Tissue Destruction Classification Systems
advertisement

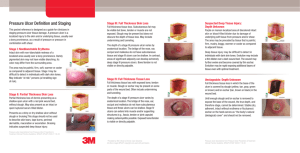
Tissue Destruction Classification Systems Assessing the level of tissue destruction in wounds can be confusing and generate several questions. Classification systems have been developed to assist with this task; however, some are specific to etiology of the wound. The purpose of this document is to help clarify how to assess the level of tissue destruction by providing information on the classification systems. All Wounds All wounds, regardless of etiology, can be assessed as either partial or full thickness. Classification of Wound by Thickness of Tissue Destruction Partial thickness © 2011 Gordian Medical, Inc. dba American Extends through the epidermis (first layer of skin), but not through dermis (second layer) Medical Technologies Full thickness © 2011 Gordian Medical, Inc. dba American Medical Technologies Extends through epidermis and dermis; may involve subcutaneous tissue, muscles, joint capsule, bone Chapter 6: The General Evaluation in Wound healing: evidence-based management, [edited by] Joseph M. McCulloch, Luther C. Kloth. 4th ed., F.A. Davis Company, Philadelphia, PA 2010. Pressure Ulcers Pressure ulcers are classified according to the most commonly accepted international classification system, which was designed uniquely for pressure ulcers and should not be used for wounds of other etiologies. International NPUAP-EPUAP Pressure Ulcer Classification System Intact skin with non-blanchable redness of a localized area usually over a bony prominence. Darkly pigmented skin may not have visible blanching; its color may differ from the surrounding area. Further description: The area may be painful, firm, soft, warmer or cooler as compared to adjacent tissue. Stage I may be difficult to detect in individuals with dark skin tones. May indicate "at risk" persons (a heralding sign of risk) Category/Stage I: Nonblanchable Erythema Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May also present as an intact or open/ruptured serum-filled blister. Further description: Presents as a shiny or dry shallow ulcer without slough or bruising.* This stage should not be used to describe skin tears, tape burns, perineal dermatitis, maceration or excoriation. Category/Stage II Category/Stage III Category/Stage IV *Bruising indicates suspected deep tissue injury Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle are not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunneling. Further description: The depth of a stage III pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow. In contrast, areas of significant adiposity can develop extremely deep stage III pressure ulcers. Bone/tendon is not visible or directly palpable. Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often include undermining and tunneling. Further description: The depth of a stage IV pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow. Stage IV ulcers can extend into muscle and/or supporting structures (e.g., fascia, tendon or joint capsule) making osteomyelitis possible. Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green or brown) and/or eschar (tan, brown or black) in the wound bed. Further description: Until enough slough and/or eschar is removed to expose the base of the wound, the true depth, and therefore stage, cannot be determined. Stable (dry, adherent, intact without erythema or fluctuance) eschar on the heels serves as "the body's natural (biological) cover" and should not be removed. Unstageable Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue. Further description: Deep tissue injury may be difficult to detect in individuals with dark skin tones. Evolution may include a thin blister over a dark wound bed. The wound may further evolve and become covered by thin eschar. Evolution may be rapid exposing additional layers of tissue even with optimal treatment. European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel. Prevention and treatment of pressure ulcers: clinical practice guideline. Washington DC: National Pressure Ulcer Advisory Panel; 2009. www.npuap.org. Venous Ulcers The CEAP Classification of venous ulcer disease is a consensus statement, of which the C, or clinical signs component is most frequently used. The C is based upon examination, whereas the other components (E, A, P) require noninvasive vascular testing. CEAP Classification Class C- Clinical signs 6 Grades, supplemented by (S) for symptomatic or (A) for asymptomatic presentation Symptoms: pain, aching, tightness, skin irritation, heaviness, muscle cramps or other complaints due to venous dysfunction Example: C3A E- Etiologic factors A- Anatomic distribution P- Pathophysiologic dysfunction Descriptors C0: No visible or palpable signs of venous disease C1: Telangiectasies or reticular veins C2: Varicose veins; distinguished from reticular veins by having 3mm or more diameter C3: Edema C4: Changes in skin & subcutaneous tissue C4a: Pigmentation or eczema C4b: Lipodermatosclerosis or atrophie blanche C5: Healed venous ulcer C6: Active venous ulcer Ec: Congenital Ep: Primary Es: Secondary (postthrombotic) En: No venous cause identified As: Superficial veins Ap: Perforator veins Ad: Deep veins An: No venous location identified Pr: Reflux Po: Obstruction Pr,o: reflux & obstruction Pn: No venous pathophysiology identifiable Eklöf B, Rutherford RB, Bergan JJ et al. Revision of the CEAP classification for chronic venous disorders: consensus statement. J Vasc Surg. 2004;40:1248-52. Sibbald RG, Williamson D, Contreras-Ruiz J et al. Venous Leg Ulcers. In: Krasner DL, Rodeheaver GT, Sibbald RG, eds. Chronic Wound Care: A Clinical Source Book for Healthcare Professionals , 4th ed. Malvern, Pa: HMP Communications, 2007:429-442. The venous clinical severity score (VCSS) augments the CEAP classification by assessing a patient’s health related quality of life as a result of the symptoms of chronic venous insufficiency (CVI). Scoring is based on ten clinical attributes that are ranked from zero to three as demonstrated by the following table. Venous Clinical Severity Score (VCSS) MODERATE = 2 ABSENT = 0 MILD = 1 SEVERE = 3 ATTRIBUTE PAIN None VARICOSE VEINS None VENOUS EDEMA None Evening ankle swelling SKIN PIGMENTATION None Diffuse, but limited in area and old (brown) INFLAMMATION None INDURATION None Mild cellulitis, limited to marginal area around ulcer Focal, circummalleolar NUMBER OF ACTIVE ULCERS ACTIVE ULCER DURATION ACTIVE ULCER DIAMETER COMPRESSION THERAPY 0 1 Diffuse over most of gaiter distribution (lower third) or recent pigmentation (purple) Moderate cellulitis, involves most of gaiter (lower third) Medial or lateral, less than lower third of leg 2 None <3 months >3 months, <1 year Not healed >1 year None <2 cm 2-6 cm >6 cm Not used or patient not compliant Intermittent use of stockings Wears elastic stocking Full compliance, most days stockings + elevation Occasional, not restricting activity or requiring pain medication Few scattered Daily moderate activity limitation; occasional pain medication Multiple; great saphenous veins, confined to calf and thigh Afternoon swelling, above ankle Dail, severe limiting activities or requiring regular use of pain medications Extensive: thigh and calf or great and small saphenous distribution Morning swelling above ankle and requiring activity change, elevation Wider distribution (above lower third) plus recent pigmentation Severe cellulitis (lower third and above) or significant Entire lower third of leg or more >2 Collins KA. Classification of lower extremity chronic venous disorders. In: UpToDate, Basow DS (ed), UpToDate, Waltham, MA, 2010. Ricci MA et al. Evaluating chronic venous disease with a new venous severity scoring system. J Vasc Surg. 2003;38:909-915. Available via American Venous Forum at: https://openaccess.leidenuniv.nl/bitstream/1887/1578/1/303_071.pdf . Accessed 2/26/11. Diabetic Foot Ulcers There are two commonly accepted classification systems for diabetic foot ulcers that were developed to guide future surgical treatment and protocols. The Wagner scale, which was developed first, incorporates depth, presence of cellulitis /abscess formation/osteomyelitis and aspects of arterial circulation by assessing gangrene levels. Wagner Scale for Diabetic Foot Ulcers Grade Description Grade 0 Pre-ulcerous lesion, healed ulcer, bony deformity Grade 1 Superficial ulcer without subcutaneous tissues involvement Grade 2 Grade 3 Deep ulcer, penetration through the subcutaneous tissue; may have exposed bone, tendon or ligament or joint capsule Deep ulcer with cellulitis, abscess formation, or osteomyelitis Grade 4 Localized gangrene of digit Grade 5 Extensive gangrene involving whole foot Wagner FW. The Dysvascular Foot: A system for diagnosis and treatment. Foot & Ankle 1981;2(2):64-122. The University of Texas system stages diabetic foot wounds based on depth of the ulcer and whether the wound is infected, ischemic, or both. 0 University of Texas Classification System of Diabetic Foot Ulcers II III I A Pre-or post-ulcerative lesion Superficial wound, not involving tendon, capsule, or bone Wound penetrating to tendon or capsule B Pre-or post-ulcerative lesion Pre- or post-ulcerative lesion, completely epithelialized with infection Superficial wound, not involving tendon, capsule, or bone with infect C Pre- or post-ulcerative lesion, Superficial wound, not involving completely epithelialized tendon, capsule, or bone with with ischemia ischemia Wound penetrating to tendon or capsule with ischemia D Pre- or post-ulcerative lesion, Superficial wound, not involving completely epithelialized tendon, capsule, or bone with with infection and ischemia infection and ischemia Wound penetrating to tendon or capsule with infection and ischemia Armstrong DG, Lavery LA, Harkless LB. Validation of a diabetic wound classification system. Diabetes care 1998;21(5):855-858.