Vulnerability to stress and psychopathology among third year
INTERNATIONAL JOURNAL OF
CLINICAL NEUROSCIENCES
AND
MENTAL HEALTH
ORIGINAL RESEARCH
Vulnerability to stress and psychopathology among third year medical students
João Gama Marques
1
, Daniel Machado
1
, Sílvia Ouakinin
1
, and Maria Luísa Figueira
1
Abstract
Background: Some studies describe high prevalence of psychological disturbances among 3rd year medical students.
The specific nature of factors like perceived stress, medical identity formation, and psychodynamic features are usually pointed as responsible for triggering factors of emotional disturbances but there is resistance among medical student to search for help. The objective of the study was to assess stress vulnerability and psychopathology risk among 3rd year medical students in Portugal.
Methods: The authors conducted a cross-sectional, survey of medical students at the biggest Portuguese medical school, through an anonymous self-report questionnaire, including sociodemographic data, psychiatric history illness, plus stress vulnerability, with 23 Questions on Vulnerability to Stress (23QVS), and psychopathology, with Symptom
Checklist 90 Revised (SCL-90-R).
Results: A 56% response rate was obtained among 228 students (70.1% women), with mean age of 20.82+1.27 years
(mean ± standard deviation). Main stress factor was academic issues (50%), with female being more vulnerable than male. Stress vulnerability’s mean value was 33.88 ± 9.28 (cut-off point 23QVS > 43) and SCL90R’s Global Severity Index mean value was 0.389 (cut-off point SCL-90-R > 1.5). In a subsample of 24 students, with levels of stress vulnerability above cut-off point (23QVS > 43), a positive correlation was found with interpersonal sensitivity (r=0.517; p=0.1), depression (r=0.497; p=0.13), phobic anxiety (r=0.443; p=0.03), psychoticism (r=0.427; p=0.038) and SCL-90-R’s Global Severity
Index (r=0.47; 0.02).
Conclusion: Low mean values for stress vulnerability and psychopathology were found, and among vulnerable subjects, there was a strong correlation between both dimensions.
Keywords: Stress, Psychopathology, Medicine, Students.
1 University Clinic of Psychiatry and Psychology, Faculty of Medicine, University of Lisbon, Lisboa, Portugal
Citation: Marques et al. Vulnerability to stress and psychopathology among third year medical students. IJCNMH 2015; 2:3
Correspondence: João Gama Marques
Clínica Universitária de Psicologia e Psiquiatria, Faculdade de Medicina,
Universidade de Lisboa
Avenida Egas Moniz, 1649-028 Lisboa, Portugal
Email address: joaogamamarques@gmail.com
Received: 07 Jan 2015; Accepted: 04 Jun 2015; Published: 29 Jun 2015
Open Access Publication Available at http://ijcnmh.arc-publishing.org
© 2015 Marques et al. This is an open access article distributed under the Creative Commons
Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
2 Stress and psychopathology in medical students
Introduction
Some studies describe an especially high prevalence of psychological disturbances among medical students, namely in the 3 rd year [1], with stress decreasing in the following years of medicine school [2]. This tendency has already been described before, in a small Portuguese medical school
[3], but has not been generalized to other medical schools in our country, where the 3 rd year is the most demanding, both in theoretical and practical classes. The specific nature of factors like perceived stress, medical education, professional practice, and psychodynamic features that lead individuals to the medical career are usually pointed as responsible for triggering factors of emotional disturbances, but unfortunately there is, whenever necessary, a huge resistance among medical student to seek help [4].
The objective of this study is to evaluate vulnerability to stress in 3 rd year medical students, identifying potential risk groups, and correlating these to general psychopathology.
A value higher than 1.5 obtained in the filling of the
SCL-90-R represents one cut-off point above which there is psychopathology. Out of the various available forms of inquiries, we opted for “paper and pen” and the test scoring was obtained manually, using a key. Results are presented in 9 Dimensions of Primary Symptoms, namely SOM =
Somatization; O-C = Obsessive-Compulsive; I-S = Interpersonal-Sensitivity; DEP = Depression; ANX = Anxiety;
HOS = Hostility; PHOB = Phobic Anxiety; PAR = Paranoid
Ideation; and PSY = Psychoticism. There are still 3 global indexes, GSI = Global Severity Index which measures the general psychological disturbance: PSDI = Positive Symptom Distress Index that defines the intensity of the symptoms; and PST = Positive Symptom Total, which concern the number of reported symptoms.
Statistical analysis was performed using SPSS v.14 and included descriptive frequency analysis, comparison of means (t-Student, Mann-Whitney, as appropriate) and correlations (R 2 Linear), using 95% confidence intervals.
Methods Results
The survey was approved by the ethical board of the Faculty of Medicine of the University of Lisbon, Lisbon, Portugal. It included a semi-structured written interview including sociodemographic, biographical data, questions on social, familiar and sexual aspects, and questions on drug and medication use.
There was also a closed-ended question regarding plausible origin or nature of stressful event: “Did you have a main stressful event in last trimester?”, with four possible categorical answers: “Academic”, “Family”, “Health”, and/ or “Economic” related issues.
Besides that, there was a scale to evaluate vulnerability to stress, 23 Questions on Vulnerability to Stress, 23QVS
[5] and a psychopathology inventory, Symptom Checklist
90 Revised, SCL-90-R [6].
The 23QVS questionnaire is a Likert-type scale, rated from “totally agree” to “totally disagree”, composed of
23 questions destined for evaluation of vulnerability to stress. It includes 7 factors: F1, Perfectionism and intolerance to frustration; F2, Inhibition and functional dependence; F3, Lack/Need of social support; F4, Adverse life conditions; F5, Dramatization of existence; F6, Subjugation; and F7, Deprivation of affection and rejection. A value higher than 43 obtained in the filling of the 23QVS represents one cut-off point above which there is vulnerability to stress.
The SCL-90-R was created to detect psychopathological symptoms. This instrument is useful for evaluating patients before, during, or after treatment, in order to help understanding their evolution. The SCL-90-R is used by clinical psychologists and psychiatrists in such areas as mental health, education, and investigation. It is an inventory composed of 90 Likert-type questions, varying from
“Never” to “Extremely”.
Out of 228 students, 127 completed questionnaires, representing a 55.7% response rate. Most (70.1%) were females, and age ranged from 19 to 27 years old, with a mean (± standard deviation) value of 20.82±1.27. The prevalence of gender of our sample was not significantly different from the complete universe of students. Most (59.9%) were living with family, more than half (57.9%) were not in a stable affective relationship and almost half (48.7%) had no previous sexual experience. Regarding life style the most used substance was alcohol (34.6%). The more important demographic data can be found in Table 1.
When asked about the origin or nature of any stressful event in the last 3 months only one fourth (24.6%) answered negative. The most common stress factor, in the last three months, was academic issues (50%).
Globally the 23QVS and SCL-90-R results were below cut-off points. We found 15.5% students highly vulnerable to stress (QVS>43) and 3.1% students with serious psychopathology (GSI SCL-90-R>1.5). Specifically there was a 23QVS mean value of 33.88 ± 9.28 (below cut-off point 43), and a GSI SCL-90-R mean value of 0.74±0.39
(below cut-off point 1.5).
There were no significant differences between genders, except for 23QVS F3 Lack/Need of social support, that was higher in female students (f=3.16; p<0.002).
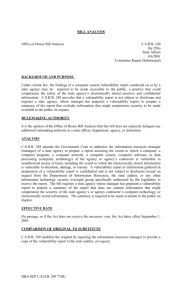
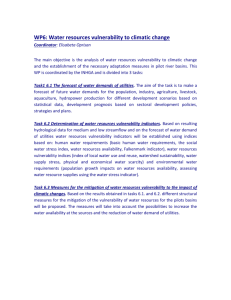
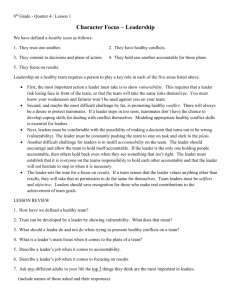
Comparing the group of individuals whose value of high vulnerability to stress (23QVS>43) with the group of low vulnerability individuals (23QVS≤43) data suggests that the most important stress factor was, in the most vulnerable students, the health-related issues. On the other hand, there was a negative correlation between vulnerability to stress and both frequency of sexual activity ( Figure 1) and alcohol consumption (Figure 2).
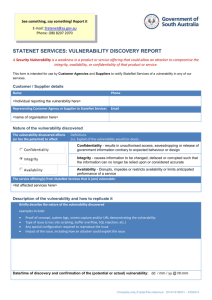
Finally, we found a pattern of correlation between
ARC Publishing
Marques et al.
Table 1. Main results in sociodemographic, biographical and lifestyle data.
Sociodemographic Characteristics
Gender, %
Female
Male
Age
Range
Mean ± standard deviation
71.1
29.9
19–27
20.81 ± 0.27
Living with, %
Family
Friends
Alone
Strangers
Biographical Characteristics
Stable relationship, %
No
Yes
Religious person, %
No
Yes
Main stressful event in last trimester, %
Academic
Family
Health
Economic
Drug use, %
None
Alcohol
Tobacco
Others
Lifestyle Characteristics
Sexual intercourse frequency, %
Never
Less than monthly
Less than weekly
More than weekly
Alcohol use frequency, %
Never
Less than weekly
More than weekly
57.9
42.1
65.4
34.6
44.0
34.6
12.7
8.7
48.7
14.8
16.5
20.0
50.0
46.0
26.0
13.0
59.9
29.1
7.9
3.1
50.4
41.7
7.9
Mann-‐Whitney Z=2.13 (p=0.033)
Never Monthly Weekly More than Weekly
Sexual Activity Frequency
Figure 1. Correlation between sexual activity frequency and vulnerability to stress (23QVS).
Mann-Whitney Z=2.50 (p=0.012)
Never Weekly More than Weekly
Alchool Intake Frequency
Figure 2. Correlation between alcohol consumption frequency and vulnerability to stress (23QVS).
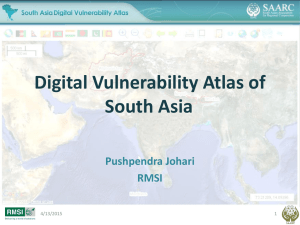
3 vulnerability to stress and symptoms of general psychopathology ( Figure 3). By selecting the subjects above the 23QVS cut-off point (n=20), we verified a positive correlation with SCL-90-R’s interpersonal sensitivity
(r=0.517; p=0.100), depression (r=0.497; p=0.130), phobic anxiety (r=0.443; p=0.030), psychoticism (r=0.427; p=0.038) ( Figure 4).
Vulnerability to Stress (23QVS) r 2 = 0.328
Figure 3. Correlation between psychopathology (SCL-90-R) and vulnerability to stress (23QVS).
IJCNMH 2015; 2:3
4 Stress and psychopathology in medical students
1.6
1.4
1.2
1
0.8
0.6
0.4
0.2
0
Discussion
23QVS≤43 23QVS>43
Psychopathology Symptoms (SCL-90-R)
Figure 4. Psychopathological dimensions (SCL-90-R) differences between low vulnerability to stress (23QVS≤43) and high vulnerability to stress (23QVS>43).
Portuguese 3 rd year medical students at Faculty of Medicine,
University of Lisbon presented low levels of stress vulnerability, and psychopathology. Females were more vulnerable to stress and academic events were the main stress factor.
In students highly vulnerable to stress, a strong correlation was found with other psychopathology. Moderate alcohol intake and healthy sexual activity were negatively correlated with stress, suggesting that an active social life may protect medical students from mental distress.
Comparison between studies with different methodology is not easy, but in our sample, vulnerability to stress was quite low (15.5%) and psychopathology prevalence was even lower (3.1%), when compared with reports in previous studies from Portugal [7] and abroad [8–11].
Probably because of cultural and anthropological aspects our students had lower levels of alcohol consumption than
American students [12] but higher sexual activity [13] when compared with African medical students.
The major stress factors were academic issues confirming previous results around the world [14–17]. Some authors referred to economical problems as a main stress factor in medical students [18,19], but that was not the case in our sample. This could be probably explained by the fact that most of the students where living with their family (59.9%), a situation that certainly eases any potential financial burden. On the other hand, family issues were pointed as the second most prevalent subtype of stressful event (46%). This data suggests that family may have an important role on the genesis of stressful events, probably related with interpersonal conflicts with kin members.
Students with health issues are more vulnerable to stress and among those, females seem to be especially vulnerable to stress associated to need or lack of social support, a result already suggested before [20–23] independently of social, cultural, and economical backgrounds of the sample.
The coexistence of stress and depression in medical students has been described [24, 25], but its interpretation is difficult. Our results showed that besides depression also interpersonal sensitivity, psychoticism, and phobic anxiety symptoms can be correlated with higher vulnerability to stress, in medical students. Still, as in previous works, it is hard to say whether stress vulnerability is cause or effect of these kind of symptoms.
We also found a possible relationship between social behaviour patterns and stress vulnerability: those with higher frequencies of alcohol consumption and sexual activity seem to be less vulnerable to stress. We believe that this correlation may result from wider social capacities and better integration with peers. We also suggest that less alcohol consumption means less interaction with colleagues and friends, especially in Portugal, a country with a lasting cultural tradition in alcohol beverages [26] and drinking habits across all ages and social positions. Following this idea less sexual activity would also mean less interaction with peers, resulting in social isolation, less social support, and thus a higher vulnerability to stress. In any case, these results should be cautiously interpreted as problematic sexual experiences [27], and especially alcohol abuse [28] can probably worsen medical students’ vulnerability to stress and other type of psychopathology.
One of the main limitations of this study was the transversal perspective and the small size of sample, with only
56% response rate. In contrast to others, we did not examine the possible correlation of other stress-related factors as alexithymia [29,30], personality traits [31, 32], coping styles [33–35], burnout [36–38], and the prevalence of stress among medical students [39]. It would be of especial interest to correlate these findings with future levels of burnout syndrome, as stress has been previously described as an important risk factor for burnout [40].
However our results are still pertinent as stress vulnerability is an important aspect to understand better ways to support this population, using both traditional approaches
[41,42], but also internet-based instruments [43,44]. This kind of approach shall be used in future studies of our group, while on the other hand, it would be also important to investigate a possible correlation between stress vulnerability, biological markers of stress [45], and academic success [46].
More detailed and longitudinal investigations shall be conducted, including randomized sampling and group control. This kind of data give us some insight about the previous studies, and might help in further opportunities for the creation of support structures in the prevention of burnout among this especially vulnerable population
Acknowledgements
This study was done with financial support from the GAPIC (Gabinete de Apoio à Investigação Científica), the Bureau of Support to Scientific
Research at the Faculty of Medicine in the University of Lisbon.
Competing interests
The authors declare no conflict of interest.
ARC Publishing
Marques et al.
5
References
1. Haglund ME, Aan Het Rot M, Cooper NS, Nestadt PS, Muller D,
Southwick SM, Charney DS. Resilience in the third year of medical school: a prospective study of the associations between stressful events occurring during clinical rotations and student well-being.
Acad Med 2009; 84(2):258-68.
2. Marjani A, Gharavi AM, Jahanshahi M, Vahidirad A, Alizadeh F.
Stress among medical students of Gorgan (South East of Caspian
Sea), Iran. Kathmandu Univ Med J (KUMJ) 2008; 6(23):421-5.
3. Roberto A, Almeida A. A saúde mental de estudantes de medicina: estudo exploratório na Universidade da Beira Interior. Acta Med
Port 2011; 24 Suppl 2:279-86.
4. Chew-Graham CA, Rogers A, Yassin N. 'I wouldn't want it on my
CV or their records': medical students' experiences of help-seeking for mental health problems. Med Educ 2003; 37(10):873-80.
5. Vaz-Serra A. Construção de uma escala para avaliar a vulnerabilidade ao stress: a 23 QVS. Psiquiatria Clínica 2000; 21(4):279-308.
6. Derogatis LR. The SCL-90-R. Baltimore: Clinical Psychometric
Research. 1975
7. Loureiro E, McIntyre T, Mota-Cardoso R, Ferreira MA. The relationship between stress and life-style of students at the Faculty of
Medicine of Oporto. Acta Med Port 2008; 21(3):209-14.
8. Leahy CM, Peterson RF, Wilson IG, Newbury JW, Tonkin AL,
Turnbull D. Distress levels and self-reported treatment rates for medicine, law, psychology and mechanical engineering tertiary students: cross-sectional study. Aust N Z J Psychiatry 2010; 44(7):608-15.
9. Koochaki GM, Charkazi A, Hasanzadeh A, Saedani M, Qorbani M,
Marjani A. Prevalence of stress among Iranian medical students: a questionnaire survey. East Mediterr Health J 2011; 17(7):593-8.
10. Abdulghani HM, AlKanhal AA, Mahmoud ES, Ponnamperuma GG,
Alfaris EA.Stress and its effects on medical students: a cross-sectional study at a college of medicine in Saudi Arabia. J Health Popul
Nutr 2011; 29(5):516-22.
11. Nandi M, Hazra A, Sarkar S, Mondal R, Ghosal MK. Stress and its risk factors in medical students: an observational study from a medical college in India. Indian J Med Sci 2012; 66(1-2):1-12.
12. Frank E, Elon L, Naimi T, Brewer R. Alcohol consumption and alcohol counselling behaviour among US medical students: cohort study. BMJ 2008; 337:a2155.
13. Daniyam CA, Agaba PA, Agaba EI. Afr Health Sci. 2010 Jun; 10(2):
150–153. Sexual behavior of medical students: A single institutional survey. Afr Health Sci 2010; 10(2): 150–153.
14. Sreeramareddy CT, Shankar PR, Binu VS, Mukhopadhyay C, Ray B,
Menezes RG. Psychological morbidity, sources of stress and coping strategies among undergraduate medical students of Nepal. BMC
Med Educ 2007; 7:26.
15. El-Gilany AH, Amr M, Hammad S. Perceived stress among male medical students in Egypt and Saudi Arabia: effect of sociodemographic factors. Ann Saudi Med 2008; 28(6):442-8.
16. Ofili AN, Oriaifo I, Okungbowa E, Eze EU. Stress and psychological health of medical students in a Nigerian university. Niger J Clin
Pract 2009; 12(2):128-33.
17. O'Rourke M, Hammond S, O'Flynn S, Boylan G. The Medical Student Stress Profile: a tool for stress audit in medical training. Med
Educ 2010; 44(10):1027-37.
18. Ross S, Cleland J, Macleod MJ. Stress, debt and undergraduate medical student performance. Med Educ 2006; 40(6):584-9.
19. Shariati M, Yunesian M, Vash JH. Mental health of medical students: a cross-sectional study in Tehran. Psychol Rep 2007;
100(2):346-54.
20. Amr M, Hady El Gilany A, El-Hawary A. Does gender predict medical students' stress in mansoura, Egypt? Med Educ Online 2008;
14;13:12.
21. Backović DV, Zivojinović JI, Maksimović J, Maksimović M. Gender differences in academic stress and burnout among medical students in final years of education. Psychiatr Danub 2012; 24(2):175-81.
22. Reang T, Bhattacharjya H. A study to assess the emotional disorders with special reference to stress of medical students of Agartala government medical college and Govinda Ballabh Pant hospital. Indian
J Community Med 2013; 38(4):207-11.
23. Haldorsen H, Bak NH, Dissing A, Petersson B. Stress and symptoms of depression among medical students at the University of Copenhagen. Scand J Public Health 2014; 42(1):89-95.
24. Bunevicius A, Katkute A, Bunevicius R. Symptoms of anxiety and depression in medical students and in humanities students: relationship with big-five personality dimensions and vulnerability to stress.
Int J Soc Psychiatry 2008; 54(6):494-501.
25. Park J, Chung S, An H, Park S, Lee C, Kim SY, Lee JD, Kim KS. A structural model of stress, motivation, and academic performance in medical students. Psychiatry Investig 2012; 9(2):143-9.
26. Kuntsche E, Wicki M, Windlin B, Roberts C, Gabhainn SN, van der
Sluijs W, Aasvee K, Gaspar de Matos M, Dankulincová Z, Hublet
A, Tynjälä J, Välimaa R, Bendtsen P, Vieno A, Mazur J, Farkas J,
Demetrovics Z. Drinking motives mediate cultural differences but not gender differences in adolescent alcohol use. J Adolesc Health
2015; 56(3):323-9.
27. Cao Y, Zhou X, Wang XQ, He QW, Lui ZP, Yang YH, Ji Y. Sexual knowledge, behaviors, and attitudes of medical students in Kunming, China. Psychol Rep 1998; 82(1):201-2.
28. Garg A, Chavan BS, Singh GP, Bansal E. Patterns of alcohol consumption in medical students. J Indian Med Assoc 2009;
107(3):151-2, 154-5.
29. Lala A, Bobirnac G, Tipa R. Stress levels, alexithymia, type A and type C personality patterns in undergraduate students. J Med Life
2010; 3(2):200-5.
30. Balaban H, Semiz M, Şentürk IA, Kavakçı Ö, Cınar Z, Dikici A,
Topaktaş S. Migraine prevalence, alexithymia, and post-traumatic stress disorder among medical students in Turkey. J Headache Pain
2012; 13(6):459-67.
31. Tyssen R, Dolatowski FC, Røvik JO, Thorkildsen RF, Ekeberg O,
Hem E, Gude T, Grønvold NT, Vaglum P. Personality traits and types predict medical school stress: a six-year longitudinal and nationwide study. Med Educ 2007; 41(8):781-7.
32. Compton MT, Carrera J, Frank E. Stress and depressive symptoms/ dysphoria among US medical students: results from a large, nationally representative survey. J Nerv Ment Dis 2008; 196(12):891-7
33. Tanaka M, Fukuda S, Mizuno K, Kuratsune H, Watanabe Y. Stress and coping styles are associated with severe fatigue in medical students. Behav Med 2009; 35(3):87-92.
34. An H, Chung S, Park J, Kim SY, Kim KM, Kim KS. Novelty-seeking and avoidant coping strategies are associated with academic stress in
Korean medical students. Psychiatry Res 2012; 200(2-3):464-8.
35. Cherkil S, Gardens SJ, Soman DK. Coping styles and its association with sources of stress in undergraduate medical students. Indian J
Psychol Med 2013; 35(4):389-93.
36. Chang E, Eddins-Folensbee F, Coverdale J. Survey of the prevalence of burnout, stress, depression, and the use of supports by medical students at one school. Acad Psychiatry 2012; 1;36(3):177-82.
37. Yusoff MS, Abdul Rahim AF, Baba AA, Ismail SB, Mat Pa MN,
Esa AR. Prevalence and associated factors of stress, anxiety and depression among prospective medical students. Asian J Psychiatr
2013; 6(2):128-33.
38. Dyrbye LN, West CP, Satele D, Boone S, Tan L, Sloan J, Shanafelt
TD. Burnout Among U.S. Medical Students, Residents, and Early
Career Physicians Relative to the General U.S. Population. Acad Med
2014; 89(3):443-51.
39. Sohail N. Stress and academic performance among medical students.
IJCNMH 2015; 2:3
6 Stress and psychopathology in medical students
J Coll Physicians Surg Pak 2013; 23(1):67-71.
40. Ishak W, Nikravesh R, Lederer S, Perry R, Ogunyemi D, Bernstein
C. Burnout in medical students: a systematic review. Clin Teach
2013; 10(4):242-5.
41. Shiralkar MT, Harris TB, Eddins-Folensbee FF, Coverdale JH. A systematic review of stress-management programs for medical students. Acad Psychiatry 2013; 37(3):158-64.
42. Pereira MA, Barbosa MA. Teaching strategies for coping with stressthe perceptions of medical students. BMC Med Educ 2013; 13:50.
43. George DR, Dellasega C, Whitehead M. Facebook stress management group for Year 1 medical students. Med Educ 2012;
46(11):1118.
44. Bauer J, Groneberg DA. Perception of stress-related working conditions in hospitals (iCept-study): a comparison between physicians and medical students. J Occup Med Toxicol 2013; 8(1):3.
45. Katsuura S, Kuwano Y, Yamagishi N, Kurokawa K, Kajita K, Akaike
Y, Nishida K, Masuda K, Tanahashi T, Rokutan K. MicroRNAs miR-144/144* and miR-16 in peripheral blood are potential biomarkers for naturalistic stress in healthy Japanese medical students.
Neurosci Lett 2012; 516(1):79-84.
46. Voltmer E, Kötter T, Spahn C. Perceived medical school stress and the development of behavior and experience patterns in German medical students. Med Teach 2012; 34(10):840-7.
ARC Publishing
 0
0
Related documents
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users