Gait Training Strategies to Optimize Functional Ambulation in Adults
advertisement

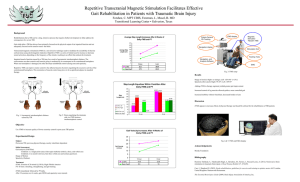
GAIT TRAINING & CHRONIC TBI Gait Training Strategies to Optimize Functional Ambulation in Adults with Chronic Traumatic Brain Injury: A Review of the Evidence Joy Iris Schoenherr, SPT Doctoral Candidate University of New Mexico School of Medicine Division of Physical Therapy Class of 2014 Advisor: Frederick Carey, PT, PhD Printed Name of Advisor: __________________________________ Signature: ______________________________ Date: ___________________ Approved by the Division of Physical Therapy, School of Medicine, University of New Mexico in partial fulfillment of the requirements for the degree of Doctor of Physical Therapy. 1 GAIT TRAINING & CHRONIC TBI ABSTRACT Background/Purpose: This case study and review of current available evidence aims to determine whether patients with chronic (>6 months post injury) traumatic brain injury (TBI) can make functional gains in ambulation with therapist directed gait training. This analysis also aims to determine which gait training methods lead to the most functional gains within this patient population. Case Description: Patient is a 48 year old male who sustained a TBI in September of 2010. He is referred to outpatient physical therapy on January 13, 2014, after having a cerebral spinal fluid (CSF) shunt placement on November 14, 2013. Outcomes: No single gait training intervention within the scope of physical therapy is superior to any other method. The various methods of gait training are each good at targeting and improving a specific deficit involved in the activity of gait. Body weight supported treadmill training is best for increasing selfselected velocity (SSV), and should be done without upper limb support for the most carry over. Robotic assisted treadmill training is best for improving the mobility domain of the Stroke Impact Scale (SIS), Functional independence measures (FIM), including FIM transfer and FIM ambulation items, and the Rivermead Motor Assessment (RMA) gross function subscale. Non-aerobic exercise interventions significantly decrease step length asymmetry when compared to over-ground gait training. Discussion: Because of the nature of chronic TBI, it is difficult to obtain a large sample size of homogenous subjects to participate in a study. Further, and more targeted, research is necessary to gain a solid conclusion as to which gait training methods lead to the most functional gains for chronic TBI patients. Based on the current available evidence, all methods improve overall gait for patients with chronic TBI, while some target more specific areas involved in gait. Therefore, tailoring a gait training program to a specific chronic TBI patient‟s areas of weakness, and using more than one intervention, will provide the 2 GAIT TRAINING & CHRONIC TBI best outcomes. All studies taken together suggest that gait training should be intensive, repetitious, and task oriented. BACKGROUND & PURPOSE Multiple studies have been conducted to establish the best gait training methods within the scope of physical therapy to improve ambulation function for patients with neurological conditions. However, the studies tend not to focus on patients with traumatic brain injuries (TBIs), but, instead those with conditions such as stroke (CVA), spinal cord injury (SCI), and Parkinson‟s Disease (PD). Studies that have been done with brain injured patients are usually are done with acute TBI patients within a rehabilitation setting, not chronic (>6 months post injury) TBI patients in an outpatient setting. Therefore, the purpose of this investigation is two-fold. The first goal is to use current literature to determine that therapist directed gait training can, in fact, lead to functional gains in patients with chronic TBI. Second, to determine which gait training methods yield the most functional gains for this patient population. The patient who served as the inspiration for this investigation has a TBI, which he sustained approximately three and a half years prior to referral to outpatient physical therapy. After evaluating the patient, the primary focus of outpatient physical therapy was aimed at improving his gait, specifically in terms of biomechanics, safety, and independence. Interventions included therapist facilitated gait training, partial body weight supported treadmill training (BWSTT), dance therapy, and therapeutic exercises targeting at improving strength, balance, and proprioception. INTRODUCTION 3 GAIT TRAINING & CHRONIC TBI Patient is a 48 year old male who sustained a TBI approximately three and a half years ago. The patient had received outpatient physical therapy in the Fall of 2013, after his first CSF shunt placement. The patient was referred to outpatient physical therapy once again after having his CSF shunt cleaned and replaced in November of 2013 to see if he could make gains in his functional independence. EXAMINATION Patient History: Patient has a past medical history of TBI, hearing loss, dental injury, retinal injury, decreased initiation, and decreased short-term memory. Since his most recent CSF surgery, the patient‟s family reported that he had increased balance, improvements in gait, and increased alertness. He is mostly nonverbal, but can verbalize. Patient lives with his parents in a single level home. He has caregivers 4 hours at a time, 4 times per week. SYSTEMS REVIEW Neurological: Incontinence of bladder, increased tone of right lower extremity (RLE). Functional Considerations: ADLs per mother‟s report: Patient requires assistance in standing balance for lower body dressing. He is independent with grooming while sitting, and he showers with modified independence, using a shower chair and hand-held shower head. He is independent with bed mobility, and requires supervision for bed transfers and ambulation with a front-wheeled walker (FWW). Observation: Patient presents with forward head and rounded shoulders. In sitting, the patient uses bilateral upper extremity support, has increased kyphosis of the thoracic spine and decreased lumbar lordosis. In standing, the patient has a left lean and decreased ability to weight shift to the right due to tone of right lower extremity. The patient is able to ambulate with a FWW with contact guard assistance (CGA) and voice commands for direction. He demonstrates decreased right DF during gait. He leans forward on 4 GAIT TRAINING & CHRONIC TBI his walker with a rounded upper body and looks down during ambulation. Patient has a tendency to lean backwards when cued to stand up straight. TESTS & MEASURES ROM: Both upper and lower body all within functional limits (WFL) except: decreased passive bilateral hip extensors, left greater than right secondary to bilateral hip flexor tightness, decreased passive right DF. Strength: All WFL except: Right hip flexors 3+/5, left hip flexors 4+/5, right knee flexors 3+/5, right knee extensors 3+/5, right ankle dorsiflexors 3-/5, right hip extensors 2/5, left hip extensors 3-/5, right hip abductors 4/5, left hip abductors 4+/5. Balance: Fair double leg stance balance in standing with eyes open, requiring contact assist and voice commands to maintain upright posture. Able to perform standing march with moderate hand-held assistance (HHA) from one person (x1) and voice cues (VCs). Reflexes: Lower extremities all WFL. Sensation: Sharp/dull in-tact BLE; light touch unable to assess lower extremities. Position Sense: Decreased in RLE, unable to test LLE. Coordination: Intact. EVALUATION Diagnosis: TBI Narrative Assessment: Patient is a 48 year old male with diagnosis of TBI who presents with postural deficits, decreased bilateral hip extension ROM, decreased right DF in gait, decreased right foot position 5 GAIT TRAINING & CHRONIC TBI sense and proprioception, tightness of bilateral hip flexors, tightness of bilateral ankle dorsi-flexors, gait dysfunction, decreased balance, and decreased initiation. Pt is transported in the community in a standard wheelchair. In his home, pt ambulates with a front-wheeled walker (FWW) with supervision/CGA, verbal cues (VCs), and tactile cues (TCs) for initiation. Goals: 1. The patient will demonstrate ability to perform a stand pivot transfer from mat to chair and chair to mat with VCs and SBA to increase functional independence and decrease caregiver burden in six weeks. 2. The patient will gain 0.5 MMT grade of all right lower extremity muscles to improve safety during transfers and ambulation in four weeks. 3. The patient will demonstrate ability to maintain upright posture with decreased pressure through his bilateral upper extremities on a FWW during ambulation to increase safety during ambulation in four weeks. 4. The patient will have an increase in bilateral hip extension ROM and increased right DF ROM to improve gait biomechanics wile ambulating with a FWW in four weeks. Plan of Care: Postural training, gait training, balance exercises, ROM exercises, strengthening exercises, neuromuscular re-education, caregiver/family education. Prognosis: Patient has fair to good prognosis. Patient has a good history of compliance and good family and caregiver support, which are facilitators to meeting goals. Patient has diagnosis of chronic TBI with decreased initiation and decreased alertness, which may pose barriers to meeting his goals. 6 GAIT TRAINING & CHRONIC TBI INTERVENTIONS Pt was treated with various therapeutic exercises in standing and sitting, conventional over-ground gait training (COGT), gait training with body weight support treadmill training (BWSTT), gait training with Bioness anterior tibialis nerve stimulator, neuromuscular re-education, and his caregivers were instructed on home exercise program (HEP) exercises to add to the patient‟s daily routine. Therapeutic Exercises: Pt sat on edge of mat (EOM) with a therapist behind him and a therapist in front of him. He was given verbal cues to reach up and forward for a rubber ball to facilitate anterior pelvic tilt, trunk control, and improved posture. Bosu was added under pt for anterior pelvic tilt. The therapist would place the ball in various positions to the sides and up above the pt, and the pt would reach for it. Pt would sit back to back with a therapist and pass a ball from side to side to encourage the patient to rotate trunk fully. Pt was verbally and tactilely cued to sit up straight and retract his shoulders during rest periods. Therapist sitting in front of pt would play catch with the patient, giving verbal cues to stay on task. Therapist would clasp hands with pt and push in various directions, cueing the patient to resist trunk movement, allowing isometric contractions of the pt‟s entire trunk. Seated ball reaching, ball pass, and manual resistance were all demonstrated to pt‟s caregiver for HEP. In standing, pt would perform step through exercises on two steps, holding on to two hand rails. Pt was cued to keep one foot on the first step, and step to the top step with the other foot. Pt required constant cueing to stay on task, to stand up straight and to look straight ahead. Pt was easily distracted by surrounding activity in the therapy gym. Pt also performed standing bilateral hip abduction while holding onto a rail with both hands; therapist performed lateral weight shift facilitation a pt‟s greater trochanters when necessary to keep pt on task. 7 GAIT TRAINING & CHRONIC TBI Pt performed rocker board, forward and backward with therapist facilitation at hips to facilitate bilateral hip, knee, and ankle disassociation/motion. Pt also received dance therapy with bilateral HHA and demonstration in front of pt, and another therapist behind pt implementing CGA and manual assist for WS. TCs/VCs to stay on task, move hips, copy movements, weight shift, and lift feet off of the ground. Music stimulus was played (“Cupid Shuffle”) which named commands for movements: step left, step right, alternating kicks, and pelvic swaying/rocking. Gait training in parallel bars: Side stepping (with and without hurdles), braiding, and forward and backward walking both directions. Forward walking over 3”x5” box hurdles with manual therapist cueing for pelvic rotation and weight shifting to the right. All exercises were performed with bilateral UE support, CGA, and implemented mass practice. COGT: Ambulating with FWW, CGA, VCs to walk more upright, TCs for pelvic rotation and weight shift to the right. Small cone hurdles added to encourage patient to decrease right toe drag, VCs to lift up right foot. Pt performed step to and step through gait over hurdles. Large mirror placed in front of pt to get him to look straight ahead and stand more upright. Initially, pt used FWW with cueing for upright posture and to decrease weight bearing through his upper extremities. Bilateral forearm supports were later added to his walker and pt was able to stand more upright. Pt‟s caregivers were instructed to have pt practice small hurdles at home for HEP. Pt also performed COGT with bilateral HHA, and another therapist behind the pt for CGA and manual assist for pelvic rotation and WS. TCs/VCs to keep pt from reaching for therapist‟s shoulders for support and to stay on task. 8 GAIT TRAINING & CHRONIC TBI Gait training with LiteGait BWSTT: Amount of body weight supported was not measured. Pt used bilateral UE support and walked at a pace of 0.6 - 0.8mph for 10 minutes total time with 1-2 rest breaks. Speed was increased each session depending on how good his gait was. Two therapists each placed a rolled up ace bandage in front of pt‟s foot in stance phase to act as a hurdle. Pt was given VCs/TCs to step over the bandage and lift his feet higher. Gait training with LiteGait BWSTT and Bioness: The Bioness was added after multiple treatments with just the LiteGait. The pt used bilateral UE support and was able to walk at a pace of 1.0mph for a duration of 10 minutes nonstop. The Bioness was set to activate dorsiflexion on patient‟s right foot as he began swing phase. A heel sensor was placed in pt‟s shoe to sense when his heel was unweighted and swing phase began. OUTCOMES Pt‟s caregivers acquired bilateral forearm supports for pt‟s walker at home which drastically decreased pt‟s weight bearing through UE during gait. Pt made noticeable improvements with gait speed and duration on LiteGait, initiated reciprocal stepping over hurdles on his own, and had increased toe clearance on the right foot with less VCs during gait. PICO In adult patients with chronic traumatic brain injury (>6 months), does physical therapist directed gait training lead to further improvements in functional gait? DATABASES SEARCHED/METHODS 9 GAIT TRAINING & CHRONIC TBI CINAHL, PubMed® (MEDLINE), Cochrane, and PEDro databases were searched. Keywords used were various combinations of „TBI‟ and: „Gait‟, „ambulation‟, „locomotion‟, „rehabilitation, and „physical therapy.‟ Reference lists of chosen articles were also searched. Inclusion Criteria: Studies conducted between January 2000 and present, subjects with diagnosis of chronic (> 6 months) TBI, and all subjects were age 18 or older when TBI acquired. Exclusion Criteria: No gait/ambulation related outcomes measured, case studies, any studies that included children, studies in which only 1 or 2 chronic TBI patients were included, studies that did not separately report TBI subjects‟ results from the results of those with other neurological diagnosis. ARTICLE SUMMARIES 1. Esquenazi, A., Lee, S., Packel, A.T., Braitman, L. (2013). A Randomized Comparative Study of Manually Assisted Versus Robotic-Assisted Body Weight Supported Treadmill Training in Persons With Traumatic Brain Injury. American Academy of Physical Medicine and Rehabilitation, 5, 280290. Level of Evidence: 2b Objectives: (1) To compare the effects of robotic-assisted treadmill training (RATT) and manually assisted treadmill training (MATT) in participants with traumatic brain injury (TBI) and (2) to determine the potential impact on the symmetry of temporal walking parameters, 6-minute walk test, and the mobility domain of the Stroke Impact Scale, version 3.0 (SIS). 10 GAIT TRAINING & CHRONIC TBI Design: Randomized prospective study. Subjects: A total of 16 participants with TBI and a baseline over ground walking self-selected velocity (SSV) of >/= 0.2 m/s to 0.6 m/s randomly assigned to either the RATT or MATT group. Intervention: Gait training for 45 minutes, 3 times a week with either RATT or MATT for a total of 18 training sessions. Outcome Measures: Primary: Overground walking SSV, maximal velocity. Secondary: Spatiotemporal symmetry, 6-minute walk test, and SIS. Results: Between-group differences were not statistically significant for any measure. However, from pretraining to post-training, the average SSV increased by 49.8% for the RATT group (P = .01) and by 31% for MATT group (P = .06). The average maximal velocity increased by 14.9% for the RATT group (P = .06) and by 30.8% for the MATT group (P = .01). Less staffing and effort was needed for RATT in this study. Step-length asymmetry ratio improved during SSV by 33.1% for the RATT group (P = .01) and by 9.1% for the MATT group (P = .73). The distance walked increased by 11.7% for the robotic group (P = .21) and by 19.3% for manual group (P = .03). A statistically significant improvement in the mobility domain of the SIS was found for both groups (P </= .03). Conclusions/Discussion: Between-group differences were not statistically significant for any measure; pretraining to post-training, the average SSV increased by 49.8% for the RATT group (P =.01) and by 31% for MATT group (P = .06); The average MV increased by 14.9% for the RATT group (P =.06) and by 30.8% for the MATT group (P = .01); Step-length asymmetry ratio improved during SSV by 33.1% for the RATT group (P = .01) and by 9.1% for the MATT group (P = .73); distance walked increased by 11.7% for the robotic group (P =.21) and by 19.3% for manual group (P =.03, 0.73); statistically significant improvement in the mobility domain of the SIS was found for both groups (P </= .03). Clinically, this means that based on specific goals for patients, available resources, and budget, different treatment methods are better for 11 GAIT TRAINING & CHRONIC TBI different things: BWSTT with manual and robotic assistance are both effective approaches to increase SSV and MV in persons with a TBI. RATT training may be better to improve step-length symmetry and SSV. MATT training may be best for improved 6MWT. Both methods significantly improve mobility. Neither training technique appears to be superior to the other; however, the Lokomat required fewer staff, less manual effort from the staff was reported, and costs less for staff required. 2. Bland, D.C., Zampieri-Gallagher, C., Damiano, D.L. (2011). Effectiveness of physical therapy for improving gait and balance in ambulatory individuals with traumatic brain injury: a systematic review of the literature. Brain Injury; 25(7-8): 664–679. doi: 10.3109/02699052.2011.576306. Level of Evidence: 3a Primary objective: Given the major impact of traumatic brain injury (TBI) on society and the fact that effective therapies for common deficits in balance and gait are not known, the purpose of this review was to investigate the efficacy or effectiveness of non-aerobic exercise interventions to improve balance and gait in functionally mild to moderate individuals with TBI (those who demonstrate the ability or capacity to ambulate) and to provide evidence-based guidelines for clinical practice. Methods: Authors searched eight databases (limits: January 1980 to December 2009) for papers including exercise interventions to improve gait and balance post TBI. Out of 984 unique citations, 20 fully met inclusion criteria. The methodological quality of studies was determined by the Physiotherapy Evidence Database (PEDro) scale and strength by Sackett's Levels of Evidence. Results: Authors found limited evidence of the positive effects of balance, gait, or the combination 12 GAIT TRAINING & CHRONIC TBI of both interventions, in TBI rehabilitation. Most studies included small sample sizes with heterogeneous groups, and the interventions were variable and lacked standardization. The outcome measures were variable and low in quality. These limitations made it difficult to draw useful evidence-based recommendations for clinical practice. Conclusions/Discussion: The state of evidence for gait and balance interventions in patients with mild to moderate TBI is surprisingly poor. The strongest evidence gathered suggests that BWSTT is no better at improving gait and balance outcomes (e.g. spatiotemporal parameters, functional gait and balance scales) in individuals with TBI than conventional over-ground gait training (COGT). Moderate evidence supports that Tai Chi is also equivalent to social activities performed in a community day center in improving individuals' self-description of coordination, flexibility and physical activity. Among those trials with control/comparison groups no intervention was shown to be significantly better than any other at improving outcomes, except in the study by Brown, which showed a greater decrease in step length asymmetry with COGT than with body-weight supported treadmill training (BWSTT). 3. Williams, G., Clark, R., Schache, A., Fini, N.A., Moore, L., Morris, M.E., McCrory, P.R. (2011). Training Conditions Influence Walking Kinematics and Self-Selected Walking Speed in Patients with Neurological Impairments. Journal of Neurotrauma, 28, 281–287. doi: 10.1089/neu.2010.1649. Level of Evidence: 2b Objectives: To identify the most effective form of gait training by comparing conditions for gait training for people with acquired brain injury (ABI). Seventeen people who had sustained an ABI and were unable to walk without assistance were recruited as a sample. Each participant was exposed to seven alternative gait 13 GAIT TRAINING & CHRONIC TBI training conditions in a randomized order. These were: (1) therapist manual facilitation; (2) the use of a gaitassistive device; (3) unsupported treadmill walking; and (4) four variations of body weight support treadmill training (BWSTT). Design: Cohort Study, non-treated control group. All subjects were recruited from a rehabilitation hospital in Australia. Setting: Gait laboratory. Participants: People who were unable to walk unassisted due to an acquired brain injury (n=17) and healthy control subjects (n=25). Interventions: The participants performed 7 alternative gait training methods in a randomized order. These were therapist manual facilitation, the use of a gait assistive device, treadmill walking with handrail support, and 4 variations of body weight–support treadmill training with combinations of handrail and/or therapist support. Main Outcome Measures: Quantitative gait analysis was performed and Gait Profile Scores (GPS) using Three-dimensional quantitative gait analysis (3DGA) gathered at each of 7 gait training conditions were generated for each participant to determine which condition most closely resembled normal walking. Results: BWSTT without additional therapist or self-support of the upper limbs was associated with more severe gait abnormality [Wilks‟ lambda = 0.20, F(6, 6) = 3.99, p = 0.047]. With the exception of therapist facilitation, the gait training conditions that achieved the closest approximation of normal walking required selfsupport of the upper limbs. When participants held on to a stable handrail, self-selected gait speeds were up to three times higher than the speeds obtained for over-ground walking [Wilks‟ lambda = 0.17, F(6, 7) = 5.85, p < 0.05]. The provision of stable upper-limb support was associated with high self-selected gait speeds that were not sustained when walking over ground. BWSTT protocols may need to prioritize 14 GAIT TRAINING & CHRONIC TBI reduction in self-support of the upper limbs, instead of increasing treadmill speed and reducing body weight support, in order to improve training outcomes. Conclusions/Discussion: The results obtained in this study indicate that if people with acquired brain injury (ABI) utilize upper limb support during BWSTT, they are most likely to be walking at a speed three times faster than that which can be obtained with therapist facilitation or the use of a gait-assistive device. The results obtained in this study indicate that if people with ABI utilize upper limb support during BWSTT, they are most likely to be walking at a speed three times faster than that which can be obtained with therapist facilitation or the use of a gait-assistive device. The bottom line, therefore, is that this study is that it is effective to gait trait TBI patients, eventually, without using upper limb support, as to gain a better idea of their true self selected speed when walking without BWS. The knowledge is valuable to me because it gives me just a little more information on how to train with BWS the most effectively. The conclusion, clinically, is that gait training with BWS should not include upper limb support in order for carry over regarding self-selected speed. 4. Clark, R.A., Williams, G., Fini, N., Moore, L., Bryant, A.L. (2012). Coordination of Dynamic Balance During Gait Training in People With Acquired Brain Injury. Archives of Physiotherapy Medical Rehabilitation, 93, 536-540. doi:10.1016/j.apmr.2011.11.002. Level of Evidence: 2b Objective: To investigate movement of the center of mass (COM) during different gait training methods in people with neurologic conditions. 15 GAIT TRAINING & CHRONIC TBI Design: Coordination of the gait cycle, represented by mediolateral COM displacement amplitude, timing, and stability, was assessed during a variety of gait training methods performed in a single session. Setting: Gait laboratory. Participants: People who were unable to walk unassisted due to an acquired brain injury (n=17) and healthy control subjects (n=25). Interventions: The participants performed 7 alternative gait training methods in a randomized order. These were therapist manual facilitation, the use of a gait assistive device, treadmill walking with handrail support, and 4 variations of body weight–support treadmill training with combinations of handrail and/or therapist support. Main Outcome Measures: Mediolateral COM movement was analyzed in terms of displacement amplitude (overall range of motion), timing (relative to stride time), and stability (steadiness of the movement). Normative values for these measures were acquired from 25 healthy participants walking at a self-selected comfortable pace. Results: Body weight–support treadmill training without any additional support resulted in significantly (P<.05) greater amplitude, altered timing, and reduced movement stability compared with non-pathologic gait. Allowing handrail support or therapist facilitation reduced this effect and resulted in treadmill training (with body weight support) having lower movement amplitudes when compared with the other training methods. Therapist manual facilitation most closely matched non-pathologic gait for timing and stability. Conclusions/Discussion: The results of this study suggest that treadmill training (with or without BWS) with handrail support appears to provide a suitable method for task-specific training of dynamic balance because it replicates mediolateral (ML) center of mass (COM) amplitudes found in non-pathologic gait. However, upper-limb support decreases timing and variability components of the gait pattern. The study suggests that BWS training is good for increasing cardiovascular endurance because it covers more 16 GAIT TRAINING & CHRONIC TBI distance in the same amount of time as OGT, but it sacrifices timing and stability. Because there are many factors to consider, and variable outcomes depend upon treatment conditions, a rehabilitation program that includes a variety of gait training strategies seems to be the safest way to improve all aspects of gait. The bottom line is that, depending on which aspects of gait my particular patient is lacking, I can choose from all training conditions to work on them individually. My patient has an issue with postural instability, but also needs work on timing. Therefore, I will implement multiple training strategies into his rehabilitation. 5. Strickey, S. (2007). There is evidence to suggest that partial weight-bearing gait training is no more effective than conventional gait training in achieving independent ambulation in a traumatic brain injury population. Retrieved from University of British Columbia: http://www.mrsc.ubc.ca/images/StrickeyCAT_2007.pdf. Level of Evidence: 3a Objectives: The purpose was to review current practices in acquired brain injury (ABI) rehabilitation and aims to achieve the following: (i) identify effective treatment interventions; (ii) identify gaps in the literature deserving further research and; (iii) serve as an accessible tool for clinicians in an effort to encourage improved evidence-based practice. Search Methods: Multiple databases searched for RCTs, systematic reviews and other non-experimental design studies of adolescents and adults who had sustained a TBI and were receiving partial weightbearing gait training (alternatively called body weight supported treadmill training). Extensive search of CINAHL, EMBASE, MEDLINE and PsycINFO from 1980-2005 inclusive. Search was limited to studies dealing with rehabilitation and therapy. All experimental and non-experimental designs as well as 17 GAIT TRAINING & CHRONIC TBI systematic reviews, mete-analyses and review articles were included. A citation search of selected articles was also performed. Main Outcome Measures: Independent ambulation as measured by the Functional Ambulation Category (FAC). Results: Five articles met the inclusion criteria; two randomized controlled trials (RCTs), one systematic review, one case study and one single case design. Both RCTs (Brown et al., 2005) (Wilson et al., 2006) found the experimental group using PWB gait training to not show any significant differences in measured outcomes than the control group using conventional gait training methods. The systematic review (Teasell et al., 2007) studied these same RCTs and made a similar conclusion. Both subjects in the single case design (Wilson & Swaboda, 2002) and the subject in the case study (Scherer, 2007) showed improvement over time, but there was no control for comparison and the results were not reported in statistical terms. Conclusions/Discussion: Based on the results of two RCTs of good or fair quality it appears that PWB gait training methods are not more effective than conventional methods. A partial weight-bearing system is a costly piece of equipment for any facility. It also requires a substantial amount of human resources to operate, so it may not be worth the cost if there is no added benefit to patient functional outcomes. The lack of evidence to support its use in the TBI population may be related to the lack of a homogenous sample that was selected, small sample sizes, outcomes measures that were not specific enough to detect change and lack of uniform treatment protocols, and improper blinding of assessors. It is difficult to find a large homogenous sample in the TBI population due to the variability of TBI sequelae, but a larger sample size study would lead to more valid evidence on this topic. 6. 18 GAIT TRAINING & CHRONIC TBI Brown, T.H., Mount, J., PT, Rouland, B.L., Kautz, K.A., Barnes, R.M., Kim, J. (2005). Body WeightSupported Treadmill Training Versus Conventional Gait Training for People With Chronic Traumatic Brain Injury. Journal of Head Trauma Rehabilitation, 20(5), 402-415. Level of Evidence: 2b Objectives: To compare body weight support treadmill training (BWSTT) to conventional overground gait training (COGT). Design: Randomized controlled trial. Setting: Residential rehabilitation center. Participants: Twenty subjects with chronic traumatic brain injury (TBI). Intervention: The BWSTT or COGT for 15 minutes plus 30 minutes of exercise 2 days per week, for 3 months. Main Outcome Measures: Functional Ambulation Category (FAC), Functional Reach (FR), Timed Up and Go; gait velocity, step width (BOS) and step length differential using instrumented gait mat. Results: Step width approached the norm without between-group differences. Step length differential improved significantly more for the COGT. Conclusions/Discussion: Physical therapy can improve gait for patients more than 6 years post-TBI. The COGT is only more effective than the BWSTT for improving gait symmetry during over-ground walking. The only outcome that improved significantly for both groups from pretest to posttest was step width during gait that narrowed (approaching the norm) and could be an indication of improved balance, and improved gait. 19 GAIT TRAINING & CHRONIC TBI The bottom line is that BWSTT for TBI patients can be used if it is convenient, or if the therapist feels that it would be safer and more ergonomic for the patient and therapist. COGT is just as effective as BWSTT, and possibly more effective for gait improvement in chronic TBI patients. 7. Hellweg, S., & Johannes, S. (2008). Physiotherapy after traumatic brain injury: A systematic review of the literature. Brain Injury, 22(5), 365-373. Level of Evidence: 3a Primary objectives: At present there are no standardized recommendations concerning physiotherapy of individuals with traumatic brain injury (TBI) resulting in a high variability of methods and intensity. The aim of this literature review is to develop recommendations concerning physiotherapy in the post-acute phase after TBI on the basis of scientific evidence. Method: literature review: data bases: PubMed, PEDro, OT-Seeker, Cochrane and Cinahl. Keywords: brain injury (in PEDro, OT-Seeker, Cochrane), brain injury AND physical therapy (in PubMed and Cinahl). Results: Fourteen studies met the inclusion criteria and were grouped into sub-groups: sensory stimulation, therapy intensity, casting/splinting, exercise or aerobic training and functional skill training. While for sensory stimulation evidence could not be proven, a strong evidence exists that more intensive rehabilitation programmes lead to earlier functional abilities. The recommendation due to casting for the improvement of passive range of motion is a grade B, while only a C recommendation is appropriate concerning tonus reduction. Strong evidence exists that intensive task-orientated rehabilitation programs lead to earlier and better functional abilities. 20 GAIT TRAINING & CHRONIC TBI Conclusions/Discussion: Although some recommendations for the effectiveness of physical therapy interventions could be expressed, there are many questions concerning the treatment of humans with TBI which have not been investigated so far. Especially on the level of activity and participation only a few studies exist. The SR gives acceptable information about treatments for patients with TBI, but does not make any advancements in current treatments, nor does it bring to light any discrepancies with current methods. Basically, regarding the functional training category that included gait training, it reinforced that the training should be repetitious, intensive, task oriented, and it does not matter if it is done with partial body-weight support or not. However, only 2 studies were used for comparison and review in this category. The studies used were not thoroughly explained, nor were their PEDro scale ratings. The authors simply said they were either low or high rated according to their own standards. Due to this lack of details, and the fact that the authors included studies with as low a PEDro score as 4/10, there is not enough information to consider this SR extremely valid. It has very low validity, but is, however, clinically relevant. 8. Chin, L.F., Lim, W.S., Kong, K.H. (2010). Evaluation of robotic-assisted locomotor training outcomes at a rehabilitation centre in Singapore. Singapore Medical Journal, 51(9), 709-715. Level of Evidence: 2b Objective: The aim of this study was to determine whether robotic-assisted locomotor training, a new clinical service introduced at the Tan Tock Seng Hospital (TTSH) Rehabilitation Centre, Singapore is effective at improving the ability to transfer and the ambulatory status of patients with an acquired brain injury (ABI). 21 GAIT TRAINING & CHRONIC TBI Design: This was a retrospective review of data collected from patients with an acquired brain injury, before and after robotic-assisted locomotor training from September 2008 to May 2009. The primary outcome measures used were the functional independence measure (FIM) for transfer and ambulation, and the Rivermead Motor Assessment (RMA) gross function subscale. The secondary outcome measures used were the Motricity Index (MI) and Modified Ashworth Scale (MAS) of the lower limb. Statistical analysis was performed on this data to evaluate whether robotic-assisted locomotor training was effective at improving the functional mobility of these patients. Results: Significant improvement was observed in the scores of FIM transfer (p < 0.05), FIM ambulation (p < 0.05) and RMA (p < 0.05) after robotic-assisted locomotor training. Significant improvements in the MI of hip flexion (p < 0.05), knee extension (p < 0.05) and ankle dorsiflexion (p < 0.05) post training have also been noted. When taken separately, the 10 subjects with chronic brain injury showed significant improvement in the FIM ambulation score and the MAS of the calf muscle. Conclusions/Discussion: This equipment could possibly help patients make more functional gains in regards to gait independence, which is significant. However, the equipment is costly, and the sample size of chronic patients was small (n=10). Since other, more affordable methods have already been shown to improve gait for the chronic TBI population, this intervention would not be appropriate for use in my clinical setting. Until there is more valid evidence to support the benefits of the Lokomat, I do not think that this intervention is cost effective enough in the clinic. DISCUSSION Based on current available research, no single gait training intervention within the scope of physical therapy is superior to any other method for this patient population, and all methods lead to improvements in gait. However, all studies to date include threats to validity that negatively impact the strength of their findings. 22 GAIT TRAINING & CHRONIC TBI Most brain injury trials are done with patients in the acute phase of rehabilitation, which is why it is important to shed light on the outcomes for the chronic brain injured population instead. I chose not to include any studies in which there were less than 4 subjects with chronic brain injury, simply because the power (of the population that I am targeting) was small in those studies, and, small power equals less validity. One problem with available research is that each study provided significant support for individual functional outcomes, but no two studies show significant findings of the same outcomes. Body weight supported treadmill training can yield significant increases in self-selected velocity (SSV), and should be done without upper limb support for the most carry over. Robotic assisted treadmill training shows the most improvement of the mobility domain of the Stroke Impact Scale (SIS). Non-aerobic exercise interventions significantly decrease step length asymmetry when compared to over-ground gait training. Homogeneity Issue: Variations among the brain injured populations make it difficult for researchers to obtain homogenous samples for their studies. One difference noted among brain injured patients is method of brain injury. If the cause was non--traumatic, the pathology is referred to as „acquired brain injury‟ (ABI) instead of „traumatic brain injury‟ (TBI). This poses a problem because the cause can range from a hemorrhagic stroke to a brain tumor. The variability in cause of brain injury, in turn, can cause large variations in presentation, function, and recovery of patients. Another notable difference between subjects is time since injury, or, chronic versus acute brain injury. Both chronic and acute TBI patients‟ outcomes are combined in every study except one (Chin, et al. 2010). Patients during the acute phase of brain injury have the capacity to make larger gains during this initial 23 GAIT TRAINING & CHRONIC TBI recovery period than they do after 6 months, meaning that the two types of patients‟ outcomes will vary considerably, and should be separated in future studies. CONCLUSION/BOTTOM LINE It is possible for chronic (>6 months post injury) TBI patients to make functional ambulation gains long after their initial injury. However, further research is necessary to gain a solid conclusion as to which gait training methods lead to the most functional gains for chronic this population. The research needs to be done with larger sample sizes, homogenous populations, blinding in all areas, and valid outcome measures. Thus far, the research has concluded that tailoring a gait training program to specific chronic TBI patient‟s areas of weakness, and using more than one intervention, is the most effective way to achieve functional improvements in gait for chronic TBI patients. All studies‟ results taken in summation also suggest that gait training for the chronic TBI population should be intensive, variable, repetitious, and task oriented. REFERENCES 1. Esquenazi, A., Lee, S., Packel, A.T., Braitman, L. (2013). A Randomized Comparative Study of Manually Assisted Versus Robotic-Assisted Body Weight Supported Treadmill Training in Persons With Traumatic Brain Injury. American Academy of Physical Medicine and Rehabilitation, 5, 280-290. 2. Bland, D.C., Zampieri-Gallagher, C., Damiano, D.L. (2011). Effectiveness of physical therapy for improving gait and balance in ambulatory individuals with traumatic brain injury: a systematic review of the literature. Brain Injury; 25(7-8): 664–679. doi: 10.3109/02699052.2011.576306. 24 GAIT TRAINING & CHRONIC TBI 3. Williams, G., Clark, R., Schache, A., Fini, N.A., Moore, L., Morris, M.E., McCrory, P.R. (2011). Training Conditions Influence Walking Kinematics and Self-Selected Walking Speed in Patients with Neurological Impairments. Journal of Neurotrauma, 28, 281–287. doi: 10.1089/neu.2010.1649 4. Clark, R.A., Williams, G., Fini, N., Moore, L., Bryant, A.L. (2012). Coordination of Dynamic Balance During Gait Training in People With Acquired Brain Injury. Archives of Physiotherapy Medical Rehabilitation, 93, 536-540. doi:10.1016/j.apmr.2011.11.002 5. Strickey, S. (2007). There is evidence to suggest that partial weight-bearing gait training is no more effective than conventional gait training in achieving independent ambulation in a traumatic brain injury population. Retrieved from University of British Columbia: http://www.mrsc.ubc.ca/images/StrickeyCAT_2007.pdf 6. Brown, T.H., Mount, J., PT, Rouland, B.L., Kautz, K.A., Barnes, R.M., Kim, J. (2005). Body WeightSupported Treadmill Training Versus Conventional Gait Training for People With Chronic Traumatic Brain Injury. Journal of Head Trauma Rehabilitation, 20(5), 402-415. 7. Hellweg, S., & Johannes, S. (2008). Physiotherapy after traumatic brain injury: A systematic review of the literature. Brain Injury, 22(5), 365-373. 8. Chin, L.F., Lim, W.S., Kong, K.H. (2010). Evaluation of robotic-assisted locomotor training outcomes at a rehabilitation centre in Singapore. Singapore Medical Journal, 51(9), 709-715. 25