Value Based Drug Assessment - Healthcare Supply Chain Association
advertisement

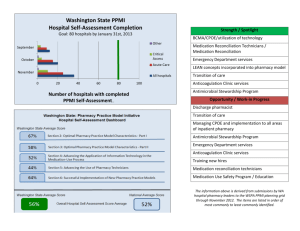
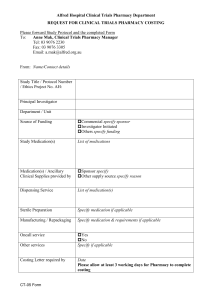
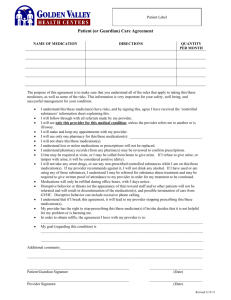
Value Based Drug Assessment Terri Corbo, PharmD, BCPS, FASHP, Vice President, Pharmacy Services, Christiana Care Health System Brian Sayre, PharmD, Health System Director of Pharmacy, Charleston Area Medical Center Martin Caponi, RPh, Director of Pharmacy, PeaceHealth Moderator: Fred Pane, RPh, BS Pharmacy, FASHP, Senior Director, The Medicines Company Adding Value to the Medication Formulary Process Terri Corbo, PharmD, BCPS, FASHP Christiana Care Health System Newark, Delaware The Concept of Value Can be defined as health outcomes achieved per dollar spent Is not a synonym for cost reduction Defined around/by the customer N Engl J Med 2010; 363:2477-2481 Criterion of Medication Value Efficacy Value = Societal Benefit Risk Cost Efficacy Four Factors within Efficacy Outcome Tolerability Evidence Duration Cure or prevention is weighted more heavily than Slows progression is weighted more heavily than End of Life Care Assessment based upon the percentage of patients dropping out of the study Modeled after the ‘strength/levels of evidence’ used by well respected consensus generating groups Data showing benefit for > 3 years is weighted the most heavily; benefit for < 3 months is weighted the least heavily Efficacy Efficacy [(Outcome x Tolerability) + Duration] x Evidence Multiplier Risk Risk Assessment • An internally developed score card 14 items containing both external and internal items indicative of risk Internal risk indicators generated from our medication event and adverse drug reaction reporting programs Cost Cost An assessment of overall revenue relative to cost If the medication requires use of routine labs or tests, those costs are included in the assessment in addition to medication cost Societal Benefit Societal Benefit Team Team members: • • • • • professor of political science and health policy professor of anthropology high school teacher pastor community activist Societal Benefit Societal Benefit Team Primary principles of societal benefit as defined by the team 1. societal benefit is linked to improving quality of life 2. there should be sustained benefit to both the community and the institution Total Medication Value Score High Score Value = Low Score Moderate Score Conclusion The traditional process of evaluating medications for formulary addition does not provide the components necessary for a value assessment Institutions can move toward a value assessment by adding patients as evaluators and assessing outcomes relative to cost Formulary Drug Selection Brian E. Sayre, PharmD Health System Director of Pharmacy Comprehensive Pharmacy Services Charleston Area Medical Center Learning Objectives 1. Understand various factors that are analyzed during the drug selection process 2. Identify opportunities to assist systems in product procurement Charleston Area Medical Center West Virginia’s Largest Medical Center • • • • Memorial Hospital General Hospital Women & Children’s Hospital 838 Licensed Beds Special Designations • • • Level I Trauma Level I PICU Level IV NICU Patient Care • • • • • 600,000 outpatient visits 100,000 ED visits 38,000 discharges 70,000 surgeries 14,000 cath lab procedures Healthgrades 2014 Distinguished Hospital Award What is Value? •Hard to define •Varies by customer •Not a one size fits all approach Value Analysis for Formulary Selection 1. Safety 2. Efficacy 3. Cost 4. Operations Safety 1. Look-alike / sound-alike drugs (LASA) 2. Reported adverse event or mix-ups 3. REMS requirements 4. Ease of Use 5. Mechanism of safety device Efficacy 1. Evidence Based Medicine 2. Advantages over current formulary items 3. Novel strategy 4. New delivery Cost 1. Price of medication 2. Impact on labor resources 3. Impact of length of stay 4. Ancillary costs Operations 1. Ease of integration with computer systems 2. Compatibility with automation 3. Education of hospital team 4. Special handling/preparation requirements 5. Waste Brand versus Generic Drug 1. Branded products limit diversity of manufacturers 2. Generic drugs may have multiple manufacturers available 3. Opportunity for added value Selecting a Manufacturer 1. 2. 3. 4. 5. Price • Lowest cost item • History of price increases • 340B price • WAC price Supply • Drug shortages • Failure to ship • Guarantee supply? Barcode • Type • Consistency in readability Partnership • Willingness to work with hospital Others • Vial size Summary 1. Value depends on the customer 2. Safety, Efficacy, and Cost are considerations 3. Integration into operations should be considered 4. Manufacturers have an opportunity to work with customers to determine how best to meet their needs EHR-CPOESAFETY QUALITY and Value Martin Caponi, BS Pharm. PeaceHealth-Pharmacy Champion Objectives Brief Overview of CPOE (how we got here) Error Reduction HITECH & Meaningful Use Clinical Decision Support EHR-CPOE & Medication Safety Projects - Results EHR Value and memes Safety Technology Convergence Martin’s Crystal Ball? Error Reduction - The Journey Harvard Medical Practice Study (1991) - 3.7% of hospitalized patients experienced adverse events IOM Report (1999) - Systems of care cause 48k-98k deaths/yr. IOM AHRQ NQF Evidence Based Practice Center Evidence Report 43 (2001) The EBP study focused on randomized clinical trials and biomedical (read technology) improvements in patient care… not error reduction and CPOE represents a “clear opportunity for research” Health systems implemented error reduction strategies based on actual errors and not based on randomized clinical trials Preventable Adverse Events3rd Leading Cause of Death (210,000 - 400,00 death/yr. 2008 data) Incentives to Change HITECH & Meaningful Use 2009 HITECH Act - $26B to providers and health care sys. Aimed at increasing utilization of HIT to make care safer Meaningful Use (incentives penalties) & Interoperability Medication related MU measures Active allergy and medication lists Drug-Drug and Drug-Allergy checking E-prescribing (Note: C-II’s special case NY law) Drug formulary checking Implement medication reconciliation MU stage 2 - 60% of IP medication orders via CPOE Creates challenges for providers – takes more time to enter e-orders 2005 study by Hillestad et al. on potential benefits of e-medical records, est. saving of $142-$371 B via better safety and improved efficiency (over 14 years) EHR-CPOE- Value & Safety Treatment, coding and safety measures built into ordersets Ordersets guide care and are pulled in automatically based on patient diagnosis CDS is configurable for both soft stops and hard stops that require input to proceed (forcing functions) Orderset can be suppressed based on facility specific parameters (CAH vs. Community Hosp.) Integration allows for merging ordersets for patients with complex care Order panels can be built to assure EBM and MU Clinical Decision Support (CDS) Metric for HIT & Medication Safety (Journal of Hospital Pharmacy) Literature review evaluated if “uniformity exist in choosing metrics to assess the impact of HIT/EHRs on medication safety-related outcomes” Results- 43 articles reviewed, 34 different measures use and 60% of measures were utilized in 2 or fewer articles No standard metric and a lot of variance! Measuring Medication Safety Measuring EHR-CPOE medication safety challenges Medication PAE’s are a small % of total orders, making it nearly impossible to power a RCT Errors occur 1/1000, and 10% the errors cause harm (1/10,000), means one would need to analyze 100,000 orders to be evidence of harm Safe Systems- TMIT EHR-CPOE flight simulator to test the safety of the CDS & CPOE system design “Trust but verify” becomes ‘Test and verif Medication Process Errors Mediation Safety- Results CPOE EHR- VBP & Benefits One e-chart that replaces inefficient paper charts Eliminate transcription time/cost and errors Integrated order workflow CDS best practice alerts demonstrate 85% reduction in provider order entry errors and duplicate therapy/test Standardize evidence based order sets (limit variation) Extend Bar-code meds to ED and Surgery pre/post-op MU and Core Measures built in The goal is to achieve the benefit metrics and not just complete the technical install Better patient care and several studies show improvement in medication safety (results do vary based on IT system, level of integration, and effective clinical decision support (CDS) Health Care Memes of 2010 - TBD In 20??, XYZ health system recognized an opportunity to increase EMR adoption while also meeting Meaningful Use objectives by mandating computerized provider order entry (CPOE). This presented a challenge because it exposed significant deficiencies in how clinicians…[insert issues here] Ambulatory provider productivity drops with the implementation of a new enterprise EHR and it can take more the 6 months to return to pre-implementation productivity. Martin’s Crystal Ball? Health care will utilized Mo-Sol-Clo strategy Big data future state- 70% ‘I’ and 30% ‘T’ ACA includes 2% Medicare cut (if Medicare represents 50% of patients, than 6% of bottom line is at risk Organizations will not be able to continue commit 30% of capital to HIT “Retalization” of health care (Part D, Exchanges, CVS) ACA- reduce cost for who? Some ACO will chose not to join exchanges Future of acute care pharmacy practice?? Questions? Contact information Martin Caponi mcaponi@peacehealth.org