Ptosis
advertisement

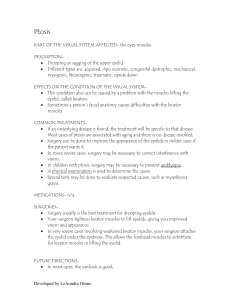
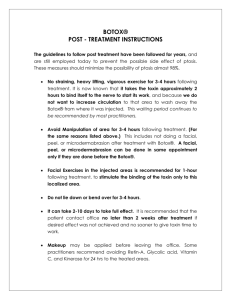
8 Ptosis Clinical Definition It signifies a drooping of the upper eye lid, which may be unilateral or bilateral, and partial or complete. Ptosis occurs due to dysfunction of the muscles that raise the eyelid or their nerve supply. It is more common in the elderly, as muscles in the eyelids may begin to deteriorate. Aetiology Ptosis is of mainly two types: A. Congenital Ptosis: This mainly occurs due to imperfect differentiation of the levator muscle. It is often associated with weakness of underlying superior rectus muscle. B. Acquired Ptosis : In most cases, an acquired drooping of the upper eyelid results from the ageing of the eyelid. Usually the tendon that attaches the ‘lifting’ muscle to the eyelid stretches Before Surgery After Surgery A R A V I N D E Y E C A R E S Y S T E M and the eyelid droops low. Occasionally the condition results from other general conditions such as Myasthenia Gravis (MG), chronic progressive external ophthalmoplegia (CPEO), IIIrd nerve palsy, myasthenia gravis, ocular myopathy, trauma etc. Clinical evaluation of ptosis: Patient history is taken considering the age of onset of the disease, family history,presence of diplopia,systemic problems and so on. Examination is done by calculating the amount of ptosis by noting the ptosis lid margin with respect to the limbus and pupil. Mild ptosis Moderate ptosis Severe ptosis – 2 mm – 3 mm - 4 mm or more Assessment of levator function: 1. The brow is immobilized by pressure with the thumb (to negate the action of frontalis) 2. Patient is asked to look down and then to look up 3. Amount of excursion of the upper lid margin is then measured with a ruler (2 mm of movement is contributed by the superior rectus muscle). Normal - 15 mm Good - 8 mm or more Fair - 5 to 7 mm Poor - 4 mm or less 9 Treatment Brow (Frontalis) suspension 1. 2. 3. 4. This is applicable in bilateral cases where the levator action is poor. Here, the tarsus is fixed to the frontalis muscle, via a sling of fascia late or non – absorbable materials. Fasanella – serral operation Levator resection Brow (Frontalis) suspension Aponeurosis strengthening Fasanella – Serrat operation It is the simple tarso – conjunctival resection and is useful in mild ptosis with good levator function (eg. Horner’s syndrome). Levator resection Useful in congenital unilateral ptosis with fair to good levator function. It may be via: a. Skin approach (Everbusch’s) : Especially where larger resection in necessary b. Conjunctival approach (Blaskowics): Particularly useful for moderate resection of LPS. Aponeurosis strengthening This is useful in acquired ptosis with good levator function and is performed either by advancement or by tucking. Advancement may be combined with levator resection in severe ptosis. Timing of surgery in congenital ptosis Severe Ptosis : Early intervention is necessary due to danger of stimulus deprivation amblyopia. Mild to Moderate Ptosis: Surgical correction is done between 3 – 4 years of age, when accurate measurement can be obtained. - Ms. M.R. Nagarani Refraction, Aravind - Theni Breast Feeding reduces the risk of ROP An international team of doctors have proved breast fed babies drop the risk of retinopathy of prematurity (ROP) from 75% to 90%. Researchers from China, Canada and the UK reanalyzed the studies, done with more than 2000 infants. The new analysis showed the reducing of the risk of ROP and it was published on Nov-16 in the medical journal “Paediatrics”. Studies in U.S. show, that 59% of babies born at 22 to 28 weeks have the ROP disorder. In China 50% of the babies weigh less than one kilogram. Breast feeding helps to prevent two conditions known as sepsis and necrotizing entercolitis which require oxygen therapy. These two conditions are linked with the higher risk of ROP. Mother’s own breast milk serves better than the donor’s milk, in this case, says Dr.Adolf Llanos, a neonatologist of Miami. Source: www.medicine net.com, (16.11.15) Compassion Oct - Dec, 2015