CASE 3
advertisement

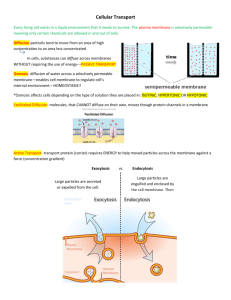
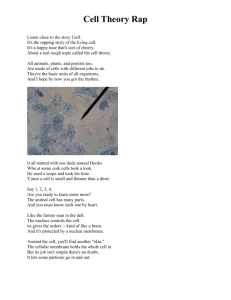
❖ CASE 3 A 6-year-old boy is brought to the family physician after his parents noticed that he had difficulty moving his arms and legs after a soccer game. About 10 minutes after leaving the field, the boy became so weak that he could not stand for about 30 minutes. Questioning revealed that he had complained of weakness after eating bananas, had frequent muscle spasms, and occasionally had myotonia, which was expressed as difficulty in releasing his grip or difficulty opening his eyes after squinting into the sun. After a thorough physical examination, the boy was diagnosed with hyperkalemic periodic paralysis. The family was advised to feed the boy carbohydrate-rich, low-potassium foods, give him glucose-containing drinks during attacks, and have him avoid strenuous exercise and fasting. ◆ What is the effect of hyperkalemia on cell membrane potential? ◆ What is responsible for the repolarizing phase of an action potential? ◆ What is the effect of prolonged depolarization on the skeletal muscle Na+ channel? 32 CASE FILES: PHYSIOLOGY ANSWERS TO CASE 3: ACTION POTENTIAL Summary: A 6-year-old boy who experiences profound weakness after exercise is diagnosed with hyperkalemic periodic paralysis. ◆ ◆ ◆ Effect of hyperkalemia on membrane potential: Depolarization. Repolarization mechanisms: Activation of voltage-gated K+ conductance and inactivation of Na+ conductance. Effect of prolonged depolarization: Inactivation of Na+ channels. CLINICAL CORRELATION Hyperkalemic periodic paralysis (HyperPP) is a dominant inherited trait caused by a mutation in the α subunit of the skeletal muscle Na+ channel. It occurs in approximately 1 in 100,000 people and is more common and more severe in males. The onset of HyperPP generally occurs in the first or second decade of life. HyperPP is neither painful nor life-threatening but can be disruptive to normal activities. Symptoms are muscle weakness and paralysis, sometimes preceded by myotonia, fasciculations, or spasms. Fortunately, significant paralysis almost never occurs in intercostals or diaphragm muscles, and so breathing is not impaired. Attacks can occur spontaneously but often are triggered by exercise, stress, fasting, or the ingestion of large quantities of K+ (eg, in bananas). For unknown reasons, exercise-induced paralysis always follows exercise—it does not occur during exercise. Because exercise can produce hyperkalemia and hyperkalemia triggers HyperPP attacks, there must be an additional mechanism that protects skeletal muscle during but not after intense activity. The mechanisms that underlie the effects of HyperPP result from several known mutations in the α subunit of the skeletal muscle Na+ channel that prevent it from closing effectively. Ineffective closing results in a small, persistent inward current that continuously depolarizes the muscle membrane; this lowers the action potential threshold, producing the hyperexcitability that results in fasciculations (spontaneous twitches) and spasms under resting conditions. If the depolarization increases further, as occurs when extracellular [K+] is elevated, the Na+ channels inactivate and remain inactivated until repolarization occurs. This inactivation blocks action potential initiation in the muscle and produces paralysis. When extracellular [K+] decreases, the depolarization is reduced, inactivation is removed, and the paralysis is relieved. Amelioration of HyperPP attacks is attempted by reducing plasma K+ levels. Insulin promotes the transport of extracellular K+ into intracellular compartments by activating the Na-K pump. Eating highcarbohydrate diets or pure glucose increases insulin secretion and thus decreases extracellular [K+]. Conversely, fasting decreases insulin secretion and can elevate extracellular [K+], increasing the chances of myotonia and paralysis in HyperPP patients. CLINICAL CASES 33 APPROACH TO ACTION POTENTIAL PHYSIOLOGY Objectives 1. 2. Know the mechanisms of the resting potential. Understand the mechanisms of the action potential in axons and skeletal muscle. Definitions Action potential: A rapid, depolarizing change in membrane potential (often overshooting, so that the potential transiently reverses) that is used by excitable cells to convey all-or-none electrical signals quickly from one point on the cell to the remainder of the cell. Electrotonic conduction: The passive, exponentially falling, spread of a difference in membrane potential between different membrane regions, which occurs with potentials subthreshold for an action potential or with perturbations of membrane potential in inexcitable membrane regions. Nernst equilibrium potential: The membrane potential at which, for a given ion, there is no net flow of the ion across the membrane, which corresponds to the electrical force that exactly offsets the driving force of the concentration gradient acting on that ion. Resting potential: The electrical potential difference across the plasma membrane in the absence of action potentials or synaptic potentials. Voltage-gated channel: Pore-forming protein complexes that allow ions to flow across a membrane, and which can be opened (or, in some cases, closed) by a change in membrane potential. DISCUSSION The mechanisms that underlie the action potential cannot be understood without an understanding of how a resting membrane potential is generated. The resting potential in nearly all mammalian cells is produced primarily by diffusion of K+ down its concentration gradient from inside to outside the cell, whereas the membrane remains relatively impermeable to other ions. The intracellular concentration of K+ is very high compared with the outside concentration because K+ is pumped into the cell by the Na+-K+-ATPase (adenosine triphosphatase) (see Figure 3-1). Because the membrane is effectively impermeable to intracellular anions, as K+ flows down its concentration gradient, it leaves behind anions. A transmembrane potential (Vm) develops as the K+ efflux brings a positive charge to the region just outside the membrane, leaving an equal amount of negative charge just inside the membrane. This process is self-limiting because as soon as a membrane becomes permeable to K+ and K+ efflux begins, the resulting separation of the charge generates an electrical driving force on the ions, and the electrical driving 34 CASE FILES: PHYSIOLOGY 2K+ β Outside α 3Na+ Inside Figure 3-1. Na+-K+-ATPase pump. The α subunit is the catalytic subunit, which uses adenosine triphosphate (ATP) for energy to drive the extrusion of three Na+ ions for every two K+ ions taken into the cell. The β subunit is important for assembly and membrane targeting of the Na+-K+-ATPase. Pump activity can be blocked by cardiac glycosides, such as ouabain. (From Horisberger JD, Lemas V, Kraehenbuhl JP, Rossier BC. Structure–function relationship of Na-K-ATPase. Ann Rev Physiol. 1991;53:565. Reproduced, with permission, from the Annual Review of Physiology, vol. 53. Copyright © 1991 by Annual Reviews Inc.) force soon equals the opposing chemical driving force (the K+ concentration gradient). For K+ or any ion X, this equilibrium occurs at a Vm called the Nernst equilibrium potential, which is defined as the electrical driving force (EX) that exactly offsets the chemical driving force. The electrical driving force is represented by the left side and the chemical driving force is represented by the right side of the Nernst equation: EX = RT [ X]o In [ X]i zF R is the gas constant, T is the temperature in degrees Kelvin, z is the valence of the ion, F is the Faraday constant, and [X]o and [X]i are the ion’s extracellular and intracellular concentrations. In the case of K+ at 37°C and converting to log10, the equation becomes E k = 60 log [K + ]o [K + ]i It is important to note that a given ion X is at equilibrium across the membrane only when Vm = EX. Because of the relatively high intracellular concentrations 35 CLINICAL CASES of K+ in mammalian cells, EK is always quite negative (eg, ∼ −90 mV). Because of the pumping action of the Na+-K+-ATPase, the concentration gradient for Na+ is in the opposite direction (ie, [Na+]o >> [Na+]i), and thus ENa = ∼ +55 mV. However, in cells, such as glia, in which there is no significant permeability to Na+, Na+ influx makes almost no contribution to Vm. In most cells, including all excitable cells, Vm ≠ EK, although the values are often close. This is the case because the membrane is also permeable to other ions, and it is the net effect of all ion permeability across the membrane that determines Vm. In many axons, Vm is determined almost entirely by opposing fluxes (or, in electrical terms, currents) carried by K+ and Na+. These can be described, in terms of the ratio of permeabilities (α = PNa/PK) and ionic concentrations, by the Goldman-Hodgkin-Katz equation, which is closely related to the Nernst equation: Vm = 60 log [K + ]o + α[ Na + ]o [K + ]i + α[ Na + ]o In an axon at rest, α = approximately 0.01, and so the contributions of the Na+ concentrations in the expression are slight, and Vm is close to EK (∼ −90 mV). In many neuronal cell bodies or dendrites, PNa is somewhat greater than this when the cell is at rest and Vm is more depolarized (eg, ∼ −65 mV). Permeabilities (P) often are referred to by their electrical equivalents, conductances (g). Note that an increase in extracellular K+, that is, hyperkalemia, will depolarize cells, whereas hypokalemia will hyperpolarize cells. An all-or-none action potential is generated in an axon when membrane depolarization reaches a level at which voltage-gated Na+ channels open, increasing PNa. This results in an inward current of Na+, which causes further depolarization, which then opens additional Na+ channels. This regenerative (positive feedback) cycle quickly produces an overshooting action potential. In terms of the Goldman-Hodgkin-Katz equation, α quickly goes from approximately 0.01 to 100, Vm becomes dominated by the Na+ concentration gradient, and thus Vm approaches ENa at the peak of the action potential. Axonal action potentials last only a few milliseconds because two mechanisms rapidly repolarize the membrane. One is the activation of voltagegated K+ channels that open with a slight delay compared with the Na+ channels, resulting in the delayed rectifier outward current carried by K+ ions. Although this reduces α by increasing PK, a second depolarization-triggered mechanism, Na+ channel inactivation, reduces α by decreasing PNa. Thus, depolarization initially opens Na+ channels (activation) but then closes Na+ channels (inactivation), and the channels remain closed until the membrane repolarizes to a level close to the normal resting potential. This means that prolonged depolarization produced for example, by hyperkalemia, can make excitable cells inexcitable. The changes in permeability, expressed in terms of conductance (g), that underlie the action potential in axons are shown in Figure 3-2. The mechanisms 36 CASE FILES: PHYSIOLOGY E Na+ Voltage or conductance Membrane potential + Na + K E K+ 1 ms Figure 3-2. The nerve action potential. The time course of changes in the Na+ and K+ conductance is depicted. for repolarizing the membrane after each action potential (which is critical for preventing summation of action potentials and permitting firing at high frequencies) are also responsible for the biphasic refractory period that follows each action potential. Inactivation of Na+ channels completely prevents action potential initiation, causing the absolute refractory period. After Na+ inactivation is removed by repolarization, the membrane remains less excitable than normal during the relative refractory period, during which the delayed rectifier K+ channels are transiently open. The action potential propagates because the depolarization and overshoot in an active region (where voltage-gated Na+ channels are open) spread passively by electrotonic conduction to adjacent regions, depolarizing those regions and triggering the same regenerative sequence when the neighboring Na+ channels are opened by the electrotonically conducted depolarization. Electrotonic conduction occurs because the positive Na+ ions entering the cell in the active region are attracted to the net negative charge inside neighboring membrane that is hyperpolarized, and neighboring anions are attracted to the CLINICAL CASES 37 positive region inside the active membrane. The opposite current flow occurs outside the membrane. These intracellular and extracellular currents combine in a local circuit that quickly depolarizes membrane adjacent to an active region. Current density underlying electrotonic propagation of depolarization (or hyperpolarization) declines exponentially with distance. The effectiveness of electrotonic propagation often is compared by using the space or length constant λ, which varies with the square root of the diameter of the axon. This means that electrotonic propagation of current in front of an active region projects farther in axons with larger diameters and therefore that conduction of action potentials is faster in larger axons. The velocity of action potential conduction also depends on how much time it takes for a region of membrane to depolarize. This is characterized by the time constant τ, which varies directly with membrane resistance Rm and membrane capacitance Cm. If Rm or Cm is large, the rate with which a region of membrane can depolarize (or hyperpolarize) is slow, and this reduces the velocity of action potential conduction. Mammals have increased action potential velocity by myelinating many axons, which in effect reduces Cm. The most rapidly conducting axons are both myelinated and have large diameters (ie, have small τ and large λ). Demyelinating diseases such as multiple sclerosis profoundly decrease conduction velocity and cause serious neurologic problems. COMPREHENSION QUESTIONS [3.1] The resting transmembrane potential (Vm ) of a nerve axon is essential for signal generation. Instantaneous elimination of which of the following would most rapidly bring Vm close to 0 mV? A. Active transport of K+ out of the cell B. Active transport of Na+ out of the cell C. Concentration gradient for Na+ D. High membrane permeability to K+ E. High membrane permeability to Na+ [3.2] Hyperkalemia reduces the excitability of neurons and muscle cells. Which of the following best describes the effect of increased extracellular potassium [K+]o? A. Depolarizes the cell, thus reducing action potential amplitude B. Depolarizes the cell, thus inactivating voltage-gated Na+ channels C. Hyperpolarizes the cell, which increases the action potential threshold D. Increases the activity of the Na-K-ATPase, which hyperpolarizes the cell E. Stimulates endocytosis of Na+ channels 38 [3.3] CASE FILES: PHYSIOLOGY The velocity of action potential conduction is noted to be affected by various parameters. If the conduction velocity were found to be augmented, which of the following characteristics would most likely be decreased? A. B. C. D. E. Action potential amplitude Effective membrane capacitance The concentration gradient for Na+ The rate at which Na+ channels open in response to depolarization Na+ channel density uniformly along a fiber Answers [3.1] D. The immediate cause of the resting potential is the high membrane permeability to K+ compared with other ions; if this permeability were to be eliminated, Vm would instantly depolarize to within several mV of 0 mV. It would not quite reach 0 mV because of the electrogenic effect of the Na+-K+-ATPase (which pumps three Na+ ions out for every two K+ ions pumped in). The diffusion of K+ down its concentration gradient in the absence of diffusion of anions out of the cell or diffusion of other cations into the cell causes a slight separation of charge across the membrane that generates most of the resting potential. The active transport of K+ into the cell (not, as in answer A, out of the cell) is necessary for setting up the concentration gradient that results in the diffusion of K+ out of the cell. This gradient (and therefore Vm) would take a long time to dissipate if active transport were stopped. Because the membrane is effectively impermeable to Na+ at rest, the transport and concentration gradient for Na+ has very little effect on the resting potential (answers B, C, and E). [3.2] B. Sustained depolarization, as occurs with hyperkalemia, inactivates voltage-gated Na+ channels, which remain inactivated until the membrane repolarizes, thus blocking action potential generation. If action potentials are generated, their amplitude will be reduced (answer A), but this is a consequence rather than a cause of reduced excitability. Hyperpolarization also can reduce excitability by increasing the depolarization needed to reach action potential threshold (answers C and D), but this would be produced by hypokalemia, not by hyperkalemia. There is no evidence that prolonged hyperkalemia decreases the number of Na+ channels in the membrane (answer E). [3.3] B. Effective membrane capacitance is decreased in many mammalian axons by myelination—the tight wrapping of many glial membranes around the axon, which is functionally equivalent to increasing the thickness of the membrane. Because conduction velocity is inversely CLINICAL CASES 39 related to membrane capacitance, which is related inversely to effective membrane thickness, a decrease in membrane capacitance increases conduction velocity. Decreasing action potential amplitude (answer A) will decrease rather than increase action potential velocity (see Case 8), as will decreasing the concentration gradient for Na+ (because this will reduce action potential amplitude). In addition, decreases in the opening rate or density of Na+ channels will decrease conduction velocity. PHYSIOLOGY PEARLS ❖ ❖ ❖ ❖ ❖ ❖ The resting potential is generated by the high permeability of the membrane to K+ compared with other ions, which allows a very small amount of K+ to diffuse out of the cell in the absence of net diffusion of other ions, causing a charge separation across the membrane. The resting potential and action potential in simple excitable systems, such as axons, that are permeable only to K+ and Na+, can be described by the Goldman-Hodgkin-Katz equation, which states that Vm is determined by opposing currents carried by K+ and Na+, which are determined entirely by (1) the ratio of permeabilities to K+ and Na+ and (2) their concentration gradients across the cell membrane. An action potential is generated when membrane depolarization reaches a level at which voltage-gated Na+ channels open, increasing PNa (or, in electrical terms, gNa), which results in an inward current of Na+, which causes further depolarization, opening additional Na+ channels in a positive feedback cycle. Inactivation of Na+ channels during an action potential prevents subsequent action potential initiation during the brief absolute refractory period, whereas the relative refractory period continues shortly thereafter because the delayed rectifier K+ channels remain open for a somewhat longer period. The spread of depolarization in front of an active region of membrane during an action potential occurs by electrotonic propagation, which is characterized by an exponential decay of the depolarization with distance along the fiber. The velocity of action potential conduction is increased by myelinating axons, which decreases their effective membrane capacitance, and by increasing the fiber diameter, which decreases the intracellular resistance. 40 CASE FILES: PHYSIOLOGY REFERENCES Byrne JH. Resting potentials and action potentials in excitable cells. In: Johnson LR, ed. Essential Medical Physiology. San Diego, CA: Elsevier Academic Press; 2003:71-96. Moczydlowski EG. Electrical excitability and action potentials. In: Boron WF, Boulpaep EL. Medical Physiology. Philadelphia, PA: Elsevier Science; 2003:172-203.