Pergamon
e l h S0968-4328(98)00006-7
Micron Wol. 29, No. 2/3, pp. 105-111, 1998
© 1998 Elsevier Science Ltd. All rights reserved
Printed in Great Britain
0968--4328/98 $19.00+0.00
Experimental Model to Study Sedimentary Kidney Stones
F. GRASES and A. LLOBERA
Laboratory of Urolithiasis Research, Department of Chemistry, University of Balearic Islands, 07(971 Palma de
Mallorca, Spain
(Received 18 July 1997; accepted 23 January 1998)
Abstract--An experimental model to reproduce, to some extent, the conditions prevailing during the formation of the so-called
sedimentary urinary stones, was developed. The results obtained demonstrated that in the absence of organic matter no calcium
phosphate crystals were deposited in cavities with scarce liquid renovation. Nevertheless, in such case a regular hydroxyapatite layer was
developed on the walls around the cavity. The presence of crystallization inhibitors cannot stop indefinitely the cr'(stal development. Therefore,
phytate manifested important inhibitory effects in concentrations normally found in urine (0.77-1.54 × 10 -" mol/l), whereas citrate only
manifested important inhibitory effects when found at high urinary concentrations (2.64 x 10 -3 mol/l). When mucin (a glycoprotein) was
present in the urine, a clear deposit of calcified organic material was formed. The organic matter appeared mixed with the sphemlites of
hydroxyapatite, this demonstrating the capacity of the glycoprotein agglomerates to act as heterogeneous nucleants of calcium salts and their
important role in the formation of sedimentary stones. The structural features of the obtained in vitro deposits were compared with the fine
structure of human sedimentary phosphate calculi. Scanning electron microscopy images demonstrated a good correspondence between in vitro
experiments and in vivo observations. © 1998 Elsevier Science Ltd. All rights reserved.
Key words: calculogenesis, sedimentary urinary calculi, citrate, phytate.
INTRODUCTION
Urolithiasis, i.e. generation of solid objects (termed calculi or stones) within the urinary tract, constitutes a serious
health problem that affects a significant section of mankind.
Between 3 and 14% of the population, depending on the
geographical region, suffer from this illness. Renal calculi
can be composed of various inorganic and/or organic compounds. As the main common components, calcium oxalate
(70% of the cases), calcium and magnesium phosphates
(15%), uric acid (15%) and cystine (1%) can be found. All
these components can be organized in a variety of different
crystalline phases, morphologies and microstructures, thus
more than 20 different types of calculi have been classified
(Grases et al., in press). The absence of a realistic concept of
the renal stone generation in an important number of cases is,
to a considerable extent, caused by the fact that this process
cannot be observed directly in vivo and all hypotheses have to
be based on results of in vitro experiments. The relevance of
in vitro experiments to urolithiasis depends on the degree of
correspondence between the experimental conditions and
those prevailing in the stone - forming kidney. In vitro
methods should reproduce some of the stages of a real biological process. In fact each experimental method employed
to the date usually enables the study of only one particular
stage of stone formation. For example, crystallizers (continuous, batch and semi-batch) allow solely the study of the
crystal growth stage. The majority of physicochemical studies on urolithiasis, to date, have dealt with this stage, and
undoubtedly although their results are of importance they still
do not explain the formation of the complex structure of the
majority of renal calculi.
The study of the fine structure of renal stones demonstrated that they can be broadly classified into two main
groups: stones mainly formed through crystal growth
mechanisms and stones formed in cavities of low urodinamic efficacy in which sedimentation processes also play
an important role (Cifuentes, 1984; Daudon et al., 1993;
Hesse et al., 1979; Iwata et al., 1986; Khan and Hackett,
1986; Leusmann, 1991; Meyer et al., 1971; Prien and Frondel, 1947). A typical example of renal stones whose structure is mainly determined by crystalline growth processes,
correspond to calcium oxalate monohydrate (COM) papillar
calculi. In such stones the initial development of a nidus of
attached particles to the papillae wall is necessary, likewise
constituting the core and thus the regular columnar growth
of COM crystals, hence, originating the main body of the
calculus (Grases et al., 1993). A number of in vitro studies
on the formation of such calculi performed in experimental
conditions closely simulating the real conditions of oxalocalcic papillary stone formation (Grases et al., 1994, 1996a,
b) together with the study of their structure, advanced understanding of their formation mechanism. The comprehension
of the formation mechanism of the so-called 'sedimentary'
stones is however lesser. Thus, it is deduced that no regular
and ordered crystalline structures are present. Moreover,
depending on the type of calculi, crystalline growth processes must also be considered. In fact, the presence of
high content of organic matter is normally observed in all
cases (SShnel et al., 1995). However, no in vitro studies
emulating the formation of these type of calculi have yet
been performed and are undoubtedly necessary in order to
relate the commented structural features and to complete the
knowledge of their formation mechanism. In the present
paper, a first attempt to partly reproduce the sedimentary
renal calculi formation in vitro with the aim to obtain new
data about its aetiology, is presented. The results obtained
were compared with those resulting from the observation by
105
F. Grases and A. Llobera
106
scanning electron microscopy of renal 'sedimentary' phosphate human stones.
MATERIALS AND METHODS
Synthetic urine
The synthetic urine was prepared immediately before use
by mixing with a T-type mixing chamber equal volumes of
solutions A and B. Both solutions were prepared by dissolving chemicals of reagent-grade purity in deionized and
redistilled water. One millilitre HzO2 30% was added to
both solutions. Once prepared, solutions were filtered
through a membrane filter with pore size of 0.45/~m. Solutions were stored for a maximum of one week at 4°C. Five
different compositions of synthetic urine were prepared.
Their compositions and pH values are given in Table 1.
Where necessary, admixtures were dissolved in solution B.
Simulation of the sedimentary stone formation
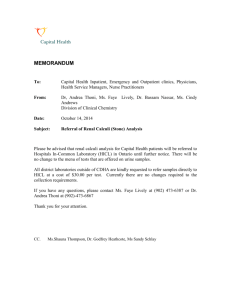
The experimental device, schematically shown in Fig. 1,
was placed in a temperature-controlled (37°C) chamber. A
flow rate of 0.28 ml/min for solutions A and B was maintained by a multichannel peristaltic pump. A replaceable
tube of 9 mm inner diameter retained the mixed solution
(i.e. artificial urine), serving as a reservoir for the solid
sedimentation and/or growth from the urine. In the present
series of experiments, the system was kept working for 24 h.
When the experiment was finished the tube was removed
from the system, carefully rinsed with distilled water and
dried at room temperature in a desiccator. One set of tubes
was used to study the type and size of crystals found on the
walls and bottom of the tube, by use of Hitachi S-530 scanning electron microscope. The other set of tubes were used
to quantify the amount of solid material deposited, by chemical analysis of the total calcium and phosphorous content.
This was accomplished by adding 2 ml of 2M hydrogen
chloride (HC1) and subsequent dilution to 25 ml with distilled water. Calcium and phosphorous determinations were
performed by inductively-coupled plasma emission spectrometry (Perkin-Elmer 2000).
The effects of sodium citrate (supplied by Probus) in the
concentration range 1.06-2.64 × 10 -3 mol/1, sodium phytate (supplied by Sigma) in the concentration range 0.771.54 × 10 -6 mold and mucin (a glycoprotein supplied by
Sigma) at 150 mg/1 were assayed by addition of different
amounts of these substances to artificial urine.
Due to the high concentration of citrate used and considering its complexing capacity of calcium ions, in experiments in which the action of citrate ions was evaluated, a
supplement of calcium was added to obtain the same calcium oxalate supersaturation value that is found in the
absence of citrate. It must be considered that a decrease in
the supersaturation would imply a decrease in the nucleation
and growth rates that could not be assigned to inhibitory
effects. Thus, in the presence of citrate (2.64 × 10 3 mol/l)
Table 1. Composition of synthetic urines*
Solution A (mol/1)
SOlution B (mol/l)
Synthetic urine I
Na2SO4.10H20
MgSO4.7H20
NH4CI
KC1
C a 2+
3.42
0.59
8.69
16.25
0.60
×
×
×
×
×
10 .2
10 -2
10 .2
10 -2
10 2
NaH2PO4-2H20
NazHPO4.12H20
NaCI
Na2C204
0.34 × 10-2
1.05 × 10 .2
22.45 × 10 -2
0 . 0 5 6 × 10 -2
3.42
0.59
8.69
16.25
0.60
×
X
×
×
×
10 .2
10 .2
10 -2
10 -2
10 .2
NaH2PO4.2H20
NazHPO4.12H20
NaC1
Na2C204
0.68 x 10 -2
2.10 x 10 -2
22.45 × 10 -2
0 . 0 5 6 × 10 -2
3.42
0.59
8.69
16.25
0.60
×
×
×
×
×
10 -2
10 -2
10 -2
10 -2
10 -2
NaH2PO4.2H20
NazHPO4.12H2 O
NaCI
Na2C204
1 . 0 0 × 10 -2
3.09 × 10 2
22.45 × 10 -2
0 . 0 5 6 × 10 -z
3.42
0.59
8.69
16.25
0.60
×
×
×
×
×
10 -2
10 -2
10 -2
10 .2
10 "2
NaH2PO4.2H20
Na2HPO4.12H20
NaCI
Na2C204
1.36 × 10 -2
4.20 × 10 .2
22.45 × 10 -2
0 . 0 5 6 × 10 °2
3.42
0.59
8.69
16.25
0.60
×
×
×
×
×
10 -z
10 -2
10 .2
10 -2
10 .2
NaH2PO4.2H20
Na2HPO4.12H20
NaCI
Na2C204
1.70 x 10 -2
5.25 × 10 .2
22.45 × 10 -2
0 . 0 5 6 × 10 -2
Synthetic urine II
Na2SO4-10H20
MgSO4.7H20
NH4CI
KC1
C a 2+
Synthetic urine III
NazSO4.10H20
MgSO4.7H20
NHnCI
KCI
C a 2+
Synthetic urine IV
NazSO4-10H20
MgSO4.7H20
NH4CI
KC1
C a 2+
Synthetic urine V
Na2SO4.10H20
MgSO4.7H20
NH4CI
KC1
C a 2+
*The p H values of all the synthetic urines used was adjusted to 6.9.
Sedimentary Kidney Stones
I I
III
I
II
Fig. 1. Schematic diagram of the model used to simulate the sedimentary stone formation. (I) Solution A for artificial urine preparation, (II) solution
B for artificial urine preparation, (III) thermostatted bath, (IV) multichannel peristaltic pump, (V) T-type mixing chamber of A and B solutions, (VI)
cylindrical flask, (VII) replaceable tube, (VIII) controlled temperature chamber, (IX) urine collector.
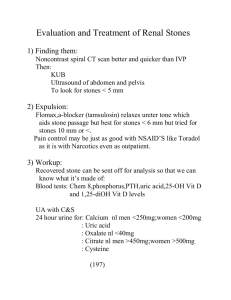
Fig. 2. (a) Hydroxyapatite crystals observed in the absence of organic matter on the surface of the cavity walls, using synthetic urine III, and (b)
using synthetic urine IV (see Table 1); (c) and (d) hydroxyapatite spherulites observed in a human sedimentary non-infective phosphate renal
calculus.
107
108
F. Grasesand A. Llobera
the total calcium concentration in the artificial urine was
3.54 x 10 -3 mol/l.
When using phytate, due to the low used levels, the
decrease in the free calcium concentration was practically
negligible, as was potentiometrically observed and, consequently, in this case it was not necessary to add a calcium
supplement.
Comparison with sedimentary renal phosphate human
stones
Renal stones classified as 'sedimentary' non-infective
phosphate calculi (main constituents hydroxyapatite and
organic matter) were selected from our stone collection containing over 1000 specimens. Stones, often in several
pieces, were fractured by scalpel along different planes.
One or several fragments of these stones were mounted on
a stub, sputtered with gold and observed by scanning electron mycroscopy.
RESULTS
In the absence of organic matter, the formation of a
hydroxyapatite regular crystalline layer on the cavity
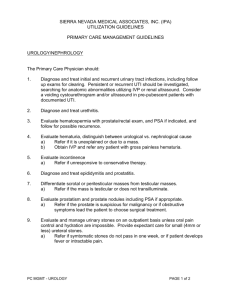
walls was observed (see Fig. 2(a, b)). The presence of larger
brushite crystals (regularly distributed) were detected on
this layer (see Fig. 3(a, b)). The uniform distribution of
crystals on the surface cavity demonstrated that all were
formed by nucleation and growth on the surface and not
by sedimentation in the cavity, since in this case they
would appear mainly as a deposit and no regular distribution
would be observed.
Obviously, the amount of crystalline mass formed
depended on the phosphate concentration (see Fig. 2 and
Fig. 3) and was also clearly affected by the presence of
crystallization inhibitors. Thus, citrate, found at normal
levels in urine (2.64 X 10 -3 mol/1), only caused notable
effects at the lower phosphate amounts essayed, as is
shown in Fig. 4. The effects caused by phytate appears in
Fig. 5. As can be seen, when present at 1.54 X 10 -6 mol/1, in
all cases it produced important inhibitory effects.
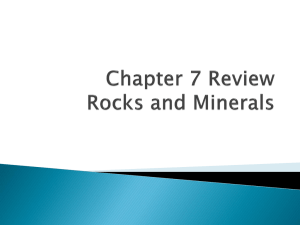
When artificial urine contained a glycoprotein (mucin), a
clear deposit of organic matter on one side of the cavity (the
lower one) was observed, where a notable increase in the
amount of hydroxyapatite and brushite crystals was detected
(see Fig. 6(a,b)).
The inner fine structure of sedimentary human renal phosphate non-infective calculi revealed structures very similar
to those obtained using the in vitro system applied in this
paper (Fig. 2(c, d), Fig. 3(c) and Fig. 6(c, d)). Thus, continuous and discontinuous layers of hydroxyapatite spherulites formed on inner surface renal calculi can be observed
in Fig. 2(c, d). Aggregates of brushite crystals are shown in
Fig. 3(c). In some cases hydroxyapatite was also found
combined with abundant organic matter and with brushite
crystals (see Fig. 6(c, d)).
DISCUSSION
Fig. 3. (a) Brushite crystalsformedin the absenceof organic matter
on the surface of the cavity walls, using synthetic urine III, and (b)
using syntheticurine IV (seeTable 1); (c) brushitecrystalsobserved
in a human phosphate non-infectiverenal calculus.
From the results it can be deduced that when no organic
matter was present, no calcium phosphate crystals (hydroxyapatite or brushite) were deposited in cavities with scarce
liquid renovation, in spite of conditions being favourable to
form crystals in the solution. Nevertheless, it was interesting
to observe in such case a regular and continuous layer of
hydroxyapatite being developed on the walls around the
cavity. This demonstrated that hydroxyapatite crystals
develop directly on the wall's cavity through heterogeneous
nucleation processes. Again this supported the importance
of the existence of a continuously renewed glycosaminoglycan layer covering the urothelium and protecting it against
urolith development (Gill et al., 1979; Grases et al., 1996b;
Grenabo et aL, 1988; See and Williams, 1992) thus, in the
absence of such a protective antiadherent layer, it is obvious
that in all cavities, with restricted urodinamic conditions,
SedimentaryKidney Stones
200-
200'
175 -
175 -
b
control
150-
150-
1.06x10" 3 mol/I citrate
2.64x
125
100-
o
•
•
control
•
2.64x10" 3 mol/l citrate
1.06x10" 3 molfl citrate
125 -
A
v
109
100-
75
~'
50
75
50
25-
25-
0
i
1,0
0,5
-
-
i
1,5
i
2,0
i
2,5
i
3,0
0
~-.
3,5
.
i
0,5
i
1,0
[Phosphate] x 10 2 (M)
1,5
2,0
2,5
3,0
3,5
[Phosphate] x 10 2 (M)
Fig. 4. Effects of citrateon crystaldevelopmentwhenvaryingthe phosphateconcentrationaccordingto the five valuesof artificialurinesof Table 1.
(a) Amountof calcium and (b) amountof phosphorous.
200.
200
175 •
175
b
control
150-
0.77x1() 6 moVI phytate
1.54xlff s mol/I phytate
125.
m control
0.77x1() e moVI p h y t a t e
1.54x11~ 6 mol/I phytate
150
J
/
~l
/ / ~
"~
125 -
A
100-
t~
E
ca
100 -
~
75-
.
75-
o
a.
50
50-
25
25-
0
",
0,5
i
1,0
•
-
o
i
,
i
1.5
2,0
2,5
3,0
0
3,5
[Phosphate] x 10 2 (M)
~.
0.5
|
1,0
•
-
115
i
r
i
2.0
2,5
3,0
3,5
[Phosphate] x 10 2 (M)
Fig. 5. Effects of phytate on crystal developmentwhen varying the phosphateconcentrationaccordingto the five values of artificial urines of
Table 1. (a) Amountof calcium and (b) amountof phosphorous.
continuous calcium incrustations would develop. It is
important to observe how the presence of crystallization
inhibitors cannot stop indefinitely the crystal development
and consequently can only stop its growth completely for a
limited period of time (Liu and Nancollas, 1970). Hence, it
is important that the solids that can appear in urine could be
eliminated as crystalluria as soon as possible to avoid the
development of bigger concretions that could be retained,
likewise completing the formation of a calculus. Therefore,
it is important to discuss the effect of the crystallization
inhibitors. In this manner, phytate manifested important
inhibitory effects for concentrations normally found in
urine (0.77-1.54 × 10 -6 mol]l). Nevertheless, citrate only
manifested important inhibitory effects at low phosphate
concentrations assayed, when found at important urinary
concentrations (2.64 × 10 -3 tool/l). Moreover, it must be
pointed out that the effects of the assayed inhibitors found in
this paper, when compared with those obtained previously
in similar but not so static conditions (Grases et al., 1994,
1996a, b), were clearly weaker. This again demonstrated
that urodynamics is important in determining the activity
of a given inhibitor. Consequently, the presence of retention
zones with a poor urodynamic efficacy implies an important
lithiasic risk factor and thus, obviously, sedentary lifestyle
contributes to an increase in such a risk. In fact previous
studies (Schulz et al., 1989a, b) have demonstrated that
morphologycal aspects can also play an important role in
the risk of renal stone formation.
When mucin (a glycoprotein) was present in the urine, a
clear deposit of calcified organic material was formed. As
can be seen in Fig. 6, this organic matter appeared mixed
with the spherulites of hydroxyapatite, demonstrating the
capacity of the glycoprotein agglomerates to act as heterogeneous nucleants of calcium salts and their important role
in the formation of the so-called sedimentary stones. Thereupon it should be pointed out that the development of
sedimentary calcium deposits was clearly detected only
when organic matter was present. This aspect confirms the
well known fact that sedimentary stones contain significant
amounts of organic matter, as can be observed in Fig. 6(c, d),
110
F. Grases and A. Llobera
Fig. 6. Hydroxyapatite (a), brushite (b) and organic matter (a, b) deposited on one side of the cavity when mucin was present, using synthetic urine
IV (see Table 1), hydroxyapatite (c), brushite (d) and organic matter (c, d) observed in a human phosphate non-infective renal calculus.
and has b e e n c o m m e n t e d on in previous papers (Grases
et al., 1996c; S r h n e l et aL, 1995). Actually, all the factors
which increase the a m o u n t of organic agglomerates will
favour the formation of c a l c i u m sedimentary renal stones.
C o m p a r i s o n o f the m o r p h o l o g y of the deposits obtained
in the in vitro experiments presented with the fine structure
o f sedimentary h u m a n n o n - i n f e c t i v e phosphate renal calculi
also demonstrated other important similarities. Thus, in real
h u m a n calculi, the occurrence of hydroxyapatite layers,
structureless from the macroscopic viewpoint, are really
c o m m o n (Fig. 2(c, d)). This was also observed in the
in vitro experiments presented (Fig. 2(a,b)). Moreover the
in vitro experiments demonstrated that such layers were
f o r m e d through the close growth of individual hydroxyapatite spheres on the same surface, in such a m a n n e r that they
finally constituted a c o n t i n u o u s layer, yet not as a result of a
s e d i m e n t a t i o n process. Association of large brushite crystals with hydroxyapatite spherulites is also frequent in renal
h u m a n calculi, as can be seen in Fig. 3(c) and Fig. 6(d), such
formations also b e i n g observed in the in vitro experiments
(Fig. 3(a, b) and Fig. 6(b)).
Finally, it is important to emphasize the f u n d a m e n t a l role
of s c a n n i n g electron m i c r o s c o p y in renal stone studies,
b e i n g essential in two f u n d a m e n t a l aspects: for the study
o f the fine structure o f renal calculi and to interpret the
results o f in vitro experiments devoted to establish the
m e c h a n i s m s of renal calculi formation and development,
REFERENCES
Cifuentes, L. D., 1984. Composici6n y estructura de los c~ilculosrenales.
Barcelona, Salvat, 57-81, 107-116.
Daudon M., Bader C. A., Jungers P., 1993. Urinary calculi: review of
classification methods and correlations with etiology. Scanning Microscopy, 7, 1081-1106.
Gill W. B., Ruggiero K., Straus F. H., 1979. Crystallization studies in a
urothelial-lined living test tube (the catheterized female rat bladder). I.
Calcium oxalate crystal adhesion to the chemically injured rat bladder.
lnv Urol, 17, 257.
Grases F., Costa-Bauz~iA., Conte A., 1993. Studies on structure of calcium
oxalate monohydrate renal papillary calculi. Mechanism of formation.
Scanning Microscopy, 7, 1067-1074.
Grases, F., Costa-BauzL A. and Garcia-Ferragut, L., in press. Biopathological crystallization: a general view about the mechanisms of renal
stone formation. Adv. Colloid Interface Sci.
Grases F., Costa-Bauzfi A., March J. G., 1994. Artificial simulation of the
early stages of renal stone formation. Brit J Urol, 74, 298-301.
Grases F., Garcia-Ferragut L., Costa-Bauzfi A., 1996. Study of the early
stages of renal stone formation: experimental model using urothelium
of pig urinary bladder. Urol Res, 24, 305-311.
Grases F., Garcia-Ferragut L., Costa-Bauz~iA., March J. G., 1996. Study of
the effects of different substances on the early stages of papillary stone
formation. Nephron, 73, 561-568.
Grases F., Srhnel O., Vilacampa A. I., March J. G., 1996. Phosphates
precipitating from artificial urine and fine structure of phosphate
renal calculi. Clin. Chim. Acta, 244, 45-67.
Grenabo L., Hedelin H., Hugosson J., Pettersson S., 1988. Adherence of
urease-induced crystals to rat bladder epithelium following acute
infection with different uropathogenic microorganims. J Urol, 140,
428.
Hesse A., Berg W., Bothor C., 1979. Scanning electron microscopic investigations on the morphology and phase conversions of uroliths, lnt
Urol Nephrol, 11, 11-20.
Iwata H., Abe Y., Nishio S., Wakatsuki A., Ochi K., Takeuchi M., 1986.
Crystal-matrix interrelations in brushite and uric acid calculi. J Urol,
135, 397-401.
Khan S. R., Hackett R. L., 1986. Identification of urinary stone and sediment crystals by scanning electron microscopy and X-ray microanalysis. J Urol, 135, 818-825.
Leusmann D. B., 1991. A classification of urinary calculi with respect
to their composition and micromorphology. Scand J Urol, 25, 141150.
Liu S.-T., Nancollas G. H., 1970. Kinetics of crystal growth of calcium
sulfate dihydrate. J Crystal Growth, 6, 281-289.
Meyer A. S., Finlayson B., DuBois L., 1971. Direct observation of urinary
stone ultrastructure. Brit J Urol, 43, 154-163.
Prien E. L., Frondel C., 1947. Studies in urolithiasis. I. The composition of
urinary calculi. J Urol, 57, 949-994.
Schulz E., BSrner R., Brundig P., M~iurerF., 1989. Influence of different
factors on the formation of calcium oxalate stones. I. Discriminant
analytical computations of morphological parameters of the
Sedimentary Kidney Stones
pelvic-calyceal systems of calcium oxalate stone formers and controls. Eur Urol, 16, 212-217.
Schulz E., B6rner R., Brundig P., M~iurer F., 1989. Influence of different
factors on the formation of calcium oxalate stones. II. Discriminant
analytical computations of morphological parameters of pelviccalyceal systems and clinicochemical urine parameters of controls
and calcium oxalate stone formers. Eur Urol, 16, 218-222.
111
See W. A., Williams R. D., 1992. Urothelial injury and clotting cascade
activation: common denominators in particulate adherence to urothelial surfaces. J Urol, 147, 541.
S6hnel O., Grases F., Garcla-Ferragut L., March J. G., 1995. Study on
calcium oxalate monohydrate renal uroliths. III. Composition and
density. Scand J Urol Nephrol, 29, 429-435.