American Journal of Emergency Medicine 32 (2014) 24–28
Contents lists available at ScienceDirect
American Journal of Emergency Medicine
journal homepage: www.elsevier.com/locate/ajem
Original Contribution
Jolt accentuation of headache and other clinical signs: poor predictors of meningitis
in adults☆,☆☆
Jolene H. Nakao, MD, MPH a, Farrukh N. Jafri, MD a,⁎, Kaushal Shah, MD b, David H. Newman, MD b
a
b
Department of Emergency Medicine, St Luke's–Roosevelt Hospital Center, New York, NY, USA
Department of Emergency Medicine, Mount Sinai School of Medicine, New York, NY, USA
a r t i c l e
i n f o
Article history:
Received 12 July 2013
Received in revised form 5 September 2013
Accepted 16 September 2013
a b s t r a c t
Jolt accentuation or exacerbation of a baseline headache with horizontal rotation of the neck is a physical
finding believed to assess for meningeal irritation. We conducted a prospective observational study of
neurologically intact emergency department (ED) patients undergoing lumbar puncture in 2 inner city
academic EDs to validate the sensitivity and specificity of jolt accentuation and to assess the sensitivity and
specificity of Kernig sign, Brudzinski sign, and nuchal rigidity, in predicting cerebrospinal fluid (CSF)
pleocytosis in individuals being assessed for meningitis. Adult patients 18 years and older undergoing lumbar
puncture between 2006 and 2009 were approached for consent. Exclusions included inability to consent and
altered mental status. Physicians were asked to answer a questionnaire of physical examination findings
before receiving CSF results. The primary outcome was the presence or absence of pleocytosis, defined as
greater than or equal to 5 cells/high-power field in the fourth CSF tube. We calculated descriptive statistics
and tests of diagnostic accuracy. A total of 230 patients consented for participation and had CSF white blood
cell counts recorded. Forty-seven individuals (20%) had pleocytosis. A total of 197 patients had headache and
were, hence, eligible for jolt accentuation assessment. For pleocytosis, the sensitivity of jolt accentuation was
21%, Kernig sign was 2%, Brudzinski sign was 2%, and nuchal rigidity was 13%. The specificity of jolt
accentuation was 82%, Kernig sign was 97%, Brudzinski sign was 98%, and nuchal rigidity was 80%. Jolt
accentuation in our cohort was poorly predictive of pleocytosis and insensitive. The presence of Kernig sign,
Brudzinski sign, or nuchal rigidity has moderate positive but no negative predictive value for pleocytosis.
© 2013 Elsevier Inc. All rights reserved.
1. Introduction
1.1. Background
Bacterial meningitis, with an annual incidence of 4 to 6 cases per
100 000 adults in the United States [1] and an overall mortality rate of
20% to 30% [2,3], is considered a medical emergency requiring rapid
diagnosis and timely intervention. The criterion standard for
diagnosing meningitis is the lumbar puncture (LP), a potentially
painful procedure that carries a risk of complications including
worsened headache, spinal hematoma, and introduction of infection.
Establishing predictive clinical variables that accurately predict the
absence of meningitis may allow clinicians to comfortably forego an
LP in very low-risk individuals.
Much of what is taught and believed to be predictive regarding the
signs and symptoms of meningitis comes from chart review data as
well as diagnostic signs developed during a meningococcal epidemic
before the discovery of antibiotics, advent of vaccinations, and
development of public health measures. The objective of our study
was to evaluate the sensitivity and specificity of clinical variables in
predicting cerebrospinal fluid (CSF) pleocytosis in neurologically
intact individuals undergoing LP for possible meningitis at our 2
affiliated urban emergency departments (EDs). Our secondary
objective was to assess the diagnostic accuracy of physicians' clinical
suspicion for meningitis. We hypothesized that jolt accentuation and
classic signs of meningeal irritation including Kernig sign, Brudzinski
sign, and nuchal rigidity are poorly predictive of CSF pleocytosis.
2. Methods
☆ Prior presentation: This work has been presented at the American College of
Emergency Physicians Scientific Assembly, October 2011, San Francisco, CA, as “Jolt
accentuation of headache: sensitive enough for pleocytosis to rule-out need for a
lumbar puncture in diagnosing meningitis?” (abstract no. 019).
☆☆ Sources of support and conflicts of interest: None.
⁎ Corresponding author. Department of Emergency Medicine, St Luke's–Roosevelt
Hospital, 1000 10th Ave, New York, NY 10019. Tel.: +1 914 263 0329.
E-mail address: fnjafri@gmail.com (F.N. Jafri).
0735-6757/$ – see front matter © 2013 Elsevier Inc. All rights reserved.
http://dx.doi.org/10.1016/j.ajem.2013.09.012
2.1. Study design and setting
We conducted an observational study of neurologically intact adult
ED patients undergoing an LP in our 2 inner city academic EDs. St
Luke's Hospital and Roosevelt Hospital are affiliated teaching
hospitals in Manhattan, New York City, with an emergency medicine
residency program and an estimated annual patient census of
J.H. Nakao et al. / American Journal of Emergency Medicine 32 (2014) 24–28
approximately 190 000. The study was approved by the St Luke's–
Roosevelt Hospital Center Institutional Review Board.
2.2. Selection of participants
A convenience sample of adult patients 18 years and older
presenting to either EDs and undergoing LP with the treating
physician suspecting meningitis as a potential diagnosis during a 4year period from January 1, 2006, to December 31, 2009, were
considered eligible for the study. Exclusions included inability to
provide consent, prisoner status, and alteration in mental status.
2.3. Data collection and processing
Trained research assistants staffed both EDs from 8 AM to midnight
on a university-based academic calendar representing approximately
60% of days annually. Research assistants monitored a real-time
tracking system for all patients with potentially associated presentations, including headache and fever, and approached treating
physicians to inquire about the potential need for an LP. The
departmental supply of LP trays was relocated to the research
assistant computer kiosk area to ensure catchment. Eligible patients
were approached for consent if the treating physician confirmed the
absence of exclusion criteria. Following informed consent, assistants
asked physicians, typically attending physicians or senior level
emergency medicine residents, to fill out a standardized data
collection tool recording patient age, sex, symptoms (including
headache and fever), clinical signs (including temperature, and
presence of Kernig sign, Brudzinski sign, jolt accentuation, nuchal
rigidity, vomiting, and rash), and physician suspicion of meningitis
after seeing the subject but before performing the LP.
All CSF samples were sent to the laboratory for cell count, glucose
level, protein level, and cultures. Data forms were collected from the
physicians by the research assistants, who entered all of the data into
a Microsoft Excel document. The results of LPs were later extracted
from the electronic medical record and recorded in the database.
These data were later reviewed by 2 study investigators; medical
record numbers, subject age, CSF analysis and culture results, and date
of LP were confirmed through the electronic medical record. The
electronic medical record was also interrogated for subject ethnicity.
2.4. Outcome measures and variable definitions
The principal outcome of this study was pleocytosis. We defined
pleocytosis as CSF white blood cell (WBC) count greater than or equal
to 5 cells/high-power field (HPF) in the fourth tube taken from the LP,
with a ratio of red blood cells to white blood cells (red blood cell:
WBC) less than 700:1. We defined moderate pleocytosis as greater than
or equal to 100 cells/HPF and severe pleocytosis as greater than or
equal to 1000 cells/HPF based on prior convention [4,5].
Headache was a subjective symptom. The variable “fever” was a
combination of subjective fever, whether a subject reported having or
having had a fever, and objective fever as measured in the ED.
Objective fever was defined as an oral or rectal temperature greater
than or equal to 100.4°F.
Jolt accentuation was defined as exacerbation of a baseline
headache with horizontal rotation of the neck, 2 to 3 times per
second [6]. Other variable definitions were, in the case of “classic”
signs of meningeal irritation, based on textbook definitions and
reviewed with department physicians at group training sessions and
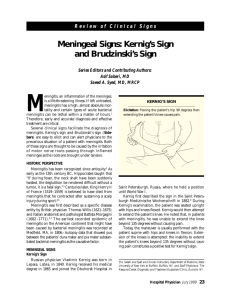
individually before and throughout the study period. A Kernig sign
was considered present “if the examiner is unable, because of
resistance and hamstring pain, to straighten the patient's leg passively
to a position of full knee extension when the patient is lying supine
with the hip flexed to a right angle” [7], and Brudzinski sign was
considered present “if attempts to flex the neck passively are
25
accompanied by flexion of the hips” [7]. Nuchal rigidity was defined
as “discomfort [or pain] on flexion of the neck” [7].
Regarding physician suspicion of meningitis, after interviewing
and examining a subject but before performing the LP, the emergency
physician was asked for his or her “impression” as to whether the
subject did (subjectively judged as 50% or higher probability) or did
not (subjectively judged as less than 50% probability) have bacterial
meningitis. This outcome was binary.
2.5. Analysis
Statistical data exploration and analysis were conducted by the
primary investigator using Stata statistical software (version 10,
2007; StataCorp LP, College Station, TX). We used common
descriptive statistics and diagnostic performance tests with 95%
confidence intervals.
3. Results
3.1. Characteristics of study participants
Over the 4-year period, 240 subjects were enrolled that met
predefined inclusion and exclusion criteria and whose data forms
were complete. Data were reviewed by 2 of the primary investigators.
Data for 10 subjects were not included in the analysis because CSF
WBC counts from the fourth tube were missing. Hence, 230 subjects
were included in the final analysis; one of these had values for
particular minor variables missing and was included in the analysis
accordingly wherever possible.
The average age of enrollees was 40.2 years, and 43.0% were male
(Table 1). Forty-seven subjects (20.4%) had pleocytosis, 15 (6.5%) had
moderate pleocytosis, and 1 (0.4%) had severe pleocytosis.
3.2. Clinical presentation
One hundred ninety-seven individuals (85.7%) reported headache,
and 90 (39.1%) reported fever (Table 2). The 197 subjects who
complained of headache were eligible for jolt accentuation assessment, and 229 had physical examination signs recorded. Of subjects
presenting with headache, 37 (18.8%) had a positive jolt accentuation
test. Of the 229 individuals with recorded physical examination signs,
6 subjects (2.6%) had a positive Kernig sign, 5 (2.2%) had a positive
Brudzinski sign, and 43 (18.8%) had nuchal rigidity.
3.3. Pleocytosis and culture-positive meningitis
The prevalence of cultures showing pathogen growth in subjects
with CSF pleocytosis was 6%. Three cultures were positive, growing
Neisseria meningitiditis, Cryptococcus neoformans, and Enterovirus,
making the prevalence of culture-positive bacterial meningitis 2%.
Table 1
Demographic characteristics, subjects receiving LP
Characteristics
Age
Age (y), mean (range)
No. of patients ≥60 years old (%)
Sex
Male
Female
Ethnicity
White
Black
Hispanic
Other/unknowna
a
All patients
40.2 (18-88)
28/230 (12.2%)
99/230 (43.0%)
131/230 (57.0%)
82/230
70/230
36/230
42/230
(35.6%)
(30.4%)
(15.7%)
(18.3%)
Patients who during registration chose not to identify themselves by race.
26
J.H. Nakao et al. / American Journal of Emergency Medicine 32 (2014) 24–28
Table 2
Clinical presentation, subjects receiving LP
Clinical characteristics
Headache
Reported fever
Temperature ≥100.4°F
Reported fever or measured temperature ≥100.4°F
Jolt accentuation
Kernig sign
Brudzinski sign
Nuchal rigidity
Focal neurologic deficit
Vomiting
Rash
Physician suspicion
Bacterial meningitis
CSF results
WBC count, mean WBCs/HPF
WBC count, median WBCs/HPF
Glucose level, mean mg/dL
Glucose level, median mg/dL
Protein level, mean mg/dL
Protein level, median mg/dL
Culture growth positive
All
(n = 230)
No pleocytosis
(n = 183)
Pleocytosis
(n = 47)
P
197/230 (85.7%)
90/230 (39.1%)
56/223 (25.1%)
90/230 (39.1%)
37/197 (18.8%)
6/229 (2.6%)
5/229 (2.2%)
43/229 (18.8%)
9/229 (3.9%)
30/229 (13.1%)
8/229 (3.5%)
154/183 (84.2%)
76/183 (41.5%)
49/176 (27.8%)
76/183 (41.5%)
28/154 (18.2%)
5/182 (2.7%)
4/182 (2.2%)
37/182 (20.3%)
8/182 (4.4%)
28/182 (15.4%)
7/182 (3.8%)
43/47 (91.5%)
14/47 (29.8%)
7/47 (14.9%)
14/47 (29.8%)
9/43 (20.9%)
1/47 (2.1%)
1/47 (2.1%)
6/47 (12.8%)
1/47 (2.1%)
2/47 (4.3%)
1/47 (2.1%)
.20
.18
.09
.18
.66
1.00
1.00
.30
.69
.05
1.00
130/230 (56.5%)
109/183 (59.6%)
21/47 (44.7%)
.07
26.9 (n = 230)
1
64.2 (n = 228)
61
49.8 (n = 229)
42
8/230 (3%)
0.7 (n = 183)
0
64.16 (n = 181)
61
42.87 (n = 182)
39
5/183 (3%)
129.0 (n = 47)
44
60.49 (n = 47)
58
76.77 (n = 47)
66
3/47 (6%)
This low prevalence is consistent with that found in prior work. The
subject with cryptococcal meningitis denied HIV infection on initial
interview but was later found to be HIV positive.
The prevalence of positive cultures in subjects without pleocytosis
was 3%, representing 5 subjects. These cultures grew Streptococcus
mitis (2), Streptococcus sanguinis, Bacillus cereus, and Staphylococcus
saccharolyticus; all were deemed likely contaminants.
3.4. Predicting pleocytosis and moderate pleocytosis
Table 3
Predicting pleocytosis among subjects receiving LP
Physician suspicion was found to have a sensitivity of 44% in
predicting pleocytosis. This sensitivity increased to 56% in subjects
with moderate pleocytosis. Among the 3 subjects whose CSF revealed
pleocytosis and whose CSF cultures were positive for infective
organisms, all 3 subjects were suspected of having bacterial
meningitis by the physician before performance of an LP.
We present a prospective investigation examining the diagnostic
utility of jolt accentuation and other classical physical findings used to
assess for potential meningitis in which there appeared to be little to
no clinical utility or predictive value in these examination finding. In
1991, a group of Japanese researchers examined candidates for LP
from a group of febrile patients with an associated headache [6],
including those seen in ED, outpatient, and inpatient settings. As in
our investigation, patients with altered mental status or presence of a
focal neurologic deficit were excluded. Fifty-four subjects were
enrolled among which 34 had pleocytosis and 33 had a positive jolt
accentuation test, suggesting jolt accentuation may detect pleocytosis
with adequate sensitivity (97%) to potentially obviate the need for LP
[6]. We were unable to replicate these findings.
In 2010, another prospective analysis of jolt accentuation was
performed by Waghdhare et al [5] in a population of intensive care
Table 4
Predicting moderate pleocytosis among subjects receiving LP
Sensitivity
(0.95 CI)
Specificity
(0.95 CI)
LR+
LR−
91% (88-95)
30% (24-36)
21% (15-27)
2% (0-4)
2% (0-4)
13% (8-17)
2% (0-4)
4% (2-7)
2% (0-4)
44% (31-59)
16% (11-21)
58% (52-65)
82% (76-87)
97% (95-99)
98% (96-100)
80% (74-85)
96% (93-98)
85% (80-89)
96% (94-99)
40% (33-47)
1.1
0.7
1.2
0.8
1.0
0.6
0.5
0.3
0.6
0.8
0.5
1.2
1.0
1.0
1.0
1.1
1.0
1.1
1.0
1.4
Abbreviation: 0.95 CI, 95% confidence interval.
3.5. Diagnostic accuracy of physician suspicion
4. Discussion
The sensitivity and specificity of classic signs of meningeal irritation
in predicting pleocytosis are shown in Tables 3 and 4, including
likelihood ratios (LRs) for a positive result (LR+) and likelihood ratios
for a negative result (LR−). Jolt accentuation had poor sensitivity for
predicting both pleocytosis (21%) and moderate pleocytosis (33%) and
only moderate specificity. Report of having or having had a headache
was the single symptom/sign with the greatest sensitivity for
pleocytosis, 91%. Although poorly sensitive, the physical examination
findings of Kernig sign, Brudzinski sign, nuchal rigidity, vomiting, and
rash were all relatively specific for both pleocytosis and moderate
pleocytosis; however, because sensitivity was low for all of these
features, LRs suggest that these findings are ultimately unhelpful. For
the finding of moderate pleocytosis, however, high specificity resulted
in potentially useful, although not diagnostic, LRs for a positive finding
of jolt accentuation, Kernig sign, and Brudzinski sign.
Headache (n = 230)
Fever (n = 230)
Jolt accentuation (n = 197)
Kernig sign (n = 229)
Brudzinski sign (n = 229)
Nuchal rigidity (n = 229)
Focal neurologic deficit (n = 229)
Vomiting (n = 229)
Rash (n = 229)
Physician suspicion (n = 230)
.00
–
.15
–
.00
–
.21
Headache (n = 230)
Fever (n = 230)
Jolt accentuation (n = 197)
Kernig sign (n = 229)
Brudzinski sign (n = 229)
Nuchal rigidity (n = 229)
Focal neurologic deficit (n = 229)
Vomiting (n = 229)
Rash (n = 229)
Physician suspicion (n = 229)
Sensitivity
(0.95 CI)
Specificity
(0.95 CI)
LR+
LR−
80%
27%
33%
7%
7%
20%
0%
7%
0%
56%
14%
60%
82%
98%
98%
81%
96%
86%
96%
43%
0.9
0.7
1.9
2.9
3.6
1.1
0.0
0.5
0.0
1.0
1.4
1.2
0.8
1.0
1.0
1.0
1.0
1.1
1.0
1.0
(75-85)
(21–32)
(27-40)
(3-10)
(3-10)
(15-25)
(0-0)
(3-10)
(0-0)
(33-77)
(9-18)
(54-66)
(77-88)
(96-100)
(96-100)
(76-86)
(93-98)
(82-91)
(94-99)
(37-50)
J.H. Nakao et al. / American Journal of Emergency Medicine 32 (2014) 24–28
unit patients with acute encephalitis syndrome (fever, headache, and
altered mental status), one-third of whom were suffering from
tuberculous meningitis. The finding exhibited a sensitivity of 6% and a
specificity of 99%. The high specificity suggested jolt accentuation may
have a role as a finding on which empiric treatment decisions could
potentially be based.
Our study prospectively examined jolt accentuation in a diverse ED
population of patients without alteration in mental status, in the
hopes of determining the utility of this finding when applied by
emergency physicians to a typical emergent patient population of
those undergoing LP for possible meningitis. Unfortunately, our study
suggests both poor sensitivity and only moderate specificity of the jolt
accentuation test. Based on the LRs associated with these findings, we
cannot recommend its use as a determinant of either the presence or
absence of meningitis.
In 1882, Vladimir Kernig, a neurologist in St Petersburg, Russia,
first described his famous clinical sign, soon discussed within
numerous case studies. In 1909, Josef Brudzinski, a pediatrician at
the Anne-Marie Kinderhospital in Poland, described a sign of
automatic flexion of hips and knees when the head of a child is
flexed. Since the middle of the 20th century, these 2 physical
examination findings have been considered elemental in the
evaluation and documentation of potential meningitis, particularly
in children [8]. Retrospective and prospective studies, however, have
challenged their utility [9,10]. Uchihara and Tsukagoshi [6] found the
sensitivity of Kernig sign to be 8.8%. Thomas et al [4], in an assessment
of 66 subjects with pleocytosis defined as a CSF WBC count greater
than or equal to 6 per milliliter, discovered sensitivities of both Kernig
and Brudzinski signs to be 5%. Furthermore, the 2010 study of
Waghdhare et al [5] of patients admitted for fever, headache, and
altered mental status suggested the sensitivity of Kernig sign to be
14.1% and Brudzinski sign to be 11.1%. Our data are consistent with
these findings.
Nuchal rigidity or pain with flexion of the neck has shown varied
results in the literature in regard to its sensitivity and usefulness as a
clinical aid. In a systematic review, Attia et al [9] found a pooled
sensitivity of 70% for nuchal rigidity in predicting meningitis. In a
prospective observational analysis of 696 patients with communityacquired bacterial meningitis, 83% had neck stiffness [11]. Sensitivity
analyses in retrospective and prospective trials demonstrate a wide
range from 15% to 88% [9], with the most recent prospective trials
demonstrating sensitivities of 30% [4] and, in a sicker population, 39%
[5]. Our results, like those of recent prospective studies, demonstrate
poor sensitivity of nuchal rigidity in the diagnosis of meningitis.
Interestingly, vomiting was present more often in those without
pleocytosis than in those with pleocytosis, which may indicate more
about which patients are considered for LP in our setting than about
the utility of vomiting as a predictor variable. We also found
physician suspicion, as a binary variable, to have poor sensitivity
(44%) in predicting pleocytosis. Although all 3 subjects whose CSF
revealed pleocytosis and whose CSF bacterial cultures were positive
for infecting agents were suspected to have meningitis by the
physician, the small number of these cases makes conclusions
limited and raises an important additional limitation in our data set:
bacterial and other identifiable causes of meningitis and encephalitis
(fungal, viral, etc) may ultimately be more relevant to clinician
practice than simple pleocytosis.
Although we were unable to identify any single symptom or sign
that is a strong predictor of pleocytosis, the development of a
diagnostic algorithm by which to predict pleocytosis based on
constellations of clinical findings, although beyond the scope of our
investigation, remains possible.
Cerebrospinal fluid analysis and culture remain the definitive
method for diagnosis of meningitis. However, when facing a
potentially fatal illness such as meningitis, early treatment is of
utmost importance. In patients presenting with the classic triad of
27
fever, nuchal rigidity, and altered mental status, diagnostic LP and
early antibiotic administration seem warranted. However, it is the
alert and oriented patient complaining of headache, fever, or both—a
patient with some features of meningitis but in whom the diagnosis is
unclear—who presents a diagnostic challenge. We focused on this
population that emergency physicians see on a daily basis, to
determine if jolt accentuation and other signs, if present or absent,
could obviate the need for an LP or help to avoid unnecessary hospital
admissions. Our study demonstrates, unfortunately, that no single
physical examination finding is able to accurately predict pleocytosis.
In the absence of definitive research demonstrating that examination
findings are much more predictive than we found, the entire clinical
picture—including symptoms, signs, laboratory studies, and physician
judgment—appears to retain primacy in determining whether a
patient should undergo LP.
Finally, although we captured only 3 cases of culture-positive
meningitis, all 3 were identified as likely being meningitis based on
physician suspicion before performing an LP, lending support to the
notion that physician judgment may be the best diagnostic tool in
detecting culture-positive meningitis.
4.1. Limitations
Our study has several limitations. We collected data when research
assistants were available and present and thus had no mechanism for
consecutive catchment. We believe that the convenience nature of our
sample, however, is unlikely to significantly impact the findings of
diagnostic utility for the clinical variables being tracked, as there is no
clear directional bias that we can identify in the pattern of missed
potential enrollments resulting from our research assistant scheduling and coverage.
Examinations were performed by residents in postgraduate years
1 through 3 as well as attending physicians, and this experiential
difference has the potential to lead to biased results or potential
limitations in extrapolating these results to a physician sample with
greater experience.
For cultures that were positive in subjects who did not have
pleocytosis, it seems likely that these species were contaminants. We
identified just 1 subject with severe pleocytosis, leaving us unable to
make inferences about the subset of patients typically of greatest
concern to emergency care providers, those with bacterial meningitis.
No subjects reported being HIV positive during initial screening;
however, 8 were subsequently consented, tested, and found to be HIV
positive. This testing was not routinely performed on all subjects
enrolled, and therefore, our study was unable to address the
association of this immunodeficiency with pleocytosis.
5. Conclusion
Jolt accentuation in our cohort, like other clinical signs and
symptoms we tested, was insensitive and poorly predictive of
pleocytosis. Physical examination signs, patient symptoms, and
clinical acumen appear to be inconsistent predictors of the presence
or absence of meningitis.
Acknowledgments
We would like to acknowledge Dr Peter Homel for his contributions to our data analysis.
References
[1] van de Beek D, de Gans J, Tunkel AR, et al. Community-acquired bacterial
meningitis in adults. N Engl J Med 2006;354:44–53.
[2] Durand ML, Calderwood SB, Weber DJ, et al. Acute bacterial meningitis in adults: a
review of 493 episodes. N Engl J Med 1993;328:21–8.
28
J.H. Nakao et al. / American Journal of Emergency Medicine 32 (2014) 24–28
[3] Saez-Lorens X, McCracken GH. Bacterial meningitis in children. Lancet 2003;361:
2139.
[4] Thomas KE, Hasbun R, Jekel J, et al. The diagnostic accuracy of Kernig's sign,
Brudzinski's sign, and nuchal rigidity in adults with suspected meningitis. Clin
Infect Dis 2002;35:46–52.
[5] Waghdhare S, Kalantri A, Joshi R, et al. Accuracy of physical signs for detecting
meningitis: a hospital-based diagnostic accuracy study. Clin Neurol Neurosurg
2010;112:752–7.
[6] Uchihara T, Tsukagoshi H. Jolt accentuation of headache: the most sensitive sign of
CSF pleocytosis. Headache 1991;31:167–71.
[7] Meurer WJ, Lavoie FW. Chapter 107: central nervous system infections. In: Marx
JA, Hockberger RS, Walls RM, editors. Rosen's emergency medicine: concepts and
clinical practice. 7th ed. Philadelphia: PA, Mosby Elsevier; 2010. p. 1417–29.
[8] Wartenberg R. The signs of Brudzinski and of Kernig. J Pediatr 1950;37(4):679–84.
[9] Attia J, Hatala R, Cook DJ, et al. Does this adult patient have acute meningitis?
JAMA 1999;282(2):175–81.
[10] Puxty JAH, Fox RA, Horan MA. The frequency of physical signs usually attributed to
meningeal irritation in elderly patients. J Am Geriatr Soc 1983;31:590–2.
[11] van de Beek D, de Gans J, Spanjaard L, et al. Clinical features and prognostic factors
in adults with bacterial meningitis. N Engl J Med 2004;351:1849–59.