)
East Tennessee State University (Johnson City)
East Tennessee Children’s Hospital/ Cherokee Behavioral Health Systems
(Knoxville)
TC Thompson Children’s Hospital/Focus Psychiatric Group (under contract
negotiations) (Chattanooga)
Each COE’s current leadership would develop its ASD unit to best draw on its current staff as
well as to maximize the ASD resources within its respective region. Each COE would
collaborate closely with the ASD Team of each Department of Education region within the
COE’s geographic area to provide consultation, care coordination, and multidisciplinary
assessment for complex cases. The geographic DOE regions would break out as follows:
• University of Tennessee – Memphis, Boling Center will serve two DOE regions
(Northwest and Southwest);
• Vanderbilt University will serve three DOE regions (Mid-Cumberland, South
Central, and Upper Cumberland);
• East Tennessee State University will serve one DOE region (Northeast);
• East Tennessee Children’s Hospital/Cherokee Health Systems center will serve
one DOE region (East);
• T.C. Thompson Children’s Hospital/Focus Psychiatric Services center will serve
one DOE region (Southeast).
Autism Services Proposal
SJR 567
35
Each regional center will have professional resources to include:
• a developmental pediatrician;
• a child psychiatrist;
• a child psychologist;
• a behavioral interventionist;
• an educational specialist;
• a speech and language pathologist;
• an occupational therapist;
• a physical therapist;
• a family resource specialist, knowledgeable about service resources within the
region and connected to families of children with ASD;
• a cadre of ASD services liaisons that will serve as specialized care coordinators
and will be located throughout each region. The family resource specialists at each
COE will supervise this cadre of liaisons.
ASD services liaison staff will report to the family resource specialists in the COEs but will
be home-based, equipped with a laptop computer, fax machine, and pager for communication
with the COEs, DOE teams, schools, and families. These staff persons will have skills to
support parents to become expert advocates for their own children. They will serve as a point
of access to the full range of services for children with ASD and their families. To do so, they
will be knowledgeable about services in all relevant departments of state government and
knowledgeable about medical, psychological, and other therapeutic resources in their area.
They will function as “boundary spanners” who are not limited by departmental lines but
bring services together to address the needs of individual children and their families. These
staff will have training in ASD and will have access to training from the Tennessee Center,
the COEs, and the DOE teams. ASD services liaison staff will work with parent groups in
their area and work on development of parent volunteers in connection with the family
resource specialist from each COE.
Regional Educational Autism Spectrum Disorder Teams
Each of the eight regions of the Department of Education (DOE) will have an ASD Team.
These teams will be administratively organized under the State DOE through the three grand
regions of DOE (West, Middle, and East). The ASD Teams will include:
•
•
•
a special educator with ASD training and experience
a speech and language pathologist with ASD training and experience
a behavioral interventionist with ASD training and experience
Each ASD Team will receive certification training from the Tennessee Center for ASD and
will maintain communication with the Tennessee Center for ongoing training. Each ASD
Team will receive updates on research from the Tennessee Center so that they will be kept
current with developments in the field of ASD. The ASD Teams will provide both replication
TRIAD workshops for educators as well as the ongoing, hands-on consultation within local
schools in their particular region in order to enhance the training of special educators who
have gone through the TRIAD workshops. As mentioned earlier, the need for follow-up with
Autism Services Proposal
SJR 567
36
educators who are instructing specific children each with unique challenges, has been a large
gap in the training program currently in place. Each ASD Team will also communicate
regularly with the regional COE for assessments and for liaison services as described above.
XIV. ASD Advisory Councils
Advisory councils should occur at two levels. Currently, the already established COEs for
children in state custody have quarterly meetings, which include the COE leaders as well as
advisors.
The ASD COEs should be overseen in a similar manner. Each ASD COE should have local
representatives (providers, parents, and other stakeholders) who would participate in quarterly
meetings to discuss the operations of the ASD service delivery system. Representatives from
the Tennessee Center should be present at these meetings and the leadership should be from
the state level government oversight unit.
At the second level, the Tennessee Department of Mental Health and Developmental
Disabilities has had a State Mental Health Planning and Policy Council for many years. Seven
regional councils composed of various stakeholders, including consumers of mental health
services represent this council. With the recent expansion in Title 33 for Developmental
Disabilities to be uniquely considered, TDMHDD has recently implemented seven regional
DD councils that will be represented at a newly formed State Policy and Planning Council for
Developmental Disabilities. The mission of this group will be to assist in the planning of a
comprehensive array of high quality prevention, early intervention, treatment, and habilitation
services and supports and to advise the DMHDD on policy, budget requests, and developing
and evaluating services and supports. To this end, it is important to have representation from
families of children with ASD. At each regional level, there should be representation from
families and providers of children with ASD and there should be representation at the state
level also. It is hoped that the regional DOE and COE units in connection with the Autism
Society chapters in Tennessee will be instrumental in facilitating representation within this
council structure. The regional representatives should have a close connection with staff at
the Tennessee Center in order to be kept abreast of best practices.
XV. Network Development
Network development should concentrate on:
•
•
•
Provider training in the field
University training for burgeoning professionals
Pilot projects
Development of the network of providers of services will require training for professionals of
many different types: pediatricians, family physicians, psychiatrists, psychologists, educators,
special educators, speech therapists, occupational therapists, behavior interventionists,
physical therapists. The Tennessee Center for ASD, the regional Centers of Excellence, and
Autism Services Proposal
SJR 567
37
the Department of Education regional ASD Teams will provide a variety of training
experiences and follow-up to develop the competencies of these professionals to provide
services for children with ASD and their families.
These centers will also recruit experts from within the state as well as recruit out-of-state
experts to come to Tennessee to participate in the development of services for children with
ASD and their families.
In addition, it is essential that the university training of professional, graduate, and
undergraduate students in the professions serving children with ASD include training on ASD
and experience in working with children with ASD. The Tennessee Center on ASD and the
regional COEs will serve as a resource to universities regarding appropriate curriculum
content for training programs for professionals such as speech and language pathologists,
occupational therapists, physical therapists, mental health and medical professionals.
Another aspect of developing the network of services for children with ASD and their families
is to fund pilot projects for model services such as model classrooms at various levels of the
educational system. While the preschool programs will emphasize intensive early intervention
“learning how to learn” approaches, the high school model classrooms should emphasize
transition to post-school education and work.
XVI. Evaluation Component
Evaluation of the effectiveness of services will be important for assessment and development
of services for children with ASD and their families. The Tennessee Center for ASD will take
the lead role in research and evaluation and will guide measurement and data collection by the
DOE ASD Teams, the COEs, and others providing services to children with ASD. One goal
of evaluation will be to develop effective methods of measuring progress of individual
children toward their IEP goals. Compilation of data on progress will provide a database for
evaluation of intervention methods and information on studies of intervention methods will be
disseminated through the service system. Effectiveness data, outcome data, and financial
data will be analyzed to assess cost-benefit characteristics of services. Additional studies will
be designed to address family outcomes and satisfaction with services. Administrative studies
such as frequency of complaints, disputes, and litigation related to services for children with
ASD will also be conducted. Some states have already implemented solid evaluation methods
for ASD services (e.g., New York; see http://web.nysed.gov/vesid/sped/autism/apqi.htm).
XVII. Financing Services for Children with ASD and their Families
Children with ASD have complex needs that require multi-disciplinary services that inevitably
span across multiple potential funding sources within the current structure of the state of
Tennessee. It is imperative that the state designate a group of policy makers to create clear
policies about payment sources and services along with clear utilization review criteria for
serving children with ASD.
Autism Services Proposal
SJR 567
38
The most significant expenditures in providing services for children with ASD are
educational, spanning from the time a developmental problem is found through the transition
out of the school system in early adulthood. A large portion of these expenses are already
borne by schools through federal and state funds, but additional funding will be necessary
both to improve the services provided to children and their families and to cope with the
increasing numbers of children with ASD to be served by the schools. Additional services to
be funded include in-home behavioral interventions, particularly in the early years (from
infancy to age eight); greater availability of speech and language therapy, particularly in the
early years; more intensive behavioral programs in the schools, and improved transition
services in both the early and the later years of schooling.
TennCare is an important source of funding for those children who are TennCare eligible.
With approximately 40% of all Tennessee children enrolled in TennCare, a significant portion
of the health and behavioral health services required for children with ASD is funded through
TennCare. Children with TennCare Medicaid coverage are entitled to medically necessary
health and behavioral health services. For routine medical care, TennCare works well for
children with ASD according to the recent survey. However, for specialized services specific
to the ASD diagnosis, such as speech therapy, occupational therapy, and physical therapy,
there continues to be a lack of clarity regarding which services should be provided by the
managed care companies and which through special education services. Furthermore, as
stated elsewhere in this document, there are explicit clauses in the BHO contract that exclude
serving children’s behavioral problems if due to a diagnosis of ASD.
For children not included in eligibility for TennCare, there is a need for a regulatory body
(e.g., Dept. of Commerce and Insurance) to review the commercial insurance policies in order
to enforce that ASD is not excluded from major insurance carriers. At this time, some of the
major companies will not accept children with ASD on their policies, even for routine medical
care.
There are several possibilities for a funding structure that need further consideration either
singularly or in combination. However, a subgroup of financial advisors is needed to think
through the cost-benefit issues involved in various funding strategies for children with ASD.
This group should:
•
•
•
•
•
•
Clearly delineate available funding sources from state, federal, and private entities
Ensure that Tennessee is drawing down all available funds from Federal and other sources
(e.g., foundations)
Clearly designate a person or entity that is in charge of authorizing funding once a funding
plan is designed.
Conduct a thorough lifespan cost-benefit analysis of treating ASD in Tennessee
Consult with experts from other states that have statewide ASD service delivery (e.g.,
North Carolina)
Consider various funding strategies such as:
Use blended funding (e.g., DOE, DCS, DMRS, TennCare, DOH)
Write a demonstration waiver for long term solutions to serving this population
Autism Services Proposal
SJR 567
39
Create a collaborative waiver model with Education as the primary source of
services and funding, but in partnership with other funding sources such as private
and public insurance. Such a model has been designed in other states and requires
that families who are not Medicaid eligible must cooperate by using their private
insurance as a supplemental form of payment for services.
Create a funding unit for children with special health care needs, much like the
model already operating under TennCare Select for children in state custody.
Direct funds to the Tennessee Respite Coalition for ASD specific respite care
Once this information is in place, there should be clarity about “who pays for what” or a new
model from which to draw down funds and direct services. Whatever the funding structure,
the proposed organizational model for ASD services will need to be funded on a yearly basis.
Estimated Costs for a Statewide Model for ASD Services
North Carolina has operated a statewide model for delivering ASD services since a legislative
directive in 1972. Division TEACCH stands for Treatment and Education of Autistic and
Related Communication Handicapped Children. Division TEACCH is funded annually by the
North Carolina legislature, tied to land grant universities. Operating with nine Regional
Centers that has a single executive director, TEACCH provides diagnostic evaluation,
individualized curriculum development, social skills training, vocational training, and parent
counseling and training all free to families. Division TEACCH provides these services for
over 5,000 persons with autism, both child and adult, however, the root of the division began
as a child-oriented service and has grown to include the lifespan.
The annual budget for Division TEACCH is $4,655,479. This does not include funding for
the model TEACCH classrooms or any educational costs. The educational costs are funded
directly through the NC Dept. of Public Education Services. NC state funds cover 140 staff
salaries out of 325 total TEACCH staff. The remaining funding comes from Medicaid
dollars.
Proposed budget estimate for the new Tennessee organizational model
The model proposed for Tennessee is more extensive than that in North Carolina. The
proposed Tennessee Center for ASD will have more extensive training and dissemination
functions than Division TEACCH; will provide direct involvement of DOE services; and will
provide some direct services through the COEs over and above diagnostic and consultative
services (e.g., liaison services; medication management).
A spreadsheet in Appendix I includes estimated costs for the Tennessee model proposed in
this document. While state-only dollars must be designated for this proposed model, it is
possible that a federal grant could be obtained to demonstrate the effectiveness of this type of
statewide model. Perhaps a blending of state and federal dollars could be achieved once the
Tennessee Center is operating and able to write a demonstration grant. The overall cost is
estimated to be $6,571,500 and will cover the following features:
Autism Services Proposal
SJR 567
40
ASD research
Statewide training to:
Enhance expertise of professionals in the health-related fields
Enhance training programs in university professional training programs
Enhance training of educators
Enhance training of parents
Regional diagnostic capacity
Regional consultative/treatment planning capacity
Some regional, direct services (e.g., medication management)
Regional family resource specialist to aid families
Locally-based service liaisons to provide care coordination to families
Regionally-based school consultative and direct services available to local school
districts
Liaison service within local schools (e.g., IEP meetings; transition planning)
Final recommendations
The original broad goals of this study included:
Generate better outcomes for children with autism and their families
Reduce overall, long-term costs by providing effective services early and intensively
Minimize legal risk exposure for the state of Tennessee
In order to reach these goals the state must ensure that there are adequately funded
services that will reach families and children with ASD. BY providing evidence-based
treatments early in development, the state can save money over the long run. BY
providing the right kinds of services and helping families afford these services, the state
will be less vulnerable to lawsuits around ASD services. While this document contains
much of our current understanding of ASD and of the services needs in Tennessee, there
are several next steps that must occur in order to best implement this plan. These steps
include:
Create a subgroup that examines more closely the financial aspects of this plan
Create an implementation task force for the plan; use some of the same committee
members that have contributed thus far to the plan; draw on the faculty at TRIAD
and the staff at the current COEs; draw on the Autism Society of America
members
Make funds available in the budget for the plan
Discern the government “home” for the oversight of the plan
Autism Services Proposal
SJR 567
41
XVIII. References
Aman, M.G., & Langworthy, K.S. (2000). Pharmacotherapy and hyperactivity in children
with autism and other pervasive developmental disorders. Journal of Autism and
Developmental Disorders, 30, 451-459.
American Academy of Pediatrics, Committee of Children with Disabilities. (2001) The
pediatrician’s role in the diagnosis and management of autism spectrum disorder in children.
Pediatrics, 107, 1221-1226
American Academy of Pediatrics Policy Statement. (2002). The Medical Home. Pediatrics,
110, 184-186.
American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental
Disorders: Fourth Edition, Text Revision. Washington, DC: American Psychiatric
Association.
Autism Society of America Fact Sheet, 2002. Bethesda, MD. www.autism-society.org
Barnard, L., Young, A.H., Pearson, J., Geddes, J., et al. (2002). A systematic review of the
use of atypical antipsychotics in autism. Journal of Psychopharmacology, 16, 93-101.
Cohen, D.J., & Volkmar, F.R. (1997). Handbook of autism and pervasive developmental
disorders (2nd edition). New York, NY: John Wiley & Sons, Inc.
Committee on Educational Interventions for Children with Autism, National Research
Council (2001). Educating children with autism. Washington, D.C.: National Academies
Press.
Dawson, G. & Osterling, J. (1997). Early intervention in autism. In M. Guralnick (ed.) The
Effectiveness of Early Intervention p. 307-326. Baltimore, MD: Paul H. Brookes Publishing.
Dworkin, P.H. (1989). British and American recommendations for developmental
monitoring: the role of surveillance. Pediatrics, 84, 1000-1010.
Filipek, P.A., Accardo, P.J., Ashwal, S., Baranek, G.T., Cook, E.H., Dawson, G., Gordon, B.,
Gravel, J.S., Johnson, C.P., Kallen, R.J., Levy, S.E., Minshew, N.J., Ozonoff, S., Prizant,
B.M., Rapin, I., Rogers, S.J., Stone, W.L., Teplin, S.W., Tuchman, R.F., Volkmar, F.R.
(2000). Practice parameters: Screening and diagnosis of autism: Report of the quality
standards subcommittee of the American Academy of Neurology and the Child Neurology
Society. Neurology, 55, 468-479.
Glascoe, F.P. (1998). Collaborating with parents: Using Parents' Evaluation of
Developmental Status to detect and address developmental and behavioral problems.
Nashville, Tennessee: Ellsworth & Vandermeer Press.
Autism Services Proposal
SJR 567
42
Glascoe, F.P. & Dworkin, P.H. (1993). Obstacles to effective developmental surveillance:
Errors in clinical reasoning. Journal of developmental and behavioral pediatrics, 14, 344-349.
Gordon, C.T. (2000). Commentary: Considerations on the pharmacological treatment of
compulsions and stereotypies with serotonin reuptake inhibitors in pervasive developmental
disorders. Journal of Autism and Developmental Disorders, 30, 437-438.
Guralnick, M.J. (1998) Effectiveness of early intervention for vulnerable children: A
developmental Perspective. American Journal of Mental Retardation, 102, 319-345.
Hurth, J. Shaw, E., Izeman, S.G., Whaley, K., Rogers, S.J. (1999). Areas of agreement about
effective practices among programs serving young children with autism spectrum disorders.
Infants and Young Children, 12, 17-26.
Ireton, H. (1992). Child Development Inventory. Minneapolis, MN: Behavior Science
Systems.
Jacobson, J.W., Mulick, J.A., and Green, G. (1998). Cost-benefit estimates for early intensive
behavioral intervention for young children with autism—general model and single state case,
Behavioral Interventions, 13, 201-226.
Jarbrink, K., Knapp, M. (2001) The economic impact on autism in Britain, Autism, 5, 7-22.
King, B.H. (2000). Pharmacological treatment of mood disturbances, aggression and selfinjuring in persons with pervasive developmental disorders. Journal of Autism and
Developmental Disorders, 30, 439-445.
Lovaas, O.I. (1987). Behavioral treatment and normal intellectual and educational
functioning in autistic children. Journal of Consulting and Clinical Psychology, 55, 3-9.
Majnemer, A. & Rosenblatt, B. (1994). Reliability of parental recall of developmental
milestones. Pediatric Neurology, 10, 304-308.
McDougle, Kresch, & Posey, (2000). Repetitive thoughts and behavior in pervasive
developmental disorders: Treatment with serotonin reuptake inhibitors. Journal of Autism
and Developmental Disorders, 30, 427-435.
McEachin, J.J., Smith,T., & Lovaas, O.I. (1993). Long term outcome for children with autism
who received early intensive behavioral treatment. American Journal on Mental Retardation,
97, 59-372.
M.I.N.D. Institute, University of California, Davis. (2002). Report to the legislature on the
principal findings from the epidemiology of autism in California: A comprehensive pilot
study R. S. Byrd, MD, MPH, principal investigator.
Autism Services Proposal
SJR 567
43
Minshew, N., & Rattan, A. (1992). The clinical syndrome of autism. In S. Segalowitz & I.
Rapin (Eds.) Handbook of neuropsychology: Child neuropsychology (Vol. 6, pp.401-441).
Amsterdam, The Netherlands: Elsevier.
New York State Department of Health Early Intervention Program. (1999). Clinical Practice
Guideline: Autism/Pervasive Developmental Disorders. New York: New York State
Department of Health.
Office of the Surgeon General. (1999). Mental health: A report of the Surgeon General.
Washington, D.C.: US Government Printing Office.
Romanczyk, R., Matey, L., & Lockshin, S.B. (1994). The children’s unit for treatment and
evaluation. In Preschool Programs for Children with Autism by S. L. Harris and J. S.
Handleman. Austin, TX: Pro-Ed Publishers.
Robins, D.L., Fein, D., Barton, M.L, & Green, D.A. (2001). The modified checklist for
autism in toddlers: An initial study investigating the early detection of autism and pervasive
developmental disorders. Journal of Autism and Developmental Disorders, 31, 131-144.
Ruble, L.A., Heflinger, C.A., Renfrew, W., & Robson, D. (in press). Medicaid managed care
and children with autism spectrum disorders. 15th Annual Research Conference Proceeding
on A System of Care for Children's Mental Health.
Strain, P.S., Wolery, M., & Izeman, S. (1998). Considerations for administrators in the design
of service options for young children with autism and their families. Young Exceptional
Children. 8-16.
Tuchman, R. (2000). Treatment of seizure disorders and EEG abnormalities of children with
autism spectrum disorders. Journal of Autism and Developmental Disorders, 30, 485-489.
Autism Services Proposal
SJR 567
44
APPENDIX A
Senate Joint Resolution Letter (SJR 567)
Letter from the Tennessee Commission of Children and Youth to Dr. Joe
McLaughlin
Letter from the Tennessee Commission of Children and Youth to Dr. Fredia
Wadley
Autism Services Proposal
SJR 567
45
Autism Services Proposal
SJR 567
46
Autism Services Proposal
SJR 567
47
Autism Services Proposal
SJR 567
48
Autism Services Proposal
SJR 567
49
Autism Services Proposal
SJR 567
50
APPENDIX B
List of Participants
Autism InterAgency Study Group Membership
State Workgroup
(held approximately weekly from Sept. 11th – Dec. 11th)
co-chairs:
Patti van Eys, Ph.D. Children’s Health Initiative
Joe McLaughlin, Ph.D. Children’s Health Initiative
Brenda Bledsoe
Department of Education
Tennessee Early Intervention System
Denny Dukes*, MSSW
Associate Director
UT Children’s Mental Health Services Research Center
UT School of Social Work
Karen Edwards, Ph.D.
Psychologist
Consultant to Department of Mental Health and Developmental Disabilities
Gayle Feltner, MS
Education & Family Services Director
Division of Mental Retardation Services
Kacie Fitzpatrick, MA
Child Health Advocate
Implementation Team
Department of Health
Patti Killingsworth, BS
Disabilities Coordinator
Office of Health Services/Bureau of TennCare
Paige Kisber
UTK
* parents of a child(ren) with autism
Autism Services Proposal
SJR 567
Michael McSurdy, MA
Director of Foster Care Services
Department of Children Services
Michael Myszka, Ph.D.
Psychologist, Medical Director’s Office
Bureau of TennCare
Linda Oneal, J.D.
Executive Director,
Tennessee Commission on Children and Youth (TCCY)
Steve Petty, BS
Legislative Specialist
TCCY
Kim Rush, Ed.S.
Mental Health Specialist III
Department of Mental Health and Developmental Disabilities
Debbie Shahla, MA
MH/DD planner
Department of Mental Health and Developmental Disabilities
Sara Smith*, MS
Adolescent Health Director
Maternal and Child Health Section
Department of Health
Ned Solomon, BA
Director, Partners in Policymaking
Tennessee Council on Developmental Disabilities
Laura Stewart, M.T.S., J.D.
Executive Assistant to the Commissioner
Health Care Advocacy, Department of Children Services
Linda Vandermeer, M.S.
Autism/Behavior/Programs & Services Director
Department of Education; Division of Special Education
* parents of a child(ren) with autism
51
Autism Services Proposal
SJR 567
Pat Wade
Director of Children’s Program Outcome Review Team
Tennessee Commission on Children and Youth
Wanda Willis, Executive Director
Tennessee Council on Developmental Disabilities
Diana Yelton, MSSW, MA
Department of Children’s Services Program Coordinator
Health Care Advocacy
Dept. of Children’s Services
Provider Workgroup
(met approximately every other week from Sept. 17- Dec. 11)
co-chairs: Patti van Eys, Ph.D.; Joe McLaughlin, PH.D.
The Children’s Health Initiative
William Allen, Ph.D.
Cherokee Behavioral Health Services
Debbie Cate, East Tennessee Regional Resource Center
Department of Education
Tom Catron, Ph.D.
Vanderbilt University Center of Excellence
Larry Faust, MD
Implementation Team, Department of Health
Tim Goldsmith, Ph.D.
Director of Clinical Services,Youth Villages (Memphis TN base; statewide services)
Al Hardy, MA
TEIS service coordinator (Lawrenceburg, TN)
Gaye Hardy, MA
Director, Unique Personalities (Lawrenceburg, TN)
*parents of a child(ren) with autism
52
Autism Services Proposal
SJR 567
Jennifer Nietfeld, MA
Director, SAIL (Strategies for Autism through Individualized Learning)
Marcy Rehse, MA
educational consultant (private practice)
Dana Simpson, MA
Southern Middle TN Children’s Coalition (Franklin County)
Behavioral Consultant (Warren County)
Janet Todd, Ph.D.
UT-Boling Center; Center of Excellence (Memphis)
Parent/advocate work group
(met once as a group; some participated in later meetings with the State and Provider work
groups)
co-chairs:
Patti van Eys, Ph.D.
The Children’s Health Initiative
Joe McLaughlin, Ph.D.
The Children’s Health Initiaitve
Dena Brown, MA, parent
Janet Curry, parent (Giles County)
Tammie Fleming (statewide advocate)
Tennessee Voices for Children
Debi Haney, parent (Knox County)
John McCaskill, parent (Henderson County)
Teri Phillips, parent (Rutherford County)
Jeff Romanczuk, MS parent (Sevier County)
Special Educator
Janet Shouse, parent (Williamson County)
Autism Society of Middle Tennessee
53
Autism Services Proposal
SJR 567
Consultants (did not attend the formal meetings described above)
Behavioral Health Advisory Committee to the Bureau of TennCare
Chair: Robert Atkins, MD
Psychiatrist, Shaller Anderson
Steve Camarata, Ph.D.
The Kennedy Center, Vanderbilt University
Anne Garfinkle, Ph.D
The Kennedy Center, Vanderbilt University
Jerry Heston, MD
Director, Division of Child Psychiatry
UT College of Medicine (Memphis)
Quentin Humberd, MD
Pediatrician, Premier Medical Group, Clarksville
Gina Hummel, Ph.D.
East Region Center of Excellence (Knoxville)
Susan McGuire, MD.
Director, SouthEast Region Center of Excellence (Chattanooga)
Robin McWilliam, Ph.D.
Child Development Center, Vanderbilt University
Fred Palmer, MD
Director, UT Boling Center for Developmental Disabilities (Memphis)
Cindy Perry, MS
Executive Director,
Select Committee on Children and Youth
Tennessee General Assembly
Andres Pumariega, MD
Director, ETSU Center of Excellence (Johnson City)
Mary Schaffer, MS
Speech and Language Pathologist,
Vanderbilt; Bill Wilkerson Center
Lisa Ruble, Ph.D.
University of Louisville
The Steering Panel for Children with Special Health Needs
Chair: Fredia Wadley, Commissioner of Health
54
Autism Services Proposal
SJR 567
Wendy Stone, Ph.D.
Diroector, TRIAD, Vanderbilt University
Mark Wolery, Ph.D.
The Kennedy Center, Vanderbilt University
Ruth Wolery, Ph.D.
The Kennedy Center, Vanderbilt University
55
Autism Services Proposal
SJR 567
56
APPENDIX C
Estimated Prevalence Rate of Children with Autism Spectrum Disorders by Tennessee County
County
Anderson
Bedford
Benton
Bledsoe
Blount
Bradley
Campbell
Cannon
Carroll
Carter
Cheatham
Chester
Claiborne
Clay
Cocke
Coffee
Crockett
Cumberland
Davidson
Decatur
DeKalb
Dickson
Dyer
Fayette
Fentress
Franklin
Gibson
Giles
Grainger
Greene
Grundy
Hamblen
Hamilton
Hancock
Hardeman
Hardin
Hawkins
Haywood
Henderson
Henry
Hickman
Houston
Humphreys
Jackson
Jefferson
Johnson
Knox
Estimated Prevalence Rate of ASD
Total
2 of every
3 of every
Population
1000
1000
Birth - 18
children
children
17,931
36
54
9,080
18
27
3,811
8
11
2,401
5
7
23,475
47
70
19,874
40
60
9,196
18
28
3,131
6
9
7,171
14
22
11,460
23
34
9,940
20
30
3,637
7
11
7,167
14
22
1,626
3
5
7,462
15
22
12,440
25
37
3,508
7
11
9,405
19
28
137,726
275
413
2,370
5
7
3,563
7
11
11,953
24
36
9,896
20
30
8,233
16
25
3,865
8
12
8,855
18
27
12,077
24
36
7,460
15
22
4,555
9
14
13,283
27
40
3,535
7
11
13,137
26
39
74,162
148
222
1,625
3
5
7,152
14
21
6,433
13
19
11,379
23
34
5,634
11
17
5,653
11
17
6,597
13
20
4,803
10
14
1,818
4
5
4,081
8
12
2,043
4
6
8,938
18
27
3,387
7
10
89,449
179
268
Autism Services Proposal
SJR 567
Lake
Lauderdale
Lawrence
Lewis
Lincoln
Loudon
Macon
Madison
Marion
Marshall
Maury
McMinn
McNairy
Meigs
Monroe
Montgomery
Moore
Morgan
Obion
Overton
Perry
Pickett
Polk
Putnam
Rhea
Roane
Robertson
Rutherford
Scott
Sequatchie
Sevier
Shelby
Smith
Stewart
Sullivan
Sumner
Tipton
Trousdale
Unicoi
Union
VanBuren
Warren
Washington
Wayne
Weakley
White
Williamson
Wilson
TOTAL
57
1,509
7,047
10,847
2,562
7,741
8,985
4,613
23,764
6,957
6,846
18,975
11,230
5,751
2,109
8,399
34,826
1,239
4,501
7,667
4,344
1,770
1,036
3,132
14,512
6,655
11,082
14,700
45,554
5,445
2,606
14,901
260,019
4,051
4,206
33,846
32,235
14,695
1,565
3,422
4,086
1,114
8,951
22,499
4,169
8,110
5,371
30,840
22,926
3
14
22
5
15
18
9
48
14
14
38
22
12
4
17
70
2
9
15
9
4
2
6
29
13
22
29
91
11
5
30
520
8
8
68
64
29
3
7
8
2
18
45
8
16
11
62
46
5
21
33
8
23
27
14
71
21
21
57
34
17
6
25
104
4
14
23
13
5
3
9
44
20
33
44
137
16
8
45
780
12
13
102
97
44
5
10
12
3
27
67
13
24
16
93
69
1,399,787
2,797
4,200
Autism Services Proposal
SJR 567
58
APPENDIX D
Blank Survey Form from the 2002 SJR 567 Workgroup
Documents form Prior State Workgroups Regarding Autism
Informal Working Paper by Lisa Ruble, Ph.D., Vanderbilt University, TRIAD
Autism Services Proposal
SJR 567
59
SURVEY FOR THE LEGISLATURE
Survey on Services for Children with Autism Spectrum Disorders:
A Report to the Tennessee Legislature
The Children’s Health Initiative needs your input for an imminent legislative proposal regarding services for
Tennessee children with Autism Spectrum Disorders. Our goal is to communicate to the legislature the current status
of such services and to propose a more adequate service array and delivery system.
If you are a resident of Tennessee, please take a few minutes to fill out this survey.
County of residence: ___________________________
1.
2.
3.
4.
a.
b.
5.
a.
b.
Please put a check mark where applicable:
Are you a:
a. ___ parent of a child with autism
b. ___ Educational provider
c. ___mental/behavioral health provider d.____ medical provider
e. ___ policy maker
f. ___ other ____________ (list)
If you are a parent, how old is your child(ren)? ___________
If you are a provider, how long have you been in the field? _______
If you are a provider, have you had autism specific training? ___yes ___no
If yes, please specify:
_____________________________________________________________________________________________
_________________________________
If yes, what services do you now provide?____________________________
Rate (check) the following services in terms of their availability and ability to serve children with
autism and their families in your geographical region:
Speech/Language
____Adequate ____Inadequate
Explain if needed:
_____________________________________________________________________________________________
_________________________________
Educational Services ____Adequate ____Inadequate
Explain if needed:
_____________________________________________________________________________________________
_____________________________________________________________________________________________
______________________________________________________________________________c. Systems
coordination: ____ Adequate ____Inadequate
Explain:
_____________________________________________________________________________________________
_______________________________________
d. Mental Health/Behavioral Health: _____Adequate ____Inadequate
Family Counseling :
_____Adequate ___Inadequate
Sibling counseling:
_____Adequate
___Inadequate
Behavioral Interventions _____ Adequate ___Inadequate
Psychiatric Medications _____ Adequate ___ Inadequate
TURN PAGE OVER
Explain any of above regarding behavioral health services:
_____________________________________________________________________________________________
_______________________________________
__________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
____________
e. Medical Services (excluding psychiatric) ____ Adequate
___Inadequate
Autism Services Proposal
SJR 567
60
Explain:
_____________________________________________________________________________________________
_______________________________________
f. Other family services:
___Adequate __Inadequate
Respite
___ Adequate ___Inadequate
Home modifications
___Adequate __Inadequate
Personal Assistance/Care ___Adequate __Inadequate
Explain:
_____________________________________________________________________________________________
_______________________________________
g. In general, what do you see as most needed in your geographical area?
__________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
____________
h. In general, what do you think are the main barriers to adequate services for children with autism in Tennessee?
__________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
____________
i.
What do you think is the best service(s) in your area? What has been most helpful to you?
__________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
__________
Thank you for helping us with this survey. You may leave it in the basket marked “Return Legislative Survey” out
in the display area, or you may FAX it to: 615-532-1383 (attn: CHI). If you want to take the survey home for others
to fill out and FAX back, please do so!
The Children’s Health Initiative
706 Church Street; Dr. Bldg. 5th floor
Nashville, TN 37247
615-253-5503
Autism Services Proposal
SJR 567
61
Comments to the Select Oversight Committee on TennCare
Regarding SB 235/HB 1021: Behavioral Health Services for Autistic Children
Date: April 19, 1999
Presented by:
Executive Director, Cindy Perry
Select Committee on Children and Youth
Tennessee General Assembly
Background
•
•
•
•
•
•
•
•
The Select Committee on Children and Youth (SCCY) conducted two (2) hearings
during 1998 on issues and concerns related to special education service delivery for
disabled children. Autism was discussed extensively as a part of those hearings.
Findings indicate that autism is a neurological disorder that occurs in the brain.
Specifically, autism affects individuals’ behavior and their ability to learn because of
how the disorder affects the brain. There is no medical cure for autism, although,
clinical research is necessary and on-going.
The onset of autism occurs in children, almost always between 0-3 years, and very
often between 18 and 30 months. Diagnosis of the disorder is typically made between
3 and 5 years of age. The incidence of autism is around 1 per 1,000 persons.
Autistic children’s ability to develop socially, emotionally, and cognitively is
compromised by this disorder. Most importantly, the autistic child’s ability to learn
and to be educated is directly compromised by this disorder. Two (2) factors related
to rehabilitating and teaching autistic children are {1} the level to which the disorder
is manifested in the person (i.e. severity) and {2} the level of treatment and
intervention provided (i.e. type, intensity and duration).
The good news is that autistic individuals can be rehabilitated and the effects of the
disorder on their lives can be treated, thus improving their quality of life and
functioning in their environment.
Timing of intervention services is a critical factor for autistic children. For all human
beings, 0-5 years old is the prime window of opportunity for learning essential life
skills. In fact, the emerging bank of knowledge about human brain development is
indicating that the first 33 months of life (including the nine month pre-natal period)
is the most critical period of human beings’ potential to live and learn functionally.
Of relevance to this public policy discussion is that there is no solid evidence to
support that the window of opportunity to learn is significantly different for autistic
children than for their non-autistic cohort. Therefore, like with all children and
especially with children who are in any way at-risk, early identification of deficits and
prompt intervention to rehabilitate them while in the high-impact learning stage of
life is good public policy.
During childhood and adolescence, the business of children is getting educated. The
education of disabled children affected by autism should be linked to the overall
efforts to rehabilitate them from the effects of the disorder. Therefore, with regard to
public service and support for children, it is important to frame interventions and
Autism Services Proposal
SJR 567
62
strategies against the backdrop of the public schools because that is the natural
environment of children.
Factors Effecting the Response to Autism
•
Because there are many “unknowns” in understanding and managing autism, and
because the response to intervention is very individualized, it is currently not possible
to effectively predict the outcomes and establish standardized treatment protocols for
intervening with autistic persons, especially children.
• There is, however, serious debate in the clinical and the public policy arenas about
how the modifying and controlling of conditioning (teaching) is best done to improve
the overall well-being of autistic people. Various models exist for the treatment and
rehabilitation of autism. It is very important to note, however, that traditional
therapeutic models and psycho-analytical approaches in service delivery do not work
effectively with autism.
• In the public policy arena, however, the debate is really about whether autism is a
medical condition and, therefore, health care systems should pay for care and
service. Or is autism a learning problem and, therefore, education should pay for
care and service. The reality is that in terms of total health and well-being and the
long-term cost impact on society, there is medical necessity coupled with
educational responsibility in order to rehabilitate and teach autistic children.
• TennCare Standard Operating Procedure #019, dated January 1,1994, addresses
the subject of MCO Responsibility to Provide Medical Treatment to Children
Receiving Special Education Services. It states in part:
"In the case of a TennCare-eligible child identified as eligible for special education as part of
the Individuals with Disabilities Education Act who is also identified as having "related
services" needs that must be met in order for the child to benefit from special education,
TennCare Managed Care Organizations (MCOs) are required to provide TennCare covered
services for TennCare children despite the inclusion of such services in the child's
individualized education program. ...Services such as occupational therapy, physical therapy,
speech therapy and any other TennCare covered services are the responsibility of the MCO."
(Copy of TSOP 019 is attached.)
•
Schools need medical expertise to effectively work with third-party payor sources to
assure that all disabled students receive the necessary and appropriate services based
on high quality individualized education plans (IEPs), and that appropriate funding
streams are utilized to cover the costs of said services. The Department of Health has
a small-scale program, Project TEACH, which is providing medical consultation to
LEAs to accomplish effective liaison with MCOs and BHOs. (Handout is attached.)
Comments on SB 235/HB 1021
As proposed, this bill sets forth a specific sub-group of disabled children as eligible for
TennCare reimbursement of behavioral services. It appears that current code and
administrative procedure already require this for the total population of disabled children,
as T.C.A. 71-5-107(a)(10) currently states "Medical screening, diagnostic and treatment
services of eligible categorically connected individuals under twenty-one (21) years of
age." And, administrative operating procedure of the Bureau of TennCare (TSOP #019)
Autism Services Proposal
SJR 567
63
requires coordination of effort between schools and managed care organizations to assure
delivery of and payment for services for TennCare eligible disabled children.
So the question is not "Should we make autistic children eligible for behavioral health
services?" But rather "How shall we assure that autistic children do in fact get behavioral
health and medical services that are expertise-based, and of an intensity and duration to
reasonably expect improved functioning and well-being?"
•
•
•
Expand the capacity of schools to obtain medical expertise in educational planning
for disabled children. Examine the effectiveness of Project TEACH through a study
of the utilization of the program by LEAs, and the cost assignment outcomes that
DOH staff involvement in determination of pay sources has yielded, i. e. how much
the schools have paid from their budgets and how much cost has been assigned to
MCOs and BHOs.
Assure that with the Bureau of TennCare's movement from Department of Health to
Department of Finance and Administration, the purpose and operation of Project
TEACH is maintained.
An expert in the field of autism for purposes of educating or treating an autistic child
should have at least five (5) years of experience and involvement with the population,
with documented emphasis and effort to understand various modes and models of
rehabilitation and teaching of autistic children from both the medical and educational
arenas. TennCare reimbursable services should be delivered by professionals meeting
this level of professional development; MCO provider networks should include such
expertise. Additionally, public schools should strive to have supervision of all staff
working with autistic children done by school personnel meeting this level of
professional development.
Autism Services Proposal
SJR 567
64
Autism Task Force
Summary of Residential/Respite Services for Autism
Betty Boner, Barb Brent, & Judy Regan
June 4,1999
Residential Services for Autistic Children:
Services:
1. Education: Education provides limited residential programs for autistic child (i.e.,
Rainswood)
2. MR Waiver: For those who qualify, MR will provide homes for individuals who
require additional support. MR usually tries to provide in-home services prior to
moving a child out of their home. MR always tries to place a child in a home setting.
3. BHO: BHOs provide residential psychiatric care for these individuals who are dually
diagnosed if their mental health needs require this level of Care.
4. DCS: DCS provides services for those children in their custody who require residential
services.
Conclusion:
MR offers quality residential services for autistic children who can be maintained in a
home setting. However, many times several questions may occur whose answers limit the
services:
• Does the individual qualify for services under the MR Waiver/State funded
services?
• Are there enough providers available: to) provide the residential services?
• Is there enough money to provide the residential services?
• Where is the individual on the waiting list?
Respite Care for Autistic Children:
Services:
I. Education: Currently Education does not provide respite care.
2. MR Waiver/State Funds: Some grants exist for state funded respite services. In
addition, some respite services are available through the waiver.
3. BHO: BHOs provide emergency respite care for psychiatric conditions.
4. DCS: DCS provides respite services for those children in their custody.
5. TN Voices for Children: TN Voices provides respite. Specifics are unknown at this
time.
Conclusion:
Respite care is provided mainly by MR. However, these services are limited by the above
questions raised under residential care (i.e., funding, availability, waiting list, qualification.)
Autism Services Proposal
SJR 567
65
Service Needs of Families and People with Autism in Tennessee
Lisa Ruble, Ph.D.
January 2001
(DRAFT written by Lisa Ruble, Ph.D. when she was a part of the Vanderbilt University
Medical Center, Division of Child Development, TRIAD)
Autism is among the most complex neurodevelopmental disorders. According to the U.S.
Department of Education (1999), autism is the largest growing low incidence disability in
public schools (Figure 1) and the third most common developmental disability (Autism
Society of America). Autism affects more than 2,000 children and 2,800 adults with
autism in Tennessee (Table 1).
The Tennessee Department of Education reported a 3-fold increase in number of students
with autism since 1992, from 367 to 967 (out of an expected 1,800) (Figure 2). The
Office of Vocational Rehabilitation reported serving 74 adults (out of an expected 2,800)
with autism in 2000. It is expected that more children and adults will be diagnosed with
autism as professionals become more knowledgeable.
The number of children receiving services and the types and costs of services provided by
agencies such as the Department of Mental Health and Developmental Disabilities
(DMHDD), TennCare, and Children's Special Services are unknown. A recent estimate
of the lifetime costs associated with autism is 4.35 million per person (Autism Society of
America; Malt by, 2000).
Types of Essential Services for Families and Individuals with Autism and TN
Agencies Responsible for Providing Services
Table 2 describes the various services needed by families and people with autism and the
corresponding state agencies responsible for such services. Case management, respite
care, in-home personal assistance, and other therapies like speech and language therapy,
behavior management therapy, parent training, and occupational therapy are necessary
for optimal growth and development of children with autism. In Tennessee, the
Department of Mental Health and Developmental Disabilities is the primary agency
responsible for providing necessary services for families. DMHDD offers a federally
funded Medicaid-Waiver Program and a state-funded Family Support Program. Parents
must wait years in order to receive services from DMHDD.
Children who receive TennCare are able to receive many services; however, it is
unlikely that many receive the services they are eligible for under the Early Periodic
Screening Diagnosis and Treatment (EPSDT) requirements as I have not yet met a family
who receives case management services or in-home behavioral support or personal
assistance.
The Department of Children’s Special Services (CSS) also provides a limited number
of services, including case management. Again, I have not worked with any families who
receive assistance from CSS.
Autism Services Proposal
SJR 567
66
Summary of Accessibility of State Services
Unfortunately, families have to wait several years to receive most of the services
available through DMHDD’s Medicaid-Waiver and Family Support Programs. My
experience with TennCare indicates that the special needs of children with autism is
unknown as almost all families receive no case management or EPSDT services designed
to promote the child’s development (such as in-home personal assistance). Finally,
Children’s Special Services, which reportedly provides services to children with autism,
is also difficult to access. I currently see 20 to 40 children with autism a month, and for
those living at home, none have a case manager, in-home personal assistance, or respite
care.
Evidence of Services Needs
The service needs of children, adolescents, and adults with autism and their families are
unknown in Tennessee. Only anecdotal evidence is available that illustrates the needs and
gaps in services for autism. Below are examples I have personally encountered in my
work as a clinical psychologist.
Issue: Lack of Case Management – Example from Franklin County
A school system from Franklin County called about a child who was in danger of hurting
himself. The child was receiving case management through a local mental health agency.
But as soon as the autism diagnosis was made aware to the agency, the case management
service was dropped. The family was told case management services can not be used for
children with autism.
Issue: Lack of Residential Options or Crisis Options – Example from Clarksville
and Maury County
A grandmother, who had custody of her grandson with autism, requested residential
placement for her grandson. She was told by DMHDD that services were not available
and that only crisis situations were given priority. She completed the application for the
Medicaid-Waiver Program, but learned several months later that the application was
never forwarded to Medicaid. She had to repeat the application process. In the meantime,
she was advised by DMHDD to give up custody of her grandson in order to receive
services. She refused this option. Eventually, she experienced medical problems and was
hospitalized, also her son (not the child's father) committed suicide. At this point, the
grandmother was unable to care for the child and contacted the local TV station. After
these episodes, the child was then placed on the Medicaid waiver and moved into a
supported living environment.
A mother from Maury County reported that she was afraid of her son, and his behavior
was getting out of control. She wanted to place him in a hospital for a medication
evaluation. The mother called the only Middle TN inpatient unit that works with
individuals with autism ( University Hospital of Lebanon) and was told that they only
take adults.
Comment: Several families have had similar experiences. They are in crisis, have
received no in-home personal assistance or case management, and have nowhere to turn.
One family did give their child up to the Department of Children's Services in order to
get help. This child is now inappropriately placed in a mental health facility and his
Autism Services Proposal
SJR 567
67
behavior has deteriorated. He has been removed from his local school due to challenging
behaviors. Medication is being used to treat behaviors rather than a positive behavior
support plan. When families contact DMHDD, they are told that the waiting lists are long
and that it will be years before they receive services. Many families feel hopeless. The
impact of a lack of services on families and the costs that families and the State of
Tennessee pay out of pocket for emergency procedures are unknown.
Issue: Lack of Respite Care- Example from Davidson County and many rural
counties {Blount County, Hardin County, Franklin County)
The Tennessee Respite Network, which is part of Tennessee Voices for Children, no
longer provides financial subsidy for respite care for children with autism. TN Voices for
Children does not work with children with autism. The Family Support Programs have
long waiting lists. Families have to hire their own providers. No training on autism for
respite providers is offered in TN.
Issue: Lack of TennCare (EPSDT) Services -Example from Davidson County
There is a Federal Medicaid Law stipulating the services available to children with
disabilities under EPSDT guidelines. No families have been able to access the range of
services described in EPSDT. One family who lives in Davidson County was unable to
acquire EPSDT services despite this law. The mother, who has a son with autism, has a
neuromotor condition that makes her unable to perform physical activities. She is unable
to cook, care for the children, clean, etc. The father has to do all the home-making
activities. When he has to take time off of work to care for his family and take his wife
and sons to appointments, he loses wages. The family contacted TennCare for EPSDT
services for case management and in-home personal assistance. The TennCare employee
who did not know what EPSDT was then referred the mother to a mental health center.
When the mother contacted the mental health center she was told that they don't work
with children with autism.
Another example comes from Davidson County .A 4-year child suspected of having
autism was on the inpatient unit in a psychiatric hospital. The family and a family
advocate were concerned that if the child was diagnosed with autism, he would receive
no services. The advocate, Tony Garr, of the TN Health Care Campaign reported that he
has worked with many families of children with autism and that the needs of these
children are not addressed when they have an autism diagnosis (children with severe
emotional disturbance (SED), have many options in TN through TN Voices for Children
and local mental health centers).
A clinical psychology doctoral student who was doing a practicum in a psychiatric
facility was encouraged by her supervisors to not diagnose autism as services for this
diagnosis was not reimbursed by insurance companies.
Issue: Lack of Services from Private Insurance -Examples from Davidson and
Williamson Counties
Many families want services such as speech and language therapy, behavior management
therapy, or social skills training. Some insurance companies deny any coverage when the
child is diagnosed with autism, Asperger's syndrome, or Pervasive Developmental
Disorder- Not Otherwise Specified -all autism spectrum disorders. One child was denied
any health care coverage due to his diagnosis of autism.
Autism Services Proposal
SJR 567
68
Recommendations
Our biggest recommendation is for a comprehensive description of current needs and
gaps in services that can be used to develop a State-Wide autism plan. For the current
legislative session, the Autism Society of Middle TN has generated the following
legislative initiatives:
Legislative Initiatives
TennCare EPSDT Services
Private Services Personnel Training
Social Services Personnel Training
State Autism Plan
State Autism Center
Description of Legislation
Autism Services Proposal
SJR 567
69
APPENDIX E
Exclusionary Language Regarding Developmental Disabilities
Found in the Contract Between TennCare and the BHO
(Compiled by an informal workgroup headed by Patti van Eys, Ph.D.)
The TennCare contract with the BHO excludes Mental Retardation/Developmental Disabilities
(MR/DD) from the category of covered mental illnesses as defined below, but explicitly includes
coverage of behavioral health services categorically to special populations. The definitions
[page A8] that excludes MR and DD:
•
Mental Health Services – Means the diagnosis, evaluation, treatment, residential
personal care, habilitation, rehabilitation, counseling or supervision of persons who have a
mental illness.
•
Mental Illness – Means a psychiatric disorder, alcohol dependence, or drug
dependence, but does not include mental retardation or other developmental disabilities.
The TennCare contract language that excludes MR/DD from the BHO states [§2.6.2.5] that
“Except as otherwise required in this CONTRACT, the Contractor shall not be responsible for
coverage of treatment services to any Participant when the need for treatment services is the
result of factors other than the Participant’s mental health or substance abuse treatment needs.”
The contract language that includes specific behavioral services for people with MR/DD states
[§2.6.2.4] “The Contractor shall insure it provides accessible and available services covered
under this CONTRACT for all Participants, including those belonging to special groups. These
special groups include, but are not limited to, individuals with physical disabilities such as
hearing loss or vision impairment [§2.6.2.4.1]; and dual diagnosed individuals (those with
diagnoses of mental illness as well as diagnoses of mental retardation or substance abuse)
[§2.6.2.4.2].”
Diagnoses excluded in the BHO contract remain the responsibility of the TennCare Bureau.
Behavioral health contribution to the treatment of patients with non-covered diagnoses is
typically in the context of acute stabilization of behavioral decompensation requiring inpatient
psychiatric hospitalization, and consultation-liaison services, either inpatient or outpatient. Just
as a psychiatrist or other behavioral clinician might consult on a patient with any medical illness,
and could treat behavioral symptoms on a consulting basis, so could the BHO provide behavioral
services to people with MR/DD with regard to their behavioral symptoms. Overall treatment
accountability remains with the TennCare Bureau or with whatever Agency to which the Bureau
has delegated responsibility for providing EPSDT-mandated MR/DD services.
Likewise, a person with MR/DD could have a co-occurring behavioral disorder, whether it is a
psychiatric condition such as depression, or an addictive disorder such as alcoholism. These cooccurring conditions would be subject to BHO treatment regardless of the MR/DD diagnosis.
These service recipients would have access to the full continuum of behavioral health services
according to BHO medical necessity criteria. MR/DD status may require clinicians/treatment
programs with particular expertise, but otherwise access to services is no different for this
population relative to similar clinical presentation in people without MR/DD.
Autism Services Proposal
SJR 567
70
APPENDIX F
Early Intervention
Federal Legislation:
Congress recognized both the preexisting state diversity and the need to coordinate (early
childhood intervention) services across agencies when it crafted the legislation that
created the Early Intervention Program for Infants and Toddlers with Disabilities
(formerly known as Part H and now Part C of the Individuals with Disabilities Education
Act of 1990 [IDEA]).
The legislation required that states identify a lead agency to administer the program,
develop a definition for developmental delay, and decide whether they would include the
“at-risk of disability” category. To address the coordination of multiple agencies involved
in service delivery, states were required to create an Interagency Coordinating Council
(ICC) and provide service coordination to each family receiving early intervention
services. 1
The goal of building an interagency system is a central idea in the Part C legislation, and
the federal legislation provided states with funds to build coordinated, interagency
systems of early intervention services. However, there can be significant variation across
states in the systems they build.
Required components for all state systems under federal statute and regulations:
•
•
•
•
•
•
•
•
•
•
•
1
Maintaining a central directory of information
Implementing a public awareness program
Maintaining a comprehensive system of childfind
Providing for evaluation and assessment of children
Development of Individualized Family Service Plans (IFSP)
Contracting, or otherwise arranging, for services
Maintaining a comprehensive system of personnel development
Maintaining provisions for implementation of procedural safeguards
Supervision and monitoring of programs and safeguards
Collecting and maintaining data on the system
Maintaining an Interagency Coordination council (ICC)
by Donna Spiker, Kathleen Hebbeler, Mary Wagner, Renee Cameto, Patti McKenna
( 2000) Topics in Early Childhood Special Education, Pages 1-22.
Autism Services Proposal
SJR 567
71
Tennessee’s Early Intervention System: T.E.I.S.
In Tennessee, Public Law 105-17, Part C, is a segment of the larger law umbrella, IDEA
(Individuals with Disabilities Education Act). This section, Part C, entitles infants and
toddlers with disabilities rights to intervention. The law lists the processes and services
that Tennessee is required to follow and provide through early intervention services.
These processes are in place to protect the family as well as the child during the early
intervention period.
TEIS works with infants and toddlers from birth to three years of age. TEIS operates nine
district level “points of entry” and a statewide toll free number to assist families.
Once a referral is made, a service coordinator makes a home visit to conduct a screen or
evaluate the child and discuss the need for additional evaluations, if needed, to determine
eligibility. TEIS uses this first opportunity with the family to explain their rights under
IDEA.
When eligibility is established, an Individual Family Service Plan (IFSP) must be written
prior to any service provision. A team of professionals and the parents convene to write a
plan for the child and family based on educational and medical needs of the child. This
plan will also include the parents’ concerns and priorities.
The service coordinator is the family’s liaison to services. This person will coordinate
with providers and professionals that are critical to the child’s development, thus creating
the family’s team. It is through this team’s effort that a plan of service is developed,
coordinated, and implemented.
When a child turns three, intervention services are provided by the local education
agency (LEA). Prior to the third year, the IFSP should be adapted to plan for the
transition from TEIS to the LEA. This transition process should address the future issues
and needs of the child and to allow for a smooth transition from one program to the next.
TEIS Services:
•
•
•
•
•
•
•
•
•
•
•
•
Screening, evaluation, and assessment
Service coordination
Family training and counseling and home visits
Special instruction (child)
Audiology
Speech pathology
Physical and occupational therapy
Vision services
Social work services
Transportation
Assistive technology
Medical services for diagnostic purposes only
Autism Services Proposal
SJR 567
•
•
Health services when necessary to allow child to benefit from other Early
Intervention Services
Implementation of procedural safeguards
Parents are afforded several rights under the law for protection. A partial list follows:
• The right to informed consent
• The right to written prior notice
• The right to a multidisciplinary evaluation and an assessment of the child
• The right to review records
• The right to mediation, and
• The right to services in a natural environment
72
Autism Services Proposal
SJR 567
73
APPENDIX G
State definition and eligibility criteria for Autism: Department of
Education: Special Education
1.
Definition (State Board of Education Rule 0520-1-9-.01)
a.
“Autism” means a developmental disability, which significantly affects verbal and
nonverbal communication and social interaction, generally evident before age three (3), that
adversely affects a child’s educational performance. Other characteristics often associated with
autism are engagement in repetitive activities and stereotyped movements, resistance to
environmental change or change in daily routines, and unusual responses to sensory experience.
The term does not apply if a child’s educational performance is adversely affected primarily because
the child has an emotional disturbance, as defined in this section.
b.
After age three (3), a child could be diagnosed as having autism if the child manifests
the above characteristics.
c.
The term of autism also includes students who have been diagnosed with an Autism
Spectrum Disorder such as Autism, Pervasive Developmental Disorder—Not Otherwise Specified
(PDD-NOS) or Asperger’s Syndrome when the child’s educational performance is adversely
affected. Additionally, it may also include a diagnosis of a Pervasive Developmental Disorder such
as Rett's or Childhood Disintegrative Disorder. Autism may exist concurrently with other areas of
disability.
2.
Eligibility Standards
a.
Children with autism demonstrate the following characteristics prior to age 3:
(1)
difficulty relating to others or interacting in a socially appropriate manner; and
(2)
absence, disorder, or delay in verbal and/or nonverbal communication; and
(3)
one or more of the following:
(a)
insistence on sameness as evidenced by restricted play patterns,
repetitive body movements, persistent or unusual preoccupations,
and/or resistance to change; and/or
(b)
b.
unusual or inconsistent responses to sensory stimuli.
The characteristics as defined above are present and cause an adverse effect on
educational performance in the classroom or learning environment.
3.
Evaluation Procedures
a.
Evaluation shall include the following:
Autism Services Proposal
SJR 567
74
(1) parental interviews including developmental history;
(2) behavioral observations in two or more settings (can be two settings within the
school);
(3) physical and neurological information from a licensed physician, pediatrician or
neurologist who can provide general health history to evaluate the possibility of
other impacting health conditions;
(4) evaluation of speech/language/communication skills, cognitive/developmental
skills, adaptive behavior skills and social skills; and
(5) documentation and assessment of how autism spectrum disorder adversely
affects educational performance in the classroom or learning environment.
4.
Evaluation Participants
a. Information shall be gathered from the following persons in the evaluation of autism
spectrum disorders:
(1) the parent(s) or guardian of the child;
(2) the child’s general education classroom teacher (with a child of less than school
age, an individual qualified to teach a child of his/her age),
(3) an appropriately licensed school psychologist, licensed psychologist, licensed
psychological examiner (under the direct supervision of a licensed psychologist),
or licensed psychiatrist;
(4) a licensed physician, neurologist, pediatrician or primary health care provider;
and
(5) a certified speech/language teacher or specialist; and other professional
personnel as needed, such as occupational therapist, physical therapist or guidance counselor.
Autism Services Proposal
SJR 567
75
APPENDIX H
Applied Behavioral Analysis Definition and Explanations from:
TRIAD
Howard County Maryland Parent Proposal
Reference Terms
Applied Behavior Analysis (ABA):
A general term that refers to a set of concepts, principles, and techniques used in the
assessment, treatment, and prevention of problem behaviors. It involves the following
components: direct measurement of behavior through systematic observation and
recording; functional analysis of the causes of behavior; an emphasis on understanding
and manipulating the antecedents of behaviors as well as the consequences; and the use
of specific techniques to increase desirable behaviors, decrease undesirable behaviors,
teach new skills, and promote generalization o f newly acquired skills across situations.
ABA is not equivalent to Lovaas. Nor is it equivalent to discrete trial training.
Discrete Trial Training (DTT):
A specific ABA technique that is used to primarily teach new skills. It occurs in a oneto-one context in a location that is free from distraction. Discrete trial training is adultcentered, in that the adult determines the time, location, and content of the teaching
activities. This approach involves breaking down the behavioral sequences into separate
components and teaching one component at a time in a highly structured manner. The
discrete trial consists of three main steps, SD-R-SR. The Discriminative Stimulus or
SD is the instruction given by the adult, which triggers the Response or R from the
student. And in turn, the adult provides positive or negative feedback, Stimulus
Reinforcer or SR. Depending on whether the feedback was positive or negative, the
student’s response will either increase or decrease respectively in the future. Each
teaching episode usually involves the repetition of many discrete training trials.
Taken from “TRIAD ABA Workshop Series Manual”
TRIAD, 2002
Autism Services Proposal
SJR 567
76
Howard County Maryland Parent Proposal
Brief Description of Applied Behavioral Analysis (ABA) Programs2
Behaviorally-Based Intervention
The most important change we feel needs to be made to HCPSS’s program for children
with autism is the use of and rigorous training in ABA techniques. There is much
evidence in favor of state-of-the-art implementations of Applied Behavior Analysis.
These programs use various behaviorally-based methodologies including discrete trial
therapy as a major part of an integrated program that first teaches children how to learn,
continues by teaching them how to generalize their learning, and finally teaches them
how to be part of society.
Any behaviorally-based, intensive intervention program requires a high level of training
for all staff working directly with the children, be it in the classroom setting or in one-onone situations. Without a specific focus on training in techniques of ABA – a focus
which currently does not exist within the county - professional staff and temporary aides
will be unable to implement the program necessary to educate young children with
autism.
This appendix has two parts: first, we give an overview of Discrete Trial-Based Applied
Behavior Analysis programs. Second, we give specific curriculum information, showing
how skills are taught in a progression of phases, and how generalization and peer
interaction are phased in after the children can best use these learning opportunities.
Discrete Trial-Based Programs
Discrete trial therapy (DTT) is a specific teaching technique used to maximize learning.
The technique consists of breaking down a skill into smaller parts, and then teaching one
sub-skill at a time. Each teaching session involves numerous trials, with each trial having
a distinct beginning (i.e., the instruction) and end (i.e., feedback). Each part of the skill is
mastered before more information is presented. DTT is contrasted with “continuous
trial” or more traditional methods of teaching which present large amounts of information
before the child’s response is sought.
In DT-based programs, children are presented with opportunities to learn necessary skills
until they are performed successfully. Children are reinforced (rewarded/praised) for
doing so, which provides motivation for the child to continue to learn. Therapists and
paraprofessionals working with the children are trained to ignore negative behavior but to
reinforce compliance and good behavior – “praise the best, ignore the rest”. Reinforcers
include for example, candy, affection, free play, and are selected on the basis of what the
child responds to best. The child’s success is closely monitored by data collection at
various degrees of detail.
Skills that the child has mastered {i.e., he/she is successfully performing with some stated
frequency, (e.g., 80% or better)} are tested subsequently to ensure that the child continues
2
Early Intervention for Young Children with Autism Part II: A Parent Proposal; A Report to the Board of
Education by the Howard County Chapter of the Autism Society of America 1998.
Autism Services Proposal
SJR 567
77
to be proficient in them. New tasks are constantly introduced to expand upon the skills
already mastered. Once a student has mastered a particular skill, steps towards
generalization begin immediately and are adapted to the specific needs of the child.
The use of discrete trials is common to behaviorally-based methods in a variety of
contexts. DT-based programs are often referred to as Applied Behavior Analysis (ABA)
programs, although the term refers more generally to behavioral methods in a variety of
circumstances. The term ABA is used here, however, to refer to a method of teaching
designed to analyze and change behavior in a precisely measurable and accountable
manner. In particular, the methodology can also be used in more natural circumstances
as part of incidental learning. However, by themselves methods that rely solely on
incidental learning (described as behavioral methods in naturally occurring situations,
routines-based learning, and other milieu teaching techniques) will not necessarily
provide sufficient learning opportunities for children with autism. Children often will not
comply with a teaching activity (this is also the difficulty faced in educating children with
autism within traditional special education programs). The Discrete Trial Therapy
component of ABA programs is designed to ensure that children learn the tasks of the
recommended curriculum. This is accomplished by persisting with teaching the tasks
until they are mastered. Trained “therapists” learn a variety of techniques to deal with
non-compliance and to get children back on task.
In order to implement the discrete trial component and to generalize skills learned to
other situations, an ABA program requires a large number of service hours. Full day
programs are indicated, often with hours added at home. As the children progress, their
education continues to require similar levels of service, but in the more natural
environment of the classroom.
Approach to Teaching
The elements of the ABA programs we wish to implement are drawn from intervention
techniques that have been described in Part I. They are:
•
•
•
•
•
•
The use of Discrete Trial Therapy
The use of a developmentally appropriate curriculum
Generalization by teaching in progressively less structured settings.
Use of functional assessments for challenging behaviors.
Use of natural situations as teaching opportunities.
Inclusive education.
Depending on the needs and age of the child the program can require a range of
placements, from a program in which one-on-one intervention predominates to one which
stresses group instruction in the regular classroom. A major one-on-one, structured
component is indicated for children who do not interact with other children well enough
to benefit form a group setting. In center-based programs, the children are included, first
in smaller then in larger groups, as their ability to interact and cope increases. The best
practices thus indicate a ‘phased approach’ in which the degree of intensive one-on-one
intervention is highest in the early stages, and more time is spent in inclusive settings
later. Tasks to be learned are also introduced in phases and developmental levels, as
explained in the curriculum section below.
Autism Services Proposal
SJR 567
78
ABA programs can be highly tailored to the individual needs of the child. They allow for
a continuum of placements depending on those needs, and are tuned to the child’s
learning pace. The usual necessity of performing at least some of the therapy at home—
so that the skills learned in the program can be generalized to what is the most important
setting the child must cope with—implies a great deal of parent involvement and
awareness. For these reasons, these programs contain many if not all of the strategies
found to be most successful in treating children with autism.
Curriculum for ABA Programs
Specific goals and objectives are established along a continuum of developmental
milestones that begin with non-verbal imitation and continue to advanced conversation,
peer socialization, and academic skills such as reading and math. An example of how an
ABA program might proceed in its early stages is given in the flowchart on the next page.
The developmental milestones or goals that make up a modern ABA program are those
that typical children pick up effortlessly from their environment. We stress again that the
autistic child must learn how to learn, beginning with very small and basic tasks,
followed by increasingly complex tasks. In the context of the school system, IEP goals
must be precisely specified and be measurable. Goals are typically written to cover the
following areas (in alphabetical order):
•
•
•
•
•
•
•
•
•
•
•
•
•
asking questions
assertiveness
attributes
block imitation
categorization
cause and effect
communication
temptations
conversation skills
(basic, intermediate,
advanced)
describing
drawing
emotions
expressive labeling
functional
communication
• general knowledge and
reasoning
• “I don’t know”
• independent work and
play
• joint attention
• matching
• motor skills
• negation
• nonverbal imitation
• observational learning
• peer interaction
• play, play scripts
• prepositions
• pronouns
• quantitative concepts
• reading
• recall
• receptive instructions
• receptive label requests
• same versus different
• self-help skills
• sequencing
• social awareness
• socialization skills
• songs
• stories
• verbal imitation
• “What’s missing”
• “yes/no”
Children using a discrete trial-based curriculum work through the “phases” of the
curriculum at their own speed, entirely dependent on their skill acquisition rate. In
addition, students may work on different phases simultaneously, especially if they have
“splinter skills.34”
3
Splinter skills are those that children have that may be advance of a child’s developmental age. The
uneven pattern of development common to children with autism often produces such anomalies: thus a
child may be unable to speak a complete sentence but able to add and subtract or read significantly above
age level.
Autism Services Proposal
SJR 567
79
APPENDIX I
Estimated Costs for the Proposed Autism Spectrum Disorder Model
Centers of Excellence ASD units
Statewide Budget
Personnel
Executive Directors
Developmental Pediatricians
Child Psychiatrists
Psychologists
Behavior Analysts
Speech & Language Therapists
Occupational Therapists
Physical Therapists
Family Resource Specialists
Liaison Staff
Composite Budget for Five Centers
FTE
1.0
2.0
2.0
2.5
4.0
4.0
4.0
2.0
3.5
50.0
Total Personnel Budget
Salary
Fringe
Total
120,000 30,000
150,000
270,000 67,500
337,500
270,000 67,500
337,500
200,000 50,000
250,000
180,000 45,000
225,000
180,000 45,000
225,000
180,000 45,000
225,000
90,000 22,500
112,500
122,500 30,625
153,125
1,500,000 375,000 1,875,000
3,112,500 778,125 3,890,625
Non-Personnel
Travel
Supplies
Telephone
Testing Materials
Computer expenses
Training expenses
5,000
8,000
20,000
15,000
150,000
40,000
Total Non-Personnel Budget
238,000
Total Centers of Excellence Budget
Department of Education Autism Teams
Personnel
Special Educators
Speech & Language Therapists
Behavior Interventionists
Total Personnel Budget
Non-Personnel
Travel
4,128,625
Composite Budget for Eight Teams
FTE
8.0
8.0
8.0
Salary
Fringe
360,000
90,000
360,000
90,000
360,000
90,000
1,080,000
Total
450,000
450,000
450,000
270,000 1,350,000
30,000
Autism Services Proposal
SJR 567
80
Supplies
Telephone
Testing Materials
Computer expenses
Training expenses
12,000
32,000
24,000
25,000
150,000
Total Non-Personnel Budget
273,000
Total Budget for DOE Autism
Teams
1,623,000
TN Center for Autism
Personnel
Executive Director
Research Coordinator
Training Coordinator
Dissemination Coordinator
Tech Support
Office Staff
Training Staff
Research Staff
Total Personnel Budget
FTE
0.25
0.3
1.0
0.5
1.0
2.0
6.0
2.0
Salary
Fringe
32,500
8125
25,000
6,250
50,000
12,500
20,000
5,000
25,000
6,250
40,000
10,000
228,000
57,000
85,000
21,250
Total
40,625
31,250
62,500
25,000
31,250
50,000
285,000
106,250
505,500
631,875
Non-Personnel
Travel
Supplies
Telephone
Testing Materials
Computer expenses
Training expenses
126,375
30,000
12,000
10,000
4,000
12,000
120,000
Total Non-Personnel Budget
188,000
Total Budget for State Center
819,875
GRAND TOTAL
6,571,500