A Critical Re-evaluation of the Diphenylamine Test for Malignancy
advertisement

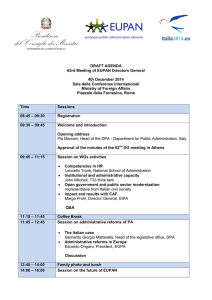
T H E AMERICAN JOURNAL OF CLINICAL PATHOLOGY Vol. 35, No. 6, pp. 479-487 June, 1961 Copyright © 1961 by The Williams & Wilkins Co. Printed in U.S.A. A CRITICAL RE-EVALUATION OF THE DIPHENYLAMINE TEST FOR MALIGNANCY ROBERT E. ZIPF, M. D., JAMES P. P. MURPHY, B. S., AND BERNARD J. KATCHMAN, P H . D . Department of Research, Miami Valley Hospital, Dayton, Ohio Received, November 2, 1960; revision received, December 20; accepted for publication February 28, 1961. Dr. Zipf is Director of Research and Associate Pathologist, Department of Pathology; Mr. Murphy is Research Biochemist; and Dr. Katchman is Assistant Director of Research. This work was supported in part by the Charles F. Kettering Foundation, Yellow Springs, Ohio; the Montgomery County Society for Cancer Control, Dayton, Ohio; and the Ella Lowe Gunckle Fund, Dayton, Ohio. gated concurrently with the DPA studies in order to correlate these 2 tests. This paper is a report of the results of our investigation of the DPA and of the "no DPA" reactions and an evaluation of their usefulness as diagnostic aids in diseased states. The results of a study of (1) the experimental conditions of the tests, and of (2) added chemicals (to serum from normal persons) that affect color intensity in both color reactions are detailed separately.9 METHOD The method used in the clinical studies was basically that of Waldo and Zipf.12 A slight modification in the procedure was necessary to perform studies of concentration of serum and to use the 1-cm. cell of the Beckman DK recording spectrophotometer. These modifications gave values in normal and pathologic serum comparable to those obtained by the original method. To serum (0.2 to 2.4 ml.) was added 5.6 ml. of 5 per cent trichloroacetic acid and water to make 8 ml. This mixture was heated for 5 min. in a boiling water bath, cooled to room temperature, and filtered. A 2-ml. aliquot of the filtrate was added to 6 ml. of the DPA reagent (180 ml. of glacial acetic acid plus 20 ml. of concentrated sulfuric acid and 1 Gm. of diphenylamine). This mixture was heated for 30 min. in a boiling water bath, cooled to room temperature in an ice-bath, and then read in the Beckman DK recording spectrophotometer between 400 to 900 m/*, using a water blank. Characteristic spectral curves were obtained for normal and pathologic serums over the ranges of serum concentration studied. These spectral curves have 2 peaks, 1 at 675 niM and the other at 530 myu. A plot of optical density vs. serum concentration for either peak usually resulted in a straight line that passed through the origin. In some instances it was noted that straight 479 Downloaded from http://ajcp.oxfordjournals.org/ by guest on March 4, 2016 For the past several years, workers concerned with the development of diagnostic tests have observed that a more intense color is obtained when diphenylamine reacts with serum from patients with rheumatic fever,1, 2- 7 nonspecific inflammations,4 malignant neoplasms,11 rheumatoid arthritis, 3, 6 typhoid fever, hepatic lesions,10 and leukemia,12 than with serum from healthy persons. These reports indicate that the diphenylamine (DPA) reaction is more likely to be a response to generalized insult than to any specific disease state. In view of the report12 that the DPA reaction could be used as a diagnostic test for malignancy, it became necessary to re-evaluate the reaction in order to ascertain conditions for specificity, if any exist. The DPA test, as described in the literature, involved measurement of the developed color intensity at a single wave length and at a convenient concentration of serum. Our studies of the DPA reaction to ascertain its specificity were broadened to include the effect of serum concentration and of chemicals added to serum on the visible absorption spectrum of the developed color. In the course of these studies, it was noted that a characteristic color was obtained in serum even when diphenylamine was omitted from the standard colordeveloping reagent. A similar finding has been described by Hess and co-workers.8 This "no DPA" color reaction was investi- 480 ZIPF ET lines that intersect the optical density axis were obtained, as well as curvilinear plots that intersect the origin. These noncharacteristic plots, observed in about 10 per cent of the data, were randomly distributed and could not be ascribed to any particular pathologic condition. The fact that about 90 per cent of the serums examined gave linear plots over the whole range of serum concentration (2.4 ml. maximal concentration) was a good indication that the test conditions were maximal for color development. Vol. 35 AL. Conditions for study of the second color reaction ("no DPA") were identical to those of the DPA reaction except that diphenylamine was omitted from the standard color-developing reagent. The peak of 470 nut, thus obtained, was very broad, but nevertheless readily recognized. Plots of the optical density at 470 nui vs. concentration of serum gave straight lines passing through the origin; there was a smaller frequency of noncharacteristic plots at this wave length than in the DPA reaction. For clinical evaluation, however, both reagents gave comparable results. Downloaded from http://ajcp.oxfordjournals.org/ by guest on March 4, 2016 04 Oi PATH0L08ICAL FIG. normal FIG. optical 12 l<« 20 14 CONCENTRATION CURVE OS l« NORMAL 14 S« 3 « 4 0 CONCENTRATION CURVE 1 (upper). Characteristic spectral curves revealing peaks at 675 imj and 530 nip for and pathologic serums when used in the DPA reaction. 2 (lower). From the characteristic spectral curves in Figure 1, corresponding plots of density vs. concentration of serum are indicated. June 1961 481 D I P H E N Y L A M I N E T E S T F O B MALIGNANCY RESULTS Figure 1 represents examples of characteristic spectral curves obtained in the DPA reaction for normal and pathologic serums; the corresponding plots of optical density vs. concentration of serum reveal linearity of the developed color at 675 nut and 530 nuj (Fig. 2). Similarly, the data for the "no DPA" reaction are illustrated in Figures 3 and 4. The linear plots of optical density vs. concentration (Figs. 2 and 4) pass through the origin and thereby substantiate the validity of the use of a water blank in the spectrophotometric analysis. 10 08 06 04 ^r\l / 02 ^" "^^_ / / / ^ ~ ~ ~ ~ 01 / •*^ / < ^S* JS ,-r S — — normal pathological 470INIWAVELENGTH 0-6 normal pathologica 2-4 32 CONCENTRATION CURVE FIG. 3 (upper). Characteristic spectral curves indicating a peak of 470 nut for normal and pathologic serums when used in the "no DPA" reaction. FIG. 4 (lower). From the characteristic spectral curves in Figure 3, corresponding plots of optical density vs. concentration of serum are indicated. Downloaded from http://ajcp.oxfordjournals.org/ by guest on March 4, 2016 Serums designated as normal were obtained from healthy blood bank donors; individual as well as pooled serum was used. Pathologic serums were obtained from persons with a recorded clinical diagnosis. All chemicals used were of highest purity commercially available. Nevertheless, during the course of this study, it was noted that some batches of acid reagents produced distorted curves. The impurity responsible for these shifts in the spectrums is unknown, and it should be noted that only by examination of the absorption spectrums of the reaction mixture can this effect be ascertained. 482 ZIPF ET Vol 35 AL. TABLE 1 DPA I N D E X I N NORMAL AND PATHOLOGIC S E R U M S 675 m/i Standard Mean value deviation* 530 mp Standard 95% Tolerance limits Mean value deviation* 95% Tolerance limits Single Valuesf Normal Malignant Nonmalignant Leukemic 53 107 107 127 316 450 437 403 316 450 437 403 ± ± ± ± 104 216 218 259 253 367 363 333 40 91 95 104 253 367 363 333 ± ± ± ± 79 183 193 212 Smoothed Values! 81 117 118 458 428 423 458 ± 175 428 ± 247 423 ± 255 372 350 347 64 98 ' 99 372 ± 138 350 ± 208 347 ± 214 * Standard deviation of individual observations. f D P A index at indicated wave length for 0.8 ml. of serum. | D P A index for 0.8 ml. of serum obtained from linear plot of serum concentration curve. TABLE 2 COLOH I N D E X * I N NOEMAL AND PATHOLOGIC S E R U M S AT 470 M,U Mean Value Standard 95% Tolerance Limits Deviation! Single V a l u e s ! Normal Malignant Nonmalignant Leukemic 104 155 160 140 21 57 46 57 104 155 160 140 ± 41 ± 114 ± 94 ± 117 Smoothed Values§ Malignant Nonmalignant Leukemic 159 ± 74 154 ± 100 159 ± 119 * Color developed without DPA in reagent. f Standard deviation of individual observations. J D P A index at indicated wave length for 0.8 ml. serum. § D P A index for 0.8 ml. serum obtained from linear plot of serum concentration curve. Table 1 is an analysis of the data obtained from the study of serums (0.8 ml.) from 240 healthy persons and 109 patients with various disease states by means of the DPA reaction. The concentration of serum chosen for analysis is comparable to that used by Waldo and Zipf.12 The mean value for normal persons of 253 units (optical density X 1000) at 530 m^i compares favorably with that of 248 units described by Waldo and Zipf12 at this wave length. For purposes of distinguishing between the serums of healthy and diseased persons, 95 per cent limits of tolerance for individual observations have been calculated. The DPA index at 675 mM is 316 ± 104 units and at 530 m/x, 253 ± 79 units for healthy persons. The mean DPA index for diseased persons is greater at either wave length than the mean indices for healthy persons at the corresponding wave length. Thus, there is good discrimination at either wave length between healthy and diseased persons. Similarly, the indices at 470 va/j. (no DPA in the reagent) also distinguish readily between the serums of healthy and diseased persons (Table 2). In serum from diseased patients, however, neither the DPA nor the "no DPA" reaction manifests distinct enough differences in the indices to permit distinction of a specific disease state among pathologic serums. The agreement between corresponding pairs of data (Tables 1 and 2) indicates that determination of a single value is just as Downloaded from http://ajcp.oxfordjournals.org/ by guest on March 4, 2016 Malignant Nonmalignant Leukemic June 1961 D I P H E N Y L A M I N E T E S T FOR 483 MALIGNANCY TABLE 3 RELATIVE FREQUENCY OF OCCURRENCE OF DPA INDICES SERUMS AMONG NORMAL AND 675 mix Number of persons Percentage of persons detectable as nonnormal at the 5 % probability level* 95th percentile D P A index Malignant 530 irnt Nonmalignant Leukemic Normal Malignant Iff Normal PATHOLOGIC Leukemic 240 41 71 35 57 33 42 240 41 71 35 57 33 46 400 658 678 638 318 550 577 523 reliable an index as a calculated value from a concentration curve for either of the color reactions. It should be noted that this lack of specificity by the DPA test at 530 nu* is not in agreement with the selectivity of this test reported by Waldo and Zipf.12 For this reason, we have recorded in Table 3 and Figure 5 the relative frequency of occurrence of ranges of DPA indices at 675 nu* and 530 nijU in serums from healthy and diseased persons. For completeness of data presentation, similar treatment for the "no DPA" reaction (peak at 470 nui) is recorded in Table 4 and Figure 6. The data in Tables 3 and 4 are arranged to show the number of indices that fall in a particular range for each of the test methods and for the 4 categories of individuals. In each of these tables is summarized the percentage of patients detectable as diseased; i.e., that percentage of patients whose indices fall outside the 95th percentile index of the healthy persons. Thus, at 530 mji, 57 per cent of nonmalignant, 71 per cent of malignant, and 46 per cent of leukemic persons have indices greater than the 95th percentile of the normal DPA index. The uniformity of these percentages at the 3 wave lengths is a good indication of the reliability of the test methods. It should be noted, however, that these data illustrate the wide distribution of indices and overlap among the serums from patients with malignant, nonmalignant, and leukemic conditions (Figs. 5 and 6), TABLE 4 R E L A T I V E FREQUENCY OF OCCURRENCE OF C O L O R I N D I C E S * AT 470 M^U AMONG NORMAL AND PATHOLOGIC SERUMS Number of persons Percentage of persons detectable as non -normal at the 5% probability levelf 95th percentile (no DPA) color index Normal Malignant Nonmalignant 224 41 61 32 59 27 41 137 280 288 296 Leukemic * Color developed without D P A in reagent. t Percentage of persons with color indices exceeding t h e 95th percentile index of t h e normal group where t h e 95th percentile color index is t h a t index which exceeds 95 per cent of t h e persons' indices in a group. and because of this overlap, the DPA and "no DPA" tests are not capable of distinguishing between various diseases. The tests may be used to distinguish between healthy and diseased persons, and, in this sense, may be a reliable measure of the extent of humoral reaction to a generalized insult of the body. DISCUSSION The DPA reagent of Waldo and Zipf,12 as well as that used in our own studies, is constituted of 1 part of sulfuric acid and 9 parts of glacial acetic acid (containing 0.5 Downloaded from http://ajcp.oxfordjournals.org/ by guest on March 4, 2016 * Percentage of persons with D P A index exceeding the 95th percentile index of t h e normal group where t h e 95th percentile DPA index is t h a t index which exceeds 95 per cent of the persons' indices in a group. 484 ZIPF ET Vol. 35 AL. 675mu 530mu NORMAL NORMAL MALIGNANT MALIGNANT NONMALIGNANT NONMALIGNANT 40 30 20 10 _^d 40 30 10 II Ul u Id 0. LLn 40 30 20 10 CL XX LEUKEMIC in ML LEUKEMIC 40 30 20 10 XI0*3 ^d X 0*5 0*6 0*7 01 0 2 0 3 0-4 0 3-Q, 0*6 0 7 OPTICAL DENSITY F I G . 5. The relative frequency of occurrence of ranges of D P A indices at 675 imt and 530 m/i among normal and pathologic serum. *~51 0*2 0*4 jr per cent diphenylamine). Niazi and State, 11 as well as Ayala and co-workers,1 used the Dische reagent per se, which is constituted of 1 part of sulfuric acid and 39 parts of glacial acetic acid (containing 1 per cent diphenylamine). Dische6 has already indicated that with these reagents the most important variable with respect to sensitivity and selectivity or specificity is the sulfuric acid-glacial acetic acid ratio. Thus, the Dische reagent does not produce color when reacted with hexoses, and its absorption spectrum reveals a strong peak at 530 m/i and a very weak one at 675 imi; this is in contrast to the DPA reagent that reacts with a wide variety of substances including hexoses, and results in strong peaks at 530 m/i and 675 m,u. Therefore, although these reagents are similary constituted, they do have different ranges of Downloaded from http://ajcp.oxfordjournals.org/ by guest on March 4, 2016 20 June 1961 DIPHENYLAMINE TEST FOR 485 MALIGNANCY 4 7 0 muMALIG N A N T OPTICAL 0-1 0 3 LEUKEMIC 0 2 DENSITY FIG. 6. The relative frequency of occurrence of ranges of "DPA" indices at 470 nn< among normal and pathologic serums. reaction response, and in this sense may be regarded as different reagents. Nevertheless, our results are in agreement with those reported by Niazi and State. 11 They, too, could distinguish only between healthy and diseased serums; high values were observed in serum from postpartum patients and in persons with pulmonary tuberculosis, rheumatic fever, inflammations, and so on. On the other hand, our results do not confirm the specificity claimed by Waldo and Zipf12 for the DPA reagent in its response to leukemic serum. In reviewing the Waldo data, 2 discordant facts are evident; the data reveal no high values for serums other than that derived from leukoproliferative disorders. Our experience, as well as that of Niazi and State11 and others, has shown high values for many malignancies and nonmalignancies, as well. In addition, we have observed low values in serums of patients with leukoproliferative disorders, while under clinical control, and have received no indication that the color index rises precipitously while the patients are under therapy. In order to demonstrate the latter point, we have prepared Table 5. It can be seen from Table 5 that many patients with leukoproliferative diseases, controlled by therapy, manifest low normal DPA indices at 530 m/i over a long period of time; even at death there was no unusually high DPA index. It is more likely that the DPA reaction measures a general response to insult of the body, as evidenced by the elevated DPA indices that are observed in serums from patients diagnosed as having polycythemia, malignancies, leukoproliferative disorders, and nonmalignancies, as described here, and rheumatic fever, inflammations, rheumatoid arthritis, typhoid fever, and hepatic lesions, as described by others. We have reported that the "no D P A " reactions give a distribution of indices comparable to those of the DPA reagent observed at 530 niju and 675 niju. This correlation between the DPA and "no DPA" test would seemingly implicate a single substance or blood component as the responsible factor in both tests. In a subsequent paper, 9 evidence is described which would indicate that the material in serum from healthy persons reponsible for the color produced in the DPA and "no DPA" tests is related to the neuraminic acids. It may be convenient to ascribe the increase in color-forming material observed in the serum of diseased persons to neuraminic acid containing glycoprotein; however, the chemical studies at least leave room for the possibility that under the conditions of these serum tests, Downloaded from http://ajcp.oxfordjournals.org/ by guest on March 4, 2016 02 NONMALIGNANT 486 Z I P F ET AL. TABLE 5 DPA Patient T . R. I N D E X AT 530 M/X DURING T H E R A P Y Diagnosis Monoblastic leukemia W. R. Lymphosarcoma with infiltration of bone marrow W. R. Polycythemia Polycythemia M. E . Polycythemia A. C. Gangrene of leg with leukocytic infiltration W. H . Chronic granulocytic leukemia M. N. J . J. S. G. Chronic lymphatic leukemia Chronic lymphatic leukemia Lymphosarcoma May 6, 1955 May 11, 1955 June 5, 1955 J u n e 7, 1955 June 29, 1955* June 17, 1955 J u l y 20, 1955 August 4, 1955 August 21, 1952 October 23, 1952 November 20, 1952 July 23, 1953 September 19, 1953 1954 August 2, 1955 September 8, 1955 June 21, 1955 July 19, 1955 June 23, 1955 July 23, 1955 J u l y 6, 1955 June 7, 1955 July 15, 1955 March 15, 1956 M a r c h 20, 1956 M a r c h 26, 1956 April 3, 1956 April 18, 1956 July 10, 1956* March 22, 1955 M a y 6, 1955 June 17, 1955 October 1, 1955 December 10, 1955 June 1, 1954 J a n u a r y 4, 1955 M a y 2, 1955 July 30, 1955f September 3, 1953 September 14, 1953 September 25, 1953 December 9, 1953 1954 M a y 4, 1955 October 29, 1955f * Patient died. t Patient still under treatment. Therapy Triethylene melanine 6-Mercaptopurine DPA Index 410 410 410 P-32 Triethylene melanine 260 280 P-32 P-32 P-32 P-32 P-32 P-32 P-32 P-32 Postamputation X-ray Myleran Myleran Myleran Myleran Myleran P-32 P-32 P-32 P-32 P-32 X-ray P-32 P-32 P-32 P-32 P-32 P-32 Triethylene melanine Triethylene melanine, P-32 Triethylene melanine, P-32 Triethylene melanine, P-32 285 215 390 380 295 308 337 509 347 516 577 495 300 265 265 295 295 208 201 182 255 225 215 332 350 296 350 Downloaded from http://ajcp.oxfordjournals.org/ by guest on March 4, 2016 S. L. Date June 1961 487 D I P H E N Y L A M I N E T E S T F O R MALIGNANCY certain normally occurring metabolites simple a executar, es usate pro sequer le (fructose, sedoheptulose, and so on) may be curso clinic de un therapia. responsible for producing enhanced serum Acknowledgments. The authors wish to acknowlDPA indices. edge t h e technical assistance of M r s . Lois Chiles Neither the DPA nor the "no D P A " who performed chemical tests, M r . K e n n e t h Busch reagent manifests specificity, when reacted for the statistical analysis, and D r . L. E . Loveless with serum, to warrant their utilization as a for his efforts on this paper. specific screening test for leukemia or any REFERENCES other malignant or nonmalignant condition. 1. AYALA, W., M O O R E , L. V., AND H E S S , E . L . : The method is simple, however, and may be Purple color reaction given b y diphenylamine reagent with normal a n d rheumatic useful in following the clinical course of fever sera. J . Clin. Invest., 30: 781, 1951. therapy after a diagnosis has been made. 2. BONOMO, E . , SALA, G., A M I B A , A., AND B A L SUMMARY 3. CECCHI, E . , AND F E B E A R I S , F . : Serum diphe- nylamine reaction in rheumatoid arthritis. Ann. R h e u m a t . Dis., 14: 267, 1955. 4. C O B U E N , A. F . , B A T E S , R. C , H A H N , J . W., AND M U R P H Y , P . : F u r t h e r observations on diphenylamine (DPA) reaction as an index of inflammation. J . Chron. Dis., 3 : 140153, 1956. 5. DISCHE, Z.: tJber einige neue charakteristische Farbreaktionen der Thymonukleinsaure und eine Mikromethode zur bestimmung derselben in tierischen Organen m i t hilfe dieser Reaktionen. Mikrochemie, 8: 4, 1930. 6. F E A R N L E Y , G. R., P I N K I S , J., D E C O E K , N . , LACKNER, R., AND M E A N O C K , R. I.: Diphenylamine reaction in rheumatoid arthritis. Ann. R h e u m a t . Dis., 14: 226231, 1955. 7. G A M P , SUMMARIO I N I N T E R L I N G U A 1. Es describite datos additional pertinente con respecto al test a diphenylamina (DPA) pro malignitate, insimul con datos pertinente con respecto al test a "nulle DPA." 2. Ambe tests manifesta intensificate indices de color in specimens de sero ab subjected morbide. 3. Le analyse statistic del datos indica que —ben que ambe tests pote esser usate pro distinguer inter subjectos malade e subjectos normal—ni le un ni le altere pote esser usate pro distinguer inequivocamente inter subjectos con diverse morbos. 4. Es proponite que iste tests, que es A.: Die Diphenylaminreaktion im Serum bei chronische-rheumatschen E r k rankungen. Med. Klin. (Munich), 50: 2146-2147, 1955. 8. H E S S , E . L., C O B U R N , A. F . , B A T E S , R. C, AND M U R P H Y , P . : N e w method for measuring sialic acid levels in serum a n d its application t o rheumatic fever. J . Clin. Invest., 36: 449-455,1957. 9. KATCHMAN, B . J . , M U R P H Y , J . P . , AND Z I P F , R. E . : The effect of chemicals on t h e serum DPA and " n o D P A " reactions. Am. J . Clin. P a t h . , 35: 488-494, 1961. 10. K U M A T E , J., VIVAR, G. M., AND B E N A V I D E S , L. V . : T h e serum D P A reaction in normal children a n d in those with typhoid fever and hepatic lesion. Bol. M e d . Hosp. Infantil. Mex., 12: 377, 1955. 11. N I A Z I , S., AND S T A T E , D.: Diphenylamine reaction of human serum. 8: 653-656, 1948. Cancer R e s . , 12. W A L D O , A. L., AND Z I P F , R. E . : T h e diphenyl- amine test on leukemic sera. 10:468, 1954. Experientia, Downloaded from http://ajcp.oxfordjournals.org/ by guest on March 4, 2016 1. Additional data pertaining to the DPA test for malignancy are described, as well as data on the "no DPA" test. 2. Both tests manifest enhanced color indices in specimens of serum from diseased persons. 3. Statistical analysis of the data indicates that, although either test may be used to distinguish between healthy and diseased persons, neither test can be used to distinguish unequivocally between persons with various diseases. 4. It is suggested that these tests that are simple to perform may be used to follow the clinical course of therapy. LABIO, C. R.: Comparative studies of serum polysaccharides in rheumatic diseases. Acta. med. scandinav. (Supp. 312), 361-365, 1956.