Intramedullary nailing and plate osteosynthesis for fractures of the
advertisement

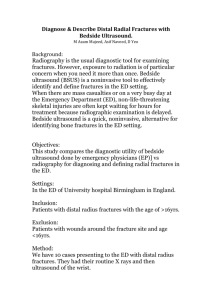
Journal of Orthopaedic Surgery ����������������� 2009;17(3):317-20 Intramedullary nailing and plate osteosynthesis for fractures of the distal metaphyseal tibia and fibula Ajay Krishan, Chetan Peshin, Dara Singh Department of Orthopaedics, GMC Jammu, India ABSTRACT Purpose. To assess the results of concurrent intramedullary nailing plus plate osteosynthesis for fractures of the distal tibia and fibula. Methods. 15 men and 10 women (mean age, 35 years) with concurrent fractures of the distal tibia and fibula underwent intramedullary nailing (for the tibia) and plate osteosynthesis (for the fibula). 17 fractures were type A1, 6 type A2, and 2 type A3. Compound type IIIB or more extensive fractures were excluded. Results. The mean follow-up duration was 2 years. The mean time to bone union was 20 weeks. Six patients underwent dynamisation and 4 bone grafting. Two patients had malalignment (angulation of >5º in any plane), but none was rotational. No patient had shortening, hardware breakdown, or deep-seated infection. Two patients had superficial cellulitis at the site of the distal locking screws. Conclusion. Concurrent intramedullary nailing and plate osteosynthesis for fractures of the distal tibia and fibula is effective in preventing malalignment. Plate osteosynthesis for the fibula provides additional stability even when a single distal locking bolt is used to fix the intramedullary nail to the tibia. Key words: bone malalignment; fibula; fracture fixation, internal; fracture fixation, intramedullary; tibia INTRODUCTION Plate osteosynthesis for fractures of the distal tibia is often associated with delayed healing, infection, and hardware problems.1,2 Locked intramedullary nailing is the treatment of choice for closed fractures of the tibial shaft.3,4 For proper alignment, the nail should be centrally placed in both the proximal and distal fragments,1,5 but does not fit properly into the distal fragment of the lower third of the tibia. This places additional stress on the distal locking bolts and may lead to breakage and malalignment. We Address correspondence and reprint requests to: Dr Chetan Peshin, Department of Orthopaedics, GMC Jammu, India. E-mail: chetanpeshin@gmail.com Journal of Orthopaedic Surgery 318 A Krishan et al. Figure 1 Radiographs showing fixation using an interlocking intramedullary nail for fractures of the distal tibia plus a dynamic compression plate for fractures of the distal fibula. assessed the results of intramedullary nailing and plate osteosynthesis for fractures of the distal tibia and fibula. MATERIALS AND METHODS Between June 2005 and October 2007, 15 men and 10 women (mean age, 35 years) underwent intramedullary nailing for fractures of the distal third of the tibia plus plate osteosynthesis (using a one third tubular plate or dynamic compression plate) for fractures of the distal third of the fibula (Figs. 1 and 2). Patients with fractures near the junction of the distal one third, compound type IIIB or more extensive fractures,6 or fractures more than 2 weeks old were excluded. All compound fractures were debrided. 17 fractures were type A1, 6 type A2, and 2 type A3, according to AO classification.7 Road traffic accident was the main cause of injury. In 4 patients with a compound type-IIIA fracture, specialised nails were used as the distance between the distal locking bolt and the nail tip was just 1 cm. In the early period when such nails were unavailable, the distal end of the nail was trimmed using a hack-saw. Due to technical reasons, 12 patients had their intramedullary nails fixed with only one distal locking bolt. Postoperatively, patients were kept non–weightbearing for 12 weeks. Active and passive movements were encouraged. At week 12, the progress of healing Figure 2 Radiographs showing intramedullary nailing using only one distal locking bolt and plate osteosynthesis for segmental fractures of the distal tibia and fibula. was assessed using radiographs and weight bearing was initiated. Malalignment (angulation of >5º in any plane)8 was assessed by comparison with the normal leg. Patients were followed up at weeks 3, 6, 12, and 24, and then every 3 months during the first year and 6 monthly thereafter. RESULTS The mean follow-up duration was 2 years. The mean time to union was 20 weeks. All patients were available for the final follow-up (Table). Six and 4 patients underwent dynamisation and bone grafting, respectively. Two patients had angular malalignment, but none had rotational malalignment. No patient had shortening, hardware breakdown, or deep-seated infection. Two patients had superficial cellulitis near the screw insertion sites and were treated with oral antibiotics, debridement, and dressing. There was no correlation between the number of locking bolts used and malalignment. DISCUSSION The characteristics and treatments offered to patients with fractures of the distal tibia and fibula Vol. 17 No. 3, December 2009 Intramedullary nailing and plate osteosynthesis for fractures of the distal tibia and fibula 319 Table Characteristics and treatment outcomes of the patients Patient Sex/age no. (years) 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 M/23 M/28 M/19 F/34 M/50 M/52 F/40 M/26 F/45 F/28 M/30 M/35 F/33 M/37 F/38 M/40 M/49 F/56 F/51 F/33 M/16 M/19 M/32 M/35 F/36 Fracture type Time to Final angulation bone union AO classification Gustillo classification Anteroposterior Mediolateral (weeks) A1 A2 A1 A2 A1 A3 A1 A1 A1 A1 A1 A1 A2 A1 A1 A2 A1 A1 A1 A1 A2 A1 A1 A2 A3 II IIIA I I II IIIA II I IIIA I IIIA differ from those having more proximal fractures. Intramedullary nailing enables closed stabilisation while preserving vascularity of the fracture site and integrity of the soft-tissue envelope. It is the treatment of choice for fractures of the tibial shaft but not the distal metaphyseal tibia. The intramedullary canal at this level prevents intimate contact between the nail and endosteum.9 There are concerns regarding fixation stability and malunion, especially when less than 2 locking bolts are used to secure the distal fragment.10,11 A fibular plate can therefore be used to enhance stability. In 63 patients treated with intramedullary nailing, all but 5 had satisfactory outcomes.5 Poor outcome was attributed to technical errors; no displacement was noted during nail insertion or locking, even in patients with distal tibial fractures and undisplaced intra-articular involvement.5 In a series of 73 distal leg fractures, 93% were closed, 83% were type A1, 17% had some comminution, and 4 had partial articular involvement.12 Interlocked Grosse-Kempf nails (entailing dynamic locking for simple fractures and static locking for comminuted fractures) were used for tibial fractures and associated fibular fractures were plated before nailing. In fractures at the level of the distal screw, the tip of the 15 14 12 17 19 23 21 17 21 20 17 21 15 21 18 17 19 21 20 20 17 16 18 20 26 5º 6º 4º 3º 5º 5º 11º 3º 4º 3º 8º 7º 8º 7º No. of distal locking bolts used 1 2 1 2 1 3 2 1 1 2 2 2 1 2 1 2 2 1 2 1 2 1 1 2 1 nail was sawed off to allow more distal seating of the nail. 96% of these fractures healed without major complications. There was no shortening of >1 cm or angulation of >5°. The 3 non-unions were managed with dynamisation, bone grafting, or the Ilizarov technique.12 In a biomechanical study, the strength of a shortened intramedullary nail (terminal 1 cm removed) for fractures within 4 cm of tibiotalar joint was not significantly different from that of a standard intramedullary nail for fractures 5 cm from joint.13 Neither construct was strong enough to resist a moderate compression bending load, and weight bearing was restricted until the bone had healed. For fractures of the distal tibia and fibula, the proportion of patients with reduction loss was significantly greater after intramedullary nailing alone than after intramedullary nailing and plate and screw fixation.14 Thus, fibular plating was recommended whenever intramedullary nailing was used in unstable distal tibiofibular fractures. In our study, the incidence of malalignment was negligible, as weight bearing was restricted until radiographic union. Results were satisfactory even when a single locking bolt was used. Only 2 cases had gross malalignment (angulation of >5º in any plane). 320 A Krishan et al. Journal of Orthopaedic Surgery REFERENCES 1. Tanna DD. Interlocking nailing. 2nd ed. New Delhi: Jaypee Publishers; 2004. 2. Olerud S, Karlstrom G. Tibial fractures treated by AO compression osteosynthesis. Experiences from a five year material. Acta Orthop Scand Suppl 1972;140:1–104. 3. Whittle AP, Wood GW. In: Canale ST, editor. Campbell’s operative orthopaedics. 10th ed. St Louis: Mosby; 2003:2757– 61. 4. Schmidt AH, Finkemeier CG, Tornetta P 3rd. Treatment of closed tibial fractures. Instr Course Lect 2003;52:607–22. 5. Robinson CM, McLauchlan GJ, McLean IP, Court-Brown CM. Distal metaphyseal fractures of the tibia with minimal involvement of the ankle. Classification and treatment by locked intramedullary nailing. J Bone Joint Surg Br 1995;77:781– 7. 6. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am 1976;58:453–8. 7. Muller ME, Nazarian S, Koch P. Classification AO des fracture des os longs. Berlin: Springer Verlag; 1998. 8. Freedman EL, Johnson EE. Radiographic analysis of tibial fracture malalignment following intramedullary nailing. Clin Orthop Relat Res 1995;315:25–33. 9. Morin PM, Reindl R, Harvey EJ, Beckman L, Steffen T. Fibular fixation as an adjuvant to tibial intramedullary nailing in the treatment of combined distal third tibia and fibula fractures: a biomechanical investigation. Can J Surg 2008;51:45–50. 10. Strauss EJ, Alfonso D, Kummer FJ, Egol KA, Tejwani NC. The effect of concurrent fibular fracture on the fixation of distal tibia fractures: a laboratory comparison of intramedullary nails with locked plates. J Orthop Trauma 2007;21:172–7. 11. Chen AL, Tejwani NC, Joseph TN, Kummer FJ, Koval KJ. The effect of distal screw orientation on the intrinsic stability of a tibial intramedullary nail. Bull Hosp Jt Dis 2001;60:80–3. 12. Tyllianakis M, Megas P, Giannikas D, Lambiris E. Interlocking intramedullary nailing in distal tibial fractures. Orthopedics 2000;23:805–8. 13. Gorczyca JT, McKale J, Pugh K, Pienkowski D. Modified tibial nails for treating distal tibia fractures. J Orthop Trauma 2002;16:18–22. 14. Egol KA, Weisz R, Hiebert R, Tejwani NC, Koval KJ, Sanders RW. J Orthop Trauma 2006;20:94–103.