Provider-Performed Microscopy
advertisement

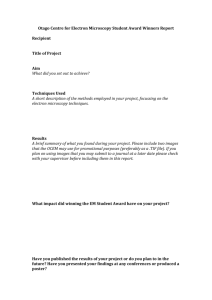
Point of Care Vol. 2, No. 1, 20–32 © 2003 Lippincott Williams & Wilkins, Inc., Philadelphia Provider-Performed Microscopy A Review Frederick L. Kiechle, MD, PhD, Isabel Gauss, MT(ASCP), and Barbara Robinson-Dunn, PhD The examinations of labile specimens under the bright-field or phase contrast microscope are classified as provider-performed microscopy (PPM). With a PPM certificate issued by the Centers for Medicare and Medicaid Services Administration, a physician, nurse practitioner, nurse midwife, physician assistant, or dentist may perform PPM and waived procedures. Provider-performed microscopy procedures use specimens, such as body fluids or skin scrapings. Because quality control material is not available for PPM procedures, quality assurance assessment is complicated. Policies and procedures must be written for each test procedure. Provider-performed microscopy procedures include wet mounts, KOH preparations, pinworm detection, fern test, postcoital test, microscopic urinalysis, fecal leukocytes, semen analysis for presence of sperm and motility, and eosinophils in nasal smears. The quality of PPM is dependent on adequate training and retraining to achieve optimal skills. Key Words: Provider-performed microscopy—Waived tests—Bright-field microscopy—Phase-contrast microscopy—KOH preparation—Wet mounts—Pinworm detection—Postcoital test—Microscopic urinalysis—Semen analysis—Nasal eosinophils. rovider-performed microscopy (PPM) refers to a group of procedures that evaluate labile specimens using bright-field or phase-contrast microscopy, which were defined in the Federal Register of April 25, 1995 and revised on October 1, 1998. A summary of the criteria for these PPM procedures is listed in Table 1. The evaluation of synovial fluid by phase-contrast microscopy for monosodium urate crystals (gout) or calcium pyrophosphate dihydrate crystals (pseudogout)1,2 is excluded from this group of PPM procedures. The microscopic evaluation of P From the Department of Clinical Pathology, William Beaumont Hospital, Royal Oak, Michigan. Address correspondence and reprint requests to Frederick L. Kiechle, MD, PhD, Department of Clinical Pathology, William Beaumont Hospital, 3601 West 13 Mile Road, Royal Oak, MI 48073–6769 (e-mail: fkiechle@beaumont.edu). 20 crystals in synovial fluid may be performed initially with an ordinary bright-field microscope (Fig 1); however, the definitive identification of the crystals requires a polarizing microscope. 2 Providerperformed microscopy procedures use specimens such as body fluids or skin scrapings (Table 2).3 The federal law described by Centers for Medicare and Medicaid Services (CMS) Administration in the Clinical Laboratory Improvement Amendments of 1988 (CLIA’88) classify laboratory procedures based on their complexity using well-defined criteria: waived, moderately complex, provider-performed microscopy, and highly complex.4,5 Provider-performed microscopy, as defined by CLIA’88, is a subset of tests classified as moderately complex. Quality assurance assessment of these PPM procedures is complicated by the absence of a readily available source of quality Table 1 Criteria for provider-performed microscopy procedures 1. The procedure must be categorized as moderately complex. 2. The examination must be personally performed by a practitioner. 3. The primary instrument for performing the test is the microscope, limited to bright-field or phase-contrast microscopy. 4. The specimen is labile, or delay in performing the test could compromise the accuracy of the test result. 5. Limited specimen handling or processing is required. 6. Control materials are not available to monitor the entire testing process. control testing material (Table 1). However, there is the potential for developing home brew material to simulate the fern test or others.6 The CMS issues certificates of registration, which may be limited to PPM or waived testing (Table 3). A certificate for performing waived testing is not sufficient to cover PPM testing. However, waived testing may be performed under a PPM certificate. With a PPM certificate, only physicians, nurse practitioners, nurse midwifes, physician assistants, or dentists may perform the testing at the time of the patient’s visit. A PPM certificate costs $200 every 2 years and in a hospital, it is usually obtained by a physician designated as responsible for PPM testing in a specific area.6 The Joint Commission on Accreditation of Health Care Organizations (JCAHO) indicates that documentation of competence or training is not required for physicians or dentists when the test is a logical part of his or her specialty.7 However, if the test is performed by a midlevel practitioner, like a nurse practitioner, nurse midwife, or physician assistant, docu- mentation of initial training and ongoing competency assessment is required. The frequency of the determination of competency assessment is a decision left to the health care organization. Also, JCAHO states that there should be a system in place to ensure the accuracy and reliability of the test results.7 Although proficiency testing is not required, it could be used to meet this standard. Kodachrome or digital images could be used to organize proficiency and competency testing. Intranet-enabled competency challenges may be custom built using Microsoft (Redmond, WA) technologies, such as Active Server Pages and Access and filing user details or using Healthstream (Nashville, TN) (formerly “m3 Learning” (Dallas, TX).8 The latter uses a combination of third-party authoring software (Macromedia Authorware, San Francisco, CA) and server scripting. Both formats provide the user with a list of questions. The answers may be scored and calculated as a percent of correct responses. Electronic documentation of test Table 2 Provider-performed microscopy tests and CPT codes CPT Code Test Description Q0111 Wet mounts, including preparations of vaginal, cervical or skin specimens Q0112 All potassium hydroxide (KOH) preparations Q0113 Pinworm examinations Q0114 Fern test Q0115 Post-coital direct, qualitative examinations of vaginal or cervical mucous 81015 Urinalysis; microscopic only 81000 Urinalysis, by dipstick or tablet reagent for bilirubin, glucose, hemoglobin, ketones, leukocytes, nitrite, pH, protein, specific gravity, urobilinogen, or any number of these constituents; non-automated, with microscopy 81001 Urinalysis, by dipstick or tablet reagent for bilirubin, glucose, hemoglobin, ketones, leukocytes, nitrite, pH, protein, specific gravity, urobilinogen, or any number of these constituents; automated, with microscopy NOTE: May only be used when the laboratory is using an automated dipstick urinalysis instrument approved as waived. Fig 1 Colorless monosodium urate crystals (bright field, original magnification x 10). Point of Care, vol. 2, no. 1 81020 Urinalysis; two or three glass test G0026 Fecal leukocyte examination G0027 Semen analysis; presence and/or motility of sperm excluding Huhner 89190 Nasal smears for eosinophils Centers for Medicare and Medicaid Services, as of April 1, 2002. CPT; Current procedural terminology. Provider-Performed Microscopy 21 information permits filterable reports that may be sorted by physician or date for documentation of compliance activity. Alternatively, this goal may be accomplished by purchasing the Excel program XL-G from the College of American Pathologists (CAP). In conclusion, competency indicators for PPM might include monitoring the number of proficiency-testing or blind samples testing failures or failed procedural observations.9 In this way, the staff and resident physician performing these procedures may be monitored. Policies and procedures must be written for each test procedure.9 The procedure manual should include a section on specimen collection, method, handling and disposal of infectious specimens, interpretation, and equipment maintenance. Maintenance includes both the microscope and the centrifuges, which should be in good condition and routinely serviced. All PPM results should be filed in the patient’s chart, along with the date and name of the person who performed the test.6,9 Regulatory agencies evaluate the performance of PPM testing using the same criteria as all other laboratory procedures with the exception of quality control records (Table 1). A recent evaluation by CMS of laboratories performing PPM revealed a variety of quality problems.10 The top four quality issues included 38% of sites did not evaluate test accuracy two times a year, 36% had no microscope and/or centrifuge maintenance, 28% had no director approved standard operating procedure manual, and 25% did not document personnel competency.10 PPM Procedures: Examples KOH and wet mount preparations Direct microscopic examination of many clinical specimens with saline or with potassium hydroxide (KOH) can reveal the presence of microorganisms such as fungi and Trichomonas vaginalis. This test can also be used to demonstrate the presence of clue cells indicative of bacterial vaginosis. Potassium hydroxide is used for direct examination of hair, skin scrapings, nails, and fluids (e.g., vaginal exudate). The fungal cell wall contains chitin making the fungi relatively resistant to the lytic action of KOH.11 Because of this property KOH can be used to 22 F. L. Kiechle et al dissolve clinical material (either solid or liquid) leaving the fungal elements. Over time (2 to 3 days), the KOH will also dissolve any fungi present in the sample. To prevent this, a small amount of glycerol added to the KOH solution will protect the fungi for several days.12 Skin scrapings should be obtained from the leading edges of a presumed “ringworm” lesion. Often, a Wood’s lamp can be used to localize the area from which the specimen should be obtained. Care must be taken to ensure that clinical specimens are not obtained with cotton or fiber swabs because those fibers may resemble fungal elements when viewed under the microscope. A 10% aqueous solution of KOH is used in this test. The KOH must be stored in a nonglass vial because the extremely basic solution will leach minerals from glass thus rendering the solution cloudy and unusable.13 A drop of KOH is mixed with the clinical specimen on a clean glass slide and a cover slip is placed over the specimen. The specimen is then gently warmed and should still be cool enough to be touched. Do not allow the KOH to boil and evaporate. The slide preparation must “cure” at room temperature until the clinical material clears (dissolves). The amount of time necessary for digestion of the proteinaceous material varies with the type and size of the specimen. For example, a piece of fingernail will take much longer to dissolve than will a skin scraping. A brightfield microscope is commonly used to examine KOH and wet mount preparations. Because most microorganisms and human cells have a very low refractive index (unless they are dematiaceous or darkly colored), it is necessary to reduce the light used for viewing the specimen. After the slide preparation is placed on the stage of the microscope, the condenser, which serves to focus the beam of light, should be lowered. (The condenser is the component of the microscope that is between the stage and the light source.) The specimen can be screened on low power and then examined in more detail on high power. Saline is used to emulsify vaginal fluids for microscopic examination. A drop of saline is mixed with a drop of the specimen on a clean glass slide and then covered with a glass coverslip. It may be gently Point of Care, vol. 2, no. 1 pressed down on the slide to provide for better viewing through the suspension. When examining the saline wet mount on low power, the microscopist should look for clue cells and for movement due to Trichomonas vaginalis. Clue cells are epithelial cells whose edges are obscured by the presence of adherent bacteria (Fig 2). T. vaginalis is a flagellated protozoan parasite whose movement has been described as “jerky.” Trichomonads are 7 to 23 µm long and 5 to 15 µm wide, with an obvious axostyle and an undulating membrane that stops halfway down the side of the protozoan (Fig 3).14 Because they are often difficult to see in a wet mount, it may be necessary to examine several specimens before finding T. vaginalis in the specimen. As it slows down, the undulating membrane may become visible. Specimens to be examined for the presence of T. vaginalis must not be refrigerated because the protozoan will rapidly become nonviable. If the clinical specimen has been digested by KOH, it should be relatively easy to determine if fungal elements are present in the specimen. It is not necessary to use an oil immersion lens to examine a KOH preparation of a clinical specimen and may actually provide some degree of confusion and “over-reading” of the specimen if it is used. The fungal elements will either appear as small pieces of septate hyphae or as budding yeasts (oval or elongated) (Fig 4). Cellulose tape preparations for detection of pinworms Infection with pinworms (Enterobius vermicularis) is one of the most common parasitic diseases and has Fig 2 Clue cells in vaginal specimen. Epithelia cell edges are obscured by bacteria (bright field, original magnification x 40). Point of Care, vol. 2, no. 1 Fig 3 Wet mount of Trichomonas vaginalis (right) and two epithelial cells (left) (bright field, original magnification x 40). been recognized since ancient times. Pinworms are acquired by fecal-oral contamination via unwashed hands, soiled pajamas, contaminated toys, or other objects. Eggs contaminating the environment can be killed by sunlight or radiation from ultraviolet lights. Following ingestion of infective eggs, the parasites hatch and develop into adult worms. The female worm matures and within approximately 1 month, is capable of producing eggs. Following fertilization by the male worm, the female migrates out of the anus and deposits eggs on the anal and perianal surfaces (Fig 5). The eggs mature rapidly and are fully infective within a few hours. Persons infected with pinworms complain of intense itching, irritability, and insomnia. The itching is due to the female worm migrating out of the anus to deposit her eggs. Since the worms migrate and lay eggs at night, specimens should be obtained after the patient has been asleep for several hours or early in the morning before the patient has used the bathroom. The irritability and insomnia that are common complaints from a person suspected of pinworm infection are also due to the itching, which interrupts normal sleep patterns. The specimen to be examined for pinworms consists of touch preparations of anal and perianal skin and can be obtained by wrapping a piece of clear cellulose tape (sticky side against the glass slide) lengthwise around the end of a glass slide. To obtain the Provider-Performed Microscopy 23 Fig 4 (A) KOH preparation of fungal elements (oval yeast and hyphae) in a skin scraping (bright field, original magnification x 40). (B) KOH preparation of budding oval yeast in a vaginal exudate (bright field, original magnification x 40). specimen, one end of the tape is released. A tongue depressor is placed against the side of the tape that is still secured to the slide and the free end of the tape is bent back against it (sticky side out). The tape is then pressed against several of the areas in which the itching is intense. To examine the specimen microscopically, the side of tape that has been used to collect the specimen is bent back around the slide and pressed against it. A drop of xylene or toluene may be added under the edge of the tape to clear it. The glass slide/tape preparation is placed on the stage of the microscope with the specimen on the top of the slide. The slide is examined under low power (10 × or 20 ×) with reduced light intensity. If a pinworm has deposited eggs, they will appear to be football-shaped with one side flattened and are 20 to 30 µm by 50 to 60 µm in size (Fig Fig 5 Female Enterobius vermicularis warm releasing eggs (bright field, original magnification x 10). 24 F. L. Kiechle et al 6). It is necessary to examine 4 to 6 consecutive negative tape preparations to rule out infection. Additionally, it is not necessary to submit fecal samples to the laboratory for diagnosis of pinworms as they are only occasionally recovered from these specimens.15 Fern test The fern test is performed to determine if rupture of the fetal membranes has occurred before the onset of labor. This premature rupture of membranes occurs in approximately 10% of pregnant patients. The test is performed by placing a small amount of vaginal fluid onto a glass slide, which is allowed to air dry. The slide is then examined microscopically for fern formation (Fig 7). The fern pattern occurs when the relative Fig 6 Scotch tape preparation demonstrating Enterobius vermicularis eggs (bright field, original magnification x 10). Point of Care, vol. 2, no. 1 Fig 7 Dried amniotic fluid on a slide demonstrating a positive fern test with an arborization pattern (bright field, original magnification x 10). concentration of electrolytes, proteins, and carbohydrates, especially sodium chloride, is sufficient to support crystallization in an arborization pattern.16,17 The salt concentration is determined by the amount of estrogen in the mucus. Amniotic fluid will crystallize after 20 weeks gestation. If the specimen is amniotic fluid, it will dry in the characteristic fern-like pattern. Other body fluids that will display this slide arborization include CSF, serum, and saliva.18,19 Urine will not dry in this unique pattern.6 Fern testing is considered to be as sensitive but less specific than Nitrazine pH testing.18 Meconium and blood at dilutions of less than 1:1 will not interfere with ferning. The best sensitivity can be achieved by using a combination of medial history, ferning, and Nitrazine testing.18 Estrogen promotes crystallization while progesterone inhibits it. Alpha fetoprotein, fetal fibronectin, and other cytologic stains may be useful in evaluating patients with possible premature rupture of membranes, but are more costly.18,19 Postcoital test The postcoital test evaluates factors that affect fertility and is performed during the middle of the ovulatory cycle. After 3 days of sexual abstinence, the patient should remain in bed 10 to 15 minutes following coitus to allow the semen to contact the cervical mucus. A sterile speculum is used to aspirate an endocervical mucus specimen, which should be collected within 24 hours of coitus.20 The complete postcoital test20–22 includes qualitative assessment (PPM procedure, Point of Care, vol. 2, no. 1 Table 2) including color, viscosity, tenacity, and the presence of ferning, as well as direct microscopic examination of sperm number and motility in cervical mucus (Sims-Huhner test; not a PPM procedure, Table 2). The cervical mucus should be clear with minimal viscosity. Its elasticity or spinnbarkeit increases at ovulation. A positive cervical mucus test is defined as a thread of mucus attached to a glass coverslip lifted from a glass slide on which cervical mucus has been placed.20,21 The clinical utility of the qualitative postcoital cervical mucus tests are in dispute.22–25 For example, qualitative cervical mucus characteristics were not predictive of a couple’s future pregnancy, whereas quantitative sperm characteristics were predictive.22 The reverse was found to be true when inducing singleton pregnancies in anovulatory women treated with human menopausal gonadotropin.24 Urinalysis: microscopic A complete urinalysis includes visual, microscopic, and chemical examination of urine.26 The kidneys and urinary tract are not available for direct physical examination.27 Therefore, evaluation of a urine specimen represents a liquid tissue biopsy of the urinary tract.3,26 Uroscopists or pisse-prophets used a urine circle composed of 21 segments describing urine color compared with known substances and associated clinical interpretation during the Byzantine era (330 to 1453 AD).28–30 For example, green coloration at the top of the specimen was associated with pleurisy.30 Today, green urine is associated with the presence of a variety of substances including bile pigment, porphyrins, mitoxantrone, and food dye and color blue number 1.28,31,32 The invention and introduction of scientific methods provided early reports of urinary microscope crystals in the 17th and 18th century, followed by more systematic evaluation of urinary sediment in the 19th century.33,34 The most accurate laboratory data is obtained from a specimen that has been properly collected.26,28 A contaminated specimen should be suspected if a large number of squamous epithelial cells and bacteria are observed.35 Formed elements in the urinary sediment including red cells (Fig 8), red cell casts (Fig 9), white cells Provider-Performed Microscopy 25 Fig 8 Red cells in urine sediment (bright field, original magnification x 10). Fig 10 Polymorphonuclear leukocytes in urine sediment (oil immersion, original magnification x 50). (Fig 10), white cell casts (Fig 11), tubular casts, granular casts, and fatty casts are associated with glomerular, tubulointerstitial, or vascular kidney disease. Acute allergic interstitial nephritis is associated with the presence of urinary eosinophils.36 These formed elements are unstable in urine. Urinary microscopy should be performed within 1 hour using storage at room temperature or within 4 hours using storage in refrigeration. In the pediatric age group, white cells are less stable and begin to degrade between 2 and 4 hours in the refrigerator.37 In a CAP Q-Probe Study,38 11.2% of never-refrigerated urine specimens from hospitalized patients were evaluated after 2 hours. To prevent this degradation of formed elements over time, a variety of preservatives have been evaluated.39,40 Some cellular elements exhibit improved survival in the presence of preservative after 3 days compared with refrigeration without a pre- servative.39 However, statistical significance between the differences was not achieved. Variations also exist in specimen preparation. The urinary elements may be examined under the microscope after centrifugation and resuspension of the pellet26,40,41 or in unspun urine39 using the Kova system (ICL Scientific, Fountain Valley, CA)42 or a hemocytometer for leukocyte counts.43 For centrifuged urine specimens, 12 mL of well-mixed, fresh urine should be spun for 400 × g for 5 minutes. The supernatant should be decanted and the sediment resuspended. A drop of resuspended sediment should be placed on a glass slide and a coverslip placed on top. Microscopic examination by bright field or phase contrast may be initiated after the cellular elements have been allowed to settle for 30 to 60 seconds.3 The centrifugation process may remove protein including casts and lipids, which will adhere to the glass surface of the tube41 and crystal formation may be altered.44 Fig 9 Red cell cast in urine sediment (bright field, original magnification x 50). 26 F. L. Kiechle et al Fig 11 Polymorphonuclear leukocyte cast in urine sediment (bright field, original magnification x 50). Point of Care, vol. 2, no. 1 The relationship between laboratory testing regulations on the availability of laboratory tests and quality practices in physician offices has been investigated.45–47 Generally, there is lower availability of tests and a reduced number of tests performed in physician office laboratories in states with laboratory regulations for the evaluation of urinary tract infections.45 For example, the American Academy of Pediatrics practice parameter48 recommends urinalysis as a screening method for urinary tract infection in young children. Results that are suggestive of a urinary tract infection in a young child or infant include a positive leukocyte esterase or nitrite on a urine dipstick analysis (a waived procedure), greater than five white cells per high power field on a spun urine sediment (a PPM procedure), or the presence of bacteria in an unspun gram-stained specimen (a moderately complex procedure). Forty-six percent of physician office laboratories have a certificate to perform only waived procedures and 32% have a PPM certificate, which would allow them to perform the first two procedures (waived and PPM) only (Table 3). Therefore, all three laboratory evaluations in the practice parameter cannot be adequately completed in most physician office laboratories.49 The three glass test (CPT code 81020, Table 2) of Meares and Stamey is used to evaluate the pathogenic site of urinary tract problems in males.50 The urine is collected sequentially in three containers and each is examined microscopically. Abnormal findings (white cells, bacteria, etc) in the first collection container Table 3 would represent a urethral problem; the second, bladder or upper urinary tract; the third, prostate, and this collection has the highest concentration of prostatic secretions. A two glass test has been used to screen for urethritis in males,51,52 as well as females.53 The scientific basis and clinical usefulness of the two glass test has been questioned.51,52 Fecal leukocytes The cause of loose, watery stools observed in patients with diarrhea may be evaluated using bacterial culture, investigation for ova and parasites, and fecal leukocytes.54 To perform this PPM procedure, a fleck of stool or mucus is placed on a glass slide and stained with Wright’s or Löffler methylene blue.55 After placing a coverslip over the mixture, a rough quantitative count of mononuclear and polymorphonuclear cells are distinguished among 200 total cells or their numbers are estimated per high power field. Greater than five leukocytes per high power field is usually considered positive.56,57 At five leukocytes per high power field, the test’s sensitivity (63.2%) and specificity (84.3%) is similar to that reported for fecal lactoferrin,57 but not as good as myeloperoxidase.58 The sensitivity of the fecal leukocyte count in the detection of shigellosis is dependent on the collection technique.59 The cup stool specimen (95% sensitive) had a sensitivity greater than swab or diaper specimens (44% sensitive). The presence of fecal leukocytes indicates the presence of an inflammatory condition caused by a specific CLIA registration and fees Enrollment No. of Labs No. of Physician Office Laboratories Total laboratories in nonexempt states 167,744 96,922 — — — Total laboratories in CLIA exempt states (New York, Washington) 5,447 Biennial Fee Application type Compliance (CMS surveys) 22,056 (13%) 14,715 (15%) — Waiver 91,516 (55%) 44,111 (46%) $150 Provider-performed microscopy 37,455 (22%) 31,376 (32%) $200 Accreditation by CMS approved organization 16,717 (10%) 6,720 (7%) Volume dependent $150–$6,220 Centers for Medicare and Medicaid Services (CMS), data from October, 2001. CLIA; Clinical Laboratory Improvement Amendments of 1988. Point of Care, vol. 2, no. 1 Provider-Performed Microscopy 27 organism like Salmonella, Shigella, invasive Escherichia coli, Campylobacter jejuni, Vibrio cholerae, Yersinia or Entamoeba histolytica, or a nonspecific etiology like ulcerative colitis, antibiotic-associated colitis, or collagenous colitis.54,55,59–64 Cases of diarrhea are associated with viruses, most parasites (excluding Entamoeba) or bacterial toxins are not associated with the presence of fecal leukocytes. Semen analysis Semen or seminal fluid is composed of products contributed by various male reproductive organs including seminal vesicles, prostate, epididymis, vas deferens, bulbourethral glands and urethral glands.65,66 Spermatozoa are maintained in semen. For example, seminal vesicular secretions are important for the maintenance of normal semen coagulation, sperm motility, and sperm chromatin stability.66 Semen analysis may be performed to evaluate an infertile couple,23,67 to detect sexual assault,68 or to investigate the effectiveness of bilateral vasectomy or the sperm’s suitability for use in artificial insemination procedures.67,69 Qualitative semen analysis, limited to the presence or absence of sperm and the detection of sperm viability, is classified as a PPM procedure (CPT code G0027, Table 2). This CPT code does not include the evaluation of the number of motile sperm per high power field in cervical mucus during the postcoital or Sims-Huhner test.21,23 Postvasectomy patients should provide several semen specimens to assure that no viable or nonviable sperm are present (Fig 12). A wet mount preparation on a glass slide with a coverslip is adequate. In the emergency center, a saline wet mount of a swap of a specimen obtained from a sexual assault victim may be used for a pointof-care search for motile or nonmotile sperm under a microscope.68 Semen should be collected in a sterile container by masturbation or with a special collection condom during intercourse after a minimum of 2 days, but not longer than 5 days, of sexual abstinence.23 The viscus yellow-gray semen forms a coagulum in which the sperm are trapped. Liquefaction begins within 10 to 20 minutes at room temperature and is complete within 1 hour.23,65 Laboratory evaluation should be performed with 1 to 2 hours after collection. Semen analysis for the evaluation of the infertile couple and adequacy for artificial insemination procedures requires additional procedures including assessment of physical semen characteristics, sperm concentration and motility grading, sperm morphology, sperm viability, and bacteriologic studies.23,65,67,69 Although the percent of sperm moving forward is used to assess sperm mobility and quality, it is not highly correlated with the fertilizing capacity of semen samples.70,71 To successfully fertilize an egg, sperm must pass through a substantial cumulus cell layer, then the thick extracellular matrix, the zona pellucida, and finally the plasma membrane.72 To complete this journey, sperm are hyperactivated, resulting in an increase in flagellar bend amplitude and beat asymmetry.73 At a biochemical level, hyperactivation requires the opening of a voltage-dependent Ca2+-channel (CatSper).74 CatSper mRNA and protein are only found in testis and the Ca2+-channel is located on the plasma membrane of the principal piece of sperm. It is required for normal sperm motility and for sperm penetration of the zona pellucida.74 The evaluation of the presence of sperm and sperm motility represents the first screen for genetic mutations that may result in male sterility (mutations in calmodulin-dependent protein kinase, Camk4, which phosphorylates protamine-2) or complete arrest of late spermiogenesis and increased germ cell apoptosis (mutations in TATA-binding proteinrelated protein, TLF, which regulates transcription during mammalian spermatogenesis).75 Eosinophils in nasal smears Fig 12 Viable sperm in semen (bright field, original magnification x 10). 28 F. L. Kiechle et al Increased eosinophils in nasal smears are associated with seasonal or airborne latex allergic rhinitis76–79 Point of Care, vol. 2, no. 1 and nonallergic chronic nasal disorders, like nasal polyposis.80 In the allergic rhinitis group, the nasal eosinophil scores significantly correlated with the clinical signs score.77 Over a 3-year study period, school children with early onset nasal hypereosinophilia were more likely to develop nasal symptoms later.78 In the chronic nonallergic nasal disorder group, the average nasal eosinophil count was 1.5 ± 2.3% compared with controls, 5 ± 2.6%.80 The degree of nasal eosinophilia correlated with the number of eosinophils detected in surgically removed nasal polyps.80 Eosinophils release granules, which contain cytotoxic proteins by two morphologic degranulation patterns, piecemeal degranulation, or eosinophil cytolysis.81 These patterns can be distinguished in tissue biopsies using transmission electron microscopy. Nasal biopsies from patients with allergic rhinitis show the greatest degree of eosinophil degranulation and nasal polyps revealed the second greatest degree compared with allergic asthma.81 These findings support the concept that the inflammatory response in the airway is unified and that allergic rhinitis of the upper airway is associated with eosinophilia of the lower airway in associated allergic bronchitis or asthma.82 Allergic rhinitis is also associated with increased transcription and translation of the inducible isoform of nitric oxide synthase and nitric oxide production79,83,84; increased expression of GATA-3 which is a transcription factor which regulates interleukin-5 gene expression 85; and increased interleukin-5 in nasal lavage fluid.79 Nasal smears are prepared by transferring a thin smear of the nasal mucus collected on a cotton swab onto a glass slide3 or by impression cytology.86 Air dry the smear and stain with either Hansel or WrightGiemsa stains. The smear should be examined under low and high power using a bright field microscope. Polymorphonuclear leukocytes will have a segmented nucleus with 2 to 5 lobes which will stain blue and the cytoplasm will be clear and homogeneous (Hansel) or neutral pink staining secondary granules (WrightGiemsa). Eosinophils will have bilobed blue nuclei and deep red granules in the cytoplasm or outside the cell if released from degranulated eosinophils (Fig 13). To estimate the number of eosinophils, locate an area that is well-stained and representative of the slide that contains approximately 50 to 100 cells. If three eosinophils are observed in a field of 50 polymorphoPoint of Care, vol. 2, no. 1 Fig 13 Bilobed eosinophil (arrow) and three polymorphonuclear leukocytes in nasal smear (Wright-Giemsa stain, oil immersion, original magnification x 50). nuclear leukocytes plus eosinophils, 6% eosinophils would be reported. A grading system may be used as illustrated below. Eosinophils/% Eosinophils None seen/0% Rare/1% to 9% Few/10% to 40% Many/more than 40% No quality control is available; however, a peripheral blood smear with increased eosinophils stained at the same time will monitor the staining quality. Conclusion Provider-performed microscopy procedures provide a method for diversification of personnel performing laboratory tests.87 In this case, the tester may be a physician, nurse practitioner, nurse midwife, physician assistant, or dentist. In a hospital setting, the CMS license to perform PPM is best obtained by a physician responsible for the clinic or subspecialty performing the PPM procedures.6 This policy removes this activity from the central laboratory’s CMS license, but allows the point-of-care coordinators to provide assistance in program design and monitoring.6 The second advantage of this organizational structure is that because both the central laboratory’s primary inspection organization, CAP, and the hospital’s primary inspection organization, JCAHO, differences in PPM regulations are minimized. 88 Because the CAP does not distinguish between the different types of test complexity described by Provider-Performed Microscopy 29 invasive techniques for measuring cellular elements or chemical constituents.100,101 References Fig 14 Artifacts introduced by scratches on the glass coverslip during urine microscopy (bright field, original magnification x 10). CLIA’88, the checklist questions for competency and training for any point-of-care test would apply for personnel performing PPM procedures. Examples of competency indicators for PPM have been described3,9 and Web-based competency testing has been reported.8,89 Efforts to reduce fatal or nonfatal medical errors in diagnoses, surgery, and prescriptions are under investigation, especially the more numerous prescription errors.90 A comparison of the emergency physicians and laboratory “technicians” to perform urine microscopy reported good agreement for red cell detection but poor agreement on detection of white cells and bacteria.91 These findings reinforce the need for adequate training and retraining to achieve optimal skills. There are a variety of printed, intranet, or internet sources available for reviewing images of formed elements in urine.8,89,92–94 Artifacts may be present and should be identified. Fig 14 illustrates the artifact introduced by scratches on the coverslip used for urine microscopy, which may be mistaken for fungal hyphae. Two or more procedures may be superior to a single procedure in detecting disease. For example, the microscopic examination of both spun urine and vaginal fluid specimen yields an improved detection rate of Trichomonas vaginalis.95 Algorithms may also be used that will recommend the next step following the completion of a screening PPM procedure,96 which should include the evidence-based logic for the algorithm’s selection.97–99 The future of point-of-care test procedures, in general, rests on the successful development of noninvasive or minimally 30 F. L. Kiechle et al 1. Kerolus G, Clayburne G, Schumacher HR Jr. Is it mandatory to examine synovial fluids promptly after arthrocentesis? Arthritis Rheum 1989;32:271–278. 2. Pascual E, Torar J, R␦iz MT. The ordinary light microscope: an appropriate tool for provisional detection and identification of crystals in synovial fluid. Ann Rheum Dis 1989;48:983–985. 3. Provider-Performed Microscopy Testing: Proposed Guideline. National Committee for Clinical Laboratory Standards Document HS2-P. Wayne, PA: NCCLS; 2000. 4. Ehrmeyer SS, Laessig RH. Regulatory requirements (CLIA’88, JCAHO, CAP) for decentralized testing. Am J Clin Pathol 1995;104(Suppl 1):S40–49. 5. Cembrowski GS, Kiechle FL. Point of care testing: critical analysis and practical application. Adv Pathol Lab Med 1994;7:3–26. 6. Kiechle FL, Gauss I. Provider-performed microscopy. Clin Lab Med 2001;21:375–387. 7. Joint Commission on Accreditation of Healthcare Organization. 2000–2001 Comprehensive Accreditation Manual for Pathology and Clinical Laboratory Services. Oakbrook Terrace, IL: JCAHO; 1999:268. 8. Kiechle FL, Gauss I, Ross K, et al. Point-of-care testing education using the intranet [Abstract]. Ann Clin Lab Sci 2001;31:301. 9. Joint Commission on Accreditation of Healthcare Organization. Quality Point of Care Testing. A Joint Commission Handbook. Oakbrook Terrace, IL: JCAHO; 1999:41–73. 10. Centers for Medicare and Medicaid Services. CMS CLIA waived/PPMP laboratory project. April 18, 2002. Available at: http;://www.cms.hhs.gov/clia/cowppmp.asp. Accessed July 10, 2002. 11. McGinnis MR. Clinical specimens. In: Laboratory Handbook of Medical Mycology. San Diego: Academic Press; 1980:73–102. 12. Larone DH. Laboratory procedures. In: Medically Important Fungi: A Guide to Identification. Washington, DC: ASM Press; 1995:209–24. 13. Robinson BE, Padhye AA. Collection, transport and processing of clinical specimens. In: Wentworth BB, Bartlett MS, Robinson BE, et al., eds. Diagnostic Procedures for Mycotic and Parasitic Infections. Washington, DC: APHA; 1988:11–32. 14. Garcia LS. Protozoa from other body sites. In: Diagnostic Medical Parasitology. Washington, DC: ASM Press; 2001:120–127. 15. Garcia LS. Intestinal nematodes. In: Diagnostic Medical Parasitology. Washington, DC: ASM Press; 2001:274–277. 16. Addison A. Obstetrical ferning test. Lab Med 1999;30:451. 17. Bauer J. Examination of body fluids in Clinical Laboratory Methods. Saint Louis: CV Mosby Co; 1974:623–629. 18. Peredy TR, Powers RD. Bedside diagnostic testing of body fluids. Am J Emerg Med 1997;15:400–407. 19. Kiechle FL. Point of care testing for body fluids. In: Kost GJ, ed. Principles and Practice of Point-of-Care Testing. Philadelphia: Lippincott, Williams & Wilkins; 2002:267–283. 20. Gronowski AM, Landau-Levine M. Reproductive endocrine function. In: Burtis CA, Ashwood ER, eds. Tietz Textbook of Point of Care, vol. 2, no. 1 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. Clinical Chemistry. Philadelphia: WB Saunders Co; 1999;1601–1641. Pagana KD, Pagana TJ. Sims-Huhner test. In: Mosby’s Diagnostic and Laboratory Test Reference. St Louis: Mosby; 2001:777–779. Beltsos AN, Fisher S, Uhler ML, et al. The relationship of the postcoital test and semen characteristics to pregnancy in 200 presumed fertile couples. Int J Fertil Menopausal Stud 1996;41:405–411. Makar RS, Toth TL. The evaluation of infertility. Am J Clin Pathol 2002;117(Suppl 1):95–103. Sallam HN, Sallam AN, Ezzelden FE, et al. Minimal requirements for a successful outcome in anovulatory patients treated with human menopausal gonadotropins. Int J Fertil Womens Med 2000;45:285–291. Oei SG, Helmerhorst FM, Keirse MJN. Routine postcoital testing is unnecessary. Hum Reprod 2001;16:1051–1053. Fuller CE, Threatte GA, Henry JB. Basic examination of urine. In: Henry JB, ed. Clinical Diagnosis and Management by Laboratory Methods. Philadelphia: WB Saunders Co; 2001:367–402. Arant BS Jr. Screening for urinary abnormalities: worth doing and worth doing well. Lancet 1998;351:307–308. Liao XC, Churchill BM. Pediatric urine testing. Ped Clin N Am 2001;48:1425–1440. Eftychiades AC. Diseases in the Byzantine world with special emphasis on the nephropathies. Am J Nephrol 1997;17:217–221. Kary M, Maife SO, eds. Kidney and Urinary Tract Infections. Indianapolis, IN: Eli Lilly & Co; 1971:28–29. Sauter C. Grüner urin. Schweiz Med Wochenschr 1998;128:2003. Carpenito G, Kurtz I. Green urine in a critically ill patient. Am J Kid Dis 2002;39:E20. Fogazzi GB, Cameron JS, Ritz E, et al. The history of urinary microscopy to the end of the 19th century. Am J Nephrol 1994;14:452–457. Fogazzi GB, Cameron JS. Urinary microscopy from the seventeenth century to present day. Kid Int 1996;50:1058–1068. National Kidney Foundation. K/DOQI practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kid Dis 2002(Suppl 1);39:S1–266. Sutton JM. Urinary eosinophils. Arch Intern Med 1986;146:2243–2244. Kierkegaard H, Feldt-Rasmussen U, Hoerder M, et al. Falsely negative urinary leukocyte counts due to delayed examination. Scand J Clin Lab Invest 1980;40:259–261. Howanitz PJ, Saladino AJ, Dale JC. Timeliness of urinalysis. A College of American Pathologists Q-Probe study of 346 small hospitals. Arch Pathol Lab Med 1997;121:667–672. Kouri T, Vuotari L, Pohjavaara S, et al. Preservation of urine for flow cytometric and visual microscopic testing. Clin Chem 2002;48:900–905. del Rosario RMM, Rodriguez MI, Leon MT, et al. A new chemical preservative that permits analysis of urine sediment for light microscopic examination 12h after emission. Nephron 1999;82:65–71. Kim Y, Jin DC, Lee G, et al. Quantitative analysis of urine sediment using newly designed centrifuge tubes. Ann Clin Lab Sci 2002;32:55–60. Okada H, Sakai Y, Kawabata G, et al. Automated urinalysis. Evaluation of the Sysmex UF-50. Am J Clin Pathol 2001;115:605–610. Point of Care, vol. 2, no. 1 43. Lin D-S, Huang F-Y, Chiu N-C, et al. Comparison of hemocytometer leukocyte counts and standard urinalyses for predicting urinary tract infections in febrile infants. Ped inf Dis J 2000;19:223–227. 44. Maslamani S, Glenton PA, Khan SR. Changes in urine macromolecular composition during processing. Urol 2000;164:230–236. 45. Flach SD, Wigton RS, Longenecker JC, et al. How physicians diagnose urinary tract infections: the potential influence of laboratory regulations on test availability and use. J Famil Pract 2001;50:613. 46. Cembrowski GS, Strauss S, Werner JR, et al. Effect of CLIA’88 on Minnesota physician’s office laboratories. JAMA 1995;273:524. 47. Strauss S, Cembrowski GS, Adlis SA. CLIA’s effect on POLs (physicians’ office laboratories). Med Lab Observer 1995;27:34–38. 48. American Academy of Pediatrics, Committee on Quality Improvement. Practice parameter: the diagnosis, treatment and evaluation of the initial urinary tract infection in febrile infants and young children. Pediatrics 1999;103:843–852. 49. Armengol CE, Hendley JD, Schlager TA. Should we abandon standard microscopy when screening for urinary tract infections in young children? Ped Inf Dis J 2001;20:1176–1177. 50. Nickel JC. Practical approach to the management of prostatitis. Tech Urol 1995;1:162–167. 51. Dinsmore WW, McBride M, Alderdice D. An audit of the ‘two-glass’ test for urethritis. Intl J STD AIDS 2000;11:607–608. 52. Chandeying V, Skov S, Tabrizi SN, et al. Can a two-glass urine test or leukocyte esterase test of first-void urine improve syndromic management of male urethritis in Southern Thailand? Intl J STD AIDS 2000;11:235–240. 53. Drake BJ. Urine-sampling apparatus for the “two-glass” test in the recognition of urethritis in women. Brit J Veneral Dis 1968;44:251–253. 54. Craig RM. Alimentary tract and exocrine pancreas. In: Noe DA, Rock RC, eds. Laboratory Medicine. The Selection and Interpretation of Clinical Laboratory Studies. Baltimore: Williams & Wilkins; 1994:383–400. 55. Harrie JC, Dupont HL, Hornick RB. Fecal leukocytes in diarrhea illness. Ann Intern Med 1972;76:697–703. 56. Nordlander E, Phuphaisans S, Bodhidatta L. Microscopic examination of stools and latex slide agglutination test for rapid identification of bacterial enteric infections in Khmer children. Diag Microbiol Inf Dis 1990;13:273–276. 57. Ruiz-Pelaez JG, Mattar S. Accuracy of fecal lactoferrin and other stool tests for diagnosis of invasive diarrhea at a Colombian pediatric hospital. Ped Inf Dis J 1999;18:342–346. 58. Bustos D, Greco G, Yapur V, et al. Quantification of fecal neutrophils by MPO determination (myeloperoxidase) in patients with invasive diarrhea. Acta Gastroenterol Latinoamericana 2000;30:85–87. 59. Korzeniowski OM, Barada FA, Rouse JD, et al. Value of examination for fecal leukocytes in the early diagnosis of shigellosis. Am J Trop Med Hygiene 1979;28:1031–1035. 60. Gupta DN, Saha DR, Sengupta PG, et al. Value of fecal leucocyte count as an indicator of invasiveness in mucoid diarrhea. J Communicable Dis 1997;29:329–332. 61. Ahmed GO, Aldel HOM, Ayoub NM, et al. Cambylobacter Provider-Performed Microscopy 31 81. jejuni in acute diarrhea in infancy and its relation to fecal leucocytic count. J Egypt Public Health Assoc 1992;67:13–25. Jendal N, Arora S. Role of fecal leucocytes in the diagnostic evaluation of acute diarrhea. Ind J Med Sci 1991;45:261–264. Cimolai N. Fecal leukocytes in Escherichia coli 0157: H7 enteritis. J Clin Pathol 1990;43:347. Lawson JM, Wolosin J, Mottet MD, et al. Collagenous colitis: an association with fecal leucocytes. J Clin Gastroenterol 1988;10:672–675. Sinton E. Seminal fluid. In: Kjeldsberg CR, Knight JA, eds. Body Fluids. Laboratory Examination of Amniotic, Cerebrospinal, Seminal, Serous and Synovial Fluids. Chicago: American Society of Clinical Pathologists; 1993:255–264. Gonzales GF. Function of seminal vesicles and their role on male fertility. Asian J Androl 2001;3:251–258. Oehninger S. Clinical and laboratory management of male infertility: an opinion on its current status. J Androl 2000;21:814–821. Collins KA. The laboratory’s role in detecting sexual assault. Lab Med 1998;29:361–365. Elder K, Dale B. Semen analysis and preparation for assisted reproductive techniques. In: In Vitro Fertilization. Cambridge, UK: Cambridge University Press; 2000:130–151. Bonde JPE, Ernst E, Jensen TK, et al. Relation between semen quality and fertility: a population-based study of 430 first-pregnancy planners. Lancet 1998;352:1172–1177. Graham JK. Assessment of sperm quality: a flow cytometric approach. Animal Reprod Sci 2001;68:239–247. Primakoff P, Myles DG. Penetration adhesion and fusion in mammalian sperm-egg interaction. Science 2002;296:2183– 2185. Ho HC, Squarez SS. Hyperactivation of mammalian spermatozoa: function and regulation. Reprod 2001;122:519–526. Ren D, Navarro B, Perez G, et al. A sperm ion channel required for sperm motility and male fertility. Nature 2001;413:603–609. Sassone-Corsi P. Unique chromatin remodeling and transcriptional regulation in spermatogenesis. Science 2002;296:2176–2178. Mackay IS, Durham SR. ABC of allergies: perennial rhinitis. Brit Med J 1998;316:917–920. Jirapongsananuruk O, Vichyanond P. Nasal cytology in the diagnosis of allergic rhinitis in children. Ann Allergy Asthma Immunol 1998;80:165–170. Okano M, Nishizaki K, Nakada M, et al. Prevalence and prediction of allergic rhinitis using questionnaire and nasal smear examination in school children. Acta Oto-Laryngol 1999;540(Suppl):58–63. Raulf-Heimsoth M, Wirtz C, Papenfuss F, et al. Nasal lavage mediator profile and cellular composition of nasal brushing material during latex challenge tests. Clin Exptl Allergy 2000;30:110–121. Jankowski R, Persoons M, Foliguet B, et al. Eosinophil count in nasal secretions of subjects with and without nasal symptoms. Rhinol 2000;38:23–32. Erjefalt JS, Greiff L, Andersson M, et al. Degranulation patterns 32 F. L. Kiechle et al 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. of eosinophil granulocytes as determinants of eosinophil driven disease. Thorax 2001;56:341–344. 82. Lipworth BJ, White PS. Allergic inflammation in the unified airway: start with the nose. Thorax 2000;55:878–881. 83. Kang BH, Chen SS, Jou LS, et al. Immunolocalization and 3-nitrotyrosine in nasal mucosa of patients with rhinitis. Eur Arch Oto-Rhino-Laryngol 2000;257:242–246. 84. Takeno S, Osada R, Furukido K, et al. Increased nitric oxide production in nasal epithelial cells from allergic patients – RT-PCR analysis and direct imaging by a fluorescence indicator: DAF-2DA. Clin Exptl Allergy 2001;31:881–888. 85. Nakamura Y, Christodoulopoulos P, Cameron L, et al. Upregulation of the transcription factor GATA-3 in upper airway mucosa after in vivo and in vitro allergen challenge. J Allergy Clin Immunol 2000;105:1146–1152. 86. Sapci T, Gurdal C, Onmus H, et al. Diagnostic significance of impression cytology in allergic rhinoconjunctivitis. Am J Rhinol 1999;13:31–35. 87. Kiechle FL. Personnel diversification. In: Kiechle FL, Main RI, eds. The Hitchhiker’s Guide to Improving Efficiency in the Clinical Laboratory. Washington, DC: AACC Press; 2002:82–91. 88. DeHoyos DR, Dolega R, Kiechle F, et al. Provider-performed microscopy (PPM) testing. Point Care 2002;1:37–38. 89. DeHoyos DR, Mann P, Okorodudu AO, et al. Development of a web site for a decentralized point-of-care testing program. Point Care 2002;1:63–70. 90. Phillips DP, Bredder CC. Morbidity and mortality from medical errors: an increasingly serious public health problem. Ann Rev Public Health 2002;23:135–150. 91. Kerr S, Marshall C, Sinclair D. Emergency physicians versus laboratory technicians: are the urinalysis and microscopy results comparable? A pilot study. J Emerg Med 1999;17:399–404. 92. Hyduke R. Resources for microscopic evaluation of urine. Lab Med 2001;32:25. 93. Ringsrud KM. Cells in the urine sediment. Lab Med 2001;32:153–155. 94. Kaplan KJ, Smirniotopoulos JG, Irvine H, et al. Med Pix: the internet teaching file for the health sciences. Arch Pathol Lab Med 2002;126:796. 95. Blake DR, Duggan A, Joffe A. Use of spun urine to enhance detection of Trichomonas vaginalis in adolescent women. Arch Pediatr Adolesc Med 1999;153:1222–1226. 96. Collins RD. Algorithmic Selection and Interpretation of Diagnostic Tests. Baltimore: Williams & Wilkins; 1998. 97. Speicher CE. The Right Test. A Physician’s Guide to Laboratory Medicine. Philadelphia: WB Saunders Co; 1998. 98. Leape LL, Berwick DM, Bates DW. What practices will most improve safety? Evidence-based medicine meets patient safety. JAMA 2002;288:501–507. 99. Shojania KG, Duncan BW, McDonald KM, et al. Safe but sound. Patient safety meets evidence-based medicine. JAMA 2002;288:508–513. 100. Kiechle FL. The impact of continuous glucose monitoring on hospital point-of-care testing programs. Diabetes Technol Therap 2001;3:647–650. 101. Winkelman JW, Tanasijevic MJ. Noninvasive testing in the clinical laboratory. Clin Lab Med 2002;22:547–558. Point of Care, vol. 2, no. 1