ACC International Associate/ Affiliate Application
advertisement

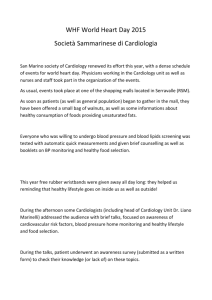
書き方のSAMPLE(日本心臓病学会 会員用) ACC International Associate/ Affiliate Application I am applying as a: ❑ Cardiovascular Specialist (International Associate Member) ✓ ❑ Non-Cardiovascular Physician/Scientist (Affiliate Member) Complete the form and return by email, post, or fax to: American College of Cardiology Member Services Department 2400 N Street, NW Washington, DC 20037, USA Email: mdavis@acc.org Fax: +1 202-375-6843 • Phone: +1 202-375-6000, ext. 5439 ✓ ❑ Male ❑ Female 10/22/1973 _____________________________ Birth Date (Month/Day/Year) Hongo University ____________________________________________________________________________________________________________________________________________________ Name of Institution Tokyo, JAPAN Internal Medicine Location (City/Country) Area of Specialization March,2000 ____________________________________________________________________________________________________________________________________________________ Graduation Date Training Program Bunkyo Hospital Name of Institution Tokyo, JAPAN Internal Medicine Location (City/Country) Area of Specialization March,2001 ____________________________________________________________________________________________________________________________________________________ Ichiro SUZUKI ____________________________________________________________________________________________________________________________________________________ (Middle Initial) Medical School ______________________________________________________________________________________________________________________________________________________ Personal Data (All Sections Must Be Completed) Full Name (First) Education, Training and Society Membership (Last) international@jcc.gr.jp ✓ ______________________________________________________________________________________________________ Please provide business or personal email addresses and check a box to indicate preferred email for ACC communications. ❑ Business ❑ Personal Dept. of Internal Medicine, Bunkyo Hospital, 4-9-22 Hongo, Bunkyo-ku ____________________________________________________________________________________________________________________________________________________ Graduation Date Japanese College of Cardiology 日本心臓病学会の会員は、この通り記入 ❑ I am a member of a recognized medical society* ______________________________________________________________________________________________________ ✓ して下さい。 Name of Society *Those without medical society memberships will need to submit a sponsor letter from a current ACC member Medical Practice or Appointments ✓ ❑ Licensed or certified to practice medicine __________________________________________________________________________________________________________ Hongo University, Tokyo JAPAN Name of Authorizing Body Preferred Address Tokyo JAPAN 113-0033 ____________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________ ❑ Academic or research appointment Name of Authorizing Body City, Province/StateCountryPostal Code +81-3-5802-0112 +81-3-5802-0118 ____________________________________________________________________________________________________________________________________________________ Office TelephoneHome TelephoneFax Please indicate your top three areas of interest relevant to your primary clinical activities by entering 1, 2, and 3 below: Principal Employment Information (For Public & Membership Directory) Dept. of Internal Medicine, Bunkyo Hospital ____________________________________________________________________________________________________________________________________________________ Institution/Practice Name Associate Professor ____________________________________________________________________________________________________________________________________________________ Title/Position 4-9-22 Hongo, Bunkyo-ku ____________________________________________________________________________________________________________________________________________________ Address Tokyo JAPAN 113-0033 ____________________________________________________________________________________________________________________________________________________ City, Province/StateCountryPostal Code +81-3-5802-0112 +81-3-5802-0118 ____________________________________________________________________________________________________________________________________________________ TelephoneAlternate TelephoneFax Which of the following best describes your work setting? ❑ Solo Practice ※個人開業 ❑ Government Hospital or Agency ※公立病院、公立機関 ❑ Industry ※民間病院、民間企業 ❑ Other (please specify) __________________________________________________________ ✓ Areas of Interest ❑ ❑ ❑ ❑ 1 ❑ ❑ ❑ ❑ ❑ ❑ ❑ ❑ Administration Adult Cardiology Adult Congenital Cardiology Anesthesiology Arrhythmias & Devices Cardiac Rehab Cardiothoracic Surgery Congenital Card. Surgery Critical Care Medicine Echocardiography Electrophysiology Emergency Medicine ❑ ❑ ❑ ❑ ❑ 2 ❑ 3 ❑ ❑ ❑ ❑ ❑ ❑ Endocrinology Family Practice General Cardiology Geriatrics/Aging Health Policy Heart Failure/Transplant Hypertension Internal Medicine Interventional CV Invasive CV Lipids Clinic MR/CT ❑ ❑ ❑ ❑ ❑ ❑ ❑ ❑ ❑ ❑ ❑ ❑ Nuclear CV Nuclear Medicine Pathology Pediatric CV Pediatric Interventional CV Pediatrics/Neonatal Pharmacology Physical Medicine Physiology Preventive CV ✓ Pulmonary Disease⎯ Radiology Research Sports & Exercise CV Thoracic Surgery Transcatheter Valve Therapy Vascular & Interventional Radiology Vascular Medicine Vascular Surgery Other ______________________________________ Public Health Membership Dues Payment Please enclose payment to ensure your application is processed. All applications are subject to a $25 one-time application fee. What is the ownership structure of your practice? ❑ Government Owned ❑ Hospital Owned ❑ Insurance Company Owned ❑ Medical School/University Owned ❑ Other (please specify) __________________________________________________________ ❑ ❑ ❑ ❑ ❑ ❑ ❑ ❑ ❑ ❑ Nephrology þ Application Fee $25 ❑ Hardcopy JACC $170 Annual Dues: ❑ CV Specialist, High-Income Country $125 ✓ ❑❑ CV Specialist, Middle/Low-Income Country $100 Payment Method: ❑ Check or money order enclosed. In US dollars drawn on a US bank. VISA, MasterCard. Discover クレジットカードの背面に記載されたメイ ンのカード番号の後に書かれた3桁の番号 ❑❑ Non-Cardiovascular Physician/Scientist, High/Mid/Low $100 ❑ ✓ ❑ ❑ MasterCard ❑ Visa ❑ American Express ❑ Discover ICHIRO SUZUKI ___________________________________________________________________________________________________________________________________________________ Cardholder Name 1234 5678 9123 4567 03/2017 891 ___________________________________________________________________________________________________________________________________________________ Card Number Expiration Date CSC #