Advance Care Planning

Queensland Health
Advance Care
Planning
Think now. Plan sooner.
Peace of mind later.
CONTENTS
Planning for your future care 4
What is advance care planning? 6
Why should I plan ahead?
Who can undertake advance care planning?
8
9
Who should make decisions on my behalf?
How do I carry out advance care planning?
10
12
Advance Health Directive 15
Enduring Power of Attorney
(EPOA)
What do I do after I complete my advance planning documents?
What if I change my mind?
Office of the Adult Guardian
Making decisions
What is capacity?
17
Can I refuse to be treated? 25
Can I insist on a particular treatment? 26
Can I put forward my spiritual or religious beliefs? 27
19
20
21
23
24
Resuscitation planning 29
What is resuscitation planning? 30
What is a life-sustaining measure? 30
Why does my doctor want to discuss resuscitation planning with me? 31
What is Cardiopulmonary
Resuscitation (CPR)? 32
What else might be involved in CPR? 33
How successful is resuscitation through CPR?
Will CPR be right for me?
34
35
What happens if an ambulance is called? 35
My rights and obligations as a substitute decision-maker 37
What is a substitute decision-maker? 38
What happens if I am asked to be someone’s decision-maker? 39
If I am a decision-maker, how long do I have to make a decision? 39
What are my legal obligations? 40
As a substitute decision-maker, what types of things should I consider? 40
2
CONTENTS
My rights and obligations as a carer
Who is a carer?
What if I’m a paid carer?
Can I be a carer and a substitute decision-maker?
What happens if I am asked to make an important decision for the person in my care?
Taking care of yourself
Special considerations
Children
Decision-making disabilities
Aboriginal and Torres Strait
Islander people
Culturally and linguistically diverse backgrounds
Mental health
Other considerations of advance care planning
45
46
46
47
47
49
53
54
54
58
61
63
67
Talking about death and dying
Talking about death and dying with children
When the time comes…
Organ and tissue donation
68
Frequently asked questions
Is it helpful to complete advance care planning documentation?
Who do I talk to about this?
75
76
76
Who should I choose to be my substitute decision-maker?
When are advance care planning documents used?
77
77
What if I become ill or I am injured while I am away from home? 78
What happens in an emergency? 78
What happens if there is disagreement after I lose capacity? 79
Do you need further information? 80
Glossary 82
69
70
72
3
PlaNNiNg fOr yOur fuTurE CarE
When you or someone close to you becomes ill, injured, disabled, or goes through a life-changing event, it can make you think about many things. Some of them aren’t easy to dwell on, such as what might happen in the future if you’re no longer able to make decisions for yourself. If you haven’t already thought about this, now might be the time to do so. The first step in advance care planning is thinking about it. For example, you might like to consider your preferences for future health care and treatment and what would be important to you at the end of life. You might also like to consider where you want to live, types of home services you want, and even planning the type of funeral you want.
The second step is to discuss your choices for future health care and any concerns you have with your doctor – seeing what is possible and planning for it. Your doctor can advise you about your options, the implication of your choices and clarify what might happen if you want to receive or refuse certain kinds of medical treatment.
4
PlaNNiNg fOr yOur fuTurE CarE
The third step is discussing the choices and decisions you have made and are still thinking about with family and friends. You might like to involve your family and friends in your decisions or you may already have firm views about what you would want.
The fourth step is optional and involves formally documenting your choices and/or nominating one or more people to make decisions on your behalf. This will involve completing some legal documents, such as an Advance Health Directive or Enduring
Power of Attorney. It is important to note that these documents will come into effect ONLY if you lose the capacity (see page 24 for a definition) to make or communicate decisions about your health care.
Advance care planning is entirely voluntary. You can change your mind and your plans (and your legal documents) at any time while you have capacity.
Please take some time to read carefully through this booklet. Even if you are fit and healthy, it is never too early to consider what health care you may want in the future.
Think now. Plan sooner. Peace of mind later.
5
WhaT iS advaNCE CarE PlaNNiNg?
Would your family, friends and doctor know what medical treatment and care you would want if you became seriously ill and could not communicate your choices? Would they know what decisions to make on your behalf? Advance care planning is the process of discussing and documenting your future health care choices.
Advance care planning is not new. Its benefits have been experienced in Australia and throughout the world for many years. It can help you to put procedures in place to ensure that your choices and decisions for future care will be heard and respected in the event you lose capacity.
Advance care planning can include:
• deciding what future health care you would want to receive
• discussing future treatment options with your doctor
• ensuring your choices to refuse particular treatments are
communicated
• discussing your decisions with your family, friends and
those you trust
6
WhaT iS advaNCE CarE PlaNNiNg?
• recording your decisions in an Advance Health Directive and/ or appointing a health attorney in an enduring document, such as an Advance Health Directive or Enduring Power of
Attorney (EPOA)
• providing copies of the documents to family, friends, your
GP and any other health care providers
• reviewing your decisions and updating your legal documents as appropriate.
Advance care planning also gives you the opportunity to discuss your beliefs and values, and helps give you peace of mind that the right thing will happen at the right time.
7
Why ShOuld i PlaN ahEad?
Discussing your values, beliefs and treatment choices with your family may not be easy for you or them because many people are uncomfortable talking about a time when they may be unwell or dying. If you find it uncomfortable, it might be easier to talk first with your doctor, community liaison nurse or social worker who can support you.
Planning ahead:
• helps to ensure your wishes are respected and the right things happen at the right time
• means your views about what you would or would not like to happen to you can be stated and respected (for example, you may want to stay at home if you become ill, or you may definitely not want certain medical treatments).
• provides an opportunity to discuss and resolve any outstanding issues about end-of-life care with your family and friends
• gives you and your family peace of mind when everyone is clear on your choices
• can help to avoid the distressing situation of health care decisions being made on your behalf in a crisis.
8
Why ShOuld i PlaN ahEad?
Who can undertake advance care planning?
Anyone aged 18 years or over can complete the formal part of advance care planning, for example completing an Advance Health
Directive and/or an EPOA.
Ideally, advance care planning should be carried out at a time when you are not seriously ill or at the end stages of life.
9
WhO ShOuld makE dECiSiONS ON my bEhalf?
Before you start the formal part of advance care planning, you may want to think about who could make decisions about your health care if you are unable to make these decisions yourself.
Many people select a close family member, but you can select anyone you think could best represent your interests. You may also wish to legally nominate someone for this role. This will require more formal procedures and you may need to see a lawyer.
Keep in mind that you can choose more than one person for this role.
Anyone you nominate must be:
• aged 18 years or over
• trusted to follow your values and instructions
• willing to accept this responsibility
• available to take on the role if required
• able to make decisions in stressful situations
• not your paid carer or health provider.
10
WhO ShOuld makE dECiSiONS ON my bEhalf?
Before you appoint someone, you should discuss your values and beliefs with them. They need to understand and respect your choices so they can represent your best interests when the time comes. You can change or update your choices at any time if circumstances change or you change your mind.
It is also important to tell those close to you about your enduring documents (Advance Health Directive or EPOA) and where you have kept them. The same applies to any copies you have made.
Because an Advance Health Directive and EPOA are legal documents, any copies you make and give to others should be certified. This means a Justice of the Peace or lawyer has to sign each page as a true copy. While photocopies could be used to inform the decision-making when the time comes, they do not provide the basis for legal consent (like an original or certified document) and your substitute decision-maker/s will be required to make health care decisions on your behalf.
11
hOW dO i Carry OuT advaNCE CarE PlaNNiNg?
Advance care planning can be carried out in two ways:
1 informal discussions about your end-of-life choices with family and close friends
2 formally, by completing an Advance Health Directive and/or
Enduring Power of Attorney (EPOA)
1. Informal discussions with family and close friends
As long as you have clearly expressed your wishes to someone (or this could be a number of people), these wishes will be taken into consideration if you lose capacity for decision-making. You may already have clear thoughts about you want, or you may wish to talk your ideas over with others before making any choices.
In legal terms, discussing your future health care choices with family and significant others is called a ‘common law’ health directive. This means you have chosen not to formalise your choices for end-of-life care by signing legal documents and having them witnessed.
If you have chosen not to complete legal documents, then become seriously ill and lose capacity for decision-making, someone close
12
hOW dO i Carry OuT advaNCE CarE PlaNNiNg?
to you becomes your ‘statutory health attorney’. You do not need to fill out any forms to make this happen as the law automatically allows this to occur. Statutory health attorneys are the most common category of substitute decision-makers.
‘Substitute decision-maker’ is the legal term for anyone you nominate, or who is appointed, or who is allowed to make decisions on your behalf.
2. Formally, by completing an Advance Health Directive and/or
Enduring Power of Attorney (EPOA)
It’s best to make an Advance Health Directive and/or EPOA before any urgent health matters arise and before decisions are required at a stressful and emotional time. However, it is particularly important if:
• you are about to be admitted to hospital
• your medical condition is likely to affect your ability to make decisions
• you have a chronic medical condition, such as cancer, diabetes, asthma or a heart or renal condition that could result in serious complications.
13
hOW dO i Carry OuT advaNCE CarE PlaNNiNg?
Sometimes capacity can fluctuate, so decisions can be communicated in different ways, such as by actions or signs. Someone may have the capacity to make decisions about where they might want to live, but not about operations or medications.
The doctor responsible for your care will be able to determine whether or when your Advance Health Directive and/or EPOA can be activated by loss of decision-making capacity.
As long as you are capable of understanding your decisions you can change or revoke (cancel) your Advance Health Directive and/ or EPOA at any time. However, because they are legal documents you need to revoke either or both in writing.
Remember: an Advance Health Directive or an EPOA for personal and health matters cannot be activated unless you lose the capacity to make or communicate decisions for yourself.
14
hOW dO i Carry OuT advaNCE CarE PlaNNiNg?
Advance Health Directive
An Advance Health Directive is a legal document that enables you to give instructions about your health care, including special health matters, for when you are no longer able to. In effect, an
Advance Health Directive becomes your decision-maker, giving instructions at the time the document is made. An Advance Health
Directive allows you to make specific directions about the care you would want and under what circumstances. The directions in an Advance Health Directive can be very detailed, or they can be broad, outlining your beliefs and values about end-of-life matters.
You may also choose to appoint a health attorney to give directions about medical treatment outside of the scope of the Advance
Health Directive. For example, if you made specific directions about matters relating to a diagnosed condition and were admitted to hospital for an unrelated reason (such as an accident), your appointed attorney could make health care decisions on your behalf. If you have an Advance Health Directive, your choices and wishes for care will be followed in accordance with good medical practice.
15
hOW dO i Carry OuT advaNCE CarE PlaNNiNg?
Legal matters
An Advance Health Directive must be signed by you and witnessed by a Justice of the Peace, Commissioner for Declarations or a lawyer. However, there are a few other legal matters about signing and witnessing an Advance Health Directive that you should know.
An eligible witness for a person making an Advance Health
Directive must be 21 years old or over and cannot be:
• someone who signed the Advance Health Directive on behalf of the person making it
• a nominated attorney of the person
• a relation of the person or a relation of a nominated attorney
• a paid carer or health provider.
An Advance Health Directive must also include a certificate signed and dated by a doctor stating that you had capacity at the time the document was made.
16
hOW dO i Carry OuT advaNCE CarE PlaNNiNg?
You may like to ask your doctor to go through each question with you and explain anything you don’t understand. Your doctor should sign your Advance Health Directive only when they are confident you understand the decisions you have made, and their implications.
You can buy the ‘prescribed’ Advance Health Directive form from a post office or newsagency, or you can download and print it from the Department of Justice and Attorney-General website justice.qld.gov.au.
However, you don’t have to use the prescribed form if you don’t want to. An Advance Health Directive can also be a letter or other document you create. Provided the signing and witnessing requirements are followed, it is valid and, therefore, legal.
Enduring Power of Attorney (EPOA)
An EPOA is a legal document that enables you to formally appoint another person/s, called attorneys, to make financial and/ or personal (including health) decisions on your behalf.
17
hOW dO i Carry OuT advaNCE CarE PlaNNiNg?
You can nominate the same attorney/s for both financial and personal/health matters, or you can nominate separate attorneys for financial matters and personal/health matters. The law does not place limits on how many attorneys you can appoint, but there may be practical difficulties if too many people are involved closely in the decision-making and co-signing process.
If you wish to appoint the same attorney for both financial and personal/health matters, you can use the short form (‘green’ form).
If you would like to appoint an attorney for financial matters and a different attorney for personal/health matters, you’ll have to use the long form (‘blue’ form).
The EPOA document must be signed by you, and must also be witnessed and signed by a Justice of the Peace, Commissioner for Declarations, lawyer or notary public. Any witness must also declare that you appeared to understand the content of the EPOA document at the time it was written.
Just as for an Advance Health Directive, the creation of an EPOA is your responsibility and comes into effect only if you are unable to make or communicate decisions for yourself.
18
hOW dO i Carry OuT advaNCE CarE PlaNNiNg?
You can buy EPOA forms from a post office or newsagency, or you can download and print the forms from the Department of
Justice and Attorney-General website at justice.qld.gov.au.
For more information, speak to your doctor, community liaison nurse or social worker, or you can contact the Adult Guardian,
Public Trustee or a solicitor.
What do I do after I complete my advance planning documents?
It is wise to keep the original documents in a safe place at your residence. You may also consider providing certified copies to:
• your substitute decision-maker/s (health attorney/s)
• your doctor/s (including your GP)
• family member/s and/or friend/s
• the hospital where you receive treatment.
19
hOW dO i Carry OuT advaNCE CarE PlaNNiNg?
What if I change my mind?
You may want to change or revoke your Advance Health Directive or EPOA for a number of reasons. Some of these might include changes to:
• your medical circumstances
• choices for future health care, following new information
• the relationship with your appointed attorney/s
• your living arrangements and lifestyle choices
• the person/s you appointed as your attorney/s – they may no longer be appropriate for the role.
Bear in mind that having multiple copies of slightly different documents can pose difficulties for your substitute decisionmaker/s or health care team in the event that you lose capacity.
As soon as you have created your new document/s, destroy any previous originals or request they be destroyed. You can also revoke the documents by completing a new document, for example, appointing a new substitute decision-maker/s. The most recent dated document overrides the older document. Make sure you let your substitute decision-maker/s know about the changes and provide them with new documents.
20
hOW dO i Carry OuT advaNCE CarE PlaNNiNg?
Office of the Adult Guardian
Sometimes these things may seem very complicated and it becomes very difficult to know that you are making the right choices. The Adult Guardian is an independent statutory officer whose role is to protect the rights and interests of adults with impaired capacity. The Adult Guardian can act as a substitute decision-maker for individuals in the areas of personal and health decision-making. The Adult Guardian is also the Statutory Health
Attorney of last resort for all adults in Queensland.
You can contact the Adult Guardian on 1300 653 187.
The Public Advocate is an independent statutory officer who delivers systems advocacy on behalf of people with impaired capacity. The Public Advocate works to influence the way which programs, policies, legislation and services work to protect the rights and interests of vulnerable people with impaired capacity.
21
diSCuSSiNg yOur fuTurE WiShES
‘
Mr Brown has lived at an aged care facility for almost four years.
Over the years, he has noticed that his condition has become gradually worse.
When Mr Brown first arrived at the facility, he decided that he did not want to receive resuscitation if he had a respiratory or cardiac arrest. This was recorded in Mr Brown’s file.
He also enjoys living at the aged care facility and the company of the other people who live there. He often speaks about, and has made it clear that, if he became seriously ill, he would not want to be admitted to hospital and given care that he did not want.
A nurse at the aged care facility told Mr Brown that his wishes to not be admitted to hospital and receive unwanted treatment may not be followed because he has not formally documented them.
It is recommended that Mr Brown begin discussions with his family, friends and doctor so he can plan for the future and make sure his wishes are respected. He may like to consider writing an
Advance Health Directive or appointing an Enduring Power of
Attorney.
22
‘
Making Decisions
23
makiNg dECiSiONS
What is capacity?
In Australia, the law recognises a person’s right to control their own lives. People are presumed to have the capacity to make decisions for themselves unless it is established by a doctor that they do not.
Generally, someone can be regarded as having decision-making capacity if they are able to:
• understand the basic medical situation
• understand the nature of the decision, including:
— the implications - benefits, risks and what the medical
treatment entails
— alternatives to the medical treatment proposed, including the
implication of no decision.
• use or weigh up the information, such as by asking questions.
• retain the information (short-term memory).
• freely and voluntarily communicate a decision in some way
(for example, by talking, using sign language or any other means).
24
makiNg dECiSiONS
‘Impaired capacity’ refers to a person’s inability to make a sound decision in a particular area of their life. Impaired decisionmaking capacity may be due to an intellectual disability, acquired brain injury, mental illness, dementia or some other cause.
Lack of capacity will not be established using someone’s age, cultural background, behaviour, appearance or physical condition, as this leads to bias and unjustified assumptions. In cases where capacity needs to be verified, a doctor may conduct a number of simple tests. In some complicated cases, capacity assessment may also involve a psychiatric evaluation.
Sometimes people also talk about competence for decision-making.
Competence and incompetence are legal terms determined by courts and judges, whereas decision-making capacity is clinically determined by a doctor’s assessment.
Can I refuse to be treated?
Yes. As long as you have the capacity to make decisions about health matters, you have the right to refuse medical treatment, even if this may cause your death or make it happen sooner. This is an automatic right of every person and is recognised by the law.
25
makiNg dECiSiONS
Doctors have to provide you with the information you need to make an informed decision. If a doctor or health care professional has doubts about your capacity to make a decision about a particular treatment they may need to assess you.
While you have the capacity to do so, you have the right to refuse treatment even if others (for example, the health care team, or your family or friends) don’t agree with or like your decision.
Can I insist on a particular treatment?
No-one can insist on medical treatment that the doctor thinks is not appropriate, would be of no benefit to you, or cause you harm.
Doctors have to meet the standards of good medical practice, and are not obliged legally or ethically to offer or provide medical treatment that in all respects would be considered futile.
Your doctor will advise you about treatment and care appropriate for your situation, as well as the likely benefits and side-effects.
You can then decide by yourself or by talking it over with your family. You can ask about other treatment options if you want to, and you can also request a second opinion.
26
makiNg dECiSiONS
Can I put forward my spiritual or religious beliefs?
If you have spiritual or religious beliefs, it is important to express your views so they can be taken into account when you are no longer able to communicate. This can be done informally by discussing your beliefs and wishes with your substitute decisionmaker/s, or formally by completing an Advance Health Directive or EPOA.
People express their spiritual and religious feelings in different ways. Some may talk about them, while others may be quietly troubled by them. Some can make medical choices based on them that doctors may consider unreasonable. In these situations, even though spiritual questions are sometimes outside of their realm, doctors and other members of the health care team will take reasonable steps to address any spiritual or religious concerns in the context of providing better care.
You may want to consider nominating a spiritual or religious advisor in addition to your substitute decision-maker/s. This is not a formal requirement and they will not be responsible for making important health care decisions on your behalf, but they can be consulted about your spiritual and religious values.
27
‘ aPPOiNTiNg aN ENduriNg POWEr Of aTTOrNEy
Mrs White lives by herself and has no living relatives. Mrs White and her friend Anna have a close relationship, and often go shopping and travelling together. Mrs White has been thinking lately about what might happen if she fell seriously ill and was unable to make decisions about her health care.
‘
Mrs White decides to appoint Anna as her Enduring Power of Attorney (for health matters). She discusses with Anna her wishes for future health care if she lost capacity in the future and was unable to decide for herself. Anna understands Mrs White’s preferences and the reasons for them, and can act accordingly should Mrs White lose capacity.
28
Resuscitation
Planning
29
rESuSCiTaTiON PlaNNiNg
What is resuscitation planning?
Resuscitation planning refers to decisions made in advance about what to do in the event you stop breathing (respiratory arrest) or your heart stops (cardiac arrest). In almost all cases, it will involve decisions about cardiopulmonary resuscitation (CPR). But there are also other life-sustaining measures which may be considered when planning resuscitation (more explanation of this later).
Resuscitation planning is appropriate for people who are at reasonable risk of cardiac and/or respiratory arrest in the foreseeable future. Resuscitation planning also involves making decisions about life-sustaining measures.
What is a life-sustaining measure?
When the decision is made to provide life-sustaining measures, the risk to a person’s health and life is very serious. If the medical treatment will save a person’s life, it will most likely be a ‘lifesustaining measure’. There are important safeguards in Queensland laws that make it clear that decisions about life-sustaining measures (whether to provide them) on behalf of a person who has lost capacity must be made in a collaborative manner.
30
rESuSCiTaTiON PlaNNiNg
In almost all cases (except for acute emergency situations), consent is required to withdraw or withhold life-sustaining measures — that is, consent not to provide them.
Life-sustaining measures can include treatments such as CPR, ventilation and tube feeding (which means providing someone with food and/or water through a tube, usually because they are unable to swallow). If a person loses capacity (perhaps through going into a coma), food and/or water tubes cannot be removed without the consent of their substitute decision-maker/s.
In all cases, the consent of your substitute decision-maker/s will be required if a blood transfusion is proposed while you do not have capacity.
Why does my doctor want to discuss resuscitation planning with me?
Your doctor may want you to consider your treatment options because you may be at risk of suffering an acute event, such as a heart attack. It can be difficult to respond to questions about things like CPR and tube feeding, but it may be preferable to talk about it now, rather than your doctor and family making these decisions in a crisis without knowing what you would have wanted.
31
rESuSCiTaTiON PlaNNiNg
If you are admitted to a hospital and the doctor wishes to discuss resuscitation planning, such things as options for resuscitation given your condition, consenting details and your choices about resuscitation will be discussed with you and documented in your medical records.
What is Cardiopulmonary Resuscitation (CPR)?
CPR refers to the use of special drugs and/or machines or very firm pressing on the chest to try to revive someone. CPR may involve simple efforts such as mouth-to-mouth resuscitation and external chest compression. Advanced CPR may involve electric shocks to the heart, insertion of a tube to open the airway, injection of medication into the heart, and in some cases, open chest heart massage.
When patients are seriously or terminally ill, CPR may not work or only partially work, leaving the patient brain-damaged or in a worse medical state than before their heart stopped. In these cases, some patients prefer to be cared for without aggressive resuscitation attempts.
Besides CPR, other medical treatment may be considered in an emergency, depending on the circumstances.
32
rESuSCiTaTiON PlaNNiNg
What else might be involved in CPR?
On television, CPR is often depicted as the ultimate life-saving technique. It has even been reported that CPR has a 67% success rate on television.
In real life, however, CPR is neither as straightforward nor as successful. In fact, it can be quite brutal. It involves pushing the centre of the chest down at least three and a half centimetres, 100 times a minute for several minutes. This can cause severe pain and may break ribs or damage the liver. Other significant problems may occur, such as brain damage due to lack of oxygen. There are definitely times when the risk of problems is outweighed by the potential benefits. Talk to your doctor about this.
When a person is in failing health from a serious and progressive illness, the heart and breathing will ultimately fail as a result of that illness. If CPR is unsuccessful, it may still be appropriate to continue with other life-sustaining measures to ensure the person remains comfortable. At that time, it may be appropriate to be transferred to palliative care.
33
rESuSCiTaTiON PlaNNiNg
How successful is resuscitation through CPR?
When successful, CPR restores heartbeat and breathing and may allow someone to resume their previous lifestyle. The success of
CPR depends on a person’s overall medical condition. Age alone does not determine whether CPR will be successful, although agerelated illnesses and frailties can be a factor.
CPR is more successful in saving the lives of those who do not have serious underlying illnesses. It is most successful when a person suffers a cardiac arrest or respiratory arrest in hospital, such as in a cardiac or intensie care unit and are attended to immediately.
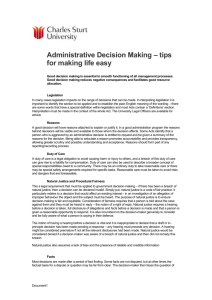
Various studies have found that initial in-hospital CPR success rates range from 16.8 to 44%. Long-term survival (discharge from hospital) rates range from 3.1 to 16.5%. An indication of overall
CPR success rates appears in the table below:
Diagnosis 1,2
Respiratory failure
Heart condition
Head injury
Acute renal failure
Survival after 24 hours
Survival to hospital discharge
Success Rate for CPR
18.9%
16.2%
7.2%
2.7%
9.2%
8.3%
34
rESuSCiTaTiON PlaNNiNg
Will CPR be right for me?
This decision may only be reached after you (or if you lack capacity, your substitute decision-maker/s) discuss it in some detail with your doctor. You may have very strong views about whether resuscitation is something you want, given the risks that will be explained to you by your doctor.
When a person suffers an arrest, it will always be considered an emergency situation. However, the decision of whether CPR should be provided does not need to be made in an emergency, particularly if it was an expected arrest. Where there is any clinical doubt and no one is aware of your wishes, the decision will always be in favour of providing CPR to save your life.
What happens if an ambulance is called?
As a general rule, the ambulance service does not have access to the records kept at the hospital or nursing home. If you are not in hospital and become ill or you have a cardiac or respiratory arrest, someone will probably call an ambulance if you have not expressed your wishes (for example, if you do not want to be resuscitated).
The Queensland Ambulance Service operating standards are that the attending paramedics will perform CPR and other resuscitation procedures in an emergency unless formal paperwork is in order
35
rESuSCiTaTiON PlaNNiNg refusing any specific resuscitation effort. Therefore, if you have strong wishes about not being resuscitated, you should formalise your decision and complete an Advance Health Directive to that effect. The attending paramedics will need to view the paperwork so it is important that it is readily accessible.
If you do not wish to have CPR performed on you, you need to make it very clear in your Advance Health Directive, including the circumstances in which this should apply. Even if your substitute decision-maker/s is with you when the ambulance is called and you suffer a cardiac or respiratory arrest, the attending paramedics will perform CPR on you if your legal documents are not in order or cannot be found. The reason for this is that not providing CPR must be under the instruction or direction of a medical doctor.
If you are being cared for in the family home, it is very important that you make others aware of your wishes about calling the ambulance service and formalise this in an Advance Health Directive. While noone likes to talk about an emergency situation that might happen when the ambulance is called, it is necessary to do so if you want your wishes respected.
1 Brooks, S.C et al. (2010). Out-of-hospital cardiac arrest frequency and survival: Evidence for temporal variability. Resuscitation, 81(2) 175-181.
2 Myrianthefs, P. et al. (2003). Efficacy of CPR in a general, adult ICU. Resuscitation, 57(1) 43-48.
36
My Rights and
Obligations as a Substitute
Decision-Maker
37
my righTS aNd ObligaTiONS aS a SubSTiTuTE dECiSiON-makEr
What is a substitute decision-maker?
‘Substitute decision-maker’ refers to a person permitted under the law to make important decisions on behalf of someone who does not have capacity (see page 24). A person can have more than one substitute decision-maker. The decisions made on your behalf by a substitute decision-maker/s can be about personal matters
(which includes health matters) or financial matters.
A substitute decision-maker can be appointed formally through:
• An order of the Queensland Civil and Administrative Tribunal
(as a guardian)
• An Enduring Power of Attorney (as a health attorney and/or financial attorney)
• An Advance Health Directive (as a health attorney).
A substitute decision-maker can also be informally delegated to this role, such as a statutory health attorney. If no-one is willing or available to be the statutory health attorney, the Adult Guardian becomes the person’s statutory health attorney.
38
my righTS aNd ObligaTiONS aS a SubSTiTuTE dECiSiON-makEr
What happens if I am asked to be someone’s decision-maker?
You can act as someone’s substitute decision-maker only if they lose capacity. Generally, you will know in advance if you will be a substitute decision-maker for a person who has lost capacity.
When the time comes for you to make important decisions about health care, the doctor-in-charge will ask you about the types of things that may be important to the person. They will give you options about available treatments and ask for your thoughts.
If I am a decision-maker, how long do I have to make a decision?
In an urgent emergency situation (for example, following a serious accident) you may need to make a decision very quickly.
The doctor-in-charge will guide you through this time.
However, in other cases, a person’s condition may have been deteriorating for some time and you may be well aware of the circumstances involved. This generally provides time to consider all the information and consult with others who may also be part of the person’s support network.
39
my righTS aNd ObligaTiONS aS a SubSTiTuTE dECiSiON-makEr
What are my legal obligations?
As a substitute decision-maker for someone who has lost capacity, you also have some important legal obligations. The law provides clear principles about how you should exercise your power.
Importantly, your decisions must be made in the person’s best interests and not restrict their rights in any way.
There must also be respect for their human worth and dignity and recognition of their role as a member of society. The Adult
Guardian can be consulted if there is any question that decisions are not being made in the person’s best interests. However, this can occur only if the person has lost capacity for decision-making.
As a substitute decision-maker, what types of things should I consider?
Until recently, many people did not discuss death and dying with their families, preferring to leave the difficult decision-making to the family doctor. Things have changed. The view now is that people have a right to know as much as possible so they can make the right decisions at the right time. You have a legal right to all the information that you need to make an informed decision.
40
my righTS aNd ObligaTiONS aS a SubSTiTuTE dECiSiON-makEr
Everyone is different and every family responds in a different way to bad news about someone they care about. Some people may want to know everything and may take comfort in being involved in the decision-making.
Others may find it distressing to be exposed to the knowledge that their loved one is dying, and that their options for further medical treatment are limited.
If you are the substitute decision-maker for someone who has lost capacity, you should:
• gain a general understanding of their medical condition and potential future complications
• gain a general understanding of future medical care options, particularly the benefits and risks of current and future treatments
• give careful consideration to their choices for end-of-life care if they have expressed them to you, as well as their goals, values and personal and spiritual beliefs
• discuss available choices with family/trusted others and document these choices
41
my righTS aNd ObligaTiONS aS a SubSTiTuTE dECiSiON-makEr
• while the person has capacity for decision-making, talk to them about formalising their decisions in an Advance Health
Directive or EPOA.
Some people may change their views and wishes during the course of their illness and, as the substitute decision-maker, you will have to take this into account.
42
N O T E S
43
‘ makiNg (Or NOT makiNg) dECiSiONS – iT’S yOur ChOiCE
Mr Gray identifies as someone of both Aboriginal and Torres Strait
Islander descent. He has suffered from renal failure for a number of years and was recently admitted to hospital for an indefinite period. A nurse at the hospital approached Mr Gray and suggested he consider discussing with his family what he would like to happen if he became too sick and unable to communicate his choices.
Mr Gray thinks that it’s pointless and too much bother to be worried about. Besides he doesn’t like talking about those kinds of things. He tells the nurse that when the time comes, his family will know what to do, so there is no point in bringing it up with them now.
Mr Gray is entitled to make his own decisions and if he does not wish to inform his family or make decisions about his future health care, he doesn’t have to. However, if Mr Gray loses capacity, a statutory health attorney will be found on his behalf (probably a close family member) who will make decisions for him. There may be many people who should be involved in this process. It is important that
Mr Gray is encouraged to tell his treating team who he wants to make health decisions on his behalf.
‘
44
My Rights and
Obligations as a Carer
45
my righTS aNd ObligaTiONS aS a CarEr
Who is a carer?
Technically speaking, a carer is an individual who provides ongoing care or assistance to someone who, because of disability, frailty, chronic illness or pain, requires assistance with everyday tasks.
Carers are often, but not always limited to, those closest to the person, such as parents, spouses, children, friends, neighbours or other family members. If you are a carer, you may be responsible for making decisions on behalf of another person. This may include important decisions about the person’s health care.
What if I’m a paid carer?
A paid carer is anyone who receives financial or ‘in kind’ contributions in return for supporting someone.
A carer who receives a carer’s pension or similar government benefit is NOT legally considered a paid carer.
A paid carer may be someone who:
• receives wages, assets or shares in assets in return for caring for someone,
• is being paid by an agency to care for someone.
46
my righTS aNd ObligaTiONS aS a CarEr
Because of the potential for conflict of interest, paid carers are not permitted to be a person’s substitute decision-maker.
Can I be a carer and a substitute decision-maker?
You cannot be a substitute decision-maker if you are a paid carer, but you can be a substitute decision-maker if you are a carer.
Similarly, the person doesn’t have to choose their carer as their substitute decision-maker. For example, they could appoint an attorney for health matters who may or may not live with or care for them. In this case, the health attorney (and not the carer) would be the substitute decision-maker if the person lost the capacity to make their own health decisions.
What happens if I am asked to make an important decision for the person in my care?
If you are the substitute decision-maker and the person no longer has capacity for making decisions about health matters, you will be responsible for making important health care decisions on their behalf. The doctor will also discuss available treatment options so
47
my righTS aNd ObligaTiONS aS a CarEr you can make an informed decision. When the time comes for you to decide, the doctor-in-charge may ask for your consent. You will also be asked about the types of things that may be important to the person, such as their values and beliefs. In most cases, consent can be verbal, and you will not have to sign anything.
End-of-life decision-making on behalf of someone who has lost capacity is a very stressful and emotionally charged time. Very often the decisions required will be difficult and you may not have had previous experience with these matters. The health care team, such as doctors, nurses, social workers, palliative care specialists and community nurses can provide understanding and support when necessary.
Keep in mind that decisions you make on behalf of the person you care for:
• must be made in their best interests
• should preserve the person’s dignity
• should not impose any unnecessary restrictions on them
• should take into account any views they have expressed to
you previously.
48
my righTS aNd ObligaTiONS aS a CarEr
Unless a decision is required immediately (such as in an emergency situation), you will be given time by the health care team to consider the information and make the decision on their behalf.
If there is more than one substitute decision-maker, they may be obliged to come to an agreement before a final decision is made.
It is your right as a carer and substitute decision-maker, and in your interests, to ask as many questions about the proposed medical treatment until you are satisfied your decision will be an informed one.
Taking care of yourself
Providing physical and emotional care can be daunting and demanding, especially if you take on the role as someone’s carer suddenly, or unexpectantly. Looking after someone who is very ill is not easy, and at different times you may need to learn new skills and find your way around a great deal of information.
You need to look after yourself to take on this sort of responsibility for someone else; attend to your own wellbeing. This will boost your quality of life and, in turn, help you to have the energy and capacity to deal with the challenges of providing effective support to the people around you.
49
my righTS aNd ObligaTiONS aS a CarEr
For more information and support, contact:
Carers Queensland
Website: www.carersqld.asn.au
Email: cas@carersqld.asn.au
Phone: (07) 3900 8100
Mail: PO Box 179, Holland Park QLD 4121
Carers Australia
Website: www.carersaustralia.com.au
Phone: 1800 242 636 (Carer Advisory and Counselling Service)
Disability and Community Care Services
Website: www.disability.qld.gov.au/support-services/carers
Email: disabilityinfo@disability.qld.gov.au
Phone: 1800 177 120
Young Carers Australia
Website: www.youngcarers.net.au
Phone: 1800 242 636
50
N O T E S
51
‘ CrEaTiNg aN advaNCE hEalTh dirECTivE
Mrs Pink has had no previous history of serious illness or hospital admission. However, as she gets older, she has begun thinking about what may happen if she gets sick. She decides to create an Advance Health Directive so that her family, doctors and other medical professionals who care for her will know what health care she would like to receive in the event she is unable to communicate.
‘
Mrs Pink consults her doctor about what illnesses a person in her situation may get in the future, and what options she has. Mrs
Pink likes the idea of the detail in an Advance Health Directive and outlines whether she wishes to receive treatment for each of the conditions. She states that in the event of a cardiac or respiratory arrest, she does not want CPR.
52
Special Considerations
53
SPECial CONSidEraTiONS
Children
Children (under 18), are not covered by the guidance in this booklet, or by the guardianship legislation. The decision-making processes involved when a child is dying are very difficult and different laws may apply. Guidelines on advance care planning in these situations will be available in 2011.
Decision-making disabilities
Under the law, everyone is presumed to have capacity unless it is established (by a doctor) they do not. Therefore people with disabilities should not be presumed to lack capacity for making health care decisions. All individuals have legal rights when it comes to making end-of-life decisions. Discussing these issues with family members, significant others and health care professionals is an important part of caring for some of the most vulnerable patients.
Advance care planning for people with disabilities is not a onesize-fits-all approach. Some people may be unable to participate in the planning, but others may choose to take an active or partial role.
54
SPECial CONSidEraTiONS
In many cases, this is something only the families and/or substitute decision-maker/s can decide, as the values and thoughts of the disabled person are best known to them. If an EPOA or Advance
Health Directive is made, a person needs to have capacity at the time in order for their choices for end-of-life care to be formalised
(see page 15-17 for Advance Health Directives and EPOAs ).
When a person with a decision-making disability reaches the end of life, all decision-making must incorporate an underlying respect for their autonomy and ensure no harm is done. People with disabilities may also have specific requirements that should be taken into consideration.
Queensland’s legal framework ensures there is always someone to represent the interests of an adult who lacks capacity, or who has never had capacity. If there is no-one else available, the Adult
Guardian acts as the substitute decision-maker for the disabled person.
When the time comes for end-of-life decisions, particularly about withholding or withdrawing life-sustaining measures, consent will be required from the disabled person’s substitute decisionmaker/s, who could be a statutory health attorney or formally appointed guardian.
55
SPECial CONSidEraTiONS
Many substitute decision-makers for adult people with disabilities are not formally appointed. Most often parents automatically become the disabled person’s statutory health attorney/s. An
Attorney or Guardian would be formally appointed only if there were any dispute, or legal authority needed for financial reasons.
In almost all cases, except for acute emergencies, consent is needed to provide or withhold/withdraw medical treatment. The substitute decision-maker/s of a disabled person in this situation would rarely be asked for proof that they are the statutory health attorney/s.
Although their engagement with making decisions may be constrained by their capacity, even people with limited capacity should be encouraged to participate in advance care planning to the extent their abilities allow. For example, those unable to make decisions about life-sustaining medical treatment may have the capacity to make decisions about low-risk medications, diet or recreation.
56
SPECial CONSidEraTiONS
End-of-life discussions with a person who has a disability can be made easier with the support of toolkits that describe to them, sometimes with pictures, what is happening to them. You may be able to access this information by contacting your community social worker or the Queensland Government’s Disability
Information Service on 1800 177 120.
Disability and Community Care Services
Website: www.disability.qld.gov.au/support-services/carers
Email: disabilityinfo@disability.qld.gov.au
Phone: 1800 177 120
Queenslanders With Disability Network Inc.
Website: www.qdn.org.au
Email: qdn@qdn.org.au
Phone: 1300 363 783
Mail: Reply Paid Suite 11, 7 O’Connell Tce, Bowen Hills QLD 4006
Queensland Aged and Disability Advocacy (QADA) Inc.
Website: www.qada.org.au
Email: info@qada.org.au
Phone: 1800 818 338
57
SPECial CONSidEraTiONS
Aboriginal and Torres Strait Islander communities
Every person’s right to make decisions about their future health care is an accepted and important part of providing health care.
This is not just a legal right.
Having a say in end-of-life decisions can help you and people in your family come to terms with death, as well as ensure the right thing happens at the right time. Someone who identifies with an Aboriginal and/or Torres Strait Islander background or community will probably have strong connections to people who can talk to them and help them through sad and difficult times.
If you are an Aboriginal or Torres Strait Islander and have a strong connection to your community, it is particularly important that you talk about your treatment choices because you may have to spend some time away from home. There may also be times when family and/or friends may need to accompany you to a hospital a long way from where you live.
There are many things to think about and arrangements to make.
To make sure that your doctors, nurses and other people looking after you know how best to provide your care, you should talk
58
SPECial CONSidEraTiONS about them now. If you put off these decisions, they’ll be much harder later. Talk to your doctor, community nurse, liaison officer or social worker. They can help.
Many Aboriginal and Torres Strait Islander people would prefer to die in their own communities. To some, this is more important to them than the treatment of their disease. If this is the case for you, it’s even more important that you receive all the necessary information about your future treatment so you can make proper choices. It’s not just for you. The more you know now, the more you can tell your family and/or friends what is happening. That way, you can make sure your wishes for end-of-life care are known and can be respected by everyone.
You can also ask someone at your hospital to contact the Liaison
Officers, to help strengthen communication between you, your family, community members and health care team.
59
SPECial CONSidEraTiONS
For more information and support, contact:
Aboriginal and Torres Strait Islander Health Strategy Unit
Website: www.health.gov.au/atsihealth/default.asp
Email: ATSIHSU@health.qld.gov.au
Phone: (07) 3234 0760
Aboriginal and Torres Strait Islander Partnerships
Website: www.atsip.qld.gov.au
Email: askatsip@communities.qld.gov.au
Phone: 131 304
Queensland Aboriginal and Islander Health Council (QAIHC)
Website: www.qaihc.com.au
Australian Indigenous Health InfoNet
Website: www.healthinfonet.ecu.edu.au
Email: healthinfonet@ecu.edu.au
Phone: (08) 9370 6336
Australian Indigenous Health Bulletin
Website: www.healthbulletin.org.au
Email: healthbulletin@ecu.edu.au
Phone: (08) 9370 6109
60
SPECial CONSidEraTiONS
Culturally and linguistically diverse backgrounds
If you are a person who identifies with another culture, your views about death and dying and end-of-life care may differ to those of other Australians. Every Australian, regardless of where they were born or what culture they are part of, has the right to make decisions about their future medical care and to have those choices respected. This is a fundamental principle of Australia’s health care system and is recognised by Australian laws.
Having a say in what you would want when you are no longer able to make decisions for yourself can give you peace of mind that the right thing will happen at the right time. To make it easier, you don’t have to do it on your own. You may, for example, like to take a friend and/or family member each time you visit the doctor.
The doctor and other members of the health care team will ask you for your views on several aspects of your future medical care. If you have been diagnosed with a serious illness and do not have long to live, there may be deeply personal or spiritual matters you would like to put in place while you are able to do so. The health care team will be very responsive to your needs to provide better health care to you and support to your family.
61
SPECial CONSidEraTiONS
If you are a friend of someone from another culture who believes they require special considerations for medical treatment at the end of life, it may be appropriate to be with them during visits to the doctor or other health professionals. This can be for translation purposes, or to put across any request for rituals that might be important to the person, such as treatment of a body and funeral arrangements.
The health care team will arrange an interpreter service if this is required. If you are concerned about the confidentiality of the information, a telephone interpreter service can also be sourced from another State.
An Advance Care Planning brochure is also available in several languages.
A comprehensive listing of more than 1500 key organisations with an ethnic community focus in Queensland is available in the Queensland Multicultural Resource Directory, which can be accessed at: www.multicultural.qld.gov.au/services-resources/resourcedirectory/index.aspx
62
SPECial CONSidEraTiONS
Mental health
Mental health issues do not always prevent someone from participating in advance care planning. For example, while a person with an episodic mental health condition has capacity, they may complete an Advance Health Directive to ensure their wishes for health care are carried out in episodes of temporary loss of capacity.
It is recognised that people do not necessarily lack capacity because they live with mental illness. The capacity to make health care decisions is assumed for all adults under law, and disputes about capacity would need to be resolved through clinical assessment.
Voluntary patients
Adults with capacity to make health care decisions may choose to leave the mental health ward or facility to which they have been admitted, even if their doctor advises them against it. This is generally known as ‘discharge at own risk’, or leaving against medical advice.
Involuntary patients
If patients are held involuntarily for an assessment, it is likely to be for a period of 24 hours (one day). However, if necessary, the
63
SPECial CONSidEraTiONS doctor can extend this to 72 hours (three days). The patient will not be able to discharge against medical advice at this time because it is believed that someone else needs to make health care decisions for them temporarily.
Patients who receive involuntary treatment must be regularly reviewed by an authorised psychiatrist. Where a person under a
Mental Health Order makes or wishes to make an Advance Health
Directive, or expresses their wishes about end-of-life care, their capacity will need to be assessed by a psychiatrist at the time the decisions are made.
What are my rights as an involuntary patient?
Advance care planning is the right of every adult. As an involuntary patient, you have the right to:
• be informed about why the doctor has decided to make an involuntary assessment, the treatment order and details of proposed treatment
• choose a person to help represent your views, wishes and interests for end-of-life care
• have access to health practitioners and legal advisors to make an informed decision
64
SPECial CONSidEraTiONS
• raise concerns with a community visitor. The Office of the
Adult Guardian administers this program for adults
• have regular reviews of your involuntary treatment by an authorised psychiatrist
• be told when you become, and stop being, an involuntary patient.
For more information contact the services and support networks listed below:
Mental Health Branch (Queensland Health)
Website: www.health.qld.gov.au/mentalhealth
Queensland Alliance of Mental Illness and Psychiatric
Disability Groups Inc.
Website: www.qldalliance.org.au
Email: admin@qldalliance.org.au
Phone: (07) 3832 2600
Mail: PO Box 919, Spring Hill QLD 4000
The Queensland Public Interest Law Clearing House Inc.
(QPILCH) has put together a comprehensive fact-sheet regarding the processes involved in being made an involuntary patient under the Mental Health Act (2000). It can be accessed at: www.pilch.org.au/resources/factsheers/Involuntary_Assessment.htm
65
N O T E S
66
Other Considerations of Advance Care
Planning
67
OThEr CONSidEraTiONS Of advaNCE CarE PlaNNiNg
Talking about death and dying
In many cultures, it’s considered impolite to talk about death and dying. It can be an uncomfortable subject at the best of times, and it seems almost unbearable to think about our own death or the death of someone we are close to. It is important to consider cultural differences and having discussions in a culturally acceptable setting.
In a world of advancing science and life-saving medical breakthroughs people can live for many years after a serious illness is diagnosed, and it is easy to delay important decisions about how we want to die, often until it is too late.
Many of us wish we had said more to someone before they died
– let them know they were important or reassured them. Sadly, issues are often avoided when someone is dying because it feels too overwhelming to even begin the conversation.
In fact, it has been reported that the person who is dying is often more comfortable with these discussions than those around them.
If your condition is terminal, you may like to take responsibility for what needs to be said. This may give you a sense of satisfaction that you have some influence over the last stages of your life.
Whether you want people to openly discuss death and dying, or focus solely on the positive, are choices only you can make.
68
OThEr CONSidEraTiONS Of advaNCE CarE PlaNNiNg
Talking about death and dying with children
Many of us hesitate to talk about death, particularly with children.
It may seem easier not to burden them. Unfortunately, children and teenagers can become more anxious if they feel secrets are being kept from them about someone they are close to.
The challenge for adults is to provide children and teenagers with information that is honest, timely and appropriate to their developmental age and situation. For example, if children are very young, they may view death as temporary, and may be more concerned about separation from loved ones than about death itself. A very young child can absorb only limited amounts of information. Answers need to be brief, simple and repeated when necessary.
Make time to talk with them. Listen to what they are asking and what they are saying. It is important to remember that every child is an individual. Communicating about death depends on their age and experiences. By talking to our children about these issues, we may discover if they have misconceptions, fears or worries. We can then help them to deal with these and to face the realities of death.
69
OThEr CONSidEraTiONS Of advaNCE CarE PlaNNiNg
When the time comes…
When you have a terminal illness or are dying, there are many things which are beyond your control, but there are also things you can control.
You can find out what to expect, and if you wish, you can plan the events that precede and follow your death. Preparing in this way can give a sense of completion and achievement because these plans will reflect your choices and wishes, which may not otherwise be known or respected if someone else has to do it all for you. The peace of mind that it may provide you and those you care about may be well worth the initial discomfort of raising the issue and involving them in your choices.
Family members can prepare for the death of a loved one by knowing the physical changes to expect. This preparation can help prevent unnecessary emergency room visits around the time of death and may allow a loved one to die peacefully at home or within a palliative care setting.
You may have an Advance Health Directive or EPOA listing the medical treatment and care you might want (or not want) in the event you lose capacity, but other things will also be important to you at the end of life.
70
OThEr CONSidEraTiONS Of advaNCE CarE PlaNNiNg
Think about making a wishlist or writing your choices in a diary about things important to you. This list can be given to your family, friends and doctors and help them to prepare for the future.
It may even make it easier for your wishes to be followed.
You can write a list or make a diary at any time in your life and update it whenever you want. You can choose to show it to people while you are well, or have it available on your death. Once written, it can provide vital information if you become unable to explain your wishes yourself, or it can simply provide reassurance to you because you’ve already made some difficult decisions.
Some of the issues you might like to cover in your list or diary are:
• where you would like to be cared for if you are dying (for example, hospital, hospice, at home)
• if you want to know about the effects of any treatment (or non-treatment) you may be offered
• if you want to be told when you are close to death (assuming your doctors are able to predict this) and if you would want other people to know
• who should talk to any children or other close family such as elderly parents about your impending death, if you are unable to do so
71
OThEr CONSidEraTiONS Of advaNCE CarE PlaNNiNg
• who should look after your pets
• how you want your final days to look and sound – what you would like in your room (flowers, pictures, music, TV and so on)
• whether you would like a spiritual advisor, such as a priest, to be made available
• whether you want any rituals associated with your culture or family tradition to be honoured
• who you wish to visit you near the end
• your funeral arrangements.
While this sort of preparation can help to give you peace of mind, it may also help those close to you to better understand your situation and deal with the difficult decisions when the time comes.
Organ and tissue donation
Organ and tissue donation is much more than simply a surgical procedure. It is a profoundly generous act that can transform the lives of people suffering debilitating or terminal illnesses. After you die, organs and tissues can be removed from your body (the donor) and transplanted into another living person (the recipient) to give them life or to improve their quality of life.
72
OThEr CONSidEraTiONS Of advaNCE CarE PlaNNiNg
Which organs and tissues you are able to donate depends on many factors such as why you died, your past medical history and where and when you die. Only about 1% of people who die can donate organs, such as heart, lungs, liver, kidneys, pancreas and bowels, because organ donation is possible only when a person dies in an intensive care unit on a ventilator.
Many more people are able to donate tissue, such as heart valves, eye tissue, skin and bone. Regardless of your age, disease, medications, if you’ve smoked or wear glasses or if you die in hospital, a hospice or at home, you may be able to donate tissue. Your individual circumstances would be assessed after your death to determine if you can be a donor and what you can donate. It’s important to remember that not everyone who wants to donate can.
You can ensure your wishes are respected by making sure your family, friends or substitute decision-maker/s are aware of your decision on organ and tissue donation. If you have a valid Advance
Health Directive, you may like to include wishes about organ and tissue donation. After your death, they will be asked to confirm your most recent wish.
If you would like to know more about organ and tissue donation, you can call Donate Life on (07) 3240 2350 or view their website at www. donatelife.gov.au.
73
N O T E S
74
Frequently
Asked Questions
75
frEquENTly aSkEd quESTiONS
Is it helpful to complete advance care planning documentation?
Yes, because:
• it helps you to think, and talk to your family and/or friends and doctor, about your future medical care if you become seriously ill
• if you become seriously ill, your family or someone appointed by you has something in writing for doctors to consider.
Who do I talk to about this?
• your family and those most likely to be involved in making decisions if you are seriously ill
• your doctor who will help you understand your health condition and treatment options
• your community liaison nurse who can help you to start your advance care planning
• your social worker who can also help to guide you to start your advance care planning
• your religious or spiritual advisor, if this applies.
A close or loving relationship does not always mean that the other person knows or understands your wishes for future health care.
76
frEquENTly aSkEd quESTiONS
Who should I choose to be my substitute decision-maker?
Someone you trust who is over the age of 18 years, not your paid carer and who:
• knows you well
• will listen carefully to your wishes for future health care
• will be able to make decisions that may need to be made under difficult circumstances.
Family members are the most common substitute decisionmakers, but it can be anyone you trust who is readily available and willing to take on the responsibility.
Formally appointing a substitute decision-maker (health attorney) for health matters allows you to choose who will make decisions for you if ever you are unable to make your own decisions.
Remember, you can appoint more than one attorney for personal/ health matters.
When are advance care planning documents used?
They can be used only if you are unable to make or communicate your own decisions (that is, when you lose capacity). Your advance care planning documents will guide the decision-making of your doctor, your substitute decision-maker/s and, where appropriate, other family members and/or friends.
77
frEquENTly aSkEd quESTiONS
What if I become ill or I am injured while I am away from home?
The best way to ensure you receive the type of care you want is to discuss your choices with your substitute decision-maker/s and make sure they have a copy of your advance care planning documents. A card in your purse or wallet with your important contacts will help if anything happens when you are away from home. You may also consider keeping your documents with you when travelling, particularly if you are in failing health. Most states in Australia will recognise a valid Advance Health Directive completed in Queensland.
What happens in an emergency?
In an emergency, your medical records may not be available at short notice and life-sustaining measures may be started. Following discussions with your substitute decision-maker/s, treatment can be stopped if it is clear that the treatment is not what you would have wanted and is providing no benefit to you.
In some urgent situations, it may not be possible to locate a substitute decision-maker. If a decision is needed in an acute emergency, clinical judgement will guide whether life-sustaining measures are commenced.
78
frEquENTly aSkEd quESTiONS
What happens if there is disagreement after I lose capacity?
If you lose capacity, the person (or persons) you have appointed as your substitute decision-maker/s will have the responsibility of acting in your best interests. If you have an Advance Health
Directive, your choices and wishes for care will be followed in accordance with good medical practice. However, even with all these arrangements in place, this is a very difficult time for families and sometimes disagreement occurs.
Most often this happens when there are differing expectations about your care and your prognosis for recovery. Disagreement can also occur where there is more than one person who is legally able to make decisions for you. In these cases, the doctors and the rest of the health care team will provide support and information so the person/s making decisions on your behalf will be supported to act in your best interests. The health care team will also allow time for families to come to terms with matters causing conflict.
If your substitute decision-maker/s is not satisfied with your care or progress, they can seek a second opinion. However, if you lack the capacity to decide, and your decision-maker/s cannot resolve matters, they or your health care team can contact the Office of the Adult Guardian to help resolve any disagreement.
79
dO yOu NEEd furThEr iNfOrmaTiON?
If you would like to find out more about advance care planning, you can speak to your doctor, community liaison nurse or to a social worker.
You can also contact the Public Trustee, the Adult Guardian or a solicitor. In addition, you can find out more by accessing the
Department of Justice and Attorney-General website at justice.qld.
gov.au.
80
imPOrTaNT CONTaCTS:
Carer/s:
Doctor:
Community Liaison Nurse:
Social Worker:
Palliative Care Services:
Palliative Care Information Service: Phone 1800 772 273
Office of the Adult Guardian: Phone 1300 653 187
Email: adult.guardian@justice.qld.gov.au
Bereavement Support:
Queensland Health website at health.qld.gov.au/advance-care-planning or email QHclinicalethics@health.qld.gov.au
81
glOSSary
Adult Guardianship Legislation
Queensland’s guardianship legislation refers to two pieces of legislation: the Powers of Attorney Act (1998) and the
Guardianship and Administration Act (2000) . These statutes legislation regulates the making of decisions by, and on behalf of, adults with impaired capacity. It deals with issues such as:
• When is an adult unable to make their own decisions?
• If an adult can’t make their own decisions, who should make them on his or her behalf?
• How should those decisions for an adult be made?
Best interests
This refers to a legal test of ‘best interests’ which is protected in legislation in some Australian states (currently excluding
Queensland), and requires that decisions made by a substitute decision-maker are to be made for the adult’s welfare or benefit.
When considering a person’s best interests, a wide range of factors must be taken into consideration, such as their culture, values and personal wishes.
Cardiac arrest
‘Cardiac arrest’ means that a person’s heart suddenly stops pumping, and their blood stops circulating through their body and brain. If untreated (such as by attempting resuscitation), sudden cardiac arrest can lead to a person’s death within minutes.
82
glOSSary
‘Common law’ health directive
In legal terms, discussing your future health care choices with family and significant others is called a ‘common law’ health directive. This means you have chosen not to formalise your choices for end-of-life care by signing legal documents and having them witnessed. However, having these discussions with those close to you ensures that your views and wishes are known, and can be considered at a time when you lose capacity and health care decisions need to be made on your behalf.
‘Impaired capacity’
‘Impaired capacity’ refers to a person’s inability to make a sound decision in a particular area of their life. Impaired decisionmaking capacity may be due to an intellectual disability, acquired brain injury, mental illness, dementia or some other cause. Lack of capacity will not be established using someone’s age, cultural background, behaviour, appearance or physical condition, as this may lead to bias and unjustified assumptions. In cases where capacity needs to be verified, a doctor may conduct a number of simple tests. In some complicated cases, capacity assessment may also involve a psychiatric evaluation.
83
Palliative care
Palliative care improves the quality of life of patients and their families who face life-threatening illness, by providing pain and symptom relief, spiritual and psychosocial support from diagnosis to the end of life and bereavement. Palliative care:
• provides relief from pain and other distressing symptoms
• affirms life and regards dying as a normal process
• intends neither to hasten nor to postpone death.
Respiratory arrest
Respiratory arrest differs from cardiac arrest, and means that a person has stopped breathing. When a person is in respiratory arrest, the heart may still be beating. Without resuscitation, their heart will stop beating soon after breathing stops. In some instances the person’s heart may stop beating first, and then their breathing will stop immediately.
84
Statutory health attorney
A statutory health attorney is the most ‘readily available and culturally appropriate’ person in someone’s support network.
The statutory health attorney must be an adult, and is chosen in the following order – spouse or partner, primary carer (but not a paid carer), and a close friend or relative. If there is no one available or willing to be the statutory health attorney, the
Adult Guardian takes on the role. A statutory health attorney is informally appointed if a person does not have a valid Advance
Health Directive.
Special health matters
When a person loses capacity, their substitute decision-maker will make decisions on health matters on their behalf. Health matters mean general health care and treatment by a health provider.
However, Queensland’s legislative framework recognises that there are some matters which are too personal for someone to make decisions about for another person. When related to health care, these are called ‘special health matters’. Special health matters include things like tissue donation, sterilisation and termination of pregnancy. This means, for example, that a substitute decisionmaker could not give consent to the termination of pregnancy for someone they would be able to make other health care decisions for.
85
N O T E S
86
N O T E S
87
Queensland Health
April 2010