Triosephosphate Isomerase Deficiency: Predictions and Facts
advertisement

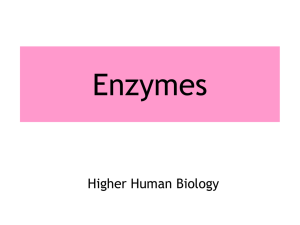
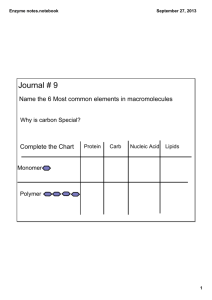
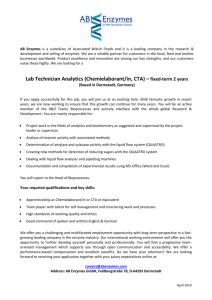
J. theor. Biol. (1996) 182, 437–447 Triosephosphate Isomerase Deficiency: Predictions and Facts* F O,† B G. V́,† S H́,‡ M H́‡ J Ó†§ †Institute of Enzymology, Biological Research Center, Hungarian Academy of Sciences, Budapest, H-1518, P.O. Box 7, Hungary and the ‡National Institute of Haematology, Blood Transfusion and Immunology, Budapest. H-1113, Daróczi út 24, Hungary Deficiencies in around 20 enzymes, associated with widely different degrees of severity and complexity, have been identified for human erythrocytes. The fact that glycolysis is crucial for erythrocyte function is reflected by the large number of inherited glycolytic enzymopathies. Triosephosphate isomerase (TPI) deficiency, a rare autosomal disease, is usually associated with nonspherocytic hemolytic anemia, progressive neurologic dysfunction, and death in childhood. The two affected Hungarian brothers studied by us have less than 3% TPI activity and enormously (30–50-fold) increased dihydroxyacetone phosphate (DHAP) concentration in their erythrocytes. The well-established concept of the metabolic control theory was used to test the contribution of TPI and some related enzymes to the control of a relevant segment of the glycolytic pathway in normal and deficient cells. Deviation indices, DEJ = (DJ/DE) E r/J r, which give a good estimation of flux control coefficients using a single large change in enzyme activity, were determined from the fluxes in the absence and presence of exogeneous enzymes. We found that PFK and aldolase are the enzymes that predominantly control the flux, however, the quantitative values depend extensively on the pH: DEJ values are 0.85 and 0.14 at pH 8.0 and 0.33 and 0.67 at pH 7.2 for aldolase and PFK, respectively. Neither the flux rates nor the capacities of the enzymes seem to be significantly different in normal and TPI deficient cells. There is a discrepancy between DHAP levels and TPI activities in the deficient cells. In contrast to the experimental data the theoretical calculations predict elevation in DHAP level at lower than 0.1% of the normal value of TPI activity. Several possibilities suggested fail to explain this discrepancy. Specific associations of glycolytic enzymes to band-3 membrane proteins with their concomitant inactivation have been demonstrated. We propose that the microcompartmentation of TPI that could further decrease the reduced isomerase activity of the deficient cells, is responsible for the high DHAP level. 7 1996 Academic Press Limited erythrocytes have been identified and it has also long been recognized that the rates of all the metabolic processes of the cell depend on the properties of the enzymes that catalyse each of the required reactions, the number and quality of enzyme molecules present, the temperature and the concentration of substrates, cofactors, activators, inhibitors and the pH within the cell. Attempts have been made to construct computer models that simulate this network of reactions in the red cell (Heinrich et al., 1977; Heinrich & Rapoport, 1974; Rapoport et al., 1974). The glycolytic flux was Glycolysis in the Red Blood Cell The mature red cell has to depend almost solely on anaerobic glycolysis to produce the energy required for its functions (cf. Fig. 1). The process of extracting energy from glucose and the utilization of this energy is carried out by a large number of enzymes. The pathways of energy and redox metabolism of * This paper is dedicated to the memory of Henrik Kacser. § Author to whom correspondence should be addressed. E-mail: ovadi.enzim.hu 0022–5193/96/190437 + 11 $25.00/0 437 7 1996 Academic Press Limited 438 . E T A L . found to be controlled by hexokinase (HK) and phosphofructokinase (PFK). The control strengths for the HK and PFK were calculated to be 0.69–0.73 and 0.31–0.27 at pH 7.2 and 0.87–0.90 and 0.13–0.1 at pH 8.2, respectively (Rapoport et al., 1974). The model was appropriate to describe the glycolytic flux using kinetic parameters determined in diluted systems with isolated enzymes. In addition, it describes the time courses of changes in concentrations of glycolytic intermediates following changes in substrate concentrations (Schauer et al., 1981), and on other effects [for references see Keleti & Ovádi (1988)]. Additional experiments from other laboratories which demonstrate the regulation of glycolysis through the change of energy charge by affecting the activity of PFK and pyruvate kinase (Yoshino & Murakami, 1985) or PFK by ATP and/or HK by glucose 6-phosphate (Ataullakhanov et al., 1981; Meléndez-Hevia et al., 1984) and of PFK and fructose 1,6-bisphosphatase by fructose 2,6-bisphosphate (Hers & Van Schaftingen, 1982) are also consistent with the model. These analyses suggest that ATP concentration is kept constant in the cell by a mechanism in which 2,3-bisphosphoglycerate by-pass acts as an ‘‘energy buffer’’ (cf. Fig. 1), it acts as energy source and ATP change is buffered by variations in the accumulation rate of fructose 1,6-bisphosphate and triose phosphate. The role of PFK in the control of red cell glycolysis has been extensively discussed (Boscá & Corredor, 1984; Fell, 1984). The published data suggest the importance of PFK in the control of erythrocyte glycolysis; however, its control depends on the type of cells which have various PFK isoforms. For example, in tumor cells or in yeast, a relatively high ratio of fructose-1,6-bisphosphate to fructose-6-bisphosphate was found indicating that PFK was not rate-limiting under glucose utilizing steady-state conditions. Therefore, the contribution of the enzymes to the control of glycolytic flux is varied by a number of effects including isoforms and cellular conditions. Compartmentation of Glycolytic Enzymes: New Concept The mathematical models including the recent ones have ignored the experimental observations that certain glycolytic enzymes associate with the erythrocyte membrane and these specific associations alter their catalytic properties. For example, convincing studies with PFK indicated that the activity curve shifts from a sigmoidal shape to a rectangular hyperbola on binding of the enzyme to the erythrocyte membrane (Karadsheh & Uyeda, 1977). Up to now several experiments using a variety of techniques indicated isotonic binding of glycolytic enzymes. Activity of glyceraldehyde-3-phosphate dehydrogenase (GAPD) in vivo was measured by using 1H NMR to monitor non-invasively a couple 1H2H exchange reactions in which the enzyme was involved (Brindle et al., 1982). The study showed that the enzyme was totally inhibited when bound to the band 3 membrane protein of erythrocytes. In a series of studies Steck and his co-workers have demonstrated that glycolytic enzymes bind specifically to the acidic N-terminal region of human erythrocyte band 3 (Jenkins et al., 1985; Tsai et al., 1982). From these enzymes aldolase and GAPD effectively compete with PFK for binding to band 3 protein and release the bound PFK (Higashi et al., 1979). More recently, a rigorous test was developed providing direct evidence for control of glycolysis by binding to the cytoplasmic extension of the anion transporter, band 3 protein in vivo. The glycolytic flux was found to be modulated over 30-fold by controlling the availability of glycolytic enzyme binding sites at extreme N terminus of the anion transporter, band 3 (Low et al., 1993). By regulating the occupancy of the enzyme binding site at the N terminus of the anion transporter, the cell has the potential to adjust its glycolytic flux over a wide range. The role of the isoenzyme-specific interactions in the regulation of glycolysis in various tissues has been extensively emphasized (for review see Ovádi, 1995). The presence of isoenzymes in several metabolic steps can keep multiple pools of intermediates by isoenzyme-isoenzyme associations as demonstrated for conversion of glucose-6-phosphate to pyruvate or glycogen via glycolytic or gluconeogenic pathways (Ureta, 1978, 1991). Recently we provided evidence that the different isoforms of brain PFK exhibited different affinity towards MAP-containing microtubules (Vértessy et al. 1996). C-type PFK that predominantly occurs in brain and tumor cells has much lower affinity to MTs than M-type has. The muscle type PFK under identical conditions binds to MTs while the binding of C isoform is not significant. The binding of muscle enzyme reduces the overall activity of the kinase since the inactive dissociated form of the enzyme associates with MTs. This finding may have physiological relevance and it may partly explain the high uncontrolled glycolytic rate in tumor cells. The data available about binding of glycolytic enzymes to microtubule suggest that the glycolytic enzymes with high isoelectric point bind to the acidic C-terminal ‘‘tail’’ of a subunit of tubulin (Carr & Knull, 1993; Itin et al., 1993; Volker & Knull, 1993). 439 GLUCOSE ATP *Hexokinase ADP G6P *Glucosephosphate isomerase F6P ATP *Phosphofructokinase ADP FDP *Aldolase DHAP *Triosephosphate isomerase GAP Pi NAD Glyceraldehyde-3phosphate dehydrogenase NADH 1,3-DPG *Diphosphoglycerate mutase ADP *Phosphoglycerate kinase 2,3-DPG Pi *Diphosphoglycerate phosphatase ATP 3PG *Phosphoglycerate mutase 2PG *Enolase PEP ADP ATP *Pyruvate kinase PYRUVATE NADH *Lactate dehydrogenase + NAD LACTATE F. 1. The glycolytic pathway in human erythrocytes. Enzymes whose deficiency have been demonstrated are indicated by an asterisk. For simplicity all reactions are denoted with single arrows. The portions of glycolysis studied in this paper are indicated by solid or dotted lines. . E T A L . 440 This C-terminal binding domain of a tubulin shares many properties with the N-terminal binding domain of human erythrocyte band 3 including sequence homology (Knull & Walsh, 1992). Since it has been demonstrated that glycolytic enzymes specifically bind to the acidic N-terminal region of band-3 membrane protein in RBC, it appears, therefore, that the binding of glycolytic enzymes to domains of either MTs or red cell membrane is highly specific and it produces similar functional consequences. These macromolecular associations have yet to be taken into account in order to understand the regulation of energy production in the RBC and the molecular alterations of diseases caused by inherited or acquired enzyme deficiency. Enzyme Deficiency Extensive evidence indicates that the metabolism of cells can be impaired if the activity of only one of the participating enzymes is altered by spontaneous mutations (inherited or acquired enzymopathies) or by the administration of toxic drugs or for any other reason (Schuster & Holzhütter, 1995). The fact that glycolysis is crucial for RBC function is reflected by the large number of inherited glycolytic enzymopathies found to result in hemolysis or other aberrations (Tanaka & Zerez, 1990). Based on the energy dependence of mature erythrocytes on glycolysis, the depletion of ATP has been proposed to be the cause of the shortened life span in deficiencies of the glycolytic enzymes (Valentine et al., 1984). However, low red cell ATP levels are not invariably associated with loss of viability, and circulating ATP levels are not necessarily diminished in patients with glycolytic enzymopathies (Beutler, 1980). For human erythrocytes, deficiencies of about 20 enzymes, associated with widely different degrees of severity and complexity have been identified so far (Fuji & Miwa, 1990; Valentine & Paglia, 1984). Nevertheless, quantitative relationships between the degree of enzyme deficiency and the extent of metabolic dysfunction are very difficult to establish experimentally. For most enzymopathies, the experimental and clinical observations can be satisfactorily rationalized by the computational results [Schuster & Holzhütter (1995) and references therein]. The models for the main metabolic pathways of the human erythrocyte were successfully employed to describe stationary and time-dependent metabolic states of the cells under normal physiological conditions as well as in the presence of enzyme deficiencies. Recently a mathematical model was evaluated for predicting the metabolic effect of large-scale enzyme activity alter- ations. This model was applied for study of enzyme deficiencies of RBCs (Schuster & Holzhütter, 1995). Triosephosphate isomerase (TPI) deficiency is a rate autosomal disease. There are only some 30 cases reported so far [Hollán et al., (1993) and references therein]. Although several isoenzymes have been identified in normal tissues, none of them have been observed to be specifically associated with a functionally deficient state. Clinically significant TPI deficiency is usually associated with non-spherocytic hemolytic anemia, progressive neurologic dysfunction, and death in childhood (Hollán et al., 1993). TPI, notable for its high catalytic efficiency, enhances the movement of a single proton to interconvert DHAP and GAP in glycolysis and gluconeogenesis by a factor of about 1010 (Nickbarg & Knowles, 1988). The rate of catalysis is diffusion limited (Rose et al., 1990), and the equilibrium favours the formation of DHAP by 20:1 (Lolis & Petsko, 1990). In fact, in the erythrocyte the most striking metabolic abnormality is the 20- to 60-fold increase in the concentration of DHAP, the substrate for the enzyme, suggestive of an almost complete metabolic block at this step (Valentine & Paglia, 1984). Therefore, the disease could be a consequence of an increased concentration of DHAP. Little or no modifications occur in the levels of ATP and 2,3-diphosphoglycerate (Hollán et al., 1993). In Hungary a 13-year-old boy (B.J. Jr.) with congenital hemolytic anemia and hyperkinetic torsion dyskinesia was found to have severe TPI deficiency (cf. Table 1). One of his two brothers, (A.J.), a 23-year-old amateur wrestler has hemolytic anemia as well, but no neurological signs or symptoms. Both are compound heterozygotes and have equally less than 3% TPI activity in their red cells. Both parents and a third brother are healthy heterozygote carriers of the defect. The main characteristics of the TPI-deficient Hungarian family are summarized in Table 1. A.J. represents a unique phenotype from the point of view that all published homozygotes and compound heterozygotes had severe neurological alterations from infancy or early childhood. In contrast to the two affected Hungarian brothers, apart from one patient (Harris et al., 1970), all compound heterozygotes died under the age of 6 years. The dramatic decrease of TPI activity occurs during the time course of biological evolution due to spontaneous mutations affecting the amino acid sequence, and, thus, the spatial arrangement of enzyme molecules. The Hungarian family is characterized by two mutations: one is mis-sense mutation within codon 240 (Chang et al., 1993). The other mutation has been recently localized (Hollán et al., 0 +++ 0 0 0 0 0 + + 0 0 0 Neurologic disordera 44 71 pearly white pearly white NT yellow gel-like 546 2 35 NT pearly white pink 20–27 854 2 1 None Partial Partial Total None Total DHAP level Characteristics of TPI nmol/ml RBC isolated ghosts thermolabilitya NT NT NT NT 745a 436a 644a 11.1 2 2.1 12.3 2 3.5 40.0 2 1.7 1051–1842 31.5 2 1.0 NT NT NT NT 3.2 2 0.9 3.3 2 0.2 Enzyme activity (Vmax ) U/g hemoglobin TPI PFK Aldolase DHAP level in whole blood was determined as in (Hollán et al., 1993). Enzyme activities were measured according to (Beutler et al., 1977). TPI activity was measured with GAP as a substrate. Ghosts were prepared according to (Vértessy & Steck, 1989). NT, not tested; a, data taken from (Hollán et al., 1993). Normal Propositus (B.J. Jr.) Brother (A.J.) Brother (T.J.) Mother (Mrs. B.J.) Father (B.J.) Hemolytic anemiaa T 1 Characteristic features in the members of the TPI deficient family 441 . E T A L . unpublished). The modified TPI termed ‘‘deficient’’ has a slightly higher Michaelis constant for DHAP but normal Michaelis constant for GAP. The mutant enzyme is heat unstable and has slower electrophoretic mobility as compared with the normal enzyme (Hollán et al., 1993). In spite of the considerable amount of knowledge accumulated about this rare genetic defect, the pathomechanism of both the hemolytic anemia and the neurological symptoms is still obscure. 30 [NADH] (µM) 442 20 Control PFK TPI Aldolase 10 0 2 4 6 Time (min) 8 10 Flux Studies in Normal and TPI Deficient Hemolysates 30 [NADH] (µM) In the cases where clinically manifested TPI defect was identified the TPI activities in erythrocytes varied between 1.6–28% of the normal value. In most cases (from 28 diseased persons) the TPI activity was less than 20.0% (Eber et al., 1991). The two affected Hungarian brothers have less than 3% activity in their RBCs (cf. Table 1). Since the activity of TPI is the highest of any glycolytic enzyme in RBCs, it has virtually no control property in normal cells and thus one can ask whether the reduced TPI occurring in deficient cells is able to sustain the normal glycolytic flux to produce the appropriate energy for red cell functions. The influence of particular enzyme activities on the flux of metabolites in a pathway can be estimated by ‘‘modulating’’ enzymes and measuring the response in selected parts of the system. In this particular case we analysed a relevant segment of glycolysis including TPI and some related enzymes but not HK which is known to be by far the enzyme of lowest capacity. The well-established concept of the metabolic control theory (Heinrich & Rapoport, 1974; Kacser & Burns, 1973) was used in our laboratory to test the contribution of TPI to the control of the segments of glycolytic pathway in TPI deficient cells in comparison to normal cells. In the first type of experiment the basic flux of normal and TPI deficient cells were analysed with excess Fru-6-P, Mg-ATP and NADH as substrates (cf. Fig. 2). In this case the formation of DHAP produced by the PFK/aldolase/TPI catalysed consecutive reactions (Fig. 1) was monitored by coupling them with GDH as auxiliary enzyme. In a second type of experiment DHAP was an intermediate of the pathway and NADH produced in equimolar amount with diphosphoglycerate, a product of GAPD reaction (Fig. 1) was monitored in the presence of excess Fru-6-P, Mg-ATP, NAD and arsenate as substrates (Fig. 3). For these studies the hemolysates of the isolated RBCs were used, prepared as described in Hollán et al. (1993). The amount of 20 Control PFK Aldolase 10 TPI 0 2 4 6 Time (min) 8 10 F. 2. Fructose-6-phosphate conversion in the consecutive reactions catalysed by PFK/aldolase/TPI in hemolyzed red blood cells from a normal individual (upper panel) and from the Propositus (B. J., Jr.) (lower panel). Packed red blood cells (prepared from the washed isotonic red blood cell preparation by a final centrifugation at 5000 g, 4°C, 20 min) were lysed by diluting them fourfold into 10 mM Tris/HCl buffer, pH 8.0, containing 1 mM EDTA and 5 mM mercaptoethanol, followed by three cycles of freezing in liquid N2 and thawing [c.f. Hollán et al. (1993)]. These lysed cells were used as hemolyzate in 150-fold dilution. Exogenous GDH was added to 0.06 mg ml-1 final concentration and flux was measured by monitoring NADH consumption at 340 nm in the presence of 1 mM MgATP and 25 mM NADH in 100 mM Tris/HCl buffer, pH 8.0 at 25°C. The reaction was started by the addition of 1 mM Fru-6-P. Exogenous enzymes PFK, aldolase or TPI, where indicated, were added separately to the assays at 0.02 mg ml−1. hemolysates (extracts) for the assays was limited by their turbidities. Accordingly, the kinetics were measured with 150-fold diluted hemolysates of the normal and deficient cells, hemoglobin content of which varied between 0.5 and 0.8 mg ml−1. As shown in Fig. 3, in the second type of experiment in which TPI catalyses the physiological DHAP 4 GAP conversion the basic fluxes catalysed by endogenous enzymes were very low. When DHAP was coupled with exogeneous GDH as indicated in the first type of experiment then the flux (NADH consumption) was well-detectable (cf. Fig. 2) and it corresponded to 1.7 mM NADH min−1 (3.1 U g-1 hemoglobin). The data were similar whether the extract of normal or TPI deficient cell was tested. These observations [NADH] (µM) 30 20 Aldolase 10 PFK Control, TPI GAPD 0 2 4 6 Time (min) 8 10 30 [NADH] (µM) Aldolase 20 10 GAPD, PFK 0 2 4 6 Time (min) 8 TPI Control 10 F. 3. Fructose-6-phosphate conversion in the consecutive reactions catalysed by PFK/aldolase/TPI/GAPD in hemolyzed red blood cells from a normal individual (upper panel) and from the Propositus (B. J., Jr.) (lower panel). Hemolyzates prepared as described in Fig. 2 were used at 150-fold dilution in the cuvettes. Flux was measured by monitoring NADH production at 340 nm in the presence of 1 mM MgATP, 4 mM NAD, 10 mM sodium arsenate in 100 mM Tris/HCl buffer, pH 8.0 at 25°C. The reaction was started by the addition of 1 mM Fru-6-P. Exogenous enzymes PFK, aldolase, TPI or GAPD, where indicated were added separately to the assays at 0.02 mg ml−1. indicate that although TPI activity of the deficient cells is only 3% or even lower than the normal RBC, the rate of DHAP formation is not limited by the TPI activity occurring in the deficient cells. To get additional data for the control role of TPI in deficient cells exogeneous TPI was added to the assays and the fluxes of both NADH consumption (GDH coupled reaction) and NADH production (in the presence of NAD and arsenate) were analysed. As shown in Fig. 2, if DHAP was coupled by excess exogeneous GDH (first type of experiment) then TPI caused additional increase in the fluxes in both normal and deficient cell hemolysates. This finding indicates that TPI activity is not in enough excess as compared to the activity of auxiliary enzyme, GDH. When TPI catalysed the DHAP 4 GAP conversion in the reaction sequence (second type of experiment) which is approximately 20-fold lower than the conversion rate of the reverse direction, a quite 443 substantial increase in TPI activity caused a marginal increase in the flux catalysed by deficient cells (Fig. 3). In the normal cells the addition of exogeneous TPI did not alter the basic flux. The observation that in the normal cell TPI virtually does not control glycolysis is in agreement with the expectation. When comparing the data of normal and deficient cells it can be argued that TPI activities around the in vivo level do not appear to limit significantly the hexose and triosephosphate conversion, even in the deficient cells. In additional experiments the concentrations of PFK, aldolase and GAPD of hemolysates were modulated by separate addition of the exogeneous enzymes and the fluxes were analysed in extracts from normal and deficient cells. The data from these studies allowed us to compare the contributions of the enzymes with the control of a segments of glycolysis, where the significant control effect of HK can be disregarded. We compared the measure of the sensitivity of fluxes to the change in the enzyme activity at PFK, aldolase and GAPD catalysed steps. The results of the titrations with excess activities of the enzymes are shown in Figs. 2 and 3. In one of his last papers, Henrik Kacser (Small & Kacser, 1993) developed a method for unbranched chains to estimate the response of metabolic systems using a single large change in enzyme activities. A deviation index, DEJ , (Small & Kacser, 1993) is introduced which gives a measure of the relative change in a flux: DEJ = (DJ/DE)E r/J r where DJ is calculated from the fluxes measured in the absence and presence of exogeneous enzymes; DE is the difference of the activities (aldolase or PFK) of the hemolysates before and after addition of exogeneous enzymes. The ratio of enzyme activity/flux (Er/J r ) was calculated at the ‘‘new point’’, after addition of exogeneous enzymes: 4 U and 0.08 U for PFK and aldolase, respectively. According to the experimental data presented in Fig. 2 and Table 1. in the case of the normal cells, at pH 8.0, DEJ values are 0.85 2 0.1 and 0.14 2 0.05 for aldolase and PFK catalysed reactions, respectively. Since there is a direct relationship between the deviation indices and control coefficients (Small & Kacser, 1993), it can be concluded from our quantitative data that under our experimental conditions aldolase has more significant control on the flux than PFK. A qualitatively similar result was observed in the case of the TPI deficient cells. It has to be added J J that the ratio of Daldolase /DPFK depends extensively on the pH, it decreases from 5.7 to 0.5 by decreasing pH from 8.0 to 7.2. These data suggest that aldolase and PFK beside HK are important control enzymes of the RBC glycolysis and that the control properties of the enzymes extensively depend on the conditions. In order to compare directly the endogenous aldolase and PFK activities of the normal and deficient cells the initial rates of the reactions were measured in the hemolysates at substrate saturations with excess auxiliary enzymes. As shown in Table 1. the Vmax of aldolase is significantly lower than that of PFK in both normal and deficient cells at pH 8.0, that predicts lower capacity for aldolase than for PFK during the glycolysis. Vmax values of TPI reaction measured in normal and deficient hemolysates (cf. Table 1) refer to GAP 4 DHAP conversion from which Vmax values for the reverse direction can be calculated assuming constant equilibrium, Kequ = [DHAP]/[GAP] = 20, for both systems. This value (50–90) for normal cell is still far above the Vmax values of both aldolase and PFK, however, for propositus (1.6) it becomes comparable with that of aldolase which is the slowest enzyme of this segment. Although from the Vmax values of the sequential enzymes must not be directly concluded for the capacities of the enzymes in the sequence, nevertheless, in the light of the Vmax data it is not surprising that the exogeneous TPI could enhance the flux to some extent in deficient cell if the reaction was coupled with GAPD. Why is the DHAP Level so High in the Deficient Cells? A distinctly elevated DHAP level was detected in the erythrocytes of all patients with defective TPI although the activity of the isomerase was varied widely. The concentration of DHAP in erythrocytes of the Hungarian family is also extensively increased and it is extremely high in the two affected brothers (cf. Table 1). The concentration of the GAP is normal and, in addition, that of ATP and 2,3-diphosphate does not differ significantly from that of normal cells (Hollán et al., 1993). Although mathematically oriented, theoretical research has predicted in many cases the metabolic changes caused by changing the activity of a given enzyme in the metabolism of RBC (Schuster & Holzhütter, 1995), considerable discrepancies can be found in the DHAP metabolism. According to the theoretical calculations a few per cent of TPI activity from the normal value should not result in any elevation in DHAP level (cf. Fig. 4). The TPI activity of the members of the Hungarian family are lower than the normal values but different from each other, thus, by determining the in vivo DHAP concentrations in their blood (Hollán et al., 1993), we were able to construct an experimental Metabolite concentration (% normal value) . E T A L . 444 5000 4000 DHAP measured 3000 2000 1000 DHAP calculated 0 0.01 0 ATP 0.1 1 10 TPI Vmax (% normal activity) 100 F. 4. The dependence of stationary DHAP concentrations on the activity (Vmax ) of TPI. TPI activity (in washed red blood cells) and ATP and DHAP levels (in whole blood) were determined according to Hollán et al. (1993). Solid circles represent ATP levels, solid and open squares represent DHAP levels measured in the present study or taken from Hollán et al. (1993), respectively. Solid curves are theoretical curves computed by Schuster et al. (1995). curve of DHAP concentration vs. TPI activity. This curve is compared with the theoretical one computed for a wide range of TPI activity (Schuster & Holzhütter, 1995). As shown in Fig. 4, according to the computation model the extensive reduction of Vmax of TPI (to about 0.1% of the normal value) results in only a two-fold elevation in the DHAP level. In contrast to the theoretical predictions, a 45-fold increase of DHAP concentration was measured at about 3% of the normal TPI activity in the patient. There are other examples that illustrate the discrepancy between DHAP level vs. TPI activity. For example, in the case of a Turkish girl, DHAP concentration is 18-fold normal while the TPI activity was reduced to only 28% of the normal (Eber et al., 1991). The ATP level determined in the RBCs (Hollán et al., 1993) appears to be consistent with the computed data (Schuster & Holzhütter, 1995) and independent of the actual values of TPI activities (cf. Fig. 4). The possible explanations for the discrepancy of DHAP level vs. TPI activity are summarized as follows: (1) The problem in obtaining experimental data for mature erythrocytes in the case of severe enzyme deficiencies originates from the fact that the population of red cells may contain large amounts of reticulocytes which generally have higher enzyme activities as well as higher intermediate concentrations than mature erythrocytes (Piomelli & Seaman, 1993). The ratios of the erythrocytes which are near or beyond the critical threshold of loosing cell integrity 445 and of reticulocytes are different in the normal and the TPI deficient cells. However, the reticulocyte contents of the patient and his compound heterozygote brother were only slightly elevated (3% vs. the range of 0.8–1.0 per cent) (Hollán et al., 1993). (2) The discrepancy for TPI deficiency may also originate from the remarkable instability of almost all abnormal enzyme variants (Tanaka & Zerez, 1990). Unstable proteins may even be more degraded during the experimental procedures and thus the activities measured may not reflect the critical level of activities causing cell damage. (3) Comparing the results of computerized calculations (Schuster & Holzhütter, 1995) with measured metabolite concentrations (cf. Fig. 4), discrepancies may originate from differences between kinetic parameters determined in normal and deficient cells. In fact, the KM of DHAP to the mutant TPI occurring in deficient cells is higher than that of the normal, while the KM of GAP is the same (Hollán et al., 1993). The velocities of the DHAP 4 GAP conversion catalysed by TPI in normal and deficient cells can be calculated according to the Michaelis–Menten equation: levels and TPI activities may be due to the fact that a number of yet unknown structural kinetic parameters are not taken into consideration. One of these parameters is the specific association of glycolytic enzymes to the N-terminus of band-3 membrane protein under physiological conditions (Harrison et al., 1991; Jenkins et al., 1985; Low et al., 1993; Rogalski et al., 1989; Tsai et al., 1982). There are data that a glycolytic enzyme complex from TPI to pyruvate kinase is bound in vivo to the cytoplasmic domain of band 3 (Fossel & Solomon, 1978). Due to these specific associations some glycolytic enzymes are inactivated, only the unbound enzymes exhibit catalytic activities (Low et al., 1993). The binding of the enzymes is reversible. Therefore, it seems to be a plausible explanation for the discrepancy of TPI activity and DHAP level that under in vivo conditions the TPI activity in the deficient cells is further reduced due to the binding of the isomerase to band 3 in the red cell membrane or to other cytoplasmic enzymes. Thus a decrease of TPI activity of deficient cells could easily reach the limit value which is not able to ensure the rapid equilibrium of the triosephosphates and results in the enormous accumulation of DHAP. norm def v norm Vmax [DHAP]norm([DHAP]def + KM ) def norm def = def norm v Vmax [DHAP] ([DHAP] + KM ) TPI Deficiency and Enzyme Compartmentation The KM values are 1.5 mM for normal and 2.8 mM and 3.0 mM for deficient TPIs from the two affected brothers (Hollán et al., 1993). [DHAP] for normal and deficient cells are given in Table 1. Vmax values of the DHAP 4 GAP conversion for normal and deficient TPIs were calculated from data presented in Table 1 using the Halden relationship assuming identical equilibrium constant for DHAP/GAP conversion catalysed by normal or mutant TPIs. The ratios of the velocities of the normal and mutant TPI catalysed reactions are 1.0 and 1.1 for B.J. Jr. and A.J., respectively. The fact that these ratios correspond to the unity suggests that in deficient cells the reduction of Vmax and increase of KM are compensated by the elevation of DHAP concentration; thus TPI may not limit the endogenous flux. (4) In general, it is postulated that the steady-state metabolite level is adjusted by its production/ conversion. DHAP is not an inert metabolite in cells which are active in lipid synthesis, since it is an essential precursor of ether lipids. However, there is no lipid synthesis in mature red blood cells. In fact, in the hemolysates we were not able to detect GDH activity, which would be responsible for the DHAP conversion to lipid synthesis (data not shown). (5) Additional reason for discrepancies between the measured and the theoretically postulated DHAP It is a widely discussed issue that the low TPI activity in deficient cells leads to a metabolic block in the glycolytic pathway that results in an increased concentration of DHAP in the erythrocytes. Nevertheless, the relationship between high DHAP levels and increased hemolysis is unclear, since accumulation of this compound occurs in cases of diphosphoglycerate mutase deficiency without hemolysis (Rosa et al., 1978). Also, there are no indications that DHAP may inhibit regulatory enzymes by its increased concentration (Eber et al., 1991). The main objective of this study was to assess the severity of cellular dysfunction associated with TPI defect. Since there is no reliable model which describes the relation between TPI activity and DHAP level characteristic for deficient cells we propose that the microcompartmentation of TPI, which may or may not be different in normal and TPI deficient cells, could be responsible for the altered metabolism in the deficient RBCs. Different binding affinity of normal and mutant isomerase molecules to the red cell membranes may originate from differences in the tertiary structure of the mutant enzyme as well as from changes in membrane fluidity (Hollán et al., 1995). Direct binding studies on this issue are in progress in our laboratory. Concerning the physiological relevance of the computerized models for the RBC . E T A L . 446 metabolism we agree with the argument of Beutler (1980) that ‘‘the usefulness of the models has been limited by the fact that all the in vivo interactions are still not entirely understood’’. In fact he referred to interactions of enzymes with metabolites, allosteric ligands etc. Now, in the light of recent data the importance of the macromolecular interactions has to be underlined. These regulatory mechanisms are probably different in normal and deficient cells. This work was supported by grants from the Hungarian National Science Foundation, OTKA, T-5412, T-6349 and T-17830 to J.O and F 017392 to B. G. V. We thank Emma Hlavanda for her expert assistance. REFERENCES A, F. I., V, V. M., Z, A. M., P, A. V., P, O. V., K, B. N. & E, L. I. (1981). The regulation of glycolysis in human erythrocytes. The dependence of the glycolytic flux on the ATP concentration. Eru. J. Biochem. 115, 359–365. B, E. (1980). A commentary. Blood Cells. 6, 827–829. B, E., B, K. G., K, J. C., L̈, G. W., R, B. & V, W. N. (1977). International Committee for Standardization in Haematology: recommended methods for red-cell enzyme analysis. Br. J. Haematol. 35, 331–340. B́, L. & C, C. (1984). Is phosphofructokinase the rate-limiting step of glycolysis? Trends Biochem. Sci. 9, 372–373. B, K. M., C, I. D. & S, R. J. (1982). A 1H n.m.r. study of the kinetic properties expressed by glyceraldehyde phosphate dehydrogenase in the intact human erythrocyte. Biochem. J. 208, 583–592. C, D. & K, H. (1993). Aldolase-tubulin interactions: removal of tubulin C-terminals impairs interactions. Biochem. Biophys. Res. Commun. 195, 289–293. C, M.-L., A, P. J., W, X., H́, S., L A. & M, L. E. (1993). Human triosephosphate isomerase deficiency resulting from mutation of phe-240. Am. J. Hum. Genet. 52, 1260–1269. E, S. W., P, A., B, A., G, M., K, W. K. G., K̈, J., M, R. & S̈, W. (1991). Triosephosphate isomerase deficiency: haemolytic anaemia, myopathy with altered mitochondria and mental retardation due to a new variant with accelerated enzyme catabolism and diminished specific activity. Eur. J. Pediatr. 150, 761–766. F, D. A. (1984). Phosphofructokinase and glycolytic flux. Trends Biochem. Sci. 9, 515–516. F, E. T. & S, K. (1978). Ouabain-sensitive interaction between human red cell membrane and glycolytic enzyme complex in cytosol. Biochim. Biophys. Acta. 510, 99–111. F, H., M, S. (1990) Recent progress in the molecular genetic analysis of erythro-enzymopathy. Am. J. Hematol. 34, 301–310. H, S. R., P, D. E., J, E. R., V, W. & K, R. L. (1970). Triosephosphate isomerase deficiency in an adult. Clin. Res. 18, 529–535. H, M. L., R, R. A, P., G, R. L. & L, P. S. (1991). Role of band 3 tyrosine phosphorylation in the regulation of erythrocyte glycolysis. J. Biol. Chem. 266, 4106–4111. H, R., R, S. M. & R, T. A. (1977). Metabolic regulation and mathematical models. Prog. Biophys. Mol. Biol. 32, 1–82. H, R. & R, T. A. (1974). A linear steady-state treatment of enzymatic chains. General properties, control and effector strength. Eur. J. Biochem. 42, 89–95. H, H.-G. & V S, E. (1982). Review article: fructose 2,6-bisphosphate 2 years after its discovery. Biochem. J. 206, 1–12. H, T., R, C. S. & U, K. (1979). The interaction of phosphofructokinase with erythrocyte membrane. J. Biol. Chem. 254, 9542–9550. H́, S., F, H., H, A., H, K., K, H., M, S., H, V., G, E. & I-K, M. (1993). Hereditary triosephosphate isomerase (TPI) deficiency: two severely affected brothers one with and one without neurological symptoms. Hum. Genet. 92, 486–490. H́, S., D, I., Ś, L., H́, M., Ḿ, M., H́, V. & F, T. (1995). Erythrocyte lipids in triose-phosphate isomerase deficiency. PNAS 92, 268–271. I, C., B, Y., C U. & D, H. (1993). Selective inhibition of Plasmodium falciparum aldolase by a tubulin derived peptide and identification of the binding site. Mol. Biochem. Parasitol. 58, 135–143. J, J. D., K, F. J. & S, T. L. (1985). Mode of interactions of phosphofructokinasae with the erythrocyte membrane. J. Biol. Chem. 260, 10426–10433. K, H. & B, J. A. (1973). The control of flux. In: Rate Control of Biological Processes (Davies, D. D. ed), pp. 65–104. Cambridge: Cambridge University Press. K, N. S. & U, K. (1977). Changes in allosteric properties of phosphofructokinase bound to erythrocyte membranes. J. Biol. Chem. 252, 7418–7420. K, T. & O, J. (1988). Control mechanism by dynamic macromolecular interactions. Curr. Top. Cell. Regul. 29, 1–33. K, H. R. & W, J. L. (1992). Association of Glycolytic Enzymes with the Cytoskeleton. Curr. Top. Cell. Regul. 33, 15–30. L, E. & P, G. A. (1990). Crystallographic analysis of the complex between triophosphate isomerase and 2- phosphoglycolate at 2.5 A resolution: implications for catalysis. Biochemistry. 29, 6619–6625. L, P. S., R, P. & H, M. L. (1993). Regulation of glycolysis via reversible enzyme binding to the membrane protein, Band 3. J. Biol. Chem. 268, 14627–14631. Ḿ-H, E., S, J. M. & Ṕ, J. A. (1984). Studies on glycolysis in vitro: role of glucose phosphorylation and phosphofructokinase activity on total velocity. Int. J. Biochem. 16, 476–496. N, E. B. & K, J. R. (1988). Triosephosphate isomerase: energetics of the reaction catalysed by the yeast enzyme expressed in Escherichia coli. Biochemistry. 27, 5939–5947. Ó, J. (1995). Cell architecture and Metabolic Channeling. Heidelberg: Springer-Verlag. P, S. & S, C. (1993). Mechanism of red blood cell aging: Relationship of cell density and cell age. Am. J. Hematol. 42, 46–52. R, T. A., H, R., J, G. & R, S. (1974). A linear steady-state treatment of enzymatic chains. A mathematical model of glycolysis of human erythrocytes. Eur. J. Biochem. 42, 107–120. R, A. A., S, T. L. & W, A. (1989). Association of glyceraldehyde-3-phosphate dehydrogenase with the plasma membrane of the intact human red blood cell. J. Biol. Chem. 264, 6438–6446. R, R., P, M-O. & B, Y. (1978). The first case of a complete deficiency of diphosphoglycerate mutase in human erythrocytes. J. Clin. Invest. 62, 907–915. R, I. A., F, W. J. & W, J. V. B. (1990). Proton diffusion in the active site of triosephosphate isomerase. Biochemistry. 29, 4312–4317. S, M., H, R. & R, S. M. (1981). Mathematische Modellierung der Glykolyse und des Adeninnukleotidstoffwechsels menschlicher Erythrozyten II. Acta Biol. Med. Germ. 40, 1683–1697. S, R. & Ḧ, H.-G. (1995). Use of mathematical models for predicting the metabolic effect of large-scale enzyme activity alterations. Application to enzyme deficiences of red blood cells. Eur. J. Biochem. 229, 403–418. S, J. R. & K, H. (1993). Responses of metabolic systems to large changes in enzyme activities and effectors. 1. The linear treatment of unbranched chains. Eur. J. Biochem. 213, 613–624. T, K. R. & Z, C. R. (1990). Red cell enzymopathies of glycolytic pathway. Sem. Hematol. 27, 165–185. T, I., M, S. N. P. & S, T. L. (1982). Effect of red cell membrane binding on the catalytic activity of glyceraldehyde3-phosphate dehydrogenase. J. Biol. Chem. 257, 1438–1442. U, T. (1978). The role of isozymes in metabolism: A model of metabolic pathways as the basis for the biological role of isozymes. Curr. Top. Cell. Reg. 13, 233–251. U, T. (1991). The role of isoenzymes in metabolite channeling. J. theor. Biol. 152, 81–84. 447 V, W. N. & P, D. E. (1984). Erythrocyte enzymopathies, hemolytic anemia, and multisystem disease: an annotated review. Blood. 64, 583–591. V́, B. G., Ḱ, J. & Ó, J. (1996). Specific characteristics of phosphofructokinase-microtubule interaction. FEBS Lett. 379, 191–195. V́, B. G. & S, T. L. (1989). Elasticity of the human red cell membrane skeleton. Effects of temperature and denaturants. Biophys. J. 55, 255–262. V, K. W. & K, H. R. (1993). Glycolytic enzyme-tubulin interactions: role of tubulin carboxy terminals. J. Mol. Recognit. 6, 167–177. Y, M. & M, K. (1985). AMP deaminase reaction as a control system of glycolysis in yeast. J. Biol. Chem. 260, 4729–4732.