Peripheral vascular checklist
advertisement

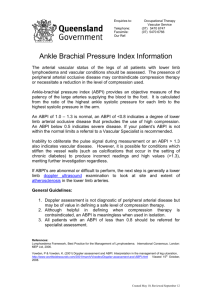
/HLFHVWHU0HGLFDO6FKRRO THE CARDIOVASCULAR SYSTEM PERIPHERAL VASCULAR EXAMINATION Impairment of the blood supply to any part of the body may be acute or chronic, caused, for example, by a thrombus or atherosclerosis respectively. You must be able to systematically examine for, and recognise, signs of vascular disease. Preparation Wash hands Introduction Consent and explanation √ Comments General Inspection Pain Conscious level Amputation √ Comments Hands Radial pulse Ulnar pulse Allen’s Test* Left Right Comments Arms Brachial pulses Blood pressure Left Right Comments Face Corneal arcus Xanthalasma Central cyanosis Anaemia Left Right Comments Neck JVP Palpate carotid pulses Auscultate carotid pulses Left Right Comments Abdomen Palpate abdominal aorta Auscultate abdominal aorta Palpate femoral pulses Auscultate femoral pulses Left Right Legs and Feet Palpate pulses: Popliteal pulses Posterior Tibialis pulses Dorsalis Pedis pulses Temperature Inspect for: Colour Capillary refill Hair loss Oedema Varicosities Ulceration/Gangrene Scars Trendelenberg Test* Burgers Test* ABPI* Left Right Comments Special Tests* Ankle:Brachial Pressure Index (ABPI) You need to know how to measure the ABPI, but you will not be required to perform it during the Phase 1 OSCE ABPI is measured using a hand-held Doppler and a sphygmomanometer. - The patient must be rested in the supine position or ankles raised to the same height as the heart. - The systolic pressure is measured in the dorsalis pedis and posterior tibial arteries of the same leg by holding the Doppler probe over the pedal artery while a blood pressure cuff wrapped around the ankle is inflated. - The pressure at which the Doppler signal disappears gives the systolic pressure in that artery. - The blood pressure (BP) should be taken in both arms and the ABPI is calculated as follows: ABPI = Highest ankle systolic pressure Highest brachial systolic pressure - A value for ABPI should be obtained for each leg Normally the systolic BP in legs ≥ arms so a normal ABPI should be ≥1 in the supine position. ABPI is a sensitive marker of arterial insufficiency. Typical values of ABPI are: - ≥1 = Normal - <0.9 = Abnormal - 0.5 – 0.9 <0.5 = Claudication = Critical Ischaemia Buergers Test - With the patient lying supine, stand at the foot of the bed. Raise the feet and support the legs at 45˚ to the horizontal. When the legs are elevated look for pallor of the sole of the foot along with emptying (or ‘guttering’) of the dorsal foot veins Ask the patient to sit up and swing the legs over the edge of the bed In the presence of critical limb ischaemia the foot will turn a deep red (‘sunset foot’) due to reactive hyperaemia. Allen’s Test This tests the collateral blood flow to the hand - Identify both radial and ulnar pulses and apply pressure simultaneously in order to occlude the arteries. - The patient should clench and unclench the hand until the palm goes pale. - Release pressure from the ulnar artery and observe for the distinct pink colouration (reactive hyperaemia) of the palm. - If the re-colouration of the palm is ≤ 5 seconds, then the circulation to the hand via the ulnar artery is adequate - The procedure can then be repeated to check the patency of the radial artery by releasing the radial artery first Trendelenbergs Test Used to test for saphenofemoral junction incompetence - only in the presence of varicose veins - Ask the patient to sit on the edge of the examination couch. - Elevate the limb as far as is comfortable for the patient and empty the superficial veins by ‘milking’ the leg. - With the leg still elevated, exert digital pressure (or apply a tourniquet) over the saphenofemoral junction o Locate the femoral artery by feeling for the pulse. The vein is medial to the artery and the saphenofemoral junction is about 2 fingers breadth below the inguinal ligament - Ask the patient to stand - In the presence of saphenofemoral junction incompetence the varicose veins will not refill until the digital pressure (or tourniquet) is removed.