(This is a sample cover image for this issue. The actual cover is not yet available at this time.)
This article appeared in a journal published by Elsevier. The attached
copy is furnished to the author for internal non-commercial research
and education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling or
licensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of the
article (e.g. in Word or Tex form) to their personal website or
institutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies are
encouraged to visit:
http://www.elsevier.com/copyright
Author's personal copy
NeuroImage 69 (2013) 256–266
Contents lists available at SciVerse ScienceDirect
NeuroImage
journal homepage: www.elsevier.com/locate/ynimg
Development of a novel robust measure for interhemispheric synchrony in the
neonatal EEG: Activation Synchrony Index (ASI)
Okko Räsänen a, Marjo Metsäranta b, Sampsa Vanhatalo c, d,⁎
a
Department of Signal Processing and Acoustics, Aalto University, Espoo, PO Box 13000, 00076 AALTO, Finland
Children's Hospital, Helsinki University Central Hospital and University of Helsinki, Helsinki, PO Box 281, 00029 HUS, Finland
Department of Children's Clinical Neurophysiology, Helsinki University Central Hospital, Helsinki, PO Box 280, 00029 HUS, Finland
d
Department of Neurological Sciences, 00014 University of Helsinki, Finland
b
c
a r t i c l e
i n f o
Article history:
Accepted 11 December 2012
Available online 20 December 2012
Keywords:
Preterm
Connectivity
Asynchrony
Asymmetry
EEG monitoring
EMG
a b s t r a c t
The degree of interhemispheric synchrony in the neonatal EEG assessment refers to the co-occurrence of activity bouts during quiet sleep or burst suppression, and it has been widely considered as a key component in
assessing background activity. However, no objective measures have been published for measuring it, and all
conventionally used visual criteria suffer from significant ambiguities. Our present study aimed to develop
such a quantitative measure of (a)synchrony, called activation synchrony index (ASI). We developed the
ASI paradigm based on the testing of statistical independence between two quantized amplitude envelopes
of wideband-filtered signals where higher frequencies had been pre-emphasized. The core parameter settings of ASI paradigm were defined using a smaller EEG dataset, and the final ASI paradigm was tested
using a visually classified dataset of EEG records from 33 fullterm and 25 preterm babies, which showed varying grades of asynchrony.
Our findings show that ASI could distinguish all EEG recordings with normal synchrony from those with
modest or severe asynchrony at individual level, and there was a highly significant correlation (p b 0.001) between ASI and the visually assessed grade of asynchrony. In addition, we showed that i) ASI is stable in recordings over several hours in duration, such as the typical neonatal brain monitoring, that ii) ASI values
are sensitive to sleep stage, and that iii) they correlate with age in the preterm babies. Comparison of ASI
to other three potential paradigms demonstrated a significant competitive advantage. Finally, ASI was
found to be remarkably resistant to common artefacts as tested by adding significant level of real EEG artefacts from noisy recordings.
An objective and reliable measure of (a)synchrony may open novel avenues for using ASI as a putative early
functional biomarker in the neonatal brain, as well as for building proper automated classifiers of neonatal
EEG background. Notably, the signature of synchrony of this kind, temporal coincidence of activity bouts, is
a common feature in biological signals, suggesting that ASI may also hold promise as a useful paradigm for
assessing temporal synchrony in other biosignals as well, such as muscle activities or movements.
© 2012 Elsevier Inc. All rights reserved.
Introduction
Neonatal EEG has been routinely performed in centers with specialized neurophysiological service for many decades, and the analysis of
Abbreviations: aEEG, amplitude integrated electroencephalogram; AS, active sleep;
ASI, activation synchrony index; BAF, band amplitude fluctuation; CC, cross correlation; EDF, European Data Format; EEG, electroencephalogram; EMG, electromyogram;
ETDF, energy weighted temporal dependency function; FbEEG, Full band electroencephalogram; FFT, fast Fourier transform; FIR, finite impulse response; FT, full term;
HPF, high-pass filter; IIR, infinite impulse response; MIF, mutual information function;
NICU, neonatal intensive care unit; QS, quiet sleep; RMS, root mean square; SAT, spontaneous activity transient; TA, trace alternant.
⁎ Corresponding author at: Department of Children's Clinical Neurophysiology, Helsinki
University Central Hospital, Helsinki, PO Box 280, 00029 HUS, Finland.
E-mail address: sampsa.vanhatalo@helsinki.fi (S. Vanhatalo).
1053-8119/$ – see front matter © 2012 Elsevier Inc. All rights reserved.
http://dx.doi.org/10.1016/j.neuroimage.2012.12.017
EEG has been conventionally based on visual recognition of waveforms
(André et al., 2010). New understanding of the consequences of neonatal adversities (Mwaniki et al., 2012), as well as the recent improvements in early neonatal care have led to a rapidly increasing need for
EEG in the neonatal care units that do not have access to expert interpretation of the EEG recordings (Boylan et al., 2010). At the same time, there
has been a surge in the academic interest to better understand physiological and pathological mechanisms in the newborn brain. This new situation has set the request to develop more objective analysis paradigms,
as well as to improve hardware for brain monitoring.
A clear priority in the recent work on automated neonatal EEG analysis has been on detecting seizures (Deburchgraeve et al., 2008; Temko
et al., 2011). However, majority of the EEG literature in the past
40 years has focused on the importance of assessing the spontaneous
EEG activity (a.k.a. background or ongoing EEG). Some characteristics
Author's personal copy
O. Räsänen et al. / NeuroImage 69 (2013) 256–266
of this ongoing EEG are established to be crucial for clinical interpretation in both acute settings (e.g. recovery from birth asphyxia) as well
as in estimating longer term prognosis (Holmes and Lombroso, 1993;
Walsh et al., 2011; Watanabe et al., 1999).
One key feature in the classification of neonatal EEG background is
visual assessment of interhemispheric synchrony, which is considered
to reflect the level of interaction between hemispheres. Synchrony of
this kind is traditionally estimated from the temporal coincidence of
the intermittent bouts of activity (often called bursts; a.k.a. spontaneous
activity transients, SATs; see Table 1 in Vanhatalo and Kaila, 2010) during quiet sleep that is characterized by a background pattern called
trace alternant/discontinu. Prior studies have shown, for instance, that
interhemispheric synchrony of this kind increases towards term age,
and that many clinical compromises in brain function will lead to a decrease in synchrony, identified as an increased asynchrony (Hahn and
Tharp, 1990; Koeda et al., 1995; Lombroso, 1979; Monod et al., 1972;
Walsh et al., 2011).
Strikingly in this context, there are no unanimous and/or unequivocal definitions of interhemispheric (a) synchrony, and likewise, there
are no established, plausible paradigms for its measurement. Some previous studies have used a notion “more than 50% asynchrony” without
indicating what the given percentage value refers to in the EEG signal.
Other studies have followed a little more detailed method introduced
by Dr. Lombroso (Lombroso, 1979): asynchrony is understood to mean
that the onset of an individual burst/activation in two hemispheres is
more than 1.5 s apart (even 2 s has been used Anderson et al., 1985),
and the level of asynchrony refers to the proportion of bursts that exceed
this threshold. There are several problems that make such criteria
unhelpful: First, the 1.5 s time lag in the context of central nerve conduction velocity in newborns (10 m/s; Khater-Boidin et al., 1992) implies
that the axonal pathway between hemisphere could be up to insensible
15 m. Second, definition of burst onset is ambiguous. It relies either on
amplitude criteria that is sensitive to highpass filter settings, or it relies
on subjective assessment shown to have significant interrater variability
(Palmu et al., 2010). Third, bursts/activations in the fullterm EEG last for
about 2–5 s, and they re-occur quasiperiodically with about 10 s intervals. Bursts in two time series of this kind would have a considerable
temporal overlap, falsely interpreted as an “apparent synchrony,” even
in the absence of a true temporal relationship. One earlier study went
even further in definitions, and considered only such bursts that involved more than four out of six electrodes (Vecchierinia et al., 2003).
Such approach obviously yields high estimates of “synchrony” due to
outright exclusion from analysis of bursts that are asynchronous.
It is obvious that an objective measure of interhemispheric synchrony can only be based on sufficiently robust statistical analysis,
which integrates assessment of temporal coincidence of the activity
bouts over longer periods of EEG signal. In the current work, we developed a computational method for automatic estimation of activation synchrony index (ASI) between two EEG signals. The method is
based on measuring statistical dependency of quantized signal envelopes of two EEG signals. The dependency is measured as a function of
delay between the signals, and weighted by the instantaneous signal
energy. Such quantification of temporal synchrony yields a simple
scalar measure that describes how large proportion of covariation
(often perceived as ‘coupling’) between the signals is mediated by
immediate (zero-delay) synchrony. In addition, the method provides
an easily interpretable representation of how signal energies of the
two channels are dependent at different temporal delays.
Materials and methods
The overview of the process for estimating activation synchrony
index (ASI) is schematically presented in Fig. 1B. In our pilot experiments, we identified the key parameters (e.g. frequency band and
window length; see Chapter 2.7.) by using a few neonatal EEG traces
with clearly normal (grade 0) and severely abnormal (grade 3)
257
scoring. We chose to define these parameters by reasoning from intermediate results, because a formal optimization would need an unambiguous reference dataset, which does not exist. After the pilot
phase, we ran through the actual study aiming to i) assess the ability
of ASI to distinguish visually detected asynchrony in the larger clinical
dataset, ii) to look at the sensitivity of the paradigm to external noise
or changes in recording configuration (different electrodes), as well
as iii) to compare ASI to some other relevant methods found in the literature. A standalone software for calculating ASI in the way described in this paper will be made available from the authors at
request.
Preprocessing
Our ASI paradigm is based on measuring the statistical dependency of amplitude levels in two signals (in most cases in this paper, F3–
P3 and F4–P4). The goal of the pre-processing stage is to facilitate this
measurement by 1) representing the signals with a desired time resolution, 2) weighting different signal frequencies according to clinical
relevance, and 3) discretizing the signals into a finite number of amplitude levels to allow statistical analysis in a discrete probability
space.
During pre-processing, signals are first down sampled to fs =
50 Hz and “pre-emphasized” (Fig. 2A) with a first order FIR highpass filter of the form H(z) = 1–0.95z −1 in order to increase the relative contribution of middle- and higher frequencies in the subsequent
analysis. Fast Fourier Transform (FFT) is then used to compute the instantaneous amplitude spectra of the signals. FFT is computed for
both channels using a sliding Hamming window of 2 s that is
moved in 100–ms steps across the entire duration of the signals. Amplitude envelopes of the signals in the frequency range of 1.5–25 Hz
are computed by summing across the individual FFT bins corresponding to these frequencies, yielding smoothed high-pass envelopes of
the EEG.
In the last pre-processing step (labeled as “Q” in Fig. 1B), the amplitude values of the continuous valued amplitude envelope (or, to be
precise, 65536 unique values at 16 bits) are quantized into a smaller
number of representative signal states, or partitions, that can be
used as a basis for statistical measurements. The idea is to represent
signals A and B with sufficiently small number of amplitude levels
so that each level occurs several times in a typical EEG recording.
This then allows reliable estimation of the joint probabilities of amplitude value combinations between the two signals, e.g. the probability
of observing high-amplitude burst simultaneously in both signals.
The requirement of a small number of amplitude levels is due to the
fact that the joint probability space increases exponentially with increasing number of quantization levels, also requiring exponentially
longer recordings for reliable estimation of the signal parameters.
The quantization is performed with quantization levels adapted to
the distribution of amplitude values in the signals. Ideally, the quantized signal representation covers the entire scale of envelope amplitudes in a way that the signal samples are uniformly distributed into
different quantization levels. In the current implementation, 10000
randomly chosen samples from the smoothed signal envelopes from
both channels were used as the input to a standard k-means clustering algorithm in order to estimate N quantization levels (in the current work, N = 8 was used). Finally, the envelopes of both channels
are quantized using the estimated levels by assigning each signal
sample to the closest quantization level and replacing the original
sample with an integer label uniquely defining the quantization
level. This leads to a representation where left hemisphere channel
F3–P3 is represented by a discrete sequence A = {a1, a2, …, aL}, ai ∈
{1, 2, …, N}, and right hemisphere channel F4–P4 as B = {b1, b2, …,
bL}, bj ∈ {1, 2, …, N}, correspondingly, and where L denotes the number of samples in the signals.
Author's personal copy
258
O. Räsänen et al. / NeuroImage 69 (2013) 256–266
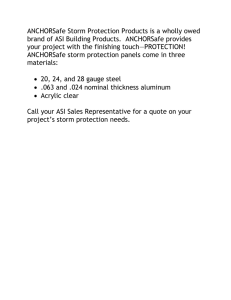
Fig. 1. Overall construct of the ASI paradigm. A)Photograph showing a neonatal EEG recording with the electrode placement according to the conventional 8–10 channel neonatal
setup. Green rings have been placed around the right side electrodes (F4 in front, P4 in the back) that were used for most analyses in this study. B) Schematic representation of the
ASI paradigm. (Ch = channel; FFT = Fast Fourier Transform; Q = quantization; ETDF = energy weighted temporal dependency function) C) Examples of signals at different stages of
ASI computation for a normally synchronous EEG. Top panel: the original signal waveforms for left (red) and right (blue) hemispheres. Middle panel: pre-emphasized and temporally smoothed energy envelopes. Bottom panel: quantization indices for the energy envelopes. D) Comparison of ETDFs calculated for four synchronous (left panel) and four asynchronous (right panel) EEG recordings. Asynchrony in brain activity is observed as a flat dependency distribution across multiple lags or as one or more peaks outside τ = 0.
Different colors show different subjects.
Energy-weighted temporal dependency function
In the current work, we define synchrony as a phenomenon where
two signals do not evolve independently of each other, but where
both signals carry predictive information regarding the concurrent
state of the other signal. Therefore, the overall goal is to measure
the dependency of signal states in two different sequences, namely
quantized amplitude envelopes recorded from left and right hemispheres. In addition, special attention is paid to the dependency of
high-energetic events (activity bursts) in the signals, whereas simultaneous occurrence of low-energy background in the trace alternant
data serves no clinical purpose. In order to integrate these considerations into a single quantitative measure, we introduce the concept
of energy-weighted temporal dependency function, or ETDF.
The starting point of the ETDF is the estimation of the statistical
dependency between the two signals of interest. As was described
in the pre-processing stage, the signals are first converted into discrete sequences of form A = {a1, a2, …, aL}, ai ∈ {1, 2, …, N} and B =
{b1, b2, …, bL}, bj ∈ {1, 2, …, N}, for the left and right hemisphere signals, respectively.
It is known from the earlier work that the mutual information
function (MIF; Li, 1990) can be used to estimate the average dependency of discrete variables a in a sequence X = {a1, a2, …, aL} when
the variables are always separated by a lag τ:
1
0 p X ðt Þ ¼ ai ; X ðt þ τ Þ ¼ aj
A
MIFðτ Þ ¼ ∑ p X ðt Þ ¼ ai ; X ðt þ τ Þ ¼ aj log2 @
i;j
pðX ðt Þ ¼ ai Þp X ðt þ τ Þ ¼ aj
ð1Þ
where t denotes time and p(X(t) = ai, X(t + τ) = aj) is the probability
of observing aj after ai with τ − 1 non-specified elements in between.
For notational simplicity, we can rewrite the above equation as
MIFðτ Þ ¼ ∑ pτ ai ; aj
i;j
1
pτ ai ; aj
A
log2 @
pðai Þp aj
0
ð2Þ
with subscript τ denoting that the aj and ai are always τ elements
apart in the sequence. The probabilities can be derived from a finite
sequence by simply counting the frequencies of occurrences of different states ai or state pairs {ai, aj} and then normalizing them by the
total frequency count (maximum-likelihood estimator).
What MIF essentially does is that it compares the joint probability
pτ(ai,aj) of two variables to the product of their individual probabilities p(ai) and p(aj). The more the ai and aj are dependent on each
other, the higher the ratio will be. This dependency is then measured
in bits and summed across all variables in the data, weighted by the
relative frequency of each element pair.
In contrast to the standard MIF, here we wish to measure the dependency of signal states between two different sequences. This is
achieved by simply exchanging the delayed state aj from the same
signal with a signal state bj originating from the second signal B, corresponding to a situation where signal B is simply delayed by τ samples in relation to the signal A. Also, we omit the logarithm in the
equation since we are not interested in bits of information but in
the overall linear dependency between the signals measured across
all possible pairs of signal states (see, e.g., Räsänen, 2012 for similar
use of non-log MIF).
Author's personal copy
O. Räsänen et al. / NeuroImage 69 (2013) 256–266
259
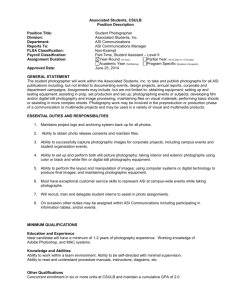
Fig. 2. Pre-processing and ASI stability. A) Frequency response profile of the filter used for pre-emphasizing the higher frequencies. B) Defining the optimal frequency band for ASI
computation. The optimal low- and high cutoff frequencies depends on the presence or absence of the pre-emphasis filter. The gray scale shows correlation between visual rating
and ASI value (dark is higher correlation) measured over the patient population. C) ASI estimates in the whole dataset without (left) and with (right) pre-emphasis filtering. Note
how the pre-emphasis filtering enhances the differentiation of normal synchrony and mild asynchrony. D) Effect of ASI window on the variability of ASI estimate. Note how ASI
estimate becomes significantly more stable, i.e. less variable when the window is extended from 15 s to 10 min. All values are calculated from one longer EEG epoch. E) Stabilization
of ASI estimate over time. The graph demonstrates ASI values in three 20 min long recordings taken from three different patients. Note how the ASI estimate fluctuates during the
first few minutes and then finds a stable level (see also Fig. 3B) as the statistical evidence of synchrony accumulates.
Finally, in order to measure the dependency of signal energy instead of purely abstract states, we weight each state pair {ai, bj}
(that are simply categorical values without ordinal information) by
the product of the amplitude values corresponding to the given
states. This leads to so-called energy weighted temporal dependency
function (ETDF):
2
2
pτ ai ; bj
pτ ai ; bj
¼ ∑ Eðai ÞE bj
ETDFðτÞ ¼ ∑ w ai ; bj
i;j
i;j
pðai Þp bj
pðai Þp bj
ð3Þ
where E(a) is the amplitude corresponding to the quantization level a in
signal A and E(b) is the amplitude corresponding to the quantization
level b in signal B. Essentially, the ETDF computes the average deviation
from statistical independency of the variables in the sequences A = {a1,
a2, …, aL} and B = {b1, b2, …, bL} when B is delayed by τ units with respect to A. Moreover, the contribution of each variable pair is weighted
by the product of the signal amplitudes corresponding to the variables,
ensuring that the measure emphasizes high-energetic parts of the signal over background activity (see Belis and Guiasu, 1968 and Dial and
Taneja, 1981, for the combination of information theoretic measures
with qualitative weights).
In order to derive ASI from the ETDF, the ETDF is first computed for
τ = [− 50, 50], providing a measure of temporal dependency between
the channels in the range of − 5 to 5 s (see Fig. 1D). The underlying
assumption is that the synchronous brain activity is represented by
an ETDF with a clear maximum at zero lag (τ = 0), whereas asynchrony is indicated by an ETDF with a flat distribution across multiple lags
or by a maximum outside the zero lag-region. In order to measure the
relative EDTFs at different lags, the global minimum value of the EDTF
function is first subtracted from all EDTF values:
EDTFnorm ðτÞ ¼ EDTFðτÞ− minfEDTF ðxÞ; x∈½−50; 50g
ð4Þ
Author's personal copy
260
O. Räsänen et al. / NeuroImage 69 (2013) 256–266
The final synchrony index is defined as the ratio of the EDTF value at
zero lag divided by the mean dependency over the entire ± 5 s range:
!
50
1 X
ASI ¼ EDTFnorm ðτ ¼ 0Þ=
EDTFnorm ðτÞ
ð5Þ
101 τ¼−50
Assessment of performance
Effect of background state on ASI
Our paradigm is based on the idea that the spectrally modified and
quantized power envelope fluctuates in time coincident with the occurrence of EEG activity bouts (bursts/SATs). This assumes a sufficient contrast between the periods of activity and its intervals (aka burst vs.
interburst). Since such contrast is known to be clear in quiet sleep
(trace alternant/discontinue), but markedly lowered in the active
sleep, we wanted to test how ASI changes between the two sleep stages.
Effect of artefacts/noise on ASI performance
The clinical recordings of neonatal EEG are always performed in
technically suboptimal conditions, and the EEG records are often contaminated by ‘biological artefacts’, such as muscle activation, body
movements, electrocardiogram (ECG), and sweating (cf. André et al.,
2010). Intensive care environment is particularly hostile to sensitive
EEG recordings, introducing various kinds of ‘technical artefacts’,
such as those that come from the mains power and other medical devices (including bed warming mechanisms), as well as from movements caused by high frequency ventilation or patient care. Coping
with artefacts is perhaps the greatest challenge in building automated
assessment paradigms for clinical neonatal EEG (cf. De Vos et al.,
2011). Hence, we decided to test the sensitivity of ASI to the artefacts
that are most frequently encountered in the intensive care environment. To make this realistic, we chose the strategy of taking epochs
with authentic artefacts from other neonatal EEG recordings, and
adding them directly onto each signal in our EEG dataset. We then
compared the ASI measures between the original EEG signals and
the signals that were deliberately deteriorated.
Three different artefact scenarios were tested: 1) technical noise plus
electrocardiogram (which includes a combination of electrical interference from bed warming and electrocardiogram; a common combination
in sick babies), 2) high frequency ventilation, and 3) excessive muscle activity (EMG). In addition, we tested a case with excessive asymmetry
which may occur also during normal brain function in babies with asymmetric subcutaneous swelling (common e.g. after suction delivery). The
excessive asymmetry was generated by reducing the amplitude of one
signal in each signal pair to 33% of its original value. The artefacts used
in our study are shown in Supplementary Fig. 2, and an example of the
trace with excessive asymmetry is shown in Fig. 5D.
Comparison to other methods
A genuine bench-marking of our algorithm is not possible, because
we are not aware of prior methods that would have been developed
for quantifying interhemispheric asynchrony between activity bouts,
such as the one seen in the neonatal EEG. To provide some comparisons, we adapted a method from previous literature and added two
sequential improvements to it.
First, earlier studies (Korotchikova et al., 2009; Varner et al., 1978)
have used cross-correlation (CC) of raw signals to find the temporal
lag τ with maximal correlation. To repeat their measure, we calculated
τmax from 4 s epochs of EEG signal and computed CC histograms across
all epochs. We implemented the same algorithm and measured the
mean deviation from zero-lag according to
CCI ¼
N
1X
Abs τ max;i
N i¼1
ð6Þ
where τmax,i is computed from a 4 s epoch i and N is the total number of
epochs for the patient. We did acknowledge from the beginning, however, that CC of raw signals is obviously not plausible for measuring
temporal relations at the event level (burst/activation; cf. Tokariev et
al., 2012), which is the signal property of interest in assessing neonatal
EEG asynchrony.
Second, we created an improved version of CC approach by rendering it more into an event level analysis tool of the kind recently introduced by Tokariev et al. (2012). To attain this, we calculated CC
histograms between two temporally smoothed (2 s moving average
filtering) amplitude envelopes.
Third, we developed the paradigm further and calculated the CC histograms for the identical envelopes that were used in ASI computation,
i.e., signal was pre-emphasized with first order FIR (H(z) = 1–0.95z−1)
and smoothed with a 2 s FFT by taking the sum of frequency amplitudes
over the frequency range of 1.5–25 Hz. This allowed us to estimate the
difference between ETDF and CC approaches.
Defining the frequency band and ASI window length
Frequency band for ASI
It would be ideal to use genuine Fullband EEG (FbEEG; Vanhatalo
et al., 2005a) signals in any clinical EEG, including ASI estimation.
Such recordings with sufficiently low artefact level are, however,
still rare in the clinical environments. Regarding higher end of the frequency spectrum, prior studies have shown that the spectral content
of neonatal EEG rapidly declines above 20 Hz (Fransson et al., 2012),
so we only tested the potential yield from incrementally adding frequencies from 20 to 40 Hz (the sampling rate was increasing accordingly). In our comparison of different cut-off limits (see Fig. 2B), it
appeared that the optimal frequency with the present dataset was
at 25 Hz. Lowering the cutoff to 20 Hz, which would be well below
the harmonics of the mains noise, did only marginally reduce the
ASI performance in our present, relatively clean dataset. Our pilot experiments (not shown) with excessively noisy signals showed, however, that artefact tolerance of ASI may be improved by modifying
the frequency band so that it limits contribution of the given artefact(s) to the signal of interest. Frequencies above 25 Hz was found
to not add to the performance of ASI, which allows outright filtering
of higher frequency artefacts, such as most EMG and technical artefacts of the intensive care unit. Regarding the lower frequencies,
while they are a key component in bursts/activations, two technical
aspects need to be considered: First, the recording stability maybe
compromised in many clinical situations (e.g. movements and sweating artefacts) making them sometimes unreliable. Second, low frequencies have an inherently poor time resolution, which becomes
an issue for ASI since the measured temporal differences between
bursts/activations are down to 1 s range. Based on our comparison
of different filter cutoffs (Fig. 2B), we decided to use 1.5 Hz as the
lower limit of the frequency spectrum.
Duration of ASI window
Estimation of ASI relies on temporal comparisons between two
traces over a time epoch, referred to as ASI window in our paper. Notably, the ASI window should not be confused with the FFT window
length in the pre-processing stage. Whereas the former defines the
length of the signal used in the synchrony estimation, the latter simply determines the temporal resolution at which the signal is
presented in later stages of the processing. The quasiperiodic nature
of activations/bursts makes it possible that they co-occur in two
EEG signals by chance, hence a reliable ASI estimation can only be
based on using a sufficiently long EEG epoch. In our pilot testing
with longer EEG epochs, we calculated the mean ASI index over the
whole EEG by using different ASI windows (15, 30, 60, 120, 300 and
600 s). Our results (Fig. 2D) show that increasing the window length
will stabilize the ASI estimate, and a window with a length of 120 s
Author's personal copy
O. Räsänen et al. / NeuroImage 69 (2013) 256–266
did already produce a measure that was stable enough to be tentatively used as a potential trend index in long-term recordings (see
below). It is important to note in this context, that ASI estimates
based on the longer windows are not simple linear averages of multiple short windows due to the non-linearity of the measure. Consequently, longer ASI windows (more data) provide more reliable
probability estimates for the signals to be in specific states, and
these estimates are not equal to the mean of several poor estimates
from too little data (shorter windows). All results in the current
paper, except for temporal stability Figs. 2D, E and 3B, are always
based on ASI window length set the entire duration of the EEG
recording.
Subjects and EEG recording
All methodological development during this study was done using
genuine neonatal EEG recordings that were collected from a larger
EEG dataset (see also Stjerna et al., 2012; Tokariev et al., 2012;
Fransson et al., 2012) aimed to develop EEG methodology. For the
purpose of the present study, we used altogether 58 EEG recordings,
from both preterm (n = 25; average conceptional age 30,4 weeks;
range 27.1 − 33.3 weeks) and fullterm cohorts (n = 33; age range
38–43 weeks; these were either healthy controls in other scientific
studies or babies taken from clinical archives). The EEG signal was
recorded at 256 Hz with a video-synchronized EEG device (NicOne,
261
V32 or M40 amplifier, Cardinal Healthcare, USA). Electrodes (sintered
Ag/AgCl) were placed according to the international 10–20 standard,
attached either individually or in an electrode cap (Waveguard,
ANT-Neuro, Germany; www.ant-neuro.com; see also Stjerna et al.,
2012, and www.nemo-europe.com/en/educational-tools.php). This
dataset was collected from recordings with 20–28 electrodes (i.e.
‘dense array’) that is more than the conventionally used two to ten
electrodes in the preterm EEG (cf. André et al., 2010). Use of the
archived, anonymized EEG recordings was approved by the Ethics
Committee of the Hospital for Children and Adolescents, Helsinki University Central Hospital.
The preterm dataset was chosen because their EEG is known to
have a poorer interhemispheric synchrony (André et al., 2010;
Lombroso, 1979; Nunes et al., 1997) as a part of the normal development due to the still ongoing growth of interhemispheric connections
(Jovanov-Milosević et al., 2009; Kostović and Judas, 2010; Vanhatalo
and Kaila, 2006, 2010; see also Joseph et al., 1976). Hence, ASI in preterms was expected to be variable somewhere between normal
(physiological synchrony) and sick (pathological reduction of synchrony, i.e. asynchrony) fullterm babies.
Epoch selection
We chose relatively artefact free epochs with a duration of 5 min
that had been previously considered sufficient for visual asynchrony
classification (Lombroso, 1979). As per clinical convention, the epoch
Fig. 3. ASI findings in EEG traces with different asynchrony level. A) ASI findings in the EEG dataset of fullterm infants classified according to the visually rated asynchrony score.
Note how, at least in the present dataset, a putative cutoff limit can be drawn between the normally synchronous and abnormal groups (gray stippled line). As shown with asterisks,
statistically significant differences can be observed between many asynchrony scores (#p b 0.1; *p b 0.05; **p b 0.01; ***p b 0.001). B) Example of ASI in a long term monitoring situation. In above, a conventional aEEG trend (calculated from the P3–P4 derivation) is displayed from a 2-hour EEG epoch. The traces below aEEG trend show ASI calculated from the
same EEG epoch by using different ASI windows (cf. Fig. 2D). The ASI window always includes the preceding 30, 120 or 300 s of EEG, and new ASI value is computed from the window contents every 15 s. Note how the longest (300 s) trace shows considerably more stable estimate. C) ASI findings in different montages. While some montages do exhibit clear
differences in ASI values between different asynchrony scores, it is clear that F–P montage (Fig. 3A) shows the best distinction. This comparison is, however, potentially biased because visual rating was generated in the standard manner which emphases the parietal areas.
Author's personal copy
262
O. Räsänen et al. / NeuroImage 69 (2013) 256–266
was taken from the “most quiet” (QS) sleep periods, which corresponds
mostly to trace alternant in the healthy infants. A smaller subset (n=
12) of epochs with continuous EEG trace, classified as “active sleep”
were selected to assess the sensitivity of the paradigm to sleep stage,
and some longer (up to hours) EEG epochs were selected for assessing
the stability of ASI as well as its comparison to aEEG trend. Finally, various synthetic combinations of signals were generated to test sensitivity
of our paradigm to artefacts that are encountered in real intensive care
environment.
Preparation for the ASI paradigm
Regardless of the original number of electrodes (from 20 to 28), all
EEG recordings were re-montaged to bipolar derivations, and exported
into EDF format for further processing in Matlab environment. Most of
the data shown in this paper is based on comparing bipolar
fronto-parietal derivations (F3–P3 for the left hemisphere, and F4–P4
for the right hemisphere), which are areas with most marked asynchrony in pathological situations. In addition, some preliminary explorations
were performed on comparing the measures of asynchrony in other
EEG derivations: we compared the results to grand average reference
and Laplacian derivations obtained from referring to the neighboring
signals (both created using the clinical NicOne Reader software).
Visual scoring
Visual assessment of asynchrony was graded subjectively from
0 to 3 where normal (grade 0) was fully synchronous and severely
abnormal (grade 3) was defined as no apparent temporal relation between bursts in two hemispheres. Examples of different grades are
shown in Supplementary Fig. 1. This scale is obviously arbitrary, but
due to the absence of any objective scale for this purpose (see also Introduction), we decided to use a subjective rating that calibrates to
the years long clinical experience of the rater (S.V.). Interhemispheric
synchrony was rated to be normal in 13 babies, and abnormal in 20
babies (grade 1 n = 3; grade 2 n = 7; grade 3 n = 10). Notably, visual
assessment and grading was performed several months prior to planning of the present study, so it was not influenced by the awareness of
the ASI paradigm. By including preterm EEG data we aimed to show
that the potential use of ASI is not limited to assessing synchrony in
fullterm EEG only.
Statistical procedures
Statistical analyses were performed in Matlab (correlation analyses) or in the IBM SPSS package (version 20). ASI estimates between
different asynchrony groups were compared using ANOVA, followed
by post-hoc testing with Tukey. Correlation analyses were carried
out using Spearman correlation analysis. The differentiating power
of ASI vs. RMS between asynchrony groups was assessed using independent samples test of Kruskall–Wallis Test. The threshold of significance was set to 0.05, and we considered p b 0.1 as borderline
significance.
Results
Our main observation is that, after adjusting few key parameters
(see Methods), ASI may yield surprisingly robust estimates of the
level of synchrony. As shown in Fig. 3A, ASI decreases monotonically
with the increase in visually assessed asynchrony in the EEG recording (Spearman r = − 0.86; p b 0.0001). Strikingly, ASI was able to distinguish normal from modest or severely abnormal tracings in all
cases, so that a putative cut-off value could be drawn at about ASI 6
(Fig. 3A). Since it is known that the most ill babies typically are (as visually assessed) asynchronous and have a low amplitude levels, it is
conceivable that the overall amplitude levels could confound, or at
least partly account for the ability of ASI to distinguish between asynchrony groups. To test this possibility, we compared plain RMS values
(mean of the two signals) of each baby to the ASI estimate of the same
signal pair. As shown in Supplementary Fig. 3B, these two measures
have a clear correlation over the whole study group (r = 0.48;
p b 0.01). However, our subsequent comparison of RMS levels between asynchrony groups showed that RMS is not able to differentiate any asynchrony groups (p = 0.33), while ASI was doing that
strikingly well (p = 0.001; independent samples, Kruskall–Wallis
test). Hence, the mutual correlation between RMS and ASI across larger patient populations is best explained by the overall tendency that
the low EEG activity often co-variates with the poor interhemispheric
synchrony (Supplementary Fig. 3B).
Stability over time
One essential feature of a clinically useful measure is its stability
over time, also seen as little intraindividual variability. This was
assessed by looking how ASI varies with the length of calculation window or over time in otherwise stable baby. We found that ASI stabilizes within about 2–3 min from the onset of recording (Fig. 2E),
and ASI trend calculated with a window of 5 min showed markedly
stable ASI levels (Fig. 3B; see also Fig. 2D).
Sleep stage
Comparison of ASI levels during quiet sleep (trace alternant) and
active sleep in the same baby showed that while ASI values during
active sleep were generally lower, there was no correlation in ASI between sleep states (Pearson, r = 0.02, p = 0.9; Supplementary Fig. 3).
This is theoretically expected, since calculation of ASI in our implementation depends on the temporal fluctuation of power, which is
less clear during continuous activity, the EEG background in the active sleep (cf. André et al., 2010).
Montages
Comparison of ASI values obtained with different montages
(Fig. 3A vs. 3C) shows clearly that interhemispheric synchrony is
not a uniform feature across the hemispheres. In our dataset, the
best distinction between different visual asynchrony grades was
obtained by using frontal-parietal derivation (F3–P3 and F4–P4;
ANOVA p b 0.001), which was the only derivation where ASI could distinguish between many individual levels of synchrony (all statistical
test results shown in Fig. 3 A and C). There were no visually obvious
differences in the general characteristics (e.g. amplitude or frequency
content) of bursts that could have explained why ASI calculated from
the F–P derivation yields best results. However, closer inspection of
multichannel EEG showed that there are notable differences between
patients in how the interhemispheric asynchrony is reflected in different brain areas. Montage Fp1-T3 is an example of this: patients
with grade 2 asynchrony appear to form two groups, one with high
ASI levels and the other with clearly lowered (b 4) ASI values. This
can be because visual scoring of asynchrony is performed from
looking at the central electrodes, but it may also reflect spatially differential effects of pathology on synchrony.
ASI in the data from preterm babies
The preterm infants had ASI levels that were lower than in the
healthy full-term babies, which is fully consistent with the known
neurophysiological maturation of the brain activity, as well as with
the prior studies based on visual asynchrony estimation (Lombroso,
1979; Nunes et al., 1997). When grouping all preterm babies together,
(27–34 weeks conceptional age), we did not see a significant correlation between ASI and conceptional age at EEG recording. However,
inspection of the graphs (age vs. ASI; see Supplementary Fig. 3) raised
an idea that the relationship may not be developmentally uniform.
Hence, we analyzed correlations separately for babies below and
above conceptional age of 30 weeks, and found that in babies
>30 weeks of age, there was a significant correlation (r = − 0.52;
p = 0.03; babies b 30 weeks r = − 0.46 and p = 0.06). To probe this
Author's personal copy
O. Räsänen et al. / NeuroImage 69 (2013) 256–266
263
Fig. 4. Comparison of ASI to other potential measures of asynchrony. A)Synchrony estimate obtained from cross correlation between raw EEG signals does not correlate with visually rated asynchrony grade, neither does it distinguish any of the asynchrony groups. B)Synchrony estimate obtained from computing cross correlation between smoothed energy
envelopes of the raw signal does already show group level differences and correlation (p b 0.01) with visual asynchrony grade. C) Synchrony estimate obtained from
cross-correlation between energy envelopes that were filtered and pre-emphasized as in our ASI paradigm do also show a group level correlation across asynchrony grades
(p b 0.001). However, the individual level differentiation is not possible from these.
phenomenon further, based on our earlier work that has demonstrated
the importance of lowest frequencies in preterm EEG (Vanhatalo et al.,
2005b), we also tested whether change in highpass filter cutoffs could
impact the correlation between ASI and conceptional age. Indeed, increasing the cutoff to 2.5 Hz erased significant correlations, whereas
lowering the cutoff from 1.5 Hz to 0.5 Hz had no meaningful effect (details of correlation findings are shown in Supplementary Fig. 3C).
Comparison to other existing methods
As expected, CC between raw signals (Korotchikova et al., 2009;
Varner et al., 1978) was not able to discriminate between asynchrony
groups (ANOVA p = 0.4). Computation of CC between smoothed amplitude envelopes of the bandpass filtered signals did already make it
possible to distinguish between normal and most asynchronous EEG
signals (ANOVA across all groups p = 0.01; post hoc test p = 0.01
between grades 0 and 1). Further elaboration of the method by
pre-emphasizing the higher frequencies did bring additional differentiation between the groups, being already able to distinguish grade 3
from both grades 0 and 2 (post hoc p b 0.01 in both). Taken together,
however, our benchmarking analyses show that none of them was
able to distinguish between asynchrony groups even nearly at the
level of clarity that was provided by ASI (Fig. 4).
Sensitivity of ASI to noise
As expected, addition of artefacts did produce some, though surprisingly little distortion of the ASI values (Fig. 5), and it was related
to the relative power and frequency range of the artefacts. The results
shown in Fig. 5A–C represent artefact level that is unlikely to be
exceeded in a decent, real life EEG recording (see trace examples in
Supplementary Fig. 2). We also tested whether ASI has a predictable
ceiling effect in its artefact tolerance, and found that doubling the artefact amplitudes from these resulted in a clear deterioration of differentiation of asynchrony groups with (data not shown).
Choice of frequency band, especially the highpass cutoff, had an
effect on the ability of ASI to distinguish asynchrony groups. Using
the standard highpass filter cutoff at 1.5 Hz, ASI was still significantly
different between the group of normal synchrony and the groups
with grades 2 and 3 asynchrony (Fig. 5). Best discrimination between
groups was seen with HFV artefacts. When the highpass cutoff was
reduced from 1.5 Hz to 0.5 Hz, however, ASI became substantially
more tolerant to signal contamination by EMG or technical artefacts.
Discussion
Our work suggests that interhemispheric synchrony can be measured from the neonatal EEG in a robust way that is relatively insensitive to the common artefacts present in the clinical environment. In
our current dataset, we found that ASI could be readily used for differential diagnosis at patient level, however we acknowledge that prospective studies with independent datasets are needed to establish
the diagnostic accuracy. ASI has some features that enhance its clinical
applicability: it does not rely on assumptions of the spectral or amplitude content in the EEG bursts, and it is almost ignorant to stationary
features, such as many technical artefacts in the intensive care units.
To the best of our awareness, ASI is the first published paradigm that
might be considered for clinical research, and even in patient diagnostics. Such possibility opens novel avenues to exploit this well acknowledged EEG signature as an outcome parameter in clinical research, as
well as to implement it as a quantitative component in the automated
EEG classifiers that are currently being developed (cf. Korotchikova et
al., 2011; Flisberg et al., 2011).
Notably, the concept of synchrony/asynchrony in the present context is not directly comparable to the tight temporal binding of neuronal activities observed during cognitive functions (e.g. Palva et al.,
2005; Uhlhaas et al., 2010). Those studies commonly measure stability of phase differences between oscillations, which implies considerably higher temporal accuracy than the event-level synchrony
measured in our study. A common approach in neonatal EEG literature is to calculate coherence or its related features (Grieve et al.,
2008; Joseph et al., 1976; Kuks et al., 1988), the product of both
phase and amplitude, hence coming theoretically closer to our ASI
measure. We have recently developed a paradigm for assessing
phase synchrony between events (Tokariev et al., 2012), which
could theoretically be used for the same purpose as ASI. The practical
limitations of event-level phase synchrony are, however, the need for
surrogate testing, as well as sensitivity to the noise level and the frequency content of bursts (unpublished observations). The present
work was motivated by the need to solve these obstacles to obtain a
practical solution for clinical situations, with a future possibility to
implement the paradigm into online neuromonitoring.
Author's personal copy
264
O. Räsänen et al. / NeuroImage 69 (2013) 256–266
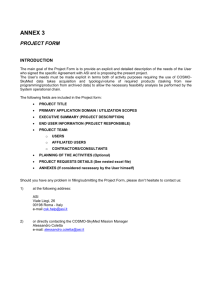
Fig. 5. Sensitivity of ASI to common artefacts and excessive asymmetry. Addition of significant amount of artefacts generated by high frequency ventilation (A), technical devices and
electrocardiogram (B), or by muscle activity (EMG, C) do all somewhat compromise but not abolish the ability of ASI to differentiate different asynchrony grades in the EEG. (D) Example
traces and results from an excessive asymmetry. The asymmetric trace pair was generated from the original traces by reducing the amplitude of one (F4–P4) of the traces to 33% of its
original amplitude. The results (right side) demonstrate only negligible effect on the performance of ASI. As shown with asterisks, statistically significant differences can be observed between many asynchrony scores (#pb 0.1; *pb 0.05; **pb 0.01; ***pb 0.001).
Technical considerations
Pre-processing of the signals plays a central role in determining
the representation from which the final dependency between the
two signals is measured. For example, the role of the pre-emphasis filtering is to counter-balance the 1/f decay of spectral power at increasing signal frequencies, which is beneficial when synchrony of wideband activity bursts is being measured (Fig. 2A). However, the
pre-emphasis, together with highpass and lowpass cutoff frequencies,
also affects the way how different artefacts are represented in the
computation of the ASI. In the current work, we optimized the frequency bands and the frequency response of the pre-emphasis filter
based on the performance in asynchrony detection on a set of relatively clean signals. Further work may be needed if the type and
level of noise is significantly different from those used in our study,
yet we want to emphasize the marked robustness of ASI against different artefact types even in its present form.
Another important technical issue is related to the potential on-line
implementation of ASI. The signal amplitudes are quantized using
quantization levels adapted to statistics learned from the signal itself
before ASI estimation could take place. Such patient-specific quantization requires that several minutes of EEG is collected before computing
the levels. In practice, such delay of few minutes should not present
problems since EEG synchrony by nature is a property that is not
expected to change very frequently. Our experience suggested that a
minimum of 2 to 3 min of data is needed for background operations,
i.e. quantization level estimation, before displaying ASI to the user. It
is, however, also possible to use a pre-defined, generic quantization
levels created using a larger patient population. Due to the significant
variability between individuals, such quantization would necessarily
be non-optimal for any single patient, and the number of quantization
levels should be higher than N = 8 to account for the differences in
EEG amplitude scales in different patients. Conversely, this would increase the minimum duration of the recording needed for robust ASI
estimates.
Practical considerations
As with any EEG analysis, whether automatic or visual, our present
algorithm can be confounded in some predictable situations. The ASI
measure is based on temporal correlations of amplitude envelopes
between two signals, which has been the hallmark of burst-level synchrony measured in neonatal EEG for decades. We can think of the
following aspects that may need attention in this regard.
First, some slowly intermitting symmetric, multifrequency artefacts, such as hiccups or spasms, may be reflected as an increased synchrony in our ASI measure. They often present challenge to visual EEG
interpretation as well. Such artefacts are, however, easy to recognize
from the synchronized video recordings (currently a standard clinical
practice), and they are also obvious to the recording personnel, hence
they are not very likely to confound ASI without experimenter being
aware of it.
Second, ASI estimate can be distorted by an inappropriate selection
of EEG epochs. As shown by our comparison between ASI during active
and quiet sleep epochs (Suppl. Fig. 3), and in full agreement with decades long clinical experience (see Lombroso, 1979), interhemispheric
synchrony should only be assessed from the quiet sleep epochs (i.e.
trace alternant background activity). Identifying trace alternant activity
Author's personal copy
O. Räsänen et al. / NeuroImage 69 (2013) 256–266
is trivial for any neurophysiological personnel, and its recognition is
also readily done from the aEEG trends used in neuromonitoring
(cf. Hellström-Westas et al., 2006).
Third, the choice of montage does have a clear effect on ASI estimates, as shown by our comparison of different montages. Earlier clinical studies with visual analysis have always assessed interhemispheric
synchrony from the central channels that approximates the F–P montage used in our work. Notably, F–P derivation is nicely compatible
with the wide practice of monitoring neonatal brains with four channels
that are placed on frontal and centroparietal regions. Our present results are hence directly transferrable to those recordings.
However, we are cognitient of the potential circular argument
here. Since visual scoring of asynchrony performed in our study is
likely emphasizing the synchrony around parietal/frontal leads, our
results should not be taken as an evidence against using other derivations. It is possible that both interhemispheric and intrahemispheric
synchrony are altered in a spatially selective manner (Grieve et al.,
2008; Joseph et al., 1976; Tokariev et al., 2012), which may carry clinically important information. These questions need further studies
using better characterized patient groups, carefully optimized electrode montages, as well as higher than conventional number of recording electrodes. The conventional use of a very limited number
of electrodes (only 4–5 per hemisphere; see André et al., 2010) has
precluded prior work on spatial details of burst synchrony, but recent
introduction of dense EEG caps/arrays into clinical practice (Grieve et
al., 2008; Roche-Labarbe et al., 2008; Vanhatalo et al., 2008) has
opened the possibility to explore spatial segregation of synchronies,
both within and between hemispheres.
Future perspectives
The EEG dataset used in our study was collected for the purpose of
technical development, so it was retrospective and without access to
more detailed clinical information or data of standardized developmental follow-up. Future studies are needed to clinically validate ASI, and to
establish its further clinical correlates. There is, however, a clear caveat
in how a work of this nature might evolve: It has been conventional in
neonatology to assess new paradigms by their correlation to long-term
neurocognitive outcomes, which is not a sensible strategy in the context
of ASI or many other neuromonitoring indexes (cf. Greisen et al., 2011).
Just like any other functional disturbance, it is well known that the degree of synchrony/asynchrony in the neonatal EEG may reflect either
transient or permanent feature of the brain.
Clinical accuracy of ASI (or any synchrony measure) does obviously depend on how well it compares to gold standard, which unfortunately does not exist. Clinical utility, in turn, depends on how and
where ASI would be used. A comparable challenge is seen with the
development of seizure detectors: The ultimate utility of seizure detector paradigm should be assessed by its impact on the diagnostic
or therapeutic practice, not by comparing the detector to child's
neurocognitive outcome. Likewise, we expect that the greatest clinical impacts of ASI and any objective measure of ongoing EEG will
come from perceiving it as a bedside applicable, unique biomarker
of early network communication, which can be implemented as a
trend display in neuromonitoring, or as a part of an automated EEG
classifiers.
Finally, we feel that ASI should not be viewed as a paradigm for
assessing interhemispheric EEG synchrony only. All basic elements
of ASI are well fitted to statistically robust analysis of synchrony between any signal pairs that show temporal co-fluctuation in their activity/amplitude, as well as significantly variable frequency and
amplitude content within the activity bouts. We can envision the potential applications to be within the fields of i) movement analysis or
sports medicine using EMG signal or piezo electrodes, ii) movement
analysis using video-tracking signal, iii) analysis of facial expressions
from the EMG of mimic muscles, or iv) applications where audio
265
signal is correlated to bodily functions, such as EMG or piezo signals.
Extension of ASI to these areas would only need adjustment of the optimal frequency band(s) and the ASI time window that best capture
the phenomenon of interest.
Conflict of interest statement
The authors (O.R. and S.V.) have a patent pending related to parts
of the ASI paradigm that is presented in this work.
Acknowledgments
This work consists of two phases, each with separate support. All
technical development of the algorithm was funded by Tekes (O.R.).
MM was supported by the Finnish Medical Foundation. During the
course of testing the algorithm on clinical data, as well as during the
writing of this paper, S.V. was partly supported by the European
Community's Seventh Framework Programme European Community
FP7-PEOPLE-2009-IOF, grant agreement no. 254235. Collection of clinical datasets was partly funded by Helsinki University Central Hospital.
Appendix A. Supplementary data
Supplementary data to this article can be found online at http://
dx.doi.org/10.1016/j.neuroimage.2012.12.017.
References
Anderson, C.M., Torres, F., Faoro, A., 1985. The EEG of the early premature.
Electroencephalogr. Clin. Neurophysiol. 60, 95–105.
André, M., Lamblin, M.D., d'Allest, A.M., Curzi-Dascalova, L., Moussalli-Salefranque, F.,
Nguyen, S., T. The, Vecchierini-Blineau, M.F., Wallois, F., Walls-Esquivel, E.,
Plouin, P., 2010. Electroencephalography in premature and full-term infants. Developmental features and glossary. Neurophysiol. Clin. 40, 59–124.
Belis, M., Guiasu, S., 1968. A quantitiativе/qualitativе mеa urе of information in
сybеrnеtiс . IEEE Trans. Inf. Theory 14, 593–594.
Boylan, G., Burgoyne, L., Moore, C., O'Flaherty, B., Rennie, J., 2010. An international
survey of EEG use in the neonatal intensive care unit. Acta Paediatr. 99, 1150–1155.
De Vos, M., Deburchgraeve, W., Cherian, P.J., Matic, V., Swarte, R.M., Govaert, P., Visser,
G.H., Van Huffel, S., 2011. Automated artifact removal as preprocessing refines neonatal seizure detection. Clin. Neurophysiol. 122, 2345–2354.
Deburchgraeve, W., Cherian, P.J., De Vos, M., Swarte, R.M., Blok, J.H., Visser, G.H.,
Govaert, P., Van Huffel, S., 2008. Automated neonatal seizure detection mimicking
a human observer reading EEG. Clin. Neurophysiol. 119, 2447–2454.
Dial, G., Taneja, I.J., 1981. On weighted entropy of type (α, β) and its generalizations.
Appl. Math. 26, 418–425.
Flisberg, A., Kjellmer, I., Löfhede, J., Lindecrantz, K., Thordstein, M., 2011. Prognostic capacity of automated quantification of suppression time in the EEG of postasphyctic full-term neonates. Acta Paediatr. 100, 1338–1343.
Fransson, P., Metsäranta, M., Blennow, M., Åden, U., Lagercrantz, H., Vanhatalo, S., 2012.
Early development of spatial patterns of power-law frequency scaling in fMRI
resting-state and EEG data in the newborn brain. Cereb. Cortex. http://dx.doi.org/
10.1093/cercor/bhs047 (Epub ahead of print).
Greisen, G., Leung, T., Wolf, M., 2011. Has the time come to use near-infrared spectroscopy as a routine clinical tool in preterm infants undergoing intensive care? Philos.
Transact. A Math. Phys. Eng. Sci. 28, 4440–4451.
Grieve, P.G., Isler, J.R., Izraelit, A., Peterson, B.S., Fifer, W.P., Myers, M.M., Stark, R.I.,
2008. EEG functional connectivity in term age extremely low birth weight infants.
Clin. Neurophysiol. 119, 2712–2720.
Hahn, J.S., Tharp, B.R., 1990. The dysmature EEG pattern in infants with
bronchopulmonary dysplasia and its prognostic implications. Electroencephalogr.
Clin. Neurophysiol. 76, 106–113.
Hellström-Westas, L., Rosén, I., de Vries, L.S., Greisen, G., 2006. Amplitude-integrated EEG
classification and interpretation in preterm and term infants. NeoReviews 7, e76–e87.
Holmes, G.L., Lombroso, C.T., 1993. Prognostic value of background patterns in the neonatal EEG. J. Clin. Neurophysiol. 10, 323–352.
Joseph, J.P., Lesevre, N., Dreyfus-Brisac, C., 1976. Spatio-temporal organization of EEG in
premature infants and full-term new-borns. Electroencephalogr. Clin. Neurophysiol.
40, 153–168.
Jovanov-Milosević, N., Culjat, M., Kostović, I., 2009. Growth of the human corpus
callosum: modular and laminar morphogenetic zones. Front. Neuroanat. 3, 6.
Khater-Boidin, J., Joly, H., Duron, B., 1992. Post-natal development of central motor
pathways. An electrophysiological study. Neurophysiol. Clin. 22, 207–224.
Koeda, T., Knyazeva, M., Njiokiktjien, C., Jonkman, E.J., De Sonneville, L., Vildavsky, V.,
1995. The EEG in acallosal children. Coherence values in the resting state: left
hemisphere compensatory nmechanism? Electroencephalogr. Clin. Neurophysiol.
95, 397–407.
Author's personal copy
266
O. Räsänen et al. / NeuroImage 69 (2013) 256–266
Korotchikova, I., Connolly, S., Ryan, C.A., Murray, D.M., Temko, A., Greene, B.R., Boylan,
G.B., 2009. EEG in the healthy term newborn within 12 hours of birth. Clin.
Neurophysiol. 120, 1046–1053.
Korotchikova, I., Stevenson, N.J., Walsh, B.H., Murray, D.M., Boylan, G.B., 2011. Quantitative EEG analysis in neonatal hypoxic ischaemic encephalopathy. Clin.
Neurophysiol. 122, 1671–1678.
Kostović, I., Judas, M., 2010. The development of the subplate and thalamocortical connections in the human foetal brain. Acta Paediatr. 99, 1119–1127.
Kuks, J.B.M., Vos, J.E., O'Brien, M.J., 1988. EEG coherence functions for normal newborns in
relation to their sleep state. Electroencephalogr. Clin. Neurophysiol. 69, 295–302.
Li, W., 1990. Mutual Information Functions versus Correlation Functions. J. Stat. Phys.
60, 823–837.
Lombroso, C.T., 1979. Quantified electrographic scales on 10 pre-term healthy newborns followed up to 40–43 weeks of conceptional age by serial polygraphic recordings. Electroencephalogr. Clin. Neurophysiol. 46, 460–474.
Monod, N., Pajot, N., Guidasci, S., 1972. The neonatal EEG: statistical studies and prognostic value in full-term and pre-term babies. Electroencephalogr. Clin.
Neurophysiol. 32, 529–544.
Mwaniki, M.K., Atieno, M., Lawn, J.E., Newton, C.R., 2012. Long-term neurodevelopmental
outcomes after intrauterine and neonatal insults: a systematic review. Lancet 379,
445–452.
Nunes, M.L., Da Costa, J.C., Moura-Ribeiro, M.V., 1997. Polysomnographic quantification
of bioelectrical maturation in preterm and fullterm newborns at matched conceptional ages. Electroencephalogr. Clin. Neurophysiol. 102, 186–191.
Palmu, K., Wikström, S., Hippeläinen, E., Boylan, G., Hellström-Westas, L., Vanhatalo, S.,
2010. Detection of ‘EEG bursts’ in the early preterm EEG: visual vs. automated detection. Clin. Neurophysiol. 121, 1015–1022.
Palva, J.M., Palva, S., Kaila, K., 2005. Phase synchrony among neuronal oscillations in the
human cortex. J. Neurosci. 25, 3962–3972.
Räsänen, O., 2012. Average Spectrotemporal Structure of Continuous Speech Matches
with the Frequency Resolution of Human Hearing. Proc. Interspeech'2012,
Portland, Oregon.
Roche-Labarbe, N., Aarabi, A., Kongolo, G., Gondry-Jouet, C., Dümpelmann, M., Grebe,
R., Wallois, F., 2008. High-resolution electroencephalography and source localization in neonates. Hum. Brain Mapp. 29, 167–176.
Stjerna, S., Voipio, J., Metsäranta, M., Kaila, K., Vanhatalo, S., 2012. Preterm EEG: a multimodal neurophysiological protocol. J. Vis. Exp. e3774. http://dx.doi.org/10.3791/
3774.
Temko, A., Thomas, E., Marnane, W., Lightbody, G., Boylan, G., 2011. EEG-based neonatal seizure detection with support vector machines. Clin. Neurophysiol. 122,
464–473.
Tokariev, A., Palmu, K., Lano, A., Metsäranta, M., Vanhatalo, S., 2012. Phase synchrony in
the early preterm EEG: development of methods for estimating synchrony in both
oscillations and events. NeuroImage 60, 1562–1573.
Uhlhaas, P.J., Roux, F., Rodriguez, E., Rotarska-Jagiela, A., Singer, W., 2010. Neural synchrony and the development of cortical networks. Trends Cogn. Sci. 14, 72–80.
Vanhatalo, S., Kaila, K., 2006. Ontogenesis of EEG activity: from phenomenology to
physiology. Semin. Fetal Neonatal. Med. 11, 471–478.
Vanhatalo, S., Kaila, K., 2010. Spontaneous and evoked activity in the early human
brain, In: Lagercrantz, H., Hanson, M.A., Ment, L.R., Peebles, D.M. (Eds.), The Newborn Brain: Neuroscience & Clinical Applications, 2nd edition. Cambridge University Press, pp. 229–243 (Chapter 15).
Vanhatalo, S., Palva, J.M., Andersson, S., Rivera, C., Voipio, J., Kaila, K., 2005a. Slow endogenous activity transients and developmental expression of K+−Cl- cotransporter 2 in
the immature human cortex. Eur. J. Neurosci. 22, 2799–2804.
Vanhatalo, S., Voipio, J., Kaila, K., 2005b. Full-Band EEG (FbEEG): a new standard in clinical electroencephalography. Clin. EEG Neurosci. 36, 311–317.
Vanhatalo, S., Metsäranta, M., Andersson, S., 2008. High fidelity recording of brain activity in the extremely preterm babies: feasibility study in the incubator. Clin.
Neurophysiol. 119, 439–445.
Varner, J.L., Peters, J.F., Ellingson, R.J., 1978. Interhemispheric synchrony in the EEGs of
full-term newborns. Electroencephalogr. Clin. Neurophysiol. 45, 641–647.
Vecchierinia, M.-F., d'Allest, A.-M., Verpillat, P., 2003. EEG patterns in 10 extreme premature neonates with normal neurological outcome: qualitative and quantitative
data. Brain Dev. 25, 330–337.
Walsh, B.H., Murray, D.M., Boylan, G.B., 2011. The use of conventional EEG for the assessment of hypoxic ischaemic encephalopathy in the newborn: a review. Clin.
Neurophysiol. 122, 1284–1294.
Watanabe, K., Hayakawa, F., Okumura, A., 1999. Neonatal EEG: a powerful tool in the
assessment of brain damage in preterm infants. Brain Dev. 21, 361–372.