Ocular side effects of disopyramide
advertisement

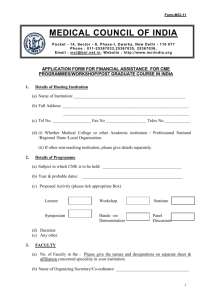
Downloaded from http://bjo.bmj.com/ on March 5, 2016 - Published by group.bmj.com British Journal of Ophthalmology, 1984, 68, 890-891 Ocular side effects of disopyramide J. FRUCHT', FREIMANN,2 AND S. MERIN' From the Departments of ' Ophthalmology and 2Cardiology, Hadassah University Hospital, Kiryat Hadassah, Jerusalem, Israel I. SUMMARY A patient who suffered from severe decrease of accommodation and pupillary dilatation following the systemic use of disopyramide is described. The ocular side effects when this drug is used in large doses result from its anticholinergic action. Disopyramide (4 di-isopropylamino-2 phenyl-2-(2pyridyl) butyramide phosphate) is currently used as an antiarrhythmic drug. ' 2 Its pharmacological effect on the heart is thought to be known.'-3 Disopyramide slows the depolarisation rate of the action potential, depresses phase 4, and prolongs the duration of repolansation.' With the widespread use of the drug several adverse side effects have been described.4 Most were caused by its anticholinergic action and included dry mouth, urinary retention,5 and acute angle closure glaucoma.6 Disopyramide has been reported47 to cause blurred vision, but no explanation of its mechanism or dose dependence was given. We describe a patient who suffered from accommodation and pupillary paralysis as a result of treatment with a high dose of disopyramide for ventricular arrhythmia. The ocular effect of high systemic doses of the drug seems to be equivalent to the anticholinergic effect of topical mydriatics and cycloplegics. tests were within the normal range. The patient had no ocular symptoms. On her second day in hospital the attacks of ventricular tachycardia no longer responded to the usual antiarrhythmic drugs and the cardiologist decided to treat her with high doses of disopyramide. The patient's weight was 49 kg. A dose of 200 mg of disopyramide was injected intravenously and 150 mg six times a day was given orally. On the next day the oral dose was raised to 300 mg six times a day. This dose finally prevented the attacks of ventricular tachycardia. On the day following the disopyramide 101 9= 8. 0 0 0 7. AA A A E E 6- Case report in S- A 16-year-old girl was referred to the Department of Cardiology, Hadassah University Hospital, because of recurrent ventricular tachycardia refractory to treatment by the usual antiarrhythmic drugs (lignocaine, quinidine, pronestyl (procainamide hydrochloride), hydantoin (phenytoin), verapamil, and ajmaline). The patient was healthy until the first ventricular tachycardia one-and-a-half months before the present admission to the hospital. General medical investigations ruled out viral, collagen, and autoimmune diseases. The blood count, sedimentation rate, tri-iodothyronine, thyroxine, thyroid stimulating hormone, calcium, phosphate, and other Correspondence to Dr J. Frucht. A 0* 0. 0 A 4AL A AL A 0 0 0@ A 2- O 1 2 3 4 56 7 8 9 E0 11 12 13 t DcLys t ft Fig. 1 Relationship between pupillary size (@=mm), accommodation (A =dioptres), and days of treatment. The two single arrows indicate beginning and end of disopyramide treatment. The double arrow indicates time of increase of the dose of quinidine to 3 - 2 glday. 890 Downloaded from http://bjo.bmj.com/ on March 5, 2016 - Published by group.bmj.com Ocularside effects of disopyramide 891 treatment the girl complained that she could not see well enough to read, had blurred vision, and a dry mouth. Her visual acuity was OD 6/6, OS 6/7*5+. The pupils were dilated to 8 mm, and the light reflex was poor. The anterior and posterior segments were normal. Refraction showed OD+0-75 6/6 OS+1-00 6/6; near point of convergence 5 cm. In each eye the amplitude of accommodation was 2*50-3*00dioptres. The patient was orthophoric. When +1-00 dioptre was added she could read from a distance of 40 cm. She continued to complain that she could not see well enough to read, had photophobia and a dry mouth. The disopyramide treatment was abruptly stopped on the seventh day, and treatment with quinidine 1*8 g/day was started. This very large dose finally controlled successfully the ventricular tachycardia. Fig. 1 shows the amplitude of accommodation and the pupillary changes during the presence of the symptoms and after stopping the treatment by disopyramide. The patient had recovered from all abnormal ocular signs and symptoms by the next morning 20 hours after taking the last dose of disopyramide. cholinergic effect on the parasympathetic system probably caused the drop of amplitude of accommodation to 2*5-3 dioptres and pupillary dilatation to 8 mm. This effect is very similar to the effect of atropine given by drops. However, the recovery time was much shorter-less than 20 hours after stopping treatment with disopyramide.4 The recorded amplitude of accommodation was 7 dioptres and a day later 8/2 dioptres. This still reduced amplitude of accommodation might be explained by the alternative use of quinidine which also has some antocholinergic effect.'0 Given the next day in a higher dose (3-2 g/day) this drug probably caused the additional reduction in amplitude of accommodation from 8*50 dioptres to 7 dioptres. No effect on pupillary muscles was recorded. The arrhythmia was controlled in our patient by a very large amount of disopyramide. The treatment was stopped because of visual system complications. However, in cases that are not controlled by other antiarrhythmic drugs these complications can be overcome by using additional plus glasses for reading. Discussion References One drop of atropine 1% instilled into the conjunctival sac of a young adult may cause pupillary dilatation to 8 mm and reduction in the amplitude of accommodation from 12 to four dioptres,8 while systemic administration has much less effect. However, 1 mg or 2 mg injected subcutaneously into a person weighing 70 kg reduces the amplitude of accommodation by 20% and by 30% respectively.9 A decrease of amplitude of accommodation, enough to cause inability to read following systemic administration of drugs with known anticholinergic side effects in a young patient, is very unusual. It has never been reported after therapeutic doses of atropine. In the present case the high dose of disopyramide given was similar to the high doses given to patients with stubborn and refractile arrhythmias.4 The anti- 1 Singh BN, Collett JT, Chew CYC. New perspectives in the pharmacologic therapy of cardiac arrhythmias. Prog Cardiovasc Dis 1980; 22: 243-301. 2 Zipes DP, Toup PJ. New antiarrhythmic agents: amiodarone aprinidine, disopiramide, athmozin, mexilectine, tocanide, rerapamile, Am J Cardiol 1978; 41: 1005-24. 3 Danilo LP, Rosen MR. Cardiac effects of disopyramide. Am Heart J 1976; 92: 532-6. 4 Koch-Weser J. Disopyramide. N Engl J Med 1979; 300: 957-62. 5 Large SH, Todd CH. Disopyramide associated with urinary retention. Lancet 1977; ii: 1362. 6 Trope GE, Hind VMD. Closed-angle glaucoma in patient on disopyramide. Lancet 1978; i: 329. 7 Braunwald E. Heart disease. A textbook of cardiovascular medicine. Philadelphia: Saunders, 1980; 713-4. 8 Wolf AV, Hodge HC. Effects of atropine sulfate, methylatropine nitrate (metropine) and hematropic hydrobromide on adult human eyes. Arch Ophthalmol 1946; 36: 293-301. 9 Riker WF Jr. Contributions to medicine by research in pharmacology. JAMA 1962; 179: 355-60. 10 Braunwald E. Heart disease. A textbook of cardiovascular medicine. Philadelphia: Saunders, 1980; 707. Downloaded from http://bjo.bmj.com/ on March 5, 2016 - Published by group.bmj.com Ocular side effects of disopyramide. J Frucht, I Freimann and S Merin Br J Ophthalmol 1984 68: 890-891 doi: 10.1136/bjo.68.12.890 Updated information and services can be found at: http://bjo.bmj.com/content/68/12/890 These include: Email alerting service Receive free email alerts when new articles cite this article. Sign up in the box at the top right corner of the online article. Notes To request permissions go to: http://group.bmj.com/group/rights-licensing/permissions To order reprints go to: http://journals.bmj.com/cgi/reprintform To subscribe to BMJ go to: http://group.bmj.com/subscribe/