Why are there so many different types
of Annuloplasty Rings?
Feroze Mahmood, MD.
Director Vascular Anesthesia &
Perioperative Echocardiography
Associate Professor of Anaesthesia & Critical Care
Harvard Medical School
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Why it is important for us to know ?
Mitral valve repair is a frequently performed operation
Pre-CPB Intraoperative TEE interrogation of mitral valve critical to repair planning
A repair is termed successful ONLY if Post-CPB TEE examination is satisfactory
“Signature” appearance of annuloplasty rings
Characteristic flow patterns
? Durability of repair
Road Map for Repair
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Presentation Outline
Why repair in the first place ?
Principles of valve reconstruction surgery
Rationale for annuloplasty ring selection
Pros and Cons of Annuloplasty rings
Assessment of a repaired mitral valve
Short-term to long-term success
Beth Israel Deaconess
Medical Center
Harvard
Medical
School
R
Why Repair ?
Beth Israel Deaconess
Medical Center
R
Harvard
Medical
School
Historical Background
Miles “Lowell” Edwards and Albert Starr
Edwards - Two bouts of
Rheumatic Fever
Presented before the American Surgical Association, Boca Raton Florida March 21-23 1961
Wanted to mechanize the
whole heart
Encouraged to design a heart
valve
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Issues with Prosthetic Valves
0.000
Outer Diameter
EOA
0.000
Rigid for flexible annulus
Flat for non-planar annulus
Circular rings for elliptical annulus
Outer diameter vs. EOA
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Replacement to Repair
Heralded by the development of
Cardiopulmonary bypass
Diseased valves were directly
visualized
Collaboration between surgeons and
engineers to develop prosthetic valves
Comprehensive valve analysis
? Replacement of valves
First CPB Machine
Dr. Alain Carpentier
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Anatomical - Functional Classification
Moves normally
Beth Israel Deaconess
Medical Center
R
Moves too much
Moves too little
Harvard
Medical
School
Principles of
Valve Repair
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Principles of Reconstructive Surgery
Principles of Reconstructive Surgery
in Degenerative
Mitral Valve Disease
in Degenerative Mitral Valve Disease
†
Farzan Filsoufi,Farzan
MD,*
and MD,*
AlainandCarpentier,
MD,
Filsoufi,
Alain Carpentier,
MD,PhD
PhD†
Degenerative mitral valve disease is the most common cause of mitral regurgitation (MR)
Degenerative mitral
valve
disease
is the
mostetiologies
common
cause
of mitralareregurgitation
(MR)
in developed
countries.
The most
common
of valvular
regurgitation
Barlow’s
disease and fibroelastic
Theetiologies
mechanism of
is type IIregurgitation
dysfunction (leaflet
in developed countries.
The mostdeficiency.
common
ofMR
valvular
are Barlow’s
prolapse) due to chordae elongation or rupture in most patients. Associated annular
disease and fibroelastic
deficiency. The mechanism of MR is type II dysfunction (leaflet
dilation is a common lesion in almost all patients with chronic MR. By means of segmental
prolapse) due valve
to analysis,
chordae
elongation
or prolapse
rupture(P2insegment)
mostis patients.
Associated
annular
isolated
posterior leaflet
often observed
in patients
with fibroelastic
deficiency,
whereas
the prolapsewith
of multiple
segments
bileaflet
prolapse
dilation is a common
lesion
in almost
all patients
chronic
MR.or By
means
of segmental
typically seen in patients with Barlow’s disease. In patients with degenerative mitral
valve analysis,is
isolated
posterior leaflet prolapse (P2 segment) is often observed in patients
valve disease and severe MR, reconstructive surgery should be performed before the
with fibroelastic
deficiency,
whereas
theatrial
prolapse
of pulmonary
multiplehypertension,
segments and
or bileaflet
occurrence
of clinical
symptoms,
fibrillation,
left ven- prolapse
tricular
enlargement.
The goals
of reconstructive
surgerywith
are preservation
or
is typically seen
in dysfunction
patients orwith
Barlow’s
disease.
In patients
degenerative
mitral
restoration of normal leaflet motion, creation of a large surface of coaptation, and stabilivalve disease zation
and ofsevere
MR,
reconstructive
surgery
should
be
performed
the entire annulus with a remodeling annuloplasty. Today, reconstructive tech- before the
are symptoms,
standardized, reliable,
and reproducible,
and therefore
should be applied
occurrence of niques
clinical
atrial fibrillation,
pulmonary
hypertension,
and left vensystematically to all patients with degenerative valvular disease.
tricular dysfunction
or enlargement. The goals of reconstructive surgery are preservation or
Semin Thorac Cardiovasc Surg 19:103-110. © 2007 Published by Elsevier Inc.
restoration of normal leaflet motion, creation of a large surface of coaptation, and stabiliKEYWORDSannulus
degenerative
mitral
disease, mitral
regurgitation, Carpentier’s
reconstruczation of the entire
with
a valve
remodeling
annuloplasty.
Today, reconstructive
techtive techniques
niques are standardized,
reliable, and reproducible, and therefore should be applied
systematically to all patients with degenerative valvular disease.
Semin
Thoracmitral
Cardiovasc
Surg
19:103-110.
Published
by Elsevier
Inc.surgical techniques
egenerative
valve disease
is the
most common © 2007
etiology,
whereas treatment
strategy and
D
cause of mitral regurgitation (MR) in developed coun-
depend on valve dysfunctions and lesions, respectively.
tries. Several
confusing terminologies
myxomatous
valvemitral Carpentier’s
functional
classification isreconstrucused to describe
KEYWORDS
degenerative
mitral(eg,
valve
disease,
regurgitation,
Carpentier’s
disease, mitral valve prolapse, floppy valve, flail leaflet) have
the mechanism of mitral regurgitation (Fig. 1).1 This classifitive
techniques
Beth Israel Deaconess
Medical Center
R
been used in the literature to describe degenerative mitral
valve disease. The understanding of valve pathology is facilitated by the use of the “pathophysiological triad.”1
D
egenerative mitral valve disease is the most common
Pathophysiology and
cause of mitral regurgitation (MR) in developed counFunctional Classification
tries. Several confusing terminologies (eg, myxomatous valve
The pathophysiologic triad is composed of etiology (cause of
disease, mitral valvetheprolapse,
floppy
flailfrom
leaflet)
haveand
disease), valve
lesionsvalve,
(resulting
the disease),
valve dysfunction
(resulting from
the lesion).1 These
distincbeen used in the literature
to describe
degenerative
mitral
tions
are relevant because
long-term
prognosisisdepends
valve disease. The understanding
of valve
pathology
facil- on
1
itated by the use of the “pathophysiological triad.”
cation is based on the opening and closing motions of the
mitral leaflets. Patients with type I dysfunction have normal
leaflet motion. Mitral regurgitation in these patients is due to
annular dilation or leaflet perforation. There is an increased
etiology,
whereas
treatment
and
techniques
leaflet motion
in patients
with type IIstrategy
dysfunction,
withsurgical
the
free edge on
of the
leafletdysfunctions
overriding the plane
the annulus
depend
valve
andoflesions,
respectively.
during systole (leaflet prolapse). The most common lesions
Carpentier’s
functional
classification
is
used
to
describe
responsible for type II dysfunction are chordae elongation or
the
mechanism
mitral
regurgitation
rupture
and papillaryof
muscle
elongation
or rupture. (Fig.
Patients1).1 This classifiwith type
dysfunction
have
a restrictedand
leaflet
motion motions of the
cation
is IIIa
based
on the
opening
closing
during both diastole and systole. The most common lesions
mitral
leaflets.
Patients
withchordae
type thickening
I dysfunction
have normal
are leaflet
thickening
and retraction,
and
shortening
or fusion,
and commissural
fusion.in
MRthese
is most
leaflet
motion.
Mitral
regurgitation
patients is due to
often associated with some degrees of mitral stenosis. The
annular
dilation
or
leaflet
perforation.
There
is
an
increased
mechanism of MR in type IIIb dysfunction is restricted leaflet
leaflet
motion
in patients
with
type II with
dysfunction,
with the
motion during
systole.
Left ventricular
enlargement
apical papillary
muscle
causes this type
valve of the annulus
free
edge of
the displacement
leaflet overriding
the ofplane
dysfunction.
during
systole
(leaflet
prolapse).
The
most
common
lesions
The functional classification is further refined by the intro-
Harvard
Medical
School
Principles of Valve Repair
*Department of Cardiothoracic Surgery, Mount Sinai School of Medicine,
New York, New York.
†Hospital European Georges-Pompidou, Paris, France.
Pathophysiology
and
Address reprint requests
to Farzan Filsoufi, MD, Associate Professor, Associate Chief Cardiac Surgery, Department of Cardiothoracic Surgery,
Mount Sinai Hospital, 1190 Fifth Avenue, Box 1028, New York, NY
Functional Classification
10029-1028. E-mail: farzan.filsoufi@mountsinai.org
The pathophysiologic triad is composed of etiology (cause of
1043-0679/07/$-see
front matter
© 2007the
Published
by Elsevier and
Inc.
the disease), valve lesions
(resulting
from
disease),
doi:10.1053/j.semtcvs.2007.04.003
valve dysfunction (resulting from the lesion).1 These distinctions are relevant because long-term prognosis depends on
responsible for type II dysfunction are chordae elongation or
rupture and papillary muscle elongation or103rupture. Patients
with type IIIa dysfunction have a restricted leaflet motion
during both diastole and systole. The most common lesions
are leaflet thickening and retraction, chordae thickening and
shortening or fusion, and commissural fusion. MR is most
often associated with some degrees of mitral stenosis. The
mechanism of MR in type IIIb dysfunction is restricted leaflet
motion during systole. Left ventricular enlargement with apical papillary muscle displacement causes this type of valve
dysfunction.
The functional classification is further refined by the intro-
Preservation/Restoration of Normal Motion
*Department of Cardiothoracic Surgery, Mount Sinai School of Medicine,
New York, New York.
†Hospital European Georges-Pompidou, Paris, France.
Address reprint requests to Farzan Filsoufi, MD, Associate Professor, Associate Chief Cardiac Surgery, Department of Cardiothoracic Surgery,
Mount Sinai Hospital, 1190 Fifth Avenue, Box 1028, New York, NY
10029-1028. E-mail: farzan.filsoufi@mountsinai.org
Create a Large Area for Coaptation
Annulus stabilization with a ring
1043-0679/07/$-see front matter © 2007 Published by Elsevier Inc.
doi:10.1053/j.semtcvs.2007.04.003
103
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Mitral Annular Shape and Dimensions
Normal
Chronic MR
AP-AL/PM
Diameter
Ratio
Reversed
3:4
Beth Israel Deaconess
Medical Center
R
4:3
Harvard
Medical
School
Why Annuloplasty ?
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Why Perform an Annuloplasty ?
Principles of Mitral Valve Repair
Equal Apposition of the Posterior and Anterior Leaflet
Reduced Height of Posterior Leaflet
Stabilization of the Anterior Leaflet
Remodeling Annuloplasty
Mastery of Cardiothoracic Surgery: In “Mitral Valve Repair” by Lawrence H Cohn. Editors: Larry R.
Kaiser, Irwing L. Kron, Thomas L. Spray. Second Edition 2007. Lippincott Williams and Wilkins.
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Rationale for
Ring
Selection
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Complete Rings
Complete circle of ‘support’ around the mitral annulus
Classic Carpentier Ring
Duran Flexible Complete Ring
Completely RIGID - Sized to Anterior Leaflet
Completely FLEXIBLE - Less Distortion
Beth Israel Deaconess
Medical Center
R
Harvard
Medical
School
Rigid versus Flexible Debate
Which one is better ?
Rigid or Flexible
Chang BC MD et al. Long-term clinical results of mitral valvuloplasty using
flexible and rigid rings: A prospective randomized study. J Thorac Cardiovasc
Surg 2007;133:995-1003
Chee T et al. Is a flexible mitral annuloplasty ring superior to semi-rigid or rigid in terms
of improvement in symptoms and survival. Interact Cardiovascular and Thoracic Surgery
7 (2008) 477-484
Flexible Annuloplasty Rings
Fixation of mitral annulus impairs LV function
Flexible rings result in better LV systolic function
Improved LV Systolic Function
LV function improved up to 6 months after implantation
Greater likelihood of recurrence of MR after flexible rings
Does not translate into improved clinical outcome
Inability to completely remodel the annulus due to flexibility
for degenerative disease
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Evolution of Ring Annuloplasty
Carpentier Physio Ring
Collvin-Galloway Future Ring -Medtronics
Rigid Anteriorly - Flexible Posteriorly
Rigid Posteriorly - Flexible Anteriorly
3:4 Ratio - Systole 4:4 Ratio - Diastole
Posterior flexibility allows
physiological motion
Saddle shaped anteriorly
Increased antero-posterior diameter
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Mitral Valve Function
Systolic Competence & Diastolic Non-Restriction
Sphincteric Action
Diastole
Cyclical
Antero-Posterior Diameter
Systole
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Effects of Annuloplasty on Mitral Valve
Prevention
of
Regurgitation
AIMS
Prevention
of Annular
Dilatation
EFFECT
Mitral annulus “FIXED” in the END-SYSTOLIC Phase
Beth Israel Deaconess
Medical Center
R
Harvard
Medical
School
Rationale for Annuloplasty Ring
Selection
When only annular
remodeling is required
When annular dilatation
has to be prevented
Flexible
Ring
Rigid Ring
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Partial Rings or Bands
Cosgrove-Edwards Annuloplasty Band
Cosgrove DM et al. Initial Experience with Cosgrove Edwards
Annuloplasty System. Ann Thorac Surg 1995;60:499-504
C-Shaped and flexible
Conforms to annular shape
St. Jude Medical CG Future Band
CosgrovePartial Band
Medtronics
Edwards Band
Not so good for prevention of annular
dilatation
Supports only the posterior annulus
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Pros and Cons of
Annuloplasty Rings
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Recap
Rigid Rings
- Predictable prevention of annular dilatation but affect left ventricular
function
Flexible Rings - Preserve left ventricular function but less predictable in prevention of
annular dilatation
Flexible & Rigid - Conform to annular dynamics (? Anterior vs. Posterior)
Bands - Likely to cause less geometric distortion but less likely to prevent annular dilatation
RIGID, FLAT & Fixed in END-SYSTOLIC position
Beth Israel Deaconess
Medical Center
R
Harvard
Medical
School
Is it all about annular area
reduction ?
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Saddle Shape and Stress Reduction
Patent
Alexander L. Liepa is credited with the invention of the saddle-shaped Pringles
chip, filing for a patent on August 2, 1974. U.S. Patent number 3998975 was
issued on December 21, 1976.
Shape and Packaging
Unique features are the saddle shape of he stackable chips and the “tennis ball
cannister” packaging, both of which were designed to minimize chip breakage.
The machine used to make Pringles chips was partly designed by science fiction and fantasy author Gene Wolfe
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Assessment of Mitral Annular Non-Planarity
1
Annular Height
3
Commissural Width
AHm
Zmin
2
4
Annular Height : Commissural Width Ratio
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Final Question
Why there are so many
annuloplasty rings?
Beth Israel Deaconess
Medical Center
R
Harvard
Medical
School
Assessment of a Repaired
Mitral Valve
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
ImmediatePost Repair Assessment
Structural Integrity -2D
Functional Integrity - Doppler
Stability
Color flow
Leaflet motion Flow dependent
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Intraoperative Assessment of Mitral Valve Area After Mitral Valve Repair:
Comparison of Different Methods
Andrew Maslow, MD,* Anthony Gemignani, MD,* Arun Singh, MD,* Feroze Mahmood, MD,† and
Athena Poppas, MD, FACC*
Objective: In the present study, 3 different methods to
measure the mitral valve area (MVA) after mitral valve repair
(MVRep) were studied. Data obtained immediately after repair were compared with postoperative data. The objective
was to determine the feasibility and correlation between
intraoperative and postoperative MVA data.
Design: A prospective study.
Setting: A tertiary care medical center.
Participants: Twenty-five elective adult surgical patients
scheduled for MVRep.
Methods: Echocardiographic data included MVAs obtained using the pressure half-time (PHT), 2-dimensional
planimetry (2D-PLAN), and the continuity equation (CE).
These data were obtained immediately after cardiopulmonary bypass and were compared with data obtained before
hospital discharge (transthoracic echocardiogram 1) and 6
to 12 months after surgery (transthoracic echocardiogram
A
CCURATE INTRAOPERATIVE ASSESSMENT of the
2). Intraoperative care was guided by hemodynamic goals
designed to optimize cardiac function.
Results: The data show good agreement and correlation
between MVA obtained with PHT and 2D-PLAN within and
between each time period. MVA data obtained with the CE
in the postoperative period were lower than and did not
correlate or agree as well with other MVA data.
Conclusion: The MVA recorded immediately after valve
repair, using PHT, correlated and agreed with MVA data
obtained in the postoperative period. These results contrast
with previously published data and could highlight the impact of hemodynamic function during the assessment of
MVA.
© 2011 Elsevier Inc. All rights reserved.
KEY WORDS: pressure half-time, planimetry, mitral valve
area, echocardiography, mitral valve repair
cardiopulmonary bypass (CPB) hemodynamic management was per-
Intraoperative
PHTafterand
2Dforplanimetry
- Good
correlation
with
postoperative
assessment
formed
according to divisional
protocol
to achieve the following
premitral valve (MV)
repair
mitral regurgitation
R
specified goals: mean systemic blood pressure between 60 and 90
(MR) is important to determine the success of the repair and
mmHg, central venous pressure !15 mmHg, pulmonary artery preswhether or not rerepair is necessary. Inherent in the repair of
sures within 25% (!) of pre-CPB values, and a cardiac index "2.5
the MV is an immediate reduction in the mitral valve area
L/min/m2. The heart rate was maintained between 80 and 100 beats/
Beth Israel
Deaconess
1-3 A further reduction in the MVA is possible during
(MVA).
Medical Center
min. Immediately after CPB, all patients were in an atrioventricular
3-6
follow-up, with significant stenosis being reported as early as
(AV) sequential rhythm (either sinus rhythm or a paced rhythm [DDD
1 year after surgery.6 Intraoperative assessment of MV patency
or DOO]) with an AV interval of !180 milliseconds.
should be a part of the routine assessment after repair.
After separation from CPB and before chest closure, a comprehenSeveral studies have used pressure half-time (PHT) and
sive transesophageal echocardiographic examination (TEE) was per1-5,7-9
2-dimensional planimetry (2D-PLAN)
to assess postoperformed by experienced echocardiographers. The assessment of the MV
ative MVA during long-term follow-up; however, only 1 has
was performed
in a similarAnnular
fashion as described for the assessment
1
1 of
Mitral Annular
Correlation
Between
7 In thisNonplanarity:
12
study, the intranativethe
valve
stenosis11 and prosthetic
2studied intraoperative measurements.
Height/Commissural Width Ratio and
Nonplanarity
Angle valves. Measurements2 and
3operative MVA by PHT underestimated that measured during
3 the
calculations of the MVA were obtained using 2D-PLAN, PHT, and
4follow-up
AQ:1,2 and
Haider
J. Warraich,
MD,* Bilal
Chaudary,*
MD,† Peterequation
J. Panzica,
MD,*
Jacob Pugsley,
MD,* using the4short
would
have resulted
in redo
surgeryAndrew
in 14%Maslow,
of
continuity
(CE).
Planimetry
was performed
5
5
7 Without a defined reference method to measure
and Feroze
Mahmood,
axis MD*
en face transgastric view from the narrowest mitral orifice. From
cases.
MVA
6
6
this view, the leaflet edges were identified and circumferentially traced
echocardiographers
have relied on transvalvular quired
7after repair, Objective:
7
To compare 2 methods of mitral annular nonduring 3-dimensional transesophageal echocardiog7 A previous case of
withwere
the leaflets
at to
maximal
8pressure gradients
8
assess
valve patency.
planarity:tothe
mathematically
calculated
annular height to
raphy
exported
Matlabexcursion.
software (MathWorks,
9post-repair commissural
the echocardiographic
examination,
theThe
CE was used, 9using
width ratioissues
(AHCWR)
the echocardioMA), which
was used to calculate
the AHCWR.
stenosis highlighted
withand
transvalvular
gra- Natick,During
10
10
graphically
derived
nonplanarity
angle.
nonplanarity
angle
was
seen
to
correlate
favorably
with
the
the
left
ventricular
outflow
tract
(LVOT)
as
a
reference
site,
to
calculate
dients.10 In this
case,
measures of MVA suggested significant AHCWR (r ! 0.70).
Design:
Prospective.
11
11
the MVA with the following equations: MVA " 0.785 (DiamLVIT #
stenosis, whereas
Doppler-derived
gradients
did not.10 Direct
Setting:
Tertiary care university
hospital.
Conclusions: A favorable correlation was found between
12
12
time velocity integral the )/TVI
MV.This suggests that
Interventions:were
Three-dimensional
transesophageal
echoAHCWR.
13
13
pressure measurements
elevated, which
is consistent
with the nonplanarity angle andLVOT
cardiography.
the nonplanarity
angle can be long-axis
used to assess
annulardiameter was
In the midesophageal
view,mitral
the LVOT
14
14mea10
mitral stenosis,
prompting
rerepair.
Participants: Patients undergoing mitral valve surgery.
nonplanarity
in a the
clinically
fashion.
sured from
innerfeasible
edge at
the level of the aortic valve 15leaflet
15
Measurements and Main Results: Using 3-dimensional
© 2011 Published
by Elsevier Inc.
11,12 In the deep transgastric view, the pulse wave16(PW)
16 The purpose of this investigation was to compare measures
insertion.
echocardiography, volumetric datasets
of the MVAtransesophageal
obtained
intraoperatively
immediately
after
repair
17
17 obDoppler measure of the LVOT time velocity integral (TVI) was
were acquired from 22 patients undergoing mitral valve
18
18
to those obtained
early
and late nonplanarity
after surgery.
surgery. The
intraoperative
angleThe
was authors
calcuKEYtained
WORDS:
valve,location.
3-dimensional
transesophageal
frommitral
this same
In 1 patient,
who underwent aortic valve
19
19
Assessment
nonplanarity angle, mitral valve repair,
hypothesizelated
thatwith
the Mitral
MVAValve
of the
repairedsoftware
valve, (Tomtec
assessed echocardiography,
replacement,
the
main
pulmonary
artery
was
used
as
the
reference
20
20 site
GmbH, Munich, Germany). Furthermore, the datasets acmitral regurgitation
intraoperatively, correlates and agrees with that measured durbecause the LVOT could not be well visualized and a diameter was
21
21 not
ing postoperative
22
22
HE examinations.
NATURAL NONPLANAR SADDLE SHAPE of the
similar geometric phenomenon, a favorable correlation would
T
R
Harvard
Medical
School
Non-Planarity Angle
AH
23
23
exist between the AHCWR and the nonplanarity angle.
mitral annulus optimizes leaflet stress.1-3 The appreciation
24
24
of this unique nonplanar geometry in a clinically practical
From the *Warren Alpert School of Medicine, Brown Medical
METHODS
25
25
fashion could haveMETHODS
important implications because the modern
School, Rhode Island Hospital, Providence, RI; and †Department of
26
26
saddle-shaped annuloplasty rings are used to restore the physThis study was conducted in patients undergoing elective
PH
Anesthesiology, HarvardNPA
Medical School, Beth Israel Deaconess
from the Internal Research Board, informed consent
27 After approval
27Mediologic shape of the mitral annulus and thus optimize repair
cardiac surgery and perioperative
3D TEE at the authors’
ical Center,
was obtaineddurability.
from 253consecutive
cardiac surgical
patients
aged this
45 to institution.
28
28
The ready availability
of a technique
to assess
These Boston,
data wereMA.
collected as part of a prospective
Address
reprint
requests
to
Andrew
Maslow,
MD,
63
Prince
Street,
90 years scheduled
for
MV
repair.
All
patients
had
severe
mitral
29
29
effect accurately can affect surgical decision making.
protocol, approved by the institutional review board, in which
30
30
Needham,
MA 02492.
E-mail:
amaslow@rcn.com
regurgitation without
evidence
of annular
mitral stenosis
before
Traditionally,
mitral
nonplanarity
has surgery.
been quanti-Zmax
patients
undergoing
mitral valve
surgery
and intraoperative
31 Intraoperative
31
fied as
the ratio of thedata
mitral
annular
height from
to the invasive
commissural
underwent
3D analysis.
A waiver of
© 2011 Elsevier
Inc.off-line
All rights
reserved.
hemodynamic
were
obtained
arte- TEE examination
32
32
theof
application
of this
off-line
F1 width (AHCWR;
Fig 1).4 During
informed
consent was obtained. Patients presenting from Au1053-0770/2502-0004$36.00/0
rial and pulmonary
artery catheters.
The use
vasoactive
medications
33
33
data points
derived initially
from the fluoroto September 2010 were included in the analysis.
doi:10.1053/j.jvca.2010.11.022
was left to technique,
the discretion
of theareattending
anesthesiologist.
Post– gust 2008
34
34
scopic tracking of surgically implanted radiopaque crystals in
Patients with contraindications to a TEE examination were
35
35
Zmin
animals or using 3-dimensional (3D) transthoracic echocardiexcluded.
Commissural
3,4
36
36 221
Recently,
mitral annular
ography in humans.
A comprehensive
Journal
of Cardiothoracic
and Vascular
Anesthesia,
Vol nonplanarity
25, No 2 (April),
2011:
pp 221-228 2-dimensional TEE examination was
Beth Israel
Deaconess
Diameter
37 Center
37
has been described as the echocardiographically measured nonperformed after the induction of general anesthesia according
Medical
38
38
planarity angle with 3D datasets acquired using transesophato published guidelines6 with an IE-33 ultrasound system
Harvard
Medical
School
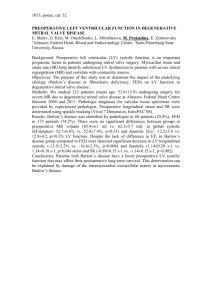
Mitral Annular Geometric Parameters
AL-PM
Diameter
AP
Diameter
5.319
Anterior Horn
Non-Planarity Angle
Annular Height
Change
3.523
4.653
Commissural
Diameter
PosteriorAnnulus
Length
AnteriorAnnulus
Length
Non-Planarity Angle
107.425
Annular Height
Change
Posterior Horn
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Conventional Geometric Analyses
Performed on a “STATIC” end-systolic frame
Snapshots of a continuous process
Not representative of the entire cardiac cycle
Extrapolation of information from a single frame
Major limiation
“ DYNAMIC” geometric analysis
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
Echocardiographic Identification of Annuloplasty Rings
Not possible reliably with 2D or 3D echocardiographic examination
Partial, Full, Flat or Saddle
Functional assessment does not separate the annuloplasty devices
Geometric distortions of annulus and leaflets CAN differentiate different
annuloplasty devices
Geometric distortions CAN impart more or less “STRESS” to the leaflets
Determine “DURABILITY” of repair
Harvard
Medical
School
Beth Israel Deaconess
Medical Center
R
What we know so far..........
Rigid full rings reliably prevent mitral annular dilatation but impair ventricular function
Flexible full rings and partial bands preserve ventricular function but are not as reliable in
preventing further annular dilatation
Rigid/Flexible full rings make the mitral annulus flatter and less non-planar
Partial bands do not affect the mitral annular non-planar shape
Saddle shaped full rings AUGMENT the saddle shape of the mitral annulus
Significant changes in mitral annular geometry with annuloplasty devices
Present analyses based on crude flow dependent variables or single frame 3D analyses
Beth Israel Deaconess
Medical Center
R
Harvard
Medical
School
What we know so far..........
When prevention of annular dilatation is the primary purpose FULL RING
When stabilization of mitral annulus is the primary purpose PARTIAL BAND
Significant Cross Over
Beth Israel Deaconess
Medical Center
R
Harvard
Medical
School