Respiratory Emergency Protocol
advertisement

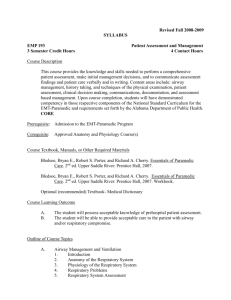
RESPIRATORY EMERGENCIES GENERAL CONSIDERATIONS A. There are a number of different treatments for respiratory distress depending on the cause. Some of these interventions can be dangerous if given to the wrong person. It is therefore important to try to determine the cause as accurately as possible. B. This protocol includes management of the following respiratory emergencies: 1. Apneic patient 2. Airway obstruction 3. Wheezing 4. Rales / pulmonary edema C. General assessment and management of all patients in respiratory distress should include: 1. Assess and manage airway: a. Administer oxygen as needed to treat shock and/or respiratory distress b. Apply pulse oximeter and treat per pulse oximeter procedure c. Be prepared to assist ventilations 2. Evaluate patient’s general appearance, relevant history of condition and determine OPQRSTI and SAMPLE. Especially ask about the severity of the patient’s underlying disease. When was the last time they seen by a doctor or hospitalized for this? Ever intubated? Ask about medication compliance. 3. Try to obtain patient’s resuscitation status (i.e., DNR Comfort Care or DNR Comfort Care Arrest). Intubation is an aggressive treatment and may be against the patient’s wishes. 4. Auscultate lung fields anteriorly, comparing side-to-side, and posteriorly when possible. (i.e., patient is able to sit up) 5. Allow patient to assume position of comfort 6. Contact Medical Control, advise of patient condition and TRANSPORT immediately unless an ALS unit is en route with an ETA < 5 minutes. APNEIC PATIENT Basic EMT A. Patient’s airway is open, breathing absent, pulse present: Provide positive-pressure ventilations with 100% oxygen. Each breath is delivered over one second with enough volume to cause chest rise 1. Pediatric rate: one breath every 3-5 seconds 2. Adult rate: one breath every 5-6 seconds Advanced EMT / Paramedic A. Secure airway. Refer to Advanced Airway Procedures. B. Place patient on cardiac monitor C. Start IV normal saline, TKO D. Transport Effective 9/3/15 Replaces 7/1/11 Respiratory Emergencies Page 1 of 4 OBSTRUCTED AIRWAY Basic & Advanced EMT A. Foreign body obstruction; patient able to speak / cough: 1. Reassure patient 2. Allow patient to attempt clearing airway by self B. Foreign body obstruction; patient unable to cough / speak, airway obstructed: 1. Adult / Child > 1 year old: Deliver abdomen / chest thrusts. Repeat until effective or patient becomes unresponsive 2. Infant (< 1 year of age): Deliver series of five backblows and five chest thrusts. Repeat until effective or patient becomes unresponsive 3. If patient becomes unresponsive, begin CPR per current AHA guidelines. Look in mouth when opening airway during CPR. Use finger sweeps ONLY to remove visible foreign body. 4. If airway cannot be cleared in 60 seconds, transport immediately to nearest appropriate hospital C. Airway obstruction due to medical cause (epiglottitis, croup, anaphylaxis) treat underlying cause 1. Croup (barking cough, stridor, retractions, typically between 6 months and 4 years old, more prevalent in fall and winter): Keep patient upright, administer humidified oxygen if available 2. Epiglottitis (sudden onset, drooling, sore throat, muffled voice, stridor): Transport upright immediately. Do NOT agitate the child. Do NOT examine throat. Advanced EMT A. Suspected croup: consider epinephrine 1:1000 0.5 mg/kg (max 5mg or 5ml) administered by nebulizer / aerosol. Paramedic A. Foreign body airway obstruction not relieved by manual maneuvers - try to visualize obstruction with laryngoscope and remove foreign body with Magill forceps if possible B. If airway cannot be cleared – perform a cricothyroidotomy (must contact Medical Control for pediatric patients) Effective 9/3/15 Replaces 7/1/11 Respiratory Emergencies Page 2 of 4 WHEEZING Basic EMT A. If suspected allergic reaction / anaphylaxis, See Allergic Reaction / Anaphylactic Shock Protocol B. Consider CPAP for adult patients. See CPAP Procedure C. May assist with prescribed metered-dose inhaler (MDI) 1. Assure that medication is prescribed for patient 2. Check medication – dose, expiration date 3. Administer MDI by having patient exhale, then activate device during inhalation and patient hold breath so that medication can be absorbed. Advanced EMT A. Suspected asthma or bronchitis administer: 1. Duoneb (ipratropium bromide 0.5 mg and albuterol sulfate 3 mg in 3 ml) aerosol: a. Adolescent and Adult Dose: 3ml by nebulizer / aerosol b. Child Dose: 1.5 ml by nebulizer / aerosol 2. If additional treatments are required, administer albuterol aerosols prn B. Suspected bronchiolitis (typically child < 2 years, history of RSV, nasal secretions, low-grade temperature, frequently occurs in winter months) – consider epinephrine 1:1000 0.5 mg/kg (max 5mg or 5ml) administered by nebulizer / aerosol. Paramedic A. Consider methylprednisolone (Solu-Medrol) : 1. Adult Dose: 125 mg Slow IVP 2. Pediatric Dose: 2 mg/kg Slow IVP B. If patient condition continues to deteriorate, consider epinephrine, 1:1000 1. Adult Dose: 0.3 mg IM 2. Pediatric Dose: 0.01 mg/kg IM Do not administer if patient is pregnant or has history of heart disease. C. Intubate as indicated. Consider administering midazolam (Versed) prior to intubation. See Procedural Sedation Protocol Effective 9/3/15 Replaces 7/1/11 Respiratory Emergencies Page 3 of 4 PULMOMARY EDEMA Pulmonary edema is most commonly associated with acute myocardial infarction but it can also result from pulmonary infections, inhaled toxins, narcotic overdose, pulmonary embolism, and decreased atmospheric pressure. Acute pulmonary edema can develop rapidly in the elderly. Pulmonary edema causes severe dyspnea associated with congestion. Other signs and symptoms include: • Rapid, labored breathing • Cough with blood-stained sputum or pink, frothy sputum • Cyanosis • Moist crackles on auscultation of lung fields; severe cases may have rhonchi • Accessory muscle use Basic EMT A. Consider CPAP for adult patients. See CPAP Procedure. Advanced EMT A. Obtain IV access – Normal Saline, TKO B. Place on cardiac monitor C. Administer Nitroglycerin 0.4 mg SL, one every 5 minutes to a maximum of 3 doses. HOLD if SPB < 100 mmHg Paramedic A. Consider administering 2-5 mg morphine slow IVP or fentanyl 50-100 mcg slow IVP if patient still in respiratory distress, anxious AND SBP remains > 100 mmHg B. Intubate as indicated. Consider administering midazolam (Versed) prior to intubation. See Procedural Sedation Protocol. Effective 9/3/15 Replaces 7/1/11 Respiratory Emergencies Page 4 of 4 KEY RESPIRATORY EMERGENCIES ABDOMINAL PAIN / NAUSEA APNEIC PATIENTS VOMITING BASIC EMT ADVANCED EMT PARAMEDIC MED CONTROL ASSESS AIRWAY OPEN AND MANAGE AIRWAY IF AIRWAY IS OPEN, BREATHING IS ABSENT MAINTAIN O2 SATS >95% AND A PULSE IS PRESENT: PROVIDE POSITIVEEVALUATE PATIENT CONDITION PRESSURE VENTILATIONS WITH OXYGEN. MONITOR VITAL SIGNS DELIVER EACH BREATH OVER ONE SECOND o HYPOPERFUSION (BP < 100 SYSTOLIC) WITH ENOUGH VOLUME TO CAUSE CHEST RISE OBTAIN MEDICAL HISTORY Oo PEDIATRIC RATE: ONE BREATH EVERY 3-5 NAUSEA/VOMITING SECONDS o SURGERY Oo ADULT RATE: ONE BREATH EVERY 5-6 TRAUMA SECONDS REASSURE PATIENT MAINTAIN O2 SATS >95% GIVE NOTHING BY MOUTH EVALUATE PATIENT CONDITION TRANSPORT IN POSTIION OF COMFORT OBTAIN MEDICAL HISTORY o SEVERITY OF UNDERLYING DISEASE? o EVER SEEN PHYSICIAN OR HOSPITALIZED FOR THIS? o HAS THE PATIENT EVER BEEN INTUBATED? o MEDICATION COMPLIANCE? o DNR STATUS? MONITOR VITAL SIGNS REASSURE PATIENT TRANSPORT SECURE AIRWAY. REFER TO ADVANCED AIRWAY IV NS (RUN TO MAINTAIN PERFUSION) PROCEDURES. MONITOR ECG IV NS (BOLUS AS MANAGEMENT NEEDED TO MAINTAIN PERFUSION) CONSIDER PAIN PROTOCOL MONITOR ECG P E D I A T R I C S RESPIRATORY EMERGENCIES ABDOMINAL PAIN / NAUSEA APNEIC PATIENTS VOMITING KEY BASIC EMT ADVANCED EMT PARAMEDIC MED CONTROL ASSESS AIRWAY OPEN AND MANAGE AIRWAY IF AIRWAY IS OPEN, BREATHING IS ABSENT AND MAINTAIN O2 SATS >95% AEVALUATE PULSE IS PRESENT: PROVIDE POSITIVEPATIENT CONDITION PRESSURE VENTILATIONS WITH OXYGEN. MONITOR VITAL SIGNS DELIVER EACH BREATH OVER SECOND o HYPOPERFUSION (BP < 100ONE SYSTOLIC) WITH ENOUGH VOLUME TO CAUSE CHEST RISE OBTAIN MEDICAL HISTORY Oo PEDIATRIC RATE: ONE BREATH EVERY 3-5 NAUSEA/VOMITING o SECONDS SURGERY MAINTAIN O2 SATS >95% o TRAUMA EVALUATE REASSUREPATIENT PATIENTCONDITION OBTAIN MEDICAL GIVE NOTHING BYHISTORY MOUTH oTRANSPORT SEVERITYIN OFPOSTIION UNDERLYING DISEASE? OF COMFORT o EVER SEEN PHYSICIAN OR HOSPITALIZED FOR THIS? o HAS THE PATIENT EVER BEEN INTUBATED? o MEDICATION COMPLIANCE? o DNR STATUS? MONITOR VITAL SIGNS REASSURE PATIENT TRANSPORT SECURE AIRWAY. REFER TO ADVANCED AIRWAY IV NS (RUN TO MAINTAIN PERFUSION) PROCEDURES. MONITOR ECG IV NS (BOLUS AS MANAGEMENT NEEDED TO MAINTAIN PERFUSION) CONSIDER PAIN PROTOCOL MONITOR ECG RESPIRATORY EMERGENCIES ABDOMINAL PAIN / NAUSEA OBSTRUCTED AIRWAY VOMITING KEY BASIC EMT ADVANCED EMT ASSESS AIRWAY OPEN AND MANAGE AIRWAY MAINTAIN O2 SATS >95% FOREIGN BODY OBSTRUCTION: PATIENT CONDITION oEVALUATE IF PATIENT ABLE TO SPEAK / COUGH – ALLOW MONITOR SIGNS CLEARING AIRAWAY BY PATIENTVITAL TO ATTEMPT o SELF HYPOPERFUSION (BP < 100 SYSTOLIC) OBTAIN MEDICAL HISTORY oo IF PATIENT UNABLE TO SPEAK / COUGH – NAUSEA/VOMITING ADULT– DELIVER ABDOMINAL THRUSTS. o SURGERY REPEAT UNTIL EFFECTIVE OR PATIENT IS o TRAUMA UNRESPONSIVE REASSURE PATIENT NOTHING BY MOUTH BEGIN CPR. FINGER oGIVE IF PATIENT UNRESPONSIVE TRANSPORT IN COMFORT SWEEP ONLY POSTIION TO REMOVEOF VISIBLE FOREIGN BODY. TRANSPORT TO NEAREST APPROPRIATE HOSPITAL IF UNABLE TO CLEAR AIRWAY IN 60 SECONDS ATTEMPT TO VISUALIZE OBSTRUCTION WITH IF NAUSEA AND VOMITING PRESENT LARYNGOSCOPE AND REMOVE WITH MAGILL FORCEPS. ADMINISTER ONDANSETRON (ZOFRAN) 4MG SLOW IV IF AIRWAY CAN NOT BE CLEARED PERFORM PUSH OR IM CRICOTHYROIDOTOMY PARAMEDIC MED CONTROL RESPIRATORY EMERGENCIES ABDOMINAL PAIN / NAUSEA OBSTRUCTED AIRWAY VOMITING BASIC KEY BASIC EMT ADVANCED EMT PARAMEDIC P E D I A T R I C S ASSESS AIRWAY OPEN AND MANAGE AIRWAY MAINTAIN O2 SATS >95% FOREIGN BODY OBSTRUCTION: PATIENT CONDITION oEVALUATE IF PATIENT ABLE TO SPEAK / COUGH – ALLOW MONITOR VITAL SIGNS PATIENT TO ATTEMPT CLEARING AIRAWAY BY o SELF HYPOPERFUSION (BP < 100 SYSTOLIC) OBTAIN MEDICAL HISTORY oo IF PATIENT UNABLE TO SPEAK / COUGH – NAUSEA/VOMITING CHILD > 1 YEAR OLD – DELIVER ABDOMINAL o SURGERY THRUSTS. REPEAT UNTILL EFFECTIVE OR o TRAUMA PATIENT IS UNRESPONSIVE REASSURE PATIENT INFANT < 1 YEAR OLD – DELIVER SERIES OF GIVE NOTHING BY MOUTH FIVE BACKBLOWS AND FIVE CHEST TRANSPORT IN POSTIION OF COMFORT THRUSTS. REPAT UNTILL EFFECTIVE OR PATIENT IS UNRESPONSIVE o IF PATIENT UNRESPONSIVE BEGIN CPR. FINGER SWEEP ONLY TO REMOVE VISIBLE FOREIGN BODY. o IF AIRWAY OBSTRUCTION DUE TO MEDICAL CAUSE- TREAT UNDERLYING CAUSE CROUP – KEEP PATIENT UPRIGHT, ADMINSTER HUMIDIFIED OXYGEN IF AVAILABLE EPIGLOTITIS – TRANSPORT UPRIGHT IMMEDIATELY. DO NOT AGITATE THE CHILD. DO NOT EXAM THE THROAT. TRANSPORT TO NEAREST APPROPRIATE HOSPITAL IF UNABLE TO CLEAR AIRWAY IN 60 SECONDS ADMINISTER EPINEPHRINE 1:1000 0.5 MG/KG (MAX 5 IV NS (RUN TO MAINTAIN PERFUSION) MG OR 5 ML) IN NEBULIZER / AEROSAL FOR CROUP MONITOR ECG PATIENT. CONSIDER PAIN MANAGEMENT PROTOCOL ATTEMPT TO VISUALIZE OBSTRUCTION WITH IF NAUSEA AND VOMITING PRESENT LARYNGOSCOPE AND REMOVE WITH MAGILL FORCEPS. ADMINISTER ONDANSETRON (ZOFRAN) 4MG SLOW IV PUSH OR IM IF AIRWAY CANPERFUSION) NOT BE CLEARED IVPEDIATRIC NS (RUN TO MAINTAIN PERFORM CRICOTHYROIDOTOMY MONITOR ECG MED CONTROL RESPIRATORY EMERGENCIES ABDOMINAL PAIN / NAUSEA WHEEZING VOMITING KEY BASIC EMT ADVANCED EMT PARAMEDIC ASSESS AND MANAGE AIRWAY OPEN AND MANAGE AIRWAY MAINTAIN O2 SATS >95% MAINTAIN O2 SATS >95% EVALUATE EVALUATE PATIENT PATIENT CONDITION CONDITION OBTAIN MEDICAL HISTORY MONITOR VITAL SIGNS oo SEVERITY OF UNDERLYING HYPOPERFUSION (BP < 100 DISEASE? SYSTOLIC) oOBTAIN EVERMEDICAL SEEN PHYSICIAN HISTORY OR HOSPITALIZED THIS? o FOR NAUSEA/VOMITING oo HAS THE PATIENT EVER BEEN INTUBATED? SURGERY oo MEDICATION COMPLIANCE? TRAUMA o DNR STATUS? REASSURE PATIENT MONITOR VITALBY SIGNS GIVE NOTHING MOUTH REASSURE PATIENT TRANSPORT IN POSTIION OF COMFORT IF LUNG SOUNDS REVEAL WHEEZES: o CONSIDER CPAP FOR ADULT PATIENTS o ASSIST PATIENT WITH PRESCRIBED METERED-DOSE-INHALER IF AVAILABLE o IF ALLERGIC REACTION / ANAPHYLAXIS SUSPECTED – SEE ALLERGIC REACTION / ANAPHYLAXIS PROTOCOL TRANSPORT FOR ASTHMAPERFUSION) / BRONCHITIS: IV NSSUSPECTED (RUN TO MAINTAIN ADMINISTER IPATROPIUM BROMIDE (ATROVENT) MONITOR ECG 0.5 MG AND PAIN ALBUTEROL SULFATE (PROVENTIL) CONSIDER MANAGEMENT PROTOCOL 3MG IN 3ML. ADULT DOSE: 3ML BY NEBULIZER / AEROSAL ABLUTEROL AEROSALS CAN BE ADMINSTERED PRN IF FURTHER TREATMENT NEEDED. CONSIDER METHYLPREDNISOLONE (SOLUIF NAUSEA AND VOMITING PRESENT MEDROL) ADULT DOSE: ONDANSETRON 125 MG SLOW IV(ZOFRAN) PUSH ADMINISTER 4MG SLOW CONSIDER IF PATIENT REMAINS IN DISTRESS: IV PUSH OR IM EPINEPHRINE 1:1000 0.3 MG IM (DO NOT ADMINISTER IF PATIENT IS PREGNANT OR HAS HISTORY OF HEART DISEASE) INTUBATE AS INDICATED – SEE PROCEDURAL SEDATION PROTOCOL. MED CONTROL RESPIRATORY EMERGENCIES ABDOMINAL PAIN / NAUSEA WHEEZING VOMITING KEY BASIC EMT ADVANCED EMT PARAMEDIC P E D I A T R I C S MED CONTROL ASSESS AND MANAGE AIRWAY OPEN AND MANAGE AIRWAY MAINTAIN O2 SATS >95% MAINTAIN O2 SATS >95% EVALUATE EVALUATE PATIENT PATIENT CONDITION CONDITION OBTAIN MEDICAL HISTORY MONITOR VITAL SIGNS oo SEVERITY OF UNDERLYING HYPOPERFUSION (BP < 100 DISEASE? SYSTOLIC) oOBTAIN EVERMEDICAL SEEN PHYSICIAN HISTORY OR HOSPITALIZED THIS? o FOR NAUSEA/VOMITING oo HAS THE PATIENT EVER BEEN INTUBATED? SURGERY oo MEDICATION COMPLIANCE? TRAUMA o DNR STATUS? REASSURE PATIENT MONITOR VITALBY SIGNS GIVE NOTHING MOUTH REASSURE PATIENT TRANSPORT IN POSTIION OF COMFORT IF LUNG SOUNDS REVEAL WHEEZES: o ASSIST PATIENT WITH PRESCRIBED METERED-DOSE-INHALER IF AVAILABLE o IF ALLERGIC REACTION / ANAPHYLAXIS SUSPECTED – SEE ALLERGIC REACTION / ANAPHYLAXIS PROTOCOL TRANSPORT FOR ASTHMAPERFUSION) / BRONCHITIS: IV NSSUSPECTED (RUN TO MAINTAIN ADMINISTER IPATROPIUM BROMIDE (ATROVENT) MONITOR ECG 0.5 MG AND ALBUTEROL SULFATE (PROVENTIL) CONSIDER PAIN MANAGEMENT PROTOCOL 3MG IN 3ML. PEDIATRICS DOSE: 1.5 ML BY NEBULIZER / AEROSAL ABLUTEROL AEROSALS CAN BE ADMINSTERED PRN IF FURTHER TREATMENT NEEDED. FOR SUSPECTED BRONCHIOLITIS (CHILDREN < 2 YEARS OLD): ADMINISTER EPINEPHRINE 1:1000 0.5 MG/KG (MAX 5 MG OR 5 ML) IN NEBULIZER / AEROSAL FOR CROUP PATIENT. CONSIDER METHYLPREDNISOLONE (SOLU-MEDROL) IF NAUSEA AND VOMITING PRESENT PEDIATRIC DOSE: 2 MG/KG SLOW IV PUSH IF PATIENT REMAINS IN RESPIRATORY ADMINISTER ONDANSETRON (ZOFRAN)DISTRESS 4MG SLOW CONSIDER 1:1000 IV PUSH OREPINEPHRINE IM PEDIATRIC DOSE: 0.01 MG/KG IM INTUBATE AS INDICATED – SEE PROCEDURAL SEDATION PROTOCOL. RESPIRATORY EMERGENCIES ABDOMINAL PAIN / NAUSEA PULMONARY EDEMA VOMITING KEY BASIC EMT ADVANCED EMT ASSESS AND MANAGE AIRWAY OPEN AND MANAGE AIRWAY MAINTAIN O2 SATS >95% MAINTAIN O2 SATS >95% EVALUATE EVALUATE PATIENT PATIENT CONDITION CONDITION OBTAIN MEDICAL HISTORY MONITOR VITAL SIGNS oo SEVERITY OF UNDERLYING HYPOPERFUSION (BP < 100 DISEASE? SYSTOLIC) oOBTAIN EVERMEDICAL SEEN PHYSICIAN HISTORY OR HOSPITALIZED THIS? o FOR NAUSEA/VOMITING oo HAS THE PATIENT EVER BEEN INTUBATED? SURGERY oo MEDICATION COMPLIANCE? TRAUMA oREASSURE DNR STATUS? PATIENT MONITOR VITALBY SIGNS GIVE NOTHING MOUTH REASSURE PATIENT TRANSPORT IN POSTIION OF COMFORT CONSIDER CPAP FOR ADULT PATIENTS TRANSPORT IV IV NS NS (RUN (RUN TO TO MAINTAIN MAINTAIN PERFUSION) PERFUSION) MONITOR ECG MONITOR ECG ADMINISTER NITROGLYCERIN SL– ONE TABLET OR CONSIDER PAIN MANAGEMENT PROTOCOL SPRAY IF BP ABOVE 100 MMHG. MAY REPEAT TWICE IF BP REMAINS GREATER THAN 100 MMHG IF PATIENT REMAINS INVOMITING DISTRESSPRESENT AND SPB > 100 IF NAUSEA AND MMHG, ADMINISTER MORPHINE OR FENTANYL (SUBLIMAZE) ADMINISTER ONDANSETRON (ZOFRAN) 4MG SLOW INTUBATE ASIM INDICATED – SEE PROCEDURAL IV PUSH OR SEDATION PROTOCOL. PARAMEDIC MED CONTROL