Classification of Pressure Ulcers
advertisement

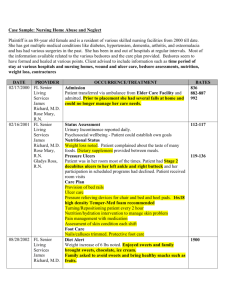
Classification of Pressure Ulcers Definition of pressure ulcers— A localised injury to the skin and/or underlying tissue, usually over a bony prominence, resulting from pressure, or pressure and shear. Category 1—Nonblanchable Intact skin with non– blanchable erythema (redness ) of a localised area usually over a boney prominence. Category 3—Full thickness skin loss Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle are not exposed. Depth may vary depending on location in body. Category 2—Partial thickness Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound without slough. Maybe intact or open blister Category 4— Full thickness tissue loss Full thickness tissue loss with exposed bone, tendon or muscle. Slough may be present. Depth may vary depending on location in body. Unstageable/ unclassified Full thickness tissue loss, in which the actual depth of the ulcer is completely obscured by slough and or eschar in the wound bed and no underlying structure is visible. Should be categorised 3. Suspected deep tissue injury This is purple or maroon localised area of discoloured intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear. Can only be classified once additional layers of tissues have been exposed. Can be category 2,3 or 4. Differences between a pressure ulcer and moisture Pressure Ulcer Moisture Lesion Further notes Causes Pressure and/ or shear must be present. Moisture must be present (e.g. shinning, wet skin caused by urinary incontinence or diarrhoea). If moisture and pressure/shear are present. The lesion is then a combined lesion. (report as moisture and pressure ulcer) Location A wound over a bony prominence It may occur over boney prominence. Pressure and shear should be excluded as causes. A moisture lesion will be superficial often multiple must be in an area where moisture is present due to incontinence. It is possible to develop pressure ulcers where soft tissue is compressed ( e.g. by a nutritional tube, nasal oxygen tube, urinary catheter) Shape Circular wounds or wounds with regular shape. If Diffuse, different superficial spots are more likely to Irregular wound shapes are often combined. The distinction lesion is limited to one spot it is likely to be a be moisture. In a kissing ulcer (copy lesion) at least between friction and pressure ulcer should be made based on histopressure ulcer. one of the wounds is most likely to be moisture ry and observation. ( urine, faeces, transpiration or wound exudate) Depth Category 2—Partial thickness skin loss (top layer of skin). Category 3 or 4—full thickness skin loss (all layers of skin). Moisture lesion are superficial (partial thickness skin loss). If infected it can be enlarged/ deepened. Necrosis Black necrotic scab = category 3 or 4. No necrosis in a moisture lesion. Necrosis soften up and changes colour but is never superficial. Distinction should be made between a black necrotic scab and a dried up blood blister. Edges Edges to be distinct. Diffuse or irregular edges. Jagged edges seen in moisture lesions that exposed to friction. Colour Red skin, non-blanchable. Can have red in wound Red skin. Pink or white surrounding skin. bed= category 2, 3 or 4. Yellow (softened necrosis) in wound bed = category 3 or 4. Black in wound bed = category 3 or 4. Green in wound bed = infection.