electrical stimulation - Advanced Therapy Institute
advertisement

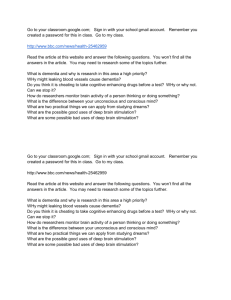
ELECTRICAL STIMULATION Electrical stimulation of human tissues is an old procedure dating from the attempts of the early Greeks to use electric eels for therapeutic purposes. The modern rediscovery of electricity and its uses in physical medicine dates from the early eighteenth century, when again, electrical stimulation generated by electric eels was applied therapeutically to relieve headaches and to affect neuromuscular paralysis. Therapeutically applied electrical stimulation has had a checkered history, enjoying long periods of popularity and respectable use interspersed with periods of widespread misuse by medical charlatans who treated everything from psychiatric conditions to cancerous tumors. One must suppose that the simplicity of electricity producing equipment (especially that utilizing static or direct current) coupled with the seemingly magical effects that electrical currents have on human tissues, unavoidably led to its exploitation by unscrupulous "practitioners" at the expense of the unsophisticated and gullible. Often billed as a near panacea for the cure of most human physical ills, over time the therapeutic use of electrical stimulation, in the minds of many, gradually became associated with quackery and therefore considered beneath the use of scrupulous and sophisticated practitioners. This state of affairs was (and is) unfortunate, since there are many physical ills that humans are afflicted with that may be improved or corrected by appropriately applied electrical stimulation. Electrical Stimulation Related Terms current of less than 1.5 milliamperes (mA) and relatively high peak currents of between 60 and 100 mA. (Amps = coulomb/second). Bipolar Electrode Placement: both cathode (negative) and anode (positive) electrodes are placed on the treatment area in relative proximity to each other. This arrangement provides for rather specific stimulation of structures with few variations in responses. Burst frequency: the number of trains of impulses produced per second; it is dependent on the “stimulation on and stimulation off” duty cycle selected. Coulomb: a basic unit of charge theoretically produced by 6.28 x 1018 electrons. Most therapeutic electrical stimulators have a low pulse charge, expressed in micro‐coulombs (10‐6 coulombs). Current density: the amount of current per unit area; i.e., the smaller the electrode, the greater the current density, making the stimulus perceptually stronger to the recipient. Monopolar electrode placement: one electrode is placed on the treatment area and the other is placed on a remote location on the body. This arrangement provides a rather general stimulation pattern because of the multiple parallel pathways the current that may be taken from one electrode to the other. One may also expect variations in the responses produced by the electrical stimulation applied this way because of the number of nerves and other structures the current may pass through. Modern instrumentation used to apply electricity to the body is designed for users who are without detailed knowledge of the instrument's internal circuitry or the physics responsible for the production of electricity. However, some knowledge of the basic principles that govern electrical stimulation is useful for an understanding of the variable results that come from the necessary “trial and error” that is a regular feature of its therapeutic use. A few terms are defined below to help those of us who have little or no education in this area. Ohm: a unit expressing the amount of resistance offered by a current conductor (the recipient’s soft tissues). Ohm's Law: “The current (amps) is directly proportional to potential (volts) and inversely proportional to resistance (ohms). Current = potential/resistance.” Amps (amperes) = volts/ohms. Ampere: the unit of flowing charge (current). Most therapeutic electrical stimulators have a low average 57 Pulse duration: the amount of time the current flows in one direction. Pulse duration is measured when the current level is at 50% of its peak, usually expressed in microseconds. dispersive), thus completing an electrical circuit with the recipient’s body. Electrical currents passed through muscle or nervous tissue from an external source (electrical stimulator) will be partially depolarized in the region of the negative and hyperpolarized in the region of the positive. If the current is sufficiently strong, the degree of depolarization will reach or exceed the critical level necessary to produce a muscle contraction or the firing of the nerve. At the anode, as the circuit is completed. The body overcompensates for electrical changes induced by the current, so that some degree of irritability is present at the anode. If sufficiently great, the irritability will also cause a muscle contraction or nerve firing under the anode. The current level required to produce a single neuron impulse or single muscle fiber contraction is called a minimal stimulus. If a stronger stimulus is required to excite all of a group of nerve fibers or denervated muscle fibers, it is called a maximal stimulus. A stimulus higher than that is called a supramaximal stimulus. The factors that determine the adequacy of a stimulus to either elicit a muscle contraction or provoke the firing of nervous tissue include pulse frequency, pulse duration, and the amplitude of the current. The minimal duration of an effective electrical stimulus (sufficient to provoke a muscle contraction or nerve firing) is 1.0 microsecond for a normal innervated muscle fiber and 0.03 microseconds for a normal nerve fiber. The strength of an electrically induced muscle contraction is related to the intensity and pulse duration of the stimulus: the greater the intensity and pulse duration, the greater the strength of contraction. Equipment Utilized in Electrical Stimulation Electrical units currently used for the stimulation of muscle or other deep tissues can be generally classified into six categories: Pulse frequency: the number of pulses produced per second, hertz (Hz) or cycles per second (c/s). Resistance to current: The body is made up of tissues and fluids that vary in their electrical conductivity and, conversely, their resistance to the passage of electricity. Tissue conductivity is proportionally related to the tissue's water content; the higher the water content the greater the conductivity and the lower the tissue's resistance. The water content of muscle is 72 to 75%, the brain is 68%, fat is 14 to 15%, and of the peripheral nerve, skin, and bone is five to 16%. Resistance varies in direct proportion to the distance between electrodes. The resistance increases, as the distance the electrical stimulus must travel increases. Volt: A volt is a unit of measure that indicates the amount of potential energy (Joule) each unit of charge (coulomb) contains (Voltage = Joule/coulomb). Electrotherapeutic currents are generally derived from the commercial lighting circuit (alternating current in the United States or direct current in some other parts of the world) or from the direct current (d/c) provided by batteries. Transformers, electromagnetic or thermionic devices, or complex circuitry (beyond our scope here) modify these basic currents to produce various therapeutic current forms. The therapeutic current forms include galvanic (square wave), interrupted galvanic, surged interrupted galvanic, sinusoidal, alternating, surged alternating, faradic, surged faradic and other hybrid waveforms (generally produced by combining two or more waveforms). The variables manipulated to produce the various waveforms include: voltage, amperage, mode flow (direction), pulse frequency, and pulse duration (pulse width). High Frequency (Medium Frequency) Stimulators: These units, by definition, generate more than 1000 c/s, with popular models producing 2500 c/s. The 2500 c/s units usually employ a duty cycle of 10 milliseconds (msec) on and 10 msec off. In this case, the 2500 c/s is interrupted at 1/100 of a second on and 1/100 of a second off with a 50% duty cycle producing 50 bursts per second with 25 cycles per burst. The 2500 c/s unit generally has a peak current of 130 mA with an average current level of from 80 to 100 mA root mean square (RMS). These units Applying Electrical Stimulation to Soft Tissues: Electrical stimulation is applied through a pair of electrodes placed on the body. The electricity is passed from the cathode (negative) pole electrode, over and through the soft tissues, to the anode (positive) pole electrode (sometimes called the 58 provide a variety of duty cycles, ramps, and peak currents from which to choose. They can create a muscle contraction that is 60% (or greater) of that produced by a maximal isometric contraction. An electrical stimulator with variable current forms High Voltage Stimulators: These units have a high peak current of 500 mA or greater with a low average current of less than one mA. They are constant voltage generators with a pulse charge of approximately four micro coulombs, and their pulse durations usually range from five to eight microseconds. They generally provide a variety of duty cycles and pulse‐frequencies from which to choose. Low Voltage Electrical Stimulators: These units have low peak currents, low voltage driving forces that can be alternate or direct currents, and their pulse duration’s are usually large, measured in msec or seconds. If using a direct current, they can produce thermal and chemical effects and can be used to produce iontophoresis. Portable Neuromuscular Stimulators: These units generally employ a constant current, which generally has a peak of 100 mA with a driving force of from 50 to 100 volts. They generally provide a choice of duty cycles, pulse frequencies, peak currents, and ramps (the time it takes for the current level to rise from zero to its peak). Interferential Stimulators: These units are constant current generators that create a pulse frequency of 4000 to 5000 c/s. The interferential units generally employ two electrical sine wave circuits, one of which has a fixed frequency while the other varies its frequency; when the two waveforms intersect, an interferential frequency is said to result. The interferential unit usually has a peak current of 60 mA. Electrodes: The electrical energy from electrical stimulators is conveyed to the recipient by conducting cables. The cables are plastic or rubber 59 insulated flexible copper or silver wires. The thickness of the cable depends on the amount of current to be carried by the conductor (the greater the current, the thicker the cable needs to be). These cables may be a uniform color or color‐coded according to function. If color‐coded, the wire to the negative (cathode) electrode is conventionally black, and that to the positive (anode) electrode is red. An electrode is a medium that intervenes between the cable from the electrical stimulator and the recipient's body (only surface electrodes will be discussed here). It generally consists of a good conducting material whose shape and form can be adapted to conform to contours of the body. Electrode mediums include water, metal foil (usually made from an alloy of lead, tin, and zinc), moist‐ pads, or flexible carbon or “silicone” pads. Flexible electrode pads Electrode pads are usually employed in pairs, often of equal size. Between two electrode pads of equal size, the current density beneath each of them is equal. If one is twice as large as the other is, the current density under the smaller one will be twice as great as that under the larger. As the current spreads between two electrode pads, across the body, its density must gradually decrease so that midway between them the density is the least. The closer the electrodes are to one another, the greater the density of the current that passes between them. The higher the current density, the greater the effect on the tissues stimulated. The electric current carried along the cable length eventually leads to some crystallization and to breaks in the conducting wires at the sites where the most bending or movement of the cable occurs, usually close to the electrode connections at both ends. Application: If low frequency sponge pad electrodes are being used, they must be well moistened with a saline solution (or water) and placed over the chosen treatment sites. If carbon or “silicone” pads are used, take care that the skin between the electrodes remains dry to avoid an “electrode bridge” that would decrease or preclude effective electrical stimulation (the electricity would pass through the water to complete the circuit, having no effect on the body). 60 Generally, place a negative electrode on the muscle's motor point (where the motor nerve is most superficial as it innervates the muscle) so that when stimulated the greatest muscle contraction is provoked. Once the best sites for electrode placement have been determined, elastic strapping, weighting, or taping may be applied to ensure good continued electrode contact. Set a watch or timer for the length of treatment. Turn the electrical stimulator on and increase the amplitude (intensity) until a visible contraction takes place, always staying within the recipient’s range of tolerance. Allow the recipient to become accustomed to the current before additional intensity increases are slowly made. Continue this process until the desired degree of contraction is reached. Closely monitor the recipient for excessive muscle spasm, cramping, joint compression, or pain. Never leave the recipient out of hearing range once the treatment has been started. the injury, the burn site appears rather small and inconsequential but becomes more alarming as the damaged tissues are subsequently sloughed off and ulceration occurs. Electrical burns are slow to heal, prone to infection, and (if sufficiently deep) may be followed by extensive unsightly scarring. Electric shock may be caused if the recipient touches a grounded object (a water pipe, radiator, or electric circuit) while being stimulated. This is especially serious if a large area is subjected to the shock. Electric shock may also occur if the electrical stimulator suffers transformer breakdown (which is unlikely with modern units). If this happens the high‐tension, low frequency current may jump to the recipient and produce an electrical burn as well as a shock. Take care to avoid over‐fatigue of the muscles stimulated. Stimulation should stop when the muscle begins to respond with less vigor. Generally, do not place electrodes over scar tissue, skin irritations or open skin lesions (unless used to help fight infection). If increased sweating, salivation or signs of nausea occur discontinue stimulation. Do not let electrical current flow across a pregnant uterus or a cardiac pacemaker. When applying electrodes, take care to avoid overlapping negative and positive electrodes, and avoid having conductive materials (electrode cream, water or gel) form a conductive “electrode” bridge between the two. Either situation will cause a completion of the circuit without involving or affecting the recipient’s tissues. When applying electrical stimulation, a gradual increase of intensity is preferred because of the tendency of natural skin resistance to suddenly break down after being exposed to an electric current for several minutes. If the apparent lack of tissue response persuades the practitioner to increase the intensity to a relatively high level before skin resistance breaks down, the recipient may pay for the practitioner's lack of patience by experiencing additional pain or discomfort. Future treatment may be put in jeopardy because of the recipient’s acquired fear. At the end of the session (if not automatically shut off) gradually decrease the intensity until it is switched off. Return all controls to zero. Remove all electrodes from the recipient. Have the recipient rest for several minutes before being allowed to exercise. Precautions: Electrical burns may occur if continuous uninterrupted galvanic current is used and an excess of current density applied to the skin or mucous membrane. If an electrical burn results, the tissue damage produced occurs in a roughly conical area, extending from the apex on the skin's surface (where the original electrical contact occurred) and fanning out into the deeper layers. Just following 61 CCIIRRCCUULLAATTIIOON NEEN NH HAAN NCCEEM MEEN NTT It has long been accepted that electrical stimulation of muscle tissue to provoke muscle contractions to rhythmically squeeze associated blood vessels may be used to therapeutically improve circulation. This process induces the muscles to artificially provide the pumping action required by nature to facilitate venous blood flow and to add impetus to lymphatic circulation. Less known or appreciated is the effect that electrical stimulation may have on capillary development. Research undertaken in the late 1970's demonstrated that continuous low frequency electrical stimulation could increase capillary to muscle fiber ratio and thus the number of capillaries present in a cross‐sectional area. The formation of new capillaries may be accompanied by an increase in the total capillary surface area and the “sprouting” of large capillaries (making new branches). Increases in capillary density (20% after 4 days of stimulation, 50% after 14, and 100% after 28 days) are apparently not a consequence of the action of the electrical current itself. They result from the muscular need for additional blood supply to support the demand of electrically induced muscular contractions. Similar changes accompany hypoxia in humans and animals (non‐primates) when engaging in aerobic exercise (repetitive isotonic contractions, like running). It should be noted that high frequency electrical stimulation (30 Hz and above) and isometric exercise have both failed to demonstrate the ability to increase capillary density. Electrode placement for electrical stimulation of the calf Because of the ability to increase capillary density, low frequency electrical stimulation may be used to good effect when treating conditions stemming from impaired or decreased blood circulation. 62 Application: To increase capillary density, the electrodes may be placed in bipolar fashion over a large muscle or muscle group in the involved extremity or associated with the involved area. Preset the electrical stimulator to deliver a pulsed square wave or faradic current flow at a pulse frequency of between four and 14 Hz (7 to 10 Hz would be ideal), for a 20‐ minute period. Turn the stimulator on, and slowly increase the intensity until a visible contraction of the muscle or muscle group develops. As the patient gets used to the sensation of electrical stimulation, gradually increase the current until the contractions are quite brisk. Daily treatments provide the best results. 63 EEDDEEM MAARREEDDUUCCTTIIOON N It has long been accepted that electrical stimulation of muscle tissue to provoke muscle contractions to rhythmically squeeze associated blood vessels may be used to therapeutically improve circulation. This induces the muscles to artificially provide the pumping action required by nature to facilitate venous blood flow and to add impetus to lymphatic circulation. Consequently, electrical stimulation may be used to good effect when the patient has lost the ability or is unable to voluntarily contract the necessary muscles (as when splinted or when closely confined for therapeutic reasons). This provides a way of reducing lymph edema that is often a consequence of syndromes in which the muscles are kept from contracting or "working out". Apart from the mechanical pumping action that electrically induced muscle contractions can provide, pulsed direct (galvanic) current has the observable and apparent ability to carry or drive fluid out of edematous tissue, possibly because of electrical ionic transfer. To facilitate lymph circulation or decrease edema, in the most effective manner, place the largest possible electrodes over the largest possible areas. For example, place the patient’s swollen ankle in a basin of water (the water above the level of the malleoli) with the positive electrode. Place the negative electrode on the low back. This set‐up will affect the greatest number of muscles possible and may additionally facilitate the flow of the edematous fluid out of the swollen extremity. To treat a single swollen joint, place a wet cloth (wet wrap) over and around the swollen joint, and the positive electrode over the area most swollen. If a dual positive is available, place each positive electrode on either side of the joint; place the negative electrode in an area distant from the swollen joint (in the midback area, for example). Application: Preset the electrical stimulator to deliver a pulsed square wave current flow at a pulse frequency of 28 Hz for a 20‐minute period. Turn the stimulator on and slowly increase the intensity until the patient’s muscles just begin to involuntarily tighten. Ideally, daily treatment is best but suitable outcomes have resulted from treatments every other day, or even two to three times a week. Electrical stimulation for the reduction of edema is remarkable for its ability to immediately reduce the swelling associated with strained, sprained, or immobilized joints. Consequently, when appropriate, following electrical stimulation the involved joint should be taped or fitted with a pressure‐splint (usually an inflated sleeve) to prevent swelling from redeveloping and to help stabilize the involved joint, thus preventing further joint trauma. 64 M MUUSSCCLLEETTOON NIIN NGG Research has confirmed that electrical stimulation, if appropriately applied, may be used to effectively increase tone, strengthen muscle, improve endurance, and increase the size of innervated muscle. Electrical stimulation has not been shown to be superior to traditional forms of voluntary exercise, for building tone and strength. Nevertheless, several studies have shown electrical stimulation to be nearly as effective. In fact, some research has demonstrated that high voltage pulsed electrical stimulation of at least 30 Hz may be used to cause involuntary isometric muscular (tetanic) contraction against resistance without causing the stress to the cardiovascular system. Both isometric and isotonic exercise cause increases in heart rate and blood pressures as a normal consequence of voluntary exertion. Review of the literature suggests that more study is needed to establish which types of electrical stimulation are most effective for increasing muscle tone and strength and which methods of application are most efficient. In addition, more study is necessary to establish which types of muscle fibers (fast or slow twitch) will respond best to electrical stimulation. Muscle toning with electrical stimulation seems to be most effectively accomplished by electrical stimulation units capable of producing currents strong enough to produce tetany (or near tetany) while being fairly comfortable for the patient. Such stimulation units generally provide a duty cycle of 10 to 15‐seconds on and 10 to 50‐seconds off. Such stimulation is usually best provided by a high voltage, high frequency (medium frequency) unit. Application: the muscle or muscle group on stretch and fixing the involved joint in place to prohibit them from moving in response to provoked contractions (i.e., an isometric contraction). Place the electrodes over the muscle or muscle group to be stimulated in a bipolar fashion. Place the cathode (negative) electrode over the dominant muscle's motor point, and the anode (positive) electrode elsewhere on the same muscle or muscle group. Turn the electrical stimulator on and slowly increase the intensity until a visible contraction develops. As the patient gets used to the stimulation (shows signs of relaxing), gradually increase the current until tetany or near tetany occurs. Continue stimulation for 10 to 15 minutes. Use a duty cycle of 10‐seconds on and 10‐ seconds off to produce maximum toning, if that option is available. Treatment may occur daily, but suitable results have come from treatments every other day or twice a week. Muscle toning with electrical stimulation has been shown to be remarkably effective for retrieving muscle tone lost as a secondary effect of long term inflammatory conditions (chronic tennis elbow or debilitating knee or ankle ailments) or disuse from prolonged bed rest. If the electrical stimulation is applied correctly and appropriately, muscle strength can be improved without any risk of reinflaming the previously involved soft tissues through strain, which is often a consequence of voluntary exercise. To tone muscle with electrical stimulation, the best results seem to come from putting 65 M MUUSSCCLLEELLEEN NGGTTH HEEN NIIN NGG Chronically “tight” muscles, muscles spasm, and trigger points may be treated by relengthening the muscles involved through the judicious use of electrical stimulation. Application: Put the involved muscle(s) on stretch and (if possible) place both the negative and positive electrode pads over either the muscle involved or its most active antagonist. If medium frequency is used, place the pads over the involved muscle. If wide‐pulsed electrical stimulation at 7 Hz is used, place the pads over the antagonist(s) of the involved muscle. Preset the electrical stimulation machine to deliver either the medium frequency current, in a duty cycle of 10‐seconds on 10‐ seconds off, or a wide‐pulse frequency of five to 7 Hz. Turn the electrical stimulation on and set it (if possible) to turn off after 10‐minutes of stimulation. Slowly turn the electrical amplitude up until the desired level of muscle contraction is produced; a firm maintained contraction if medium frequency is used or a brisk, brief visible contraction if wide‐pulse stimulation is used. Turn the machine off after 10 minutes of stimulation. If the medium frequency current was used, encourage the patient not to move and to maintain the “stretched‐out” position for five minutes. If the wide‐pulsed current was used, vibrate the “tight” muscle’s antagonist(s) for one minute (each site), and then have the patient maintain the “stretch‐out” position for five minutes. Remove the pads and any remaining electrode cream or gel from the patient’s skin. 66 A variation of the above technique may be used to enhance the effects of both cervical and lumbar traction, by itself or in combination with vibration (refer to Vertebral Traction, Electrical Stimulation Enhancement, and Electrical Stimulation and Vibration Enhancement in Combination). TTIISSSSUUEEAAN NDDBBOON NEERREEPPAAIIRR Clinical research and experience have confirmed that low intensity, low frequency, electrical stimulation may facilitate the healing processes of damaged soft and bony tissues, increasing the quality and rate of repair. Electrical stimulation has been shown to be remarkably effective for precipitating the healing of long‐term nonunion fractures and the closure of healing‐resistant incisions and pressure sores (decubiti). Not only has electrical stimulation been shown to facilitate tissue growth, but also research has shown monophasic (one direction) electrical stimulation to have a bacteriostatic or antibiotic effect on some types of bacteria commonly associated with dermal lesions, including pseudomonas aeruginosus (in vivo). Many types of electrical instrumentation provide current forms with the requisite amplitudes (0 to 100 mA or up to 90 volts), frequencies (1 to 10 Hz), and pulse width duration (100 to 200 msec) necessary to inhibit bacterial infection and facilitate soft tissue or bone healing. Of all the current forms, the pulsed square wave has been shown to be the most effective and safest. 67 BBAACCTTEERRIIAALLIIN NFFEECCTTIIOON N To utilize electrical stimulation to help fight bacterial infection the following steps should be taken: Higher currents are not thought to be advisable, so don’t allow any involuntary muscle contraction or increased in muscle tonus to occur. If necessary, undress the dermal lesion and cleanse it of any exudates or loose debris, following sanitary debridement guidelines. Place a sterilized sponge electrode, moistened with pure saline solution, over the dermal lesion. Attach this electrode to the electrical stimulation device as the negative electrode. Place the positive or dispersive electrode some distance away from the lesion. Preset the electrical stimulator unit at zero amplitude, at a minimum frequency of 28 Hz, and at the longest pulse width possible (from 100 to 200 msec). Turn the electrical stimulator on and slowly increase the intensity until the patient reports feeling the stimulation, which usually occurs at 20 mA or slightly less. 68 Stimulate for from 20 to 60 minutes. Ideally, apply this treatment three or four times a day, at equally spaced intervals. Successful treatment has been noted to occur if stimulation is provided only once a day, or even as little as three times a week. However, the speed of healing seems directly related to the number and frequency of treatment sessions. Following treatment, remove the electrodes. If necessary, redress the dermal lesion according to hygienic guidelines. Sanitize the electrodes according to institutional hygienic guidelines (i.e., soaked in a bactericide solution or sterilized) before reuse. OOSSTTEEOOGGEEN NEESSIISS patient shows signs of being aware of the stimulation, usually occurring at the 20 mA level or slightly less. Higher currents are not thought to be advisable, so allow no involuntary muscle contraction or increased muscle tonus to occur. To promote osteogenesis with electrical stimulation, go through the following steps: Place surface electrodes above and below the fracture site, so that the current flow is parallel with the long axis of the bone. If the electrical stimulation unit is monophasic, place the negative electrode(s) as close to the fracture site as is possible, even over the site (since osteogenesis is promoted right under it). Preset the electrical stimulation unit at zero amplitude, at a minimum frequency of 28 Hz, and at the longest pulse width possible (from 100 to 200 msec). Turn the electrical stimulation unit on and slowly increase the intensity until the 69 Stimulate for 20 to 60 minutes. Ideally, apply this treatment three or four times a day, at equally spaced intervals. However, successful treatment has been noted to occur if stimulation is provided only once a day. Following treatment, remove the surface electrodes and thoroughly cleanse the skin under the electrodes. W WOOUUN NDDH HEEAALLIIN NGG To promote wound healing (without the presence of infection) with electrical stimulation go through the following steps: Place surface electrodes in opposition on either side of the open wound. If four electrodes are available, arrange the electrodes a crisscross pattern (negative‐ positive, positive‐negative) to allow the current flow to intersect over the surface of the wound. Preset the electrical stimulation unit at zero amplitude, at a minimum frequency of 28 Hz, and at the longest possible pulse width (from 100 to 200 msec). Turn the electrical stimulation unit on and the slowly increase the intensity until the patient reports feeling the stimulation, usually at 20 mA or slightly less. Higher currents are not thought to be advisable, so do not allow an involuntary muscle contraction or increased muscle tonus to occur. Stimulate for 30 to 60 minutes. Ideally, apply this treatment three or four times a day, at equally spaced intervals. Successful treatment has been noted to occur if stimulation is provided once a day, or as little as three times a week. However, the speed of healing seems directly related to the number and frequency of treatment sessions. Following treatment, remove the surface electrodes and cleanse the skin formerly under the electrodes. Precautions: As mentioned above, the selection of the electrode site and electrode polarity may be critical to the healing process it facilitates. Osteogenesis is facilitated by the presence of the negative electrode and inhibited by the presence of the positive electrode. Additionally, research has demonstrated that if the electrodes are placed in opposition to one another across the fracture site, perpendicular to the long axis of the bone, it will cause osteogenesis to occur in a manner that creates bone cells at right angles to the long axis of the bone. This will produce a relatively weak union and a weakened bone. A stronger union is produced if the electrodes are placed in opposition across the fracture site, parallel to the long axis of the bone; this facilitates osteogenesis of bone cells parallel with the long axis of the bone more closely imitating original bone formation. If osteogenesis (calcific deposit) is not desired, the positive electrode should be placed over the treatment site and the negative electrode placed in a relatively distant site, and the protocol described above for osteogenesis should be followed in all other particulars. This technique may be useful in discouraging calcium deposit in joints, muscles or along tendons. 70 References G. Alon, "High Voltage Stimulation," Physical Therapy, 65:6, June 1985. Pp. 890‐895 L.L. Baker, K. Parker and D. Sanderson, "Neuromuscular Electrical Stimulation for the Head‐Injured Patient," Physical Therapy, 63:12, December 1983. Pp. 1967‐1974 S.A. Binder‐Macleod, L.R. McDermond, "Changes in the Force‐Frequency Relationship of the Human Quadriceps Femoris Muscle Following Electrically and Voluntarily Induced Fatigue," Physical Therapy, 72:2, February 1992. Pp. 95‐104 D.P. Currier and R. Mann, "Muscular Strength Development by Electrical Stimulation in Healthy Individuals," Physical Therapy, 63:6, June 1983. Pp. 915‐921 A. Delitto, J.M. McKowen, J.A. McCarthy, R.A. Shively and S.J. Rose, "Electrically Elicited Co‐contraction of Thigh Musculature After Anterior Cruciate Ligament Surgery," Physical Therapy, 68:1, January 1988. Pp. 45‐50 A. Delitto and S.J. Rose, "Comparative Comfort of Three Waveforms Used in Electrically Eliciting Quadriceps Femoris Muscle Contractions," Physical Therapy, 66:11, November 1986. Pp. 1704‐1707 L.F. Eckerson and J. Axelgaard, "Lateral Electrical Surface Stimulation as an Alternative to Bracing in the Treatment of Idiopathic Scoliosis," Physical Therapy, 64:4, April 1984. Pp. 483‐490 C.B. Killian, "Electrical Stimulation Overview Introduction to High Frequency Stimulation," Presented at a Combined Section Meeting in Orlando, Florida, February 1985. [Reprint available from Mr. Clyde Killian, Department of Physical Therapy, 1400 East Hanna Avenue, Indianapolis, In, 46227.] T. Mohr, B. Carlson, C. Sulentic and R. Landry, "Comparison of Isometric Exercise and High Volt Galvanic Stimulation on Quadriceps Femoris Muscle Strength," Physical Therapy, 65:5, May 1985. Pp. 607‐609 R.A. Newton and T.C. Karselis, "Skin pH Following High Voltage Pulsed Galvanic Stimulation," Physical Therapy, 63:10, October 1983. Pp. 1593‐ 1596 A.J. Nitz and J.J. Dobner, "High Intensity Electrical Stimulation Effect on Thigh Musculature During Immobilization for Knee Sprain," Physical Therapy, 67:2, February 1987. Pp. 219‐222 J. Owens and T. Malone, "Treatment Parameters of High Frequency Electrical Stimulation as Established on the Electro‐Stim 180," JOSPT, 4:3, winter 1983. Pp. 162‐168 R. Packman‐Braun, "Relationship Between Functional Electrical Stimulation Duty Cycle and Fatigue in Wrist Extensor Muscles of Patients with Hemi paresis," Physical Therapy, 68:1, January 1988. Pp. 51‐56 D.M. Selkowitz, "Improvement in Isometric Strength of the Quadriceps Femoris Muscle After Training with Electrical Stimulation," Physical Therapy, 65:2, February 1985. Pp. 186‐196 W.J. Shriber, A Manual of Electrotherapy, Lea & Febiger, Philadelphia, Pa., 1975. Pp. 110‐123, 139‐147 D.R. Sinacore, A. Delitto, D.S. King, S.J. Rose, "Type II Fiber Activation with Electrical Stimulation: A Preliminary Report," Physical Therapy, 70:7, July 1990. Pp. 416‐422 G.K. Stillwell, Therapeutic Electricity and Ultraviolet Radiation, The Williams & Wilkins Co., Baltimore, Md., 1983. Pp. 1‐64, 65‐108, 124‐173 R.A. Wong, "High Voltage Versus Low Voltage Electrical Stimulation," Physical Therapy, 66:8, August 1986. Pp. 1209‐1214 71 Circulation Enhancement M. Brown and P.P. Gogia, "Effects of High Voltage Stimulation On Cutaneous Wound Healing in Rabbits," Physical Therapy, 67:5, May 1987. Pp. 662‐667 C. Brown, O. Hudlicka, and G. Vrbova, "The Effects of Different Patterns of Muscle Activity on Capillary Density, Mechanical Properties and Structure of Slow and Fast Rabbit Muscles," Pflugers Arch., 361:241, 1979. F.R. Clemente, D.H. Matulionis, K.W. Barron, D.P. Currier, "Effect of Motor Neuromuscular Electrical Stimulation on Microvascular Perfusion of Stimulated Rat Skeletal Muscle," Physical Therapy, 71:5, May 1991. Pp. 397‐406 D.P. Currier, C.R. Petrilli and A.J. Threlkeld, "Effect of Graded Electrical Stimulation on Blood Flow to Healthy Muscle," Physical Therapy, 66:6, June 1986. Pp. 937‐943 O. Hudlicka, M. Brown, M. Cotter, M. Smith, and G. Vrbova, "The Effect of Long‐term Stimulation of Fast Muscles on Their Blood Flow, Metabolism and Ability to Withstand Fatigue," Pflugers Arch., 369:141, 1977. H‐I. Liu, D.P. Currier and A.J. Thelkeld, "Circulatory Response of Digital Arteries Associated with Electrical Stimulation of Calf Muscle in Healthy Subjects," Physical Therapy, 67:3, March 1987. Pp. 340‐350 T. Mohr, T.K. Akers and H.C. Wessman, "Effect of High Voltage Stimulation on Blood Flow in the Rat Hind Limb," Physical Therapy, 67:4, April 1987. Pp. 526‐533 R. Myrhage and O. Hudlicka, "Capillary Growth in Chronically Stimulated Adult Skeletal Muscle as Studied by Intravital Microscopy and Histological Methods in Rabbits and Rats," Mirovasc Res 16:73, 1978. S. Salmons and F.A. Streter, "The Adaptive Response of Skeletal Muscle to Increased Use," Muscle Nerve, 4:94, 1981. G.K. Stillwell, Therapeutic Electricity and Ultraviolet Radiation, The Williams & Wilkins Co., Baltimore, Md., 1983. Pp. 130‐131 J.E. Tracy, D.P. Currier, A.J. Threlkeld, "Comparison of Selected Pulse Frequencies from Two Different Electrical Stimulators on Blood Flow in Healthy Subjects," Physical Therapy, 68:10, October 1988. Pp. 1526‐1532 D.C. Walker, D.P. Currier and A.J. Threlkeld, "Effects of High Voltage Pulsed Electrical Stimulation on Blood Flow," Physical Therapy, 68:4, April 1988. Pp. 481‐485 Edema Reduction G. Alon, "High Voltage Stimulation," Physical Therapy, 65:6, June 1985. Pp. 890‐895 J.A. Bettany, D.R. Fish, F.C. Mendel, "Influence of High Voltage Pulsed Direct Current on Edema Formation Following Impact Injury," Physical Therapy, 70:4, April 1990. Pp. 219‐224 K.A. Cosgrove, G. Alon, S.F. Bell, S.R. Fischer, N.R. Fowler, T.L. Jones, J.C. Myaing, T.M. Crouse, L.J. Seaman, "The Electrical Effect of Two Commonly Used Clinical Stimulators on Traumatic Edema in Rats," Physical Therapy, 72:3, March 1992. Pp. 227‐233 D.R. Fish, F.C. Mendel, A.M. Schultz, L.M. Gottstein‐Yerke, "Effect of Anodal High Voltage Pulsed Current on Edema Formation in Frog Hind Limbs," Physical Therapy, 71:10, October 1991. Pp. 724‐733 A.C. Guyton, Textbook of Medical Physiology, W.B. Saunders Co., Philadelphia, Pa., 1971. Pp. 242‐248 C.B. Killian, "Electrical Stimulation Overview Introduction to High Frequency Stimulation," Presented at a Combined Section Meeting in Orlando, Florida, February 1985. [Reprint available from Mr. Clyde Killian, Department of Physical Therapy, 1400 East Hanna Avenue, Indianapolis, In., 46227.] J. Owens and T. Malone, "Treatment Parameters of High Frequency Electrical Stimulation as Established on the Electro‐Stim 180," JOSPT, 4:3, winter 1983. Pp. 162‐168 72 B.V. Reed, "Effect of High Voltage Pulsed Electrical Stimulation on Microvascular Permeability to Plasma Proteins," Physical Therapy, 68:4, April 1988. Pp. 491‐495 W.J. Shriber, A Manual of Electrotherapy, Lea & Febiger, Philadelphia, Pa., 1975. Pp. 110‐123, 139‐147 G.K. Stillwell, Therapeutic Electricity and Ultraviolet Radiation, The Williams & Wilkins Co., Baltimore, Md., 1983. p. 151 K. Taylor, D.R. Fish, F.C. Mendel, H.W. Burton, "Effect of a Single 30‐Minute Treatment of High Voltage Pulsed Current on Edema Formation in Frog Hind Limbs," Physical Therapy, 72:1, January 1992. Pp. 63‐68 K. Taylor, D.R. Fish, F.C. Mendel, H.W. Burton, "Effect of Electrically Induced Muscle Contractions on Posttraumatic Edema Formation in Frog Hind Limbs," Physical Therapy, 72:2, February 1992. Pp. 127‐132 R.A. Wong, "High Voltage Versus Low Voltage Electrical Stimulation," Physical Therapy, 66:8, August 1986. Pp. 1209‐1214 Muscle Toning G. Alon, "High Voltage Stimulation," Physical Therapy, 65:6, June 1985. Pp. 890‐895 L.L. Baker, K. Parker and D. Sanderson, "Neuromuscular Electrical Stimulation for the Head‐Injured Patient," Physical Therapy, 63:12, December 1983. Pp. 1967‐1974 L.L. Baker, C. Yeh, D. Wilson and R.L. Waters, "Electrical Stimulation of Wrist and Fingers for Hemiplegic Patients," Physical Therapy, 59:12, December 1979. Pp. 1495‐1506 U. Bogataj, N. Gros, M. Malezic, B. Kelih, M. Kljajic, R. Acimovic, "Restoration of Gait During Two to Three Weeks of Therapy with Multichannel Electrical Stimulation," Physical Therapy, 69:5, May 1989. Pp. 319‐327 D.P. Currier, J. Lehman and P. Lightfoot, "Electrical Stimulation in Exercise of the Quadriceps Femoris Muscle," Physical Therapy, 59:12, December 1979. Pp. 1508‐1512 D.P. Currier and R. Mann, "Pain Complaint: Comparison of Electrical Stimulation with Conventional Isometric Exercise," The Journal of Orthopaedic and Sports Physical Therapy, 5:6, 1984. Pp. 318‐323 D.P. Currier and R. Mann, "Muscular Strength Development by Electrical Stimulation in Healthy Individuals," Physical Therapy, 63:6, June 1983. Pp. 915‐921 A. Delitto, J.M. McKowen, J.A. McCarthy, R.A. Shively and S.J. Rose, "Electrically Elicited Co‐contraction of Thigh Musculature After Anterior Cruciate Ligament Surgery," Physical Therapy, 68:1, January 1988. Pp. 45‐50 A. Delitto, J.M. McKowen, J.A. McCarthy, R.A. Shively, S.J. Rose, "Electrically Elicited Co‐Contraction of Thigh Musculature After Anterior Cruciate Ligament Surgery," Physical Therapy, 68:1, January 1988. Pp. 45‐50 A. Delitto, S.J. Rose, J.M. McKowen, R.C. Lehman, J.A. Thomas, R.A. Shively, "Electrical Stimulation Versus Voluntary Exercise in Strengthening Thigh Musculature After Anterior Cruciate Ligament Surgery," Physical Therapy, 68:5, May 1988. Pp. 660‐663 A. Delitto, L. Snyder‐Mackler, "Two Theories of Muscle Strength Augmentation Using Percutaneous Electrical Stimulation," Physical Therapy, 70:3, March 1990. Pp. 158‐164 A. Delitto and S.J. Rose, "Comparative Comfort of Three Waveforms Used in Electrically Eliciting Quadriceps Femoris Muscle Contractions," Physical Therapy, 66:11, November 1986. Pp. 1704‐1707 L.F. Eckerson and J. Axelgaard, "Lateral Electrical Surface Stimulation as an Alternative To Bracing in the Treatment of Idiopathic Scoliosis," Physical Therapy, 64:4, April 1984. Pp. 483‐490 C.B. Killian, "Electrical Stimulation Overview Introduction to High Frequency Stimulation," Presented at a Combined Section Meeting in Orlando, Florida, February 1985. [Reprint available from Mr. Clyde Killian, Department of Physical Therapy, 1400 East Hanna Avenue, Indianapolis, In., 46227.] 73 J. Kleinkort, Isoelectronic Rehabilitation Program, Dynatronics Research Corporation, Salt Lake City, U., 1986. J.F. Kramer, "Effect of Electrical Stimulation Current Frequencies on Isometric Knee Extension Torque," Physical Therapy, 67:1, January 1987. Pp. 31‐38 J. Kramer, D. Lindsay, D. Magee, S. Mendryk, and T. Wall, "Comparison of Voluntary and Electrical Stimulation Contraction Torques,” Journal of Orthopaedic and Sports Medicine Physical Therapy, 5:6, May/June, 1984. Pp. 324‐331 R.K. Laughman, J.W. Youdas, T.R. Garrett, and E.Y.S. Chao, "Strength Changes in the Normal Quadriceps Femoris Muscle as a Result of Electrical Stimulation," Physical Therapy, 63:4, April 1983. Pp. 494‐499 R.L. Lieber, M.J. Kelly, "Factors Influencing Quadriceps Femoris Muscle Torque Using Transcutaneous Neuromuscular Electrical Stimulation," Physical Therapy, 71:10, October 1991. Pp. 715‐723 T. Mohr, B. Carlson, C. Sulentic and R. Landry, "Comparison of Isometric Exercise and High Volt Galvanic Stimulation on Quadriceps Femoris Muscle Strength," Physical Therapy, 65:5, May 1985. Pp. 606‐609 A.J. Nitz and J.J. Dobner, "High Intensity Electrical Stimulation Effect on Thigh Musculature During Immobilization for Knee Sprain," Physical Therapy, 67‐2, February 1987. Pp. 219‐222 J. Owens and T. Malone, "Treatment Parameters of High Frequency Electrical Stimulation as Established on the Electro‐Stim 180," Journal of Orthopaedic and Sports Physical Therapy, 4:3, 1983. Pp. 162‐168 R. Packman‐Braun, "Relationship Between Functional Electrical Stimulation Duty Cycle and Fatigue in Wrist Extensor Muscles of Patients with Hemiparesis," Physical Therapy, 68:1, January 1988. Pp. 51‐56 C.A. Phillips, "Functional Electrical Stimulation and Lower Extremity Bracing for Ambulation Exercise of the Spinal Cord Injured Individual: A Medically Prescribed System," Physical Therapy, 69:10, October 1989. Pp. 842‐849 D.M. Selkowitz, "Improvement in Isometric Strength of the Quadriceps Femoris Muscle After Training with Electrical Stimulation," Physical Therapy, 65:2, February 1985. Pp. 186‐195 C‐L. Soo, D.P. Currier and A.J. Threlkeld, "Augmenting Voluntary Torque of Healthy Muscle by Optimization of Electrical Stimulation," Physical Therapy, 68:3, March 1988. Pp. 333‐337 M.H. Trimble, R.M. Enoka, "Mechanisms Underlying the Training Effects Associated with Neuromuscular Electrical Stimulation," Physical Therapy, 71:4, April 1991. Pp. 273‐282 D.J. Twist, "Acrocyanosis in a Spinal Cord Injured Patient‐Effects of Computer‐Controlled Neuromuscular Electrical Stimulation: A Case Report," Physical Therapy, 70:1, January 1990. Pp. 45‐49 Y. Urabe, "Strengthening the Quadriceps Femoris by Electrical Stimulation," Physical Therapy, 66:2, February 1986. p. 283 D.C. Walker, D.P. Currier and A.J. Threlkeld, "Effects of High Voltage Pulsed Electrical Stimulation on Blood Flow," Physical Therapy, 68:4, April 1988. Pp. 481‐485 R.P. Walmsey, G. Letts, and J. Vooys, "A Comparison of Torque Generated by Knee Extension with a Maximal Voluntary Muscle Contraction vis‐ à‐vis Electrical Stimulation," Journal of Orthopaedic and Sports Medicine Physical Therapy, 6:1, July/August, 1984. Pp. 10‐17 R.A. Wong, "High Voltage Versus Low Voltage Electrical Stimulation, Physical Therapy, 66:8, August 1986. 1209‐1214 Tissue and Bone Repair H. Aro, J. Aho, K. Vaatoranta and T. Ekfors, "Asymmetric Biphasic Voltage Stimulation of the Osteotomized Rabbit Bone," Acta Orthop. Scand., vol. 51, 1980. Pp. 711‐718 M. Brown, M.K. McDonnell, D.N. Menton, "Electrical Stimulation Effects on Cutaneous Wound Healing in Rabbits," Physical Therapy, 68:6, June 1988. Pp. 955‐960 74 J.A. Feeder, L.C. Kloth, G.D. Gentzkow, "Chronic Dermal Ulcer Healing Enhanced with Monophasic Pulsed Electrical Stimulation," Physical Therapy, 71:9, September 1991. Pp. 639‐649 J.W. Griffin, R.E. Tooms, R.A. Mendius, J.K. Clifft, R.V. Zwaag, F. El‐Zeky, "Efficacy of High Voltage Pulsed Current for Healing of Pressure Ulcers in Patients with Spinal Cord Injury," Physical Therapy, 71:6, June 1991. Pp. 433‐444 D.B. Harrington and R. Meyer, "Effects of Small Amounts of Electric Current at the Cellular Level," Annals of the N.Y. Academy of Science, vol. 238, October 11, 1974. Pp. 300‐305 M.J. Im, W.P.A. Lee, J.E. Hoopes, "Effect of Electrical Stimulation on Survival of Skin Flaps in Pigs," Physical Therapy, 70:1, January 1990. Pp. 37‐ 40 J. Kahn, "Transcutaneous Electrical Nerve Stimulation for Nonunited Fractures," Physical Therapy, 62:6, June 1982. Pp. 840‐844 C.B. Kincaid, K.H. Lavoie, "Inhibition of Bacterial Growth In Vitro Following Stimulation with High Voltage, Monophasic, Pulsed Current, Physical Therapy, 69:8, August 1989. Pp. 651‐655 L.C. Kloth, J.A. Feedar, "Acceleration of Wound Healing with High Voltage, Monophasic, Pulsed Current," Physical Therapy, 68:4, April 1988. Pp. 503‐508 K. Piekarski, O. Demetriades and A. Mackensie, "Osteogenetic Stimulation by Externally Applied DC Current," Acta Orthop. Scand., vol. 49, 1978. Pp. 113‐120 B.A. Rowley, J.M. McKenna and G.R. Chase, "The Influence of Electrical Current on an Infecting Microorganism in Wounds," Annals of the N.Y. Academy of Sciences, vol. 238, October 11, 1974. Pp. 543‐551 I. Yasuda, "Mechanical and Electrical Callus," Annuls of the N.Y. Academy of Science, vol. 238, October 11, 1974. Pp. 457‐465 75