SECRETION AND ABSORPTION in the INTESTINE
advertisement

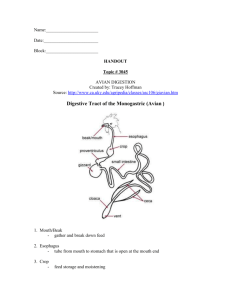
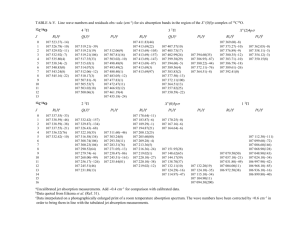
May 29, 2004 Intestinal Secretion and Absorption Ron Lynch, Ph.D 626-2472 SECRETION AND ABSORPTION in the INTESTINE Objectives: 1. Describe the mechanism for salt and water secretion in the small and large intestine, and what its role is. 2. Understand the importance of the stem cell division and migration cycle in the maintenance of epithelial integrity. 3. Identify the mechanism of absorption of the primary metabolites. 4. Understand how water absorption can be modified and how such alterations can lead to diarrhea and constipation. Water movement follows the movement of osmolytes including ions and nutrients. Therefore, understanding the mechanisms of osmolyte transport and the anatomical distribution of specific cell types along the length of the intestine forms the basis for understanding how and where water moves. In general, there is net fluid secretion from cells located within the intestinal crypts, while there is net fluid absorption by the enterocytes lining the villi. The surface area of the villi is massive compared to the crypts such that net water absorption is normally favored. However, continuous secretion of water, and therefore osmolytes is required to maintain the intestine moist particularly under resting (inter-digestive) periods. I. General Functional Anatomy: Small Intestine A. Intestinal Villi refers to the extensive foldings observed in the surface of the intestine. The villi are covered by a layer of epithelial cells with only a few other cell types interspersed. This folding arrangement dramatically increases surface area providing an optimal situation for absorption. B. Crypts of Lieberkuhn are extensive pits found between villi at their base which extend to the submucosa and are found in all parts of the intestine. The crypts contain multipotential cells which can differentiate into absorptive epithelial cells as they migrate towards the villus tip. In addition to these precursor cells, a large variety of mucus secreting goblet cells, and endocrine cells are found in the crypts. It is likely that most nutrient sensing endocrine secreting cells are located in these structures 2/17/2006 8:50 AM Absorption/02 1 May 29, 2004 Intestinal Secretion and Absorption Ron Lynch, Ph.D 626-2472 II. Cell Growth and Differentiation : Stem cells are located in the crypts. Epithelial cell turnover at the tip of a villus is high (3-6 day cycle), and a significant rate of migration of cells from the crypts is necessary to replace lost cells. As cells move from the crypts, changes in cell function occur: the absorptive capacity and the level of brush border enzymes both increase dramatically. Therefore, any process that increases cell death at the tip or slows differentiation in the crypts will reduce absorptive capacity eventually leading to diarrhea. Since mucosal stem cells divide rapidly, interventions which alter the cell cycle lead to absorptive disorders. III. Secretions of the Colon and Small Intestine Single mucus secreting cells (Goblet cells) are found throughout the intestine. The Crypts of Lieberkuhn are present but less extensive in the colon. In the colon, crypts contain goblet cells and stem cells as in the small intestine, however, no endocrine cells are observed. Mucus represents the largest component of colonic secretions acting to protect the colon wall and cause fecal material to adhere together. Normally there is net water absorption together with HCO3 secretion to the lumen in exchange for Cl-. In addition, a low rate of water secretion at an alkaline pH protects the colon walls from acid produced by bacteria. However, in response to infection or introduction of a noxious compound into the intestine, fluid secretion into the lumen can be activated. VIP acting as a neurotransmitter activates water secretion by elevating cAMP and Cl- conductance (cAMP activated CL- Channel) within colonic and small intestinal enterocytes. Inflamation of the large intestinal wall generally leads to elevation in cell cAMP (local histamine release) which sets up an acute secretory response that causes flushing of the colon. Cholera toxin mediates profound diarrhea through this pathway. 2/17/2006 8:50 AM Absorption/02 2 May 29, 2004 Intestinal Secretion and Absorption Ron Lynch, Ph.D 626-2472 Figure: Idealized diagram demonstrating the mechanism for active water secretion in the intestines. IV. Absorption of Nutrients. Only monomers and dimers of the initial complex nutrients can be absorbed by the lumenal cells (enterocytes) of the small intestine. Therefore, in the absence of normal digestion of complex nutrients, absorption is severely limited. A. Carbohydrates: The duodenum and upper jejunum have the highest capacity to absorb simple carbohydrates. Less absorptive capacity exists in lower jejunum and ileum. Glucose and galactose are absorbed via sodium dependent transport across luminal membranes, and Na+ independent facilitative transport across the basolateral membrane. Fructose is transported via an apical Na+-independent transport mechanism. The presence of enzymes within the brush border completes the breakdown of more complex sugars into transported species. As indicated in the figure, enzymes for cleaving 1,6 (dextrinase) and 1,4 bonds (glucoamylase) are present. Substantial levels of amylase are also present in pancreatic secretions, so the brush border enzymes are not critical. On the other hand, little if any lactase is found in pancreatic secretions, so its presence in the brush border is important for cleaving lactose to glucose and galactose which can then be absorbed. 2/17/2006 8:50 AM Absorption/02 3 May 29, 2004 Intestinal Secretion and Absorption Ron Lynch, Ph.D 626-2472 Mechanisms for carbohydrate uptake across the enterocyte luminal membrane. A method for measuring the capacity for absorption is to follow uptake of the sugar like Xylose. Xylose is transported into epithelial cells via the Na+ independent fructose carrier. This sugar is not metabolized, so the amount of xylose excreted in urine after an oral load reports on the ability of intestinal epithelia to absorb it. B. Proteins. Protein digestion products are absorbed as amino acids or as dipeptides by specific transporters. Amino acid absorption occurs primarily in the duodenum and upper jejunum. A small amount of protein can be absorbed in the form of small peptides by pinocytosis. Pinocytosis can account for a significant amount of protein uptake (eg. IgG) in newborn infants but becomes very limited with age. The basic mechanism of amino acid transport is a sodium co-transport mechanism similar + to that for glucose. By coupling nutrient uptake to the Na gradient, cells use energy developed + by the Na-K ATPase to transport amino acids. In addition, uptake with Na assures net ion flux to the blood setting the driving force for water absorption. C. Fat Absorption. Fat in the diet is emulsified by mixing in the stomach and interacting with biles salts in the duodenum. As digestion of emulsified fat begins, small fat droplets coated with bile called micelles form. Micelles diffuse to the epithelial cell surface coming into contact with the brush border. The micelles are loaded with lipid soluble digestion products (monoglycerides, fatty acids, cholesterol) allowing them to diffuse across the enterocyte apical membrane. Bile salts are not absorbed, but rather remain within the intestinal lumen to ferry more lipid digestion products to the brush border until they reach the ileum. 2/17/2006 8:50 AM Absorption/02 4 May 29, 2004 Intestinal Secretion and Absorption Ron Lynch, Ph.D 626-2472 A small amount of short to medium chain length fatty acids (<8 carbons) can be released from enterocytes directly into the portal blood. However, once inside the epithelial cells, most fragments of lumenal lipid digestion are resynthesized to triglycerides, cholesterol esters and phospholipids. The resynthesized fat products are accumulated into vesicles which are coated with h-lipoprotein to enhance their solubility. This vesicular structure is referred to as a chylomicron. Chylomicrons are moved from the cell by exocytosis into the interstitial space of the villus passing from the interstitial space into lymphatic vessels and eventually into the venous circulation via the thoracic duct. Thus, lymphatic flow greatly increases during absorption of a fatty meal. In addition to chylomicrons, very low density lipoproteins (VLDL) also are formed in intestinal epithelia, and are an important carrier for transport of cholesterol to blood via the lymphatics. However, chylomicrons are the primary carrier of dietary lipids to the systemic circulation. V. i. Ion Absorption + + Sodium Absorption: Na is absorbed along the entire intestine, although the bulk of Na is + + reabsorbed in the jejunum (60-80%). Na absorption is dependent on the Na gradient generated by the basolateral Na-K ATPase. H2O movement is critically + linked to Na+ absorption. Na moves into epithelial cells down its electrochemical gradient through the apical (luminal) membrane by co-transport with nutrients, via + + + + Na /H exchange or through Na channels (primary route in jejunum). Na is actively transported across the basolateral membrane to the interstitial space by the Na-K ATPase. H2O follows NaCl down the osmotic gradient. ii. Chloride Absorption. The absorption of Cl- is passive in the proximal intestine where tight junctions between cells are leaky. In the jejunum, Cl- moves passively through + paracellular pathways to offset net positive charge movement caused by rapid Na uptake coupled with nutrient absorption. As the epithelia become less leaky in the distal intestine, electroneutral transport of Cl- across the lumenal membrane becomes important for its absorption to the blood.. In the ileum and colon, uptake of Cl- across the lumen membrane occurs through a HCO3 coupled antiport mechanism. This mechanism is electroneutral, and provides increased capacity for buffering bacterial H+ production. Carbonic anhydrase has been found in colonic enterocytes, and is likely important in facilitating HCO3- production, and thereby a favorable chemical gradient for HCO3 movement to the lumen coupled to Cl- absorption into the cells. 2/17/2006 8:50 AM Absorption/02 5 May 29, 2004 Intestinal Secretion and Absorption Ron Lynch, Ph.D 626-2472 OVERVIEW Mechanism + Location Na Channels Distal Intestine; Colon Na+ -Substrate Transporters Proximal Intestine to Ileum Na+ / H+ High in Proximal Intestine, low in Colon : Aldosterone: Increases # Na+ Channels and NKA and thereby Increases Na+Absorption which is particularly important for regulating water absorption in the colon. Cl- Absorption Paracellular: Proximal Intestine Cl- / HCO3 Distal/Colon The largest fraction of Na+ is absorbed into the villus enterocytes through Na+ channels, however significant amounts are absorbed via Na+ -coupled co-transporters. The Na-K ATPase removes this “absorbed” Na+ to the blood. Cl- moves to the blood via paracellular pathways to maintain electroneutrality. 2/17/2006 8:50 AM Absorption/02 6 May 29, 2004 Intestinal Secretion and Absorption Ron Lynch, Ph.D 626-2472 Ileal/Colonic Absorption: Na+ uptake remains the driving force for water reabsorption, however the number of Na+ channels and Na+/H+ exchangers are much lower. Moreover, Cl/HCO3 exchange is relatively more important due to the need for net HCO3 secretion to neutralize H+ production by bacteria iv. Calcium Absorption. Ca2+ uptake is critically dependent on active transport via the basolateral Ca2+ ATPase, as well as, a wide range of Ca2+ binding proteins which reside within the enterocytes. Transport of calcium from lumen to blood occurs primarily in the proximal intestine. Initially, calcium moves passively from the lumen into the cell down its electrochemical gradient. After entry, Ca2+ binds to a range of Ca2+ binding proteins some which are housed in intracellular stores. This sequestration keeps the free Ca2+ concentration low within the cell. Calcium is pumped to the blood primarily via a Ca2+ ATPase and secondarily by Na+-Ca2+ exchange on the basolateral membrane. Therefore, the capacity for Ca2+ uptake is primarily dependent on the expression of both the level of Ca2+ ATPase and Ca2+ binding proteins. 2/17/2006 8:50 AM Absorption/02 7 May 29, 2004 Intestinal Secretion and Absorption Ron Lynch, Ph.D 626-2472 Hormonal Regulation of Ca2+ absorption. Vitamin D3 acts to stimulate the uptake of calcium by increasing expression of Ca2+ binding proteins and Ca2+ ATPase molecules. Parathyroid Hormone acts to promote calcium uptake by enhancing renal formation of Vitamin D3 (1, 25 dihydroxycholecalciferol). iv. Absorption of Water: About 90 - 95% of water (re)absorption takes place in the small intestine in association with nutrient (ion linked) absorption. The remaining 1-2 L/day is absorbed in the colon. Water permeability in the colon is low, so it is at this level that regulation of stool water content takes place under normal conditions. A normal colon can reabsorb a maximum of about 4.5 liters of H2O per day. Rapid equilibration of H2O between lumen and blood occurs in the proximal intestinal tract following the rules of osmosis. In the duodenum chyme is quickly brought to isotonicity. Ingestion of a hypotonic meal leads to rapid movement of water to blood with isotonicity of the chyme reached prior to the jejunum. Water permeability decreases from proximal to distal small intestine, and the colon has the lowest permeability. The mechanism of H2O absorption is based on the Theory of Standing Gradient Osmosis. The driving force is the Na+ that is pumped into the lateral extracellular space by the Na+ - K+ ATPase. Cl- follows Na+ by diffusion through intercellular junctions, or facilitative transport as in the colon. These ion movements create hypertonic fluid near the lumenal end of the lateral intercellular space creating a gradient for water movement into the lateral spaces. 2/17/2006 8:50 AM Absorption/02 8 May 29, 2004 Intestinal Secretion and Absorption Ron Lynch, Ph.D 626-2472 Pathophysiology of Diarrhea. Objectives: 1. Identify why changes in motility, absorption and secretion work together to alter colonic transit. 2. Understand how water absorption can be modified and how such alterations can lead to diarrhea and constipation. The causes of Diarrhea can be delineated into 3 categories which may be inter-related depending on the type of primary insult: Defects in Absorption, Secretion, or Motility. Since intestinal contents are relatively high in K+, profound diarrhea is associated with both hypokalemia, as well as, systemic dehydration. 1. Motility. Factors that alter the normal transit of a meal through the alimentary canal will effect the consistency of the fecal contents. Therefore, decreases in motility are correlated with constipation (more time for water removal), whereas increases in motility are correlated with diarrhea. Sedatives (codeine) and pregnancy (progesterone) elicit decreases in motility and are associated with constipation. 2. Absorptive. Any treatment or infection which alters the viability and/or function of the enterocytes of the small intestine will lead to elevated water flux to the colon. If this flux is greater than 4.5 L/day, then diarrhea will ensue. Generally, the volume of diarrhea is only moderate with absorptive disorders, and is diminsihed upon fasting. a. Lactase deficiency: Lactose in diary products is not digested, and therefore, can not be absorbed leading to an osmotic diarrhea. b. Ileal resection; terminal ileal disease: elevated bile salts and their metabolites (bacterial produced) in the colon are strong osmotic agents and also stimulate secretion. c. Celiac disease (Sprue; gluten sensitivity) Wheat flour contains gluten. In the absence of gluten hydrolase, gluten is converted to a toxic metabolite gliadin. Gliaden causes the destruction of enterocytes, and mucosal endocrine cells, severely limiting absorption in the jejunum. Normal motility keeps bacteria restricted mostly to the colon. Significant decreases in Motility in the small intestine which occur after surgery (use of anticholinergics) can lead to migration of bacteria into the small intestine, and this in turn can lead to a decrease in eneterocyte viability and absorptive diarrhea. Furthermore, patients using H2 antagonists or other inhibitors of HCl secretion are susceptible to parasitic and bacterial infections which can lead to absorptive problems. 2/17/2006 8:50 AM Absorption/02 9 May 29, 2004 Intestinal Secretion and Absorption Ron Lynch, Ph.D 626-2472 3. Secretory. The primary mechanism for active secretion of water into the colon is coupled to the opening of apical Cl- channels. This is the "cystic fibrosis" channel. In addition, digestive (bacterial) products of bile salts act as secretagogues, though their mechanism of action is as yet unknown. Specific effectors which alter cAMP levels in enterocytes can lead to excessive secretion of ions and fluid into the colon. cAMP appears to regulate (open) the Clchannel in the colonic enterocyte luminal membrane. VIP is known to elevate cAMP in these cells during the post-prandial period. For this reason, VIP-oma's are correlated with massive secretory diarrhea. Cholera toxin stimulates intestinal secretion through the same mechanism, i.e., elevating cAMP. 2/17/2006 8:50 AM Absorption/02 10