COA July 2013 Meeting Agenda
advertisement

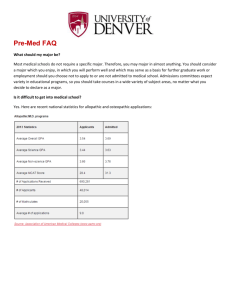
Group on Student Affairs-Committee on Admissions (GSA-COA) AAMC Headquarters, Washington D.C. Tuesday, July 9, 2013 – 5:00 pm to 7:00 pm EST Wednesday, July 10, 2013 – 8:30 am to 3:00 pm EST AGENDA Tuesday July 9, 2013 5:00 pm – 5:15pm GSA-COA Welcome and Introductions Robert Larkin, • Approval of January 2013 minutes • Welcome Claire Sadler 5:15 pm – 6:00pm GSA Regional and Section Reports Refer to written reports on regional/section issues and concerns that relate to admissions. Oral reports should briefly highlight these issues. • Central GSA …………………………....Adrian Jones, J.D. • Northeast GSA ………………………....Maria Demmler, MGPGP • Southern GSA ………………………….Robert E. Larkin • Western GSA …………………………..Carolyn Kelly, M.D. • CODA………………… ……………….Michelle E. Jacobs, M.D. • OSR ……………………………………Claire Sadler • NAAHP ………………………………..Julie Chanatry, Ph.D. 6:00 pm – 7:00pm Admissions Traffic Rules • Maria Demmler 7:15 pm Group dinner • FireFly/Sea Catch/On your own 7/5/2013 JF Wednesday July 10, 2013 7:30 am Breakfast available 8:00 am – 9:00 am Joint Committee Breakfast SAP Updates • Geoffrey H. Young, Ph.D., AAMC Staff • N130 9:00 am – 9:30 am AMCAS Update • 9:30 am – 10:00 am Kelly Begatto, AAMC Staff Holistic Review • S. Elizabeth White, AAMC Staff • Amy Addams, AAMC Staff • Henry Sondheimer, M.D., AAMC Staff 10:00 am – 10:15 am Break 10:15 am – 11:30 am MCAT Update • Karen Mitchell, Ph.D., AAMC Staff • Scott Oppler, AAMC Staff • Cynthia Searcy, Ph.D., AAMC Staff • Rebecca Rice, AAMC Staff 11:30am – 12:00 pm Guidelines for Shadowing • Geoffrey H. Young, Ph.D., AAMC Staff 12:00 pm – 1:00 pm Lunch Break 1:00 pm – 1:30 pm Admissions Initiative • Dana Dunleavy, AAMC Staff • Stephen Fitzpatrick, AAMC Staff • Tom Geiger, AAMC Staff 1:30 pm – 2:15 pm Fisher v. University of Texas at Austin Update • Frank Trinity, J.D., AAMC Staff 2:15 pm – 2:30 pm Break 2:30 pm – 3:00 pm COA Hot Topics Parking Lot • Robert Larkin 3:00 pm Adjourn 2 Adrian Jones CGSA Regional Report Updates CGSA Regional Conference was held in St. Louis, MO April 4-7, 2013. We had a few sessions dealing with admissions issues. The great folks from AAMC did a wonderful workshop on new initiatives. We are busy preparing for next years joint conference in San Diego. Geoff and I, also did a workshop on Competencies vs Pre-Requisites trying to clarify some of the confusion many people, including myself were struggling with trying to understand the new changes. We got some very good feedback and I think it was helpful for schools to start talking the discussion about how these are distinct topics. I have had several requests from peers who wanted to know how our admissions office runs, the old adage “you see one admissions office, you’ve seen one admissions office”. Some have asked if there could be a session at the National conference that talks about “How do you run an admissions office?” This would include everything from processing, screening, interviewing, COA committee make up, technical standards, etc. Early Assurance Programs – One of our constituents has a big concern with Early Assurance programs and the possible level of unfair influence they have over students. If a student is accepted to an early assurance program, this limits their options later if they decide to apply or want to apply to another school, thereby creating a level of undue influence over the student. I was just wandering if anyone else had this impression and what information could I pass on to my colleague. AAMC GSA Committee on Admissions Teleconference Southern Region July 1, 2013 REL Larkin, Admissions Director University of Central Florida College of Medicine 2013 SGSA/SGEA/SOSR Regional Meeting April 18-21 This meeting took place at the Marriott in Savannah, Georgia. The schedule for this meeting did not allow for an admissions session to discuss the traffic rules. Major changes were briefly presented at the SGSA business meeting to all attendees. After the meeting an email including the proposed changes was sent to SGSA admissions officers soliciting feedback. That feedback was discussed and included in subsequent COA discussions. AAMC/COA – Monthly Admissions Teleconference: January-June, 2013 These teleconferences were used for COA business. Discussions primarily focused on changes to the Admissions Traffic Rules proposals as well as provide feedback on a letter regarding applicant shadowing guidelines in tandem with NAAHP representatives. State MD Admissions/Pre-Health Advisors Meeting, February 8, 2013 The 8th annual meeting occurred at the University of Florida at the college of medicine. This meeting was the largest with the state’s nine physician programs and over 80 pre-health advisors from most of the 4-year programs and community colleges in the state. New M.D. Program Accreditation Update Full Accreditation Achieved: Florida International University and the University of Central Florida. Provisional Accreditation Achieved: Florida Atlantic University AAMC GSA Committee on Admissions Western Region Report July 3, 2013 Carolyn Kelly, MD UCSD School of Medicine Comments from Western constituents: • Feedback on proposed changes in traffic rules was solicited from Western Region admissions representatives. Some feedback was obtained solely through electronic communications and phone calls; there was also a robust discussion of the topic at the WGSA business meeting at the WGSA/WGEA/WAAHP/WOSR meeting in May, 2013 at UC Irvine. • Additional discussion of the proposed changes in traffic rules was held at UC Office of the President meeting of Admissions Deans from the 9 California medical schools. • The majority of respondents were in favor of the proposed changes or neutral about them, in particular changing the “May 15th deadline” to April 30th or May 1st. There was strong objection to changing that date to April 15th. Some schools had concerned about the formatting of communicating between schools regarding “summer offers” and felt it may augment workload without improving process. • At the UCOP meeting, a school queried whether the rising number of applications/school is solely a function of increasing numbers of applicants, or also increasing numbers of applications/applicant. Many schools are experiencing cutbacks in staffing for their admissions operations. Most schools agreed that the review of 6000-8000 applications is becoming challenging, and can contribute to overreliance on academic metrics. The question was raised whether COA would consider discussing limiting the number of schools to which an applicant could apply. They recognized that AAMC/AMCAS likely has lots of data on the distribution of how many schools students currently apply to, and this proposal may be tempered by review of that data. Western regional initiatives: • 29th Annual Western Regional LMSA conference at UCSD, March 29-30th, 2013. UCSD had 550600 registrants for this meeting! Undergraduates, medical students, and residents from the Western region were in attendance at a two day meeting that covered many aspects of the pathway to medicine and careers in medicine. Pipeline programs and admissions offices were well represented both at tables as well as in didactic and small group sessions. Portions of the conference were broadly applicable to all applicant groups, while other sessions were more focused toward students from backgrounds underrepresented in medicine. To: Committee on Admissions Michelle Jacobs, MD Liaison to the Committee on Admissions Committee on Diversity Affairs Association of American Medical Colleges June, 2013 The Committee on Diversity Affairs has been working on the following initiatives 1. Diversity Affairs representatives handbook 2. Continuing to strengthen bonds with the National Association of Advisors in Health Professions 3. Working with Advisors at historically black colleges and universities as well as institutions with a large Hispanic/Latino student population to ensure they are aware of all the changes for MCAT 2015. Educating students about the new classes they need for the exam 4. Having liaisons have conference calls to increase communication. AAMC Organization of Student Representatives (OSR) Update – July 2013 Chair – Ronnie Zeidan, M.D., Department of Anesthesiology and Critical Care, Hospital of the University of Pennsylvania, Zeidan.ronnie@gmail.com On behalf of the OSR Administrative Board, I would like to thank you for making the 2013 AAMC-OSR regional meetings so meaningful and successful. A special thank you to all the regional chairs and regional delegates for all of the hard work that went into the planning of the meetings. OSR Ad Board Focus on Issues – The OSR Ad Board will continue to focus on a number of issues including but not limited to: the rapidly increasing debt of U.S. medical students, its effect on primary care, and the difficulty of increasing the number of underrepresented minorities entering the field of medicine; enhancing the OSR presence at the 141 AAMC member medical schools; providing additional resources to OSR representatives on student issues; opportunities for involvement in the legislative process at both the federal and state levels; curriculum; tools for the OSR to increase communication; and advocating for innovation in undergraduate medical education. Joining Forces – The AAMC-OSR is focusing efforts this year on Joining Forces, a national initiative to mobilize society to give opportunities and support to our service members and their families. We encourage all OSR reps to join the AAMC in this endeavor by designing and implementing Joining Forces projects at your local institutions to meet the unique needs of veterans’ health. OSR/GSA academic career advising initiative – The OSR Administrative Board and GSA Steering Committee launched a pilot initiative that matched OSR reps interested in a career in academic medicine with GSA reps from the western region who will provide advice and guidance regarding a career in academic medicine. There were five GSA and eight OSR applicants who were paired at the end of May. Pairs were matched based on identified career goals, mutual academic interests, and communication styles. All of the pairs were sent an introduction email with supporting documents, including a getting started guide with practical advice on how to make the most of the partnership. Students were encouraged to contact their GSA mentors. Participants will be sent monthly emails with topics for discussion or journal articles to help foster discussions. Student Debt – In 2010, the OSR Administrative Board developed a survey for OSR representatives in order to obtain an updated picture of medical student debt, as well as to discern how students are currently involved in the process of setting tuition, the origin of medical school funding sources, and what is being done at the university level to help alleviate and educate students about their escalating debt. Written by the OSR student affairs committee, “The High Price of a Dream Job” analyzes the findings of the survey. Legislative Affairs – The legislative affairs committee continues to produce bi-weekly health policy updates that are disseminated via the OSR listserve. In conjunction with the biweekly updates, the committee has started publishing articles on “often mentioned, but seldom understood” topics in legislative affairs. The first of these addresses Accountable Care Organizations. Updates and archived articles are available on the OSR web site. Communications – OSR Advice on Applying to Residency – The OSR Communications Committee utilized feedback from recently matched medical students to provide a comprehensive guide for applying to residency programs covering topics such as away rotations, residency applications and interviews, and saving money during the process. Student Affairs – Understanding the Role of Spirituality in Medicine – A Resource for Medical Students The OSR Committee on Student Affairs created this document as a guide for medical students in approaching topics of spirituality and religion with patients to provide high quality, holistic medical care. Additional Updates on the activities and projects of the OSR Administrative Board are available via the OSR web site: https://www.aamc.org/members/osr/updates/ The OSR Administrative Board will be met June 10-11, 2013 in Washington, DC. During this time, we continued planning the 2013 AAMC-OSR Annual Meeting in Philadelphia, developed goals and focus issues for 2013; and discussed future projects. Ultimately, our goal is to serve you. If you have questions or concerns, please contact me or a member of the OSR Administrative Board. We are eager to help you in any way we can. For additional information about the OSR, please contact the OSR Director, Ally Anderson aanderson@aamc.org or visit the OSR web site: https://www.aamc.org/members/osr/ REPORT FROM NAAHP Liaison to Group on Student Affairs Committee on Admissions (GSA-COA) July 1, 2013 Presented by Julie A. Chanatry, President National Association of Advisors for the Health Professions (NAAHP) NAAHP Advisory Council: NAAHP and its Advisor Council met in January 2013 for our annual Winter Retreat. Jody Frost and APTA graciously hosed the event at their headquarters in Alexandria, VA. Topics of conversation included development of a consistent policy on sponsorships for National and Regional meetings and development of a research committee. The NAAHP Strategic Plan was also a central topic of conversation and the AC representatives provided us with great insight and expertise. Nine of the eighteen members of the Advisory Council joined the NAAHP Board of Directors in San Francisco on Monday, June 24th. It was a productive meeting in which we reviewed aspects of the NAAHP strategic plan and we received some very valuable suggestions and guidance. Also discussed were the 2013 regional meetings and the upcoming National Meeting. JoAnn Yanez, from the Association of Accredited Naturopathic Medical College volunteered to serve as liaison to the 2014 National Program Chairs and the 2015 Regional Program Chairs. Geoffrey Young of the American Association of Medical Colleges volunteered to help JoAnn. Regional Meetings: Susan Maxwell and I represented NAAHP at the SAAHP and NEAAHP Regional Meetings. The SAAHP meeting was held from April 7-10 in Louisville, KY, and the NEAAHP (a joint meeting with NEGSA) was held on April 11-14 in Atlantic City, NJ. At those meetings I gave a short talk NAAHP which included who we are and a brief overview of our strategic plan. Chuck Hauck and Susan Maxwell represented NAAHP at the CAAHP that was held April 18-21, in Detroit, MI. Ruth Bingham and Cassie Flambouras represented NAAHP at the WAAHP (a joint meeting with WGSA) that was held May 3-7 in Irvine CA. Chuck and Ruth both gave a similar talk at their respective regional meetings. NAAHP Board of Directors Meeting: The NAAHP annual Board of Directors meeting was held June 22 – June 26, 2013 at the San Francisco Hilton. We had a productive meeting over four days in which we reviewed progress on our strategic plan and moved forward on several key issues. We have initiated two new committees – the Research Committee and the Grants Committee. We are filling those committee spots over the next few months. We have restructured the editorial review duties of Communications Committee. In addition, to the Director of and Assistant Director of Communications, we are creating two other Assistant Director positions to help more efficiently handle the increasing workload of the Communications Committee. Committee on Diversity and Inclusion: The CDI committee has been very active over the past year. Francisco Castelan, the committee chair, has been involved with the AAMC’s Tour for Diversity over the past year. Francisco and Michelle Klein, from Prince George’s Community College, recently represented NAAHP at the Maryland Department of Health and Mental Hygiene joint meeting with the AAMC in June 2013. The CDI requested that a representative from the committee be included in regional program planning committees or as a representative to regional boards so that there is increased and consistent communication between the national CDI and the regions. All of the regional presidents were in agreement with this and the regions either already have a representative to their regional board in place or are working on a structure that will facilitate consistent communication with the national CDI. As our new website comes online, the members of the CDI are going work closely with our Communications Committee to update and help maintain the diversity and inclusion resources on our website. In addition, members of the CDI are working closely with our Membership Committee to identify and reach out to advisors at MSI and to community colleges. NAAHP Strategic Plan: NAAHP continues to move forward with the strategic plan that was adopted at our June 2012 Board of Directors meeting. We continue to make progress in four key target areas: Governance, Membership, Professional Development and Technology. The NAAHP Board of Directors hired Lori Provost as a consultant to help with the implementation of the NAAHP Strategic Plan. Each Task Force worked with Lori to advance their objectives during 2012 – 2013. We have made significant progress on meeting our goals. The continuing work of the task forces will be transferred to each of the respective committees as we move into year two of our strategic plan. Professional Development: The Professional Development Task Force worked with the Communications Committee, Technology Committee and our National Office staff to create “Advisor Toolboxes” which are available on our current website. In collaboration with Jody Frost from APTA and using NAAHP's Best Practices document as the foundation, the Professional Development Task force drafted two documents on competencies for pre-health advising, one for institutions/programs and one for pre-health advisors. These documents were reviewed and approved by the NAAHP Board of Directors at our June meeting. The Professional Development and Leadership Committee will now finalize the documents and will distribute them for feedback throughout the regions. The competencies will also be a focus of the PD&L pre-conference workshop at the 2014 NAAHP National Conference. The goal is to use the competencies as the foundation for a certification process. Membership: As part of the strategic plan, the Membership Task Force has articulated several goals aimed at increasing recruitment and retention of members. The Task Force has been working with the National Office manager and medial specialist to advertise the benefits of membership. The Membership Task Force has recently sent out a survey to our members and the results were shared with Board and our Advisory Council at our June meeting. In addition, the Membership, Technology and Professional Development and Leadership Committees are exploring areas that will increase member benefits. To date, the membership stands at 1244 members. Governance Committee: The NAAHP Board of Directors approved an updated Employee Handbook and Performance Review procedure at our meeting in June. The new review process will be implemented over the summer. The initial chapters of a Board of Directors Orientation Manual was produced with the help of Lori Provost, our consultant, and was distributed to incoming Board members. This manual will be expanded over the course of this year. The Governance Committee continues to work to update other key documents. A review and update of our Policy and Procedure Manual is now underway. Technology (Publications/Website/Database): Our national publications such as the Advisor, the Health Professions Advisor’s Guide (HPAG) and related publications continue to do very well under the leadership of our Communications Director Carol Baffi-Dugan, with support from the NAAHP Communications Committee. We have rolled out new features on our website including an online archive of the Advisor and our “Toolboxes” as part of our strategic plan. We have hired a Media Specialist to work on our publications, website design and maintenance and increased use of social media. In addition, we have also hired student interns to help with the overload of work in upgrading and maintaining our website. Our website is scheduled to be migrated to an updated platform over the summer. The migration is about 50% complete at this point. In conjunction with the migration of our website, we will be rolling out a new design for the website with more features for our advisor and patron members. The NAAHP Letters of Recommendation Task Force: The LOR Task Force is continuing to work with the AAMC Letters Working Group. Glenn Cummings of Franklin and Marshall and Jennifer Kimble of Georgia Institute of Technology are the NAAHP representatives to the AAMC Letters Working Group. NAAHP National Meeting: Planning is underway for the next NAAHP National Meeting to be held at the San Francisco Hilton from June 25-29, 2014. The conference rate at the hotel is $185.00 (single/double occupancy). Debrah Beck, University of North Texas and Suzette Combs, University of Cincinnati are the National Meeting Program Co-Chairs. See the NAAHP website www.naahp.org for more details. AAMC Advisory Committee on Holistic Review The Work Moving Forward Introduction The AAMC's mission reflects its commitment to support medical school efforts to educate a “culturally competent, diverse, and prepared health and biomedical workforce," which, in turn, will lead to "improved health and health equity” 1 throughout the United States. The work of the Advisory Committee on Holistic Review is focused on this vital goal. Educating a workforce that can and will meet the health care needs of all is inextricably dependent on the teaching and learning that is occurring - to enhance students' cultural competence and their ability to engage with others from different backgrounds, and improve their understanding of health issues of populations with which they may not be familiar. In its initial phase, this project focused explicitly on transforming admissions, identifying compositional diversity as an essential - and as yet unrealized - first step for moving toward the goal of enhanced teaching and learning to prepare a diverse workforce. The Project is now working with and through medical schools and other AAMC committees to build on that critical admissions work to transform the learning environment in order to maximize the benefits of diversity and inclusion for teaching, learning and optimal patient care. Vision A diverse physician workforce that achieves equitable, high quality healthcare for all. Mission Lead and support the U.S. academic medicine community to build and leverage learner diversity to realize their unique institutional missions. The Committee’s purpose is to focus on the constellation of issues associated with admitting and enhancing the education of a diverse student body. We aim to create synergy between the broad framework of holistic admissions 2, and the institutional policies and practices that sustain a learning and working environment in which members of our diverse communities are supported, empowered to share their talents, and expected to work collaboratively to achieve high quality, equitable care for all. 1 See AAMC’s Mission, Vision, and Strategy (May 31, 2013). A broad framework of holistic admissions includes a focus on pipeline, outreach, recruitment, admissions, financial aid, and other related practices. 2 June 12, 2013 Draft Advisory Committee on Holistic Review Charge The AAMC Advisory Committee on Holistic Review is charged with: • • Setting the strategic direction of the Project, aligned with the AAMC strategic priorities. Advancing the Project’s three priority areas (institutional alignment, inclusive learning environments, and leadership in the changing legal and policy environments) by: • Informing and engaging other stakeholders inside and outside the AAMC across the medical education continuum on priority issues and the development of strategies and tools; • Providing practical and adaptable institutional services and resources (ranging from broad strategic guidance to concrete policy, practice, and measurement tools) associated with Committee priorities; • Effectively leveraging the work of other AAMC Committees to ensure a full perspective on the range of access, diversity and inclusion, and cultural competency central to AAMC's leadership on these issues; and • Gathering and analyzing data to demonstrate both the Project’s and medical schools’ progress and outcomes, and to celebrate the innovative achievements of the medical schools. Key Terms Diversity - Diversity as a core value embodies inclusiveness, mutual respect, and multiple perspectives and serves as a catalyst for change resulting in health equity. In this context, we are mindful of all aspects of human differences such as socioeconomic status, race, ethnicity, language, nationality, sex, gender identity, sexual 3 orientation, religion, geography, disability and age. (For the purposes of this committee’s work, we recognize that diversity must be defined at the institutional level and should be explicitly connected to each institution’s mission and goals.) Inclusion - Inclusion is a core element for successfully achieving diversity. Inclusion is achieved by nurturing the climate and culture of the institution through professional development, education, policy, and practice. The objective is creating a climate that fosters belonging, respect, and value for all and encourages engagement and 4 connection throughout the institution and community. Institutional alignment involves coordination and alignment along a school's continuum of relevant practices to find synergies and efficiencies to enhance institutional effectiveness and success – and to do so in a cost-effective manner. This continuum reflects a focus on the distinct but overlapping enrollment actions—recruitment and outreach, admissions, financial aid, and retention—along with those associated with the student learning experience, with a range of issues such as pedagogy, curriculum, and climate. 3 4 AAMC Group on Diversity and Inclusion Ibid June 12, 2013 2010-13 HOLISTIC REVIEW ADMISSION WORKSHOP SCHOOL SITES CENTRAL REGION (18) Central Michigan (N) Chicago Medical School—Rosalind Franklin* Des Moines Univ. Coll. of Osteopathic Medicine Mayo Clinic College of Medicine Michigan State University CHM Northeast Ohio Medical School Oakland Beaumont School of Medicine (N) Ohio State University College of Medicine Rush Medical College University of Arkansas School of Medicine University of Chicago—Pritzker SOM University of Cincinnati SoM University of Kansas School of Medicine University of Minnesota School of Medicine University of Missouri—Columbia SoM University of Missouri—Kansas City SoM Wayne State University School of Medicine Western Michigan University School of Medicine (N) Type Public Private Public Private Public Public Private Public Private Public Private Public Public Public Public Public Public Public 2010 NORTHEAST REGION (13) Albany Medical College Albert Einstein College of Medicine Cooper Medical School of Rowan University (N) Dartmouth Medical School Frank Netter School of Medicine (N) Hofstra School of Medicine (N) New York University School of Medicine Pennsylvania State University COM University of Buffalo School of Medicine University of Buffalo School of Nursing University of Vermont College of Medicine University of Massachusetts Medical School UMDNJ School of Medicine Type Private Private Public Private Private Private Private Private Public Public Public Public Public 2010 SOUTHERN REGION (15) Eastern Virginia Medical School (N) Florida International University SoM (N) Georgia Health Sciences University—MCG Meharry Medical College* Mercer University School of Medicine Texas A&M College of Medicine University of Alabama-Birmingham SOM University of Florida College of Medicine Virginia Commonwealth Univ. School of Medicine Louisiana State University-Shreveport SOM University of Louisville School of Medicine University of Mississippi School of Medicine University of Texas-Houston School of Medicine Virginia Tech Carilion School of Medicine (N) West Virginia University School of Medicine Type Private Public Public Private Private Public Public Public Public Public Public Public Public Private Public 2010 Updated on 03/13/2013 2011 2012 2013 X X X X X X X X X X X X X X X X X X X 2011 2012 2013 X X X X X X X X X X X X X 2011 2012 2013 X X Primary contact(s) Joel Lanphear; Christopher Austin LaMont Vaughn Karen McLean; Karen Lewis Susan Romanski Joel Maurer Dr. Erik Porfelli; Luke Gloeckner Christina Grabowski Quinn Capers Cynthia Boyd; Jill Volk Linda Dupuy Sylvia Robertson Stephen Manuel Sandy McCurdy Theresa Baultrippe Rachel Brown Alice Arredondo Silas Norman Dr. Peter Ziemkowski Primary contact(s) Henry Pohl Noreen Kerrigan John McGeehan Ann Davis Michael Ellison Rona Woldenberg Rafael Rivera, Jr. Dwight Davis Ms. Donna Lariviere Dr. Carol Brewer Janice Gallant Mariann Manno George Heinrich; Mercedes Rivero Primary contact(s) Dr. Don Meyer Barbara Roller; Andria Garcia X X Kathleen Martin X X X X X X X X X X X Angelo Lee Alice House Filo Maldenado Nathan Smith Leila Amiri Dr. Michelle Whitehurst-Cook Scott Kennedy Pamela Osborne Steve Case LaTanya Love Stephen Workman Dr. Hannah Hazard WESTERN REGION (7) University of Arizona-Phoenix SoM (N) University of Arizona-Tucson SoM University of California-Davis School of Medicine University of Nevada School of Medicine University of New Mexico School of Medicine University of Utah School of Medicine University of Washington School of Medicine Type Public Public Public Public Public Public Public 2010 2011 2012 2013 X X X X X X X Primary contact(s) Tara Cunningham Lori Alvorad Mark Henderson; Frank Sousa Peggy Dupey; Kristine Nelson Marlene Ballejos Benjamin Chan Carol Teitz 53 workshops to date / 51 MD-granting schools (9 new schools) / 1 DO-granting school / 1 School of Nursing Updated on 03/13/2013 AM Last Page AM Last Page: The MCAT Exam: Comparing the 1991 and 2015 Exams Marc Kroopnick, MEng, PhD, Manager, MCAT2015 Development and Psychometrics, Association of American Medical Colleges (AAMC) In the spring of 2015, potential physicians will take the MCAT2015 exam, the newest version of the MCAT exam. The MR5 Committee (the advisory committee for the MCAT2015 exam) redesigned the exam to test the academic competencies* that tomorrow’s physicians will need to know to succeed in medical school. The design is based on survey responses from over 2,700 medical school and baccalaureate faculty members and feedback from expert panelists and participants in over 90 outreach events. The MCAT2015 exam will, like the current exam (the MCAT1991 exam, introduced in 1991), test concepts in the natural sciences, as well as skills in critical analysis and reasoning. Unlike the MCAT1991 exam, the MCAT2015 exam will also cover concepts from the behavioral and social sciences. The table below highlights the features the MCAT2015 exam shares with the MCAT1991 exam, as well as its new features. How Are the MCAT1991 and MCAT2015 Exams the Same? What’s Different on the MCAT2015 Exam? Content • Concepts from biology, general chemistry, organic chemistry, and physics that are rated as important for success in medical school are tested; in fact, approximately 75% of questions on the MCAT2015 exam test concepts that also appear on the MCAT1991 exam. • Questions require examinees to demonstrate their scientific reasoning and problem-solving skills. • Two test sections focus on natural sciences concepts. Natural Sciences • Biochemistry concepts that are rated as important for success in medical school are tested. • Questions test scientific competencies* by asking examinees to solve problems about biological and living systems and to integrate concepts from multiple disciplines. • Questions require examinees to use research methods and statistical skills to solve problems in the same ways that natural scientists do. Behavioral and Social Sciences • Concepts from psychology and sociology (along with related biology concepts) that provide the foundation for learning about the behavioral and sociocultural determinants of health and health outcomes are tested. • Questions test scientific competencies* by asking examinees to integrate knowledge from different disciplines (just like in the natural sciences sections). • Questions require examinees to demonstrate scientific reasoning and problem-solving skills and to use research methods and statistical skills in the same ways that social and behavioral scientists do. Critical Analysis and Reasoning Skills • Passages from the social sciences and humanities that emphasize cultural studies, population health, ethics, and philosophy are included. • No natural sciences and technology passages are included. • Questions test examinees’ analysis and reasoning skills using the most current science on cognitive processing. • This is a brand new test section. • No specific content knowledge is needed to do well on this section. • Passages include content from the social sciences and humanities. • Questions require examinees to demonstrate a variety of analytical and reasoning skills (i.e., cognitive-processing skills). Writing Skills • This section has been eliminated. Test Administration and Score Reporting • Multiple-choice questions are predominantly prompted by passages and, in some cases, graphs, tables, or charts. • Section scores and an aggregate total score are reported to examinees and medical schools. • A computer-based testing format that has proven effective is used. • Individual test sections include more questions than on the MCAT1991 exam; accordingly, the test day is longer by approximately two hours. • Reliable comparisons of section scores for different examinees are made possible by the greater number of test questions. *The natural sciences competencies tested on the MCAT 2015 exam align with the competencies described by the AAMC-sponsored Scientific Foundations for Future Physicians Committee. The behavioral and social sciences competencies tested on the MCAT 2015 exam build on the competencies that are described in the Institute of Medicine’s report, Improving Medical Education: Enhancing the Behavioral and Social Content of Medical School Curricula (National Academies Press; 2004; edited by Patricia A. Cuff and Neal Vanselow), and promulgated by the AAMC-sponsored Behavioral and Social Science Foundations for Future Physicians Committee. Acknowledgments: The author would like to thank the following AAMC personnel for reviewing earlier drafts of this Last Page: Karen Mitchell and Cynthia Searcy. Author contact: mkroopnick@aamc.org Academic Medicine, Vol. 88, No. 5 / May 2013 737 MCAT® Update We are pleased to provide an update of key milestones for the current exam, as well as progress we are making toward the new MCAT2015 exam that will begin in Spring 2015. To keep admissions officers and advisors updated on all things related to the new MCAT exam, we have launched the new quarterly eNewsletter – MCAT2015 Q-UPP: A Quarterly Update of Progress and Projections for the MCAT2015 Exam. The second issue of the newsletter is available in print format in these materials. As always, we welcome your comments, suggestions and questions. You can reach us via e-mail at rrice@aamc.org. 2012 Testing Year • 78,542 individuals took the MCAT exam in 2012. • The scaled score tables and percentiles for these examinees appear online at www.aamc.org/students/applying/mcat/admissionsadvi sors/. 2013 Testing Year • The Writing Sample section was removed from the 2013 exam to make room for a Trial Section that tests out questions for the 2015 exam. Through the May 23 administration, the opt in rate for the Trial Section is averaging 72.5%. Of those who opt in, an average of 87.1% are making a good faith effort based on the established set of metrics. Information about how examinees can volunteer for this section and what they get in return is available online. www.aamc.org/mcat/volunteer • A new tool that students with disabilities can use to submit applications for testing accommodations was launched this Spring. Information about the new MCAT Accommodations Online system is available at www.aamc.org/students/applying/mcat/accommodatio ns/. • An informational webinar for advisors about the 2013 exam is posted online at www.aamc.org/students/applying/mcat/admissionsadvi sors/ . MCAT Preparation Products • The Official MCAT® Self-Assessment Package is now available at no cost to examinees who qualify for AAMC’s Fee Assistance Program (FAP). Other FAP benefits include reduced test administration fees, reduced application fees, free copies of the Official Guide to the MCAT Exam and Medical School Admissions Requirements book, and scholarships for evaluations for examinees with documented disabilities who need updated evaluations. For more information about the Fee Assistance Program, please visit www.aamc.org/fap. • An informational webinar for advisors about The Official MCAT® Self-Assessment Package is posted online at www.aamc.org/students/applying/mcat/admissionsadvi sors/. • The Official Guide to the MCAT® Exam, Third Edition was published in January 2013. MCAT2015 Resources and Planning Efforts • The second edition of the Preview Guide for the MCAT2015 Exam is posted online at www.aamc.org/mcat2015/admins. A screen-reader accessible version is also available. • Presentation slides and speaker notes are available online for presentations about MCAT2015 to prospective examinees. Slides and notes are also available for advisor and faculty audiences. Both sets of slides and notes are at www.aamc.org/mcat2015/admins. • Winners of the first call for submissions for the Prehealth Collection within MedEdPORTAL’s iCollaborative were announced this Spring. www.mededportal.org/icollaborative/pre-health • The Course-Mapping Tool for the MCAT2015 Exam, along with an instructional video on how to use the tool is available online at www.aamc.org/mcat2015/admins. • An article titled “Helping Students Prepare for the MCAT2015 Exam: Competencies and Courses” was published in the March 2013 issue of The Advisor. • A “decision tree” was developed to help students decide which MCAT exam they should take, based on when they want to start medical school and when they will be ready to test. The graphic, along with important factors to consider when deciding which exam to take, can be found online at: www.aamc.org/mcat/whichexam Continued on reverse side © 2013 The Association of American Medical Colleges MCAT® is a program of the Association of American Medical Colleges and related trademarks owned by the Association include Medical College Admission Test, MCAT and MCAT2015. • • • • The May issue of Academic Medicine focused on preparation for medical school, with articles on the current and 2015 exam, and the application process. The issue included a chart, The MCAT Exam: Comparing the 1991 and the 2015 Exams, which outlines what is the same and what is new. http://journals.lww.com/academicmedicine/toc/2013/0 5000#-577578117 On April 2, AAMC announced a new collaboration with Khan Academy and The Robert Wood Johnson Foundation. The Khan Academy contest was launched to produce the best pre-health video lessons and accompanying questions for content on the MCAT2015 exam. The submission deadline was June 14 and over 65 submissions were received. The judges are now reviewing the videos and will announce the winners of the contest in July. www.khanacademy.org/about/med-competition The American Association of Colleges and Universities’ Peer Review journal published a topical issue called: Essential Learning Outcomes, the New MCAT and Curricular Change. It appears online at www.aacu.org/peerreview/pr-fa12/Editor.cfm. We have a new resource available on our website for students, advisors and undergraduate faculty. Our Sociology & Psychology Textbook Resource Worksheet outlines the concepts that will be tested by the new MCAT exam and where publishers have indicated this information is covered in their introductory textbooks. We have four textbooks on the worksheet so far, and will be following up with additional publishers to include more textbooks in the future. Access the worksheet at: https://www.aamc.org/students/download/346368/dat a/sociologyandpsychologytextbook.pdf Resources for admissions officers and pre-health advisors: Current MCAT Exam: www.aamc.org/mcat MCAT2015 Exam: www.aamc.org/mcat2015/admins © 2013 The Association of American Medical Colleges MCAT® is a program of the Association of American Medical Colleges and related trademarks owned by the Association include Medical College Admission Test, MCAT and MCAT2015. Update on MCAT2015 Validity Research: The Psychological, Social, and Biological Foundations of Behavior (PSBB) Validity Research Study Purpose The MCAT research team launched its first study to examine the predictive validity of the 2015 MCAT exam. The purpose of this project is collect empirical data to support the use of MCAT2015 PSBB scores in medical school admissions in 2016. Medical schools participating in the study will administer the PSBB test to currently-enrolled medical students, and PSBB scores will be used to predict students’ performance in courses and clerkships with behavioral and social sciences (BSS) content (e.g., grades in BSS courses, clerkship ratings in psychiatry rotations, etc.). Who’s Participating? The AAMC is partnering with 11 medical schools to conduct this research. Participating Schools Boston University School of Medicine Columbia University College of Physicians and Surgeons Memorial University of Newfoundland Faculty of Medicine Stanford University School of Medicine University of California, San Francisco, School of Medicine University of Central Florida College of Medicine University of Illinois College of Medicine University of Mississippi School of Medicine University of North Carolina at Chapel Hill School of Medicine University of Texas Medical School at Houston University of Texas School of Medicine at San Antonio Update on Progress Participating schools held their first meeting on June 11 and 12. At the meeting they talked about IRB and FERPA issues, research design, procedures for administering the PSBB test and collecting outcome data, and plans for disseminating the results. Progress on each of the study tasks is described on page 2. © 2013 The Association of American Medical Colleges MCAT® is a program of the Association of American Medical Colleges and related trademarks owned by the Association include Medical College Admission Test, MCAT and MCAT2015. Phase 1: Create the project infrastructure. AAMC received initial IRB approval for the study; the IRB plan also addresses FERPA issues. It will be submitting amendments for approval the week of June 24 based on feedback from schools. Our goal is to receive final approval early in July. AAMC is working with its IT department to determine the requirements for exchanging data securely and for protecting the confidentiality of student data collected for this research. The system design will begin in July so that it is ready for the first wave of data, scheduled for receipt August 2013. Phase 2: Design the research protocol. AAMC conducted a kickoff meeting June 11-12 with participating schools to discuss the study design and which courses, what kinds of grades, and which student samples are most appropriate for the study. Phase 3: Administer prototype MCAT2015 PSBB form. AAMC assembled a prototype PSBB test form that will be administered it via proctored Internet administration. We’ll be testing the delivery system midJuly 2013. Schools will administer the test in early August. Participating students will receive $75, a score report, and a thank you letter from Dr. Kirch. Phase 4: Collect outcome data. At the kickoff meeting, schools identified courses that emphasize or rely on behavioral and social sciences knowledge (e.g., Brain and Behavior, Public Health, Psychiatry clerkships) Schools also discussed what measures of performance (e.g., grades, test scores, clerkship ratings) will be best for this study. We’ll be finalizing these decisions in July 2013. Data collection and exchange will occur between September 2013 and January 2015. Phase 5: Analyze data. AAMC will conduct analyses throughout the project, finishing in early Spring 2015. We plan to form a working group with 3 to 4 participating schools to develop prototype validity reports for each school. We’ve enlisted the support of a testing expert who provides technical guidance to the College Board for its validity studies service to help us think through the analyses. The participating schools are already being asked to give presentations about the study. We’ll be working on easy-todigest materials about the study and will collaborate with the participating schools on all outreach materials. © 2013 The Association of American Medical Colleges MCAT® is a program of the Association of American Medical Colleges and related trademarks owned by the Association include Medical College Admission Test, MCAT and MCAT2015. The group will develop recommendations for admissions officers on the kinds of outcomes that PSBB scores predict, based on the results of the study and their observations along the way. These recommendations and the validity results will be shared with admissions officers before the start of the 2016 application cycle. © 2013 The Association of American Medical Colleges MCAT® is a program of the Association of American Medical Colleges and related trademarks owned by the Association include Medical College Admission Test, MCAT and MCAT2015. TABLE OF CONTENTS INTRODUCTION ............................................................................................................................. 1 Learning objectives for the pre-medical student ...................................................................................................... 1 Pre-medical student responsibilities .............................................................................................................................. 2 Physician—pre-medical student agreement .............................................................................................................. 2 RESOURCES .................................................................................................................................... Code of Conduct for Pre-medical Students Participating in Shadowing ................ Appendix A Confidentiality and Privacy of Patient Information ................................................ Appendix B Guidelines for Clinical Shadowing Experiences for Pre-medical Students Learning what it means to be a physician is essential for college students considering a career in medicine. Participation in a variety of activities that provide exposure to diverse health care settings can help achieve this goal. These activities allow students to gauge and affirm their interest in medicine as a career. Shadowing is different from volunteering; volunteering enables a pre-medical student the unpaid opportunity to help in a healthcare setting. Depending on the clinical environment, volunteering might include filing paperwork, answering phones, reading a book or playing a game with a child. Shadowing experiences, however, are observational in nature. The pre-medical student observes as the healthcare professional provides care to patients. This may occur in varied clinical settings including hospitals, outpatient clinics, long term care facilities and/or private practice. Observation always occurs under the appropriate supervision of a licensed physician or other licensed health care professional. A shadowing experience not only provides an introduction to the profession of medicine and the day-today responsibilities of the health care provider, but it also offers the physician and/or other health care provider the opportunity to model professionalism as well as ethical and culturally sensitive treatment of patients. Critical to the experience is the awareness and education of both the pre-medical student and the patient regarding the importance of the patient’s rights, privacy and confidentiality Since the primary purpose of shadowing is observation, the experience should focus on watching the physician as s/he performs his or her duties. The pre-medical student should never engage in any activity that is considered the practice of medicine. These activities include, but are not limited to: diagnosing diseases, administering medications, performing surgical procedures, suturing or other tasks generally reserved for the trained health professional. The following learning objectives serve as guidelines for the pre-medical shadowing experience: Learning objectives for the pre-medical student: • Determine the fit of the profession including aptitude, dedication, and attributes needed to pursue and practice medicine • Enhance knowledge of how the patient perspective impacts quality care • Better understand the roles of the health care team Pre-medical student responsibilities: • Provide proof of required immunizations or immunity (i.e., MMR, Varicella (or had chicken pox), Td, TB) prior to shadowing. • Complete HIPAA compliance training or review the training provided by the healthcare provider prior to shadowing experience. • Sign an agreement to adhere to a Code of Conduct (Appendix A). • Pre-medical student should sign an agreement of confidentiality (Appendix B) Physician – pre-medical student agreement: • Establish how pre-medical student will be introduced to patients • Establish a protocol as to how and when a patient is asked if the pre-medical student can observe the patient-physician interaction (e.g., informed verbal consent - patient is asked by medical staff during check in; patient’s response noted in medical record) Establish boundaries and expectations as to when a pre-medical student’s questions are to be asked and answered (e.g., between patients visits or at the end of a shadowing shift) Resources: http://www.hpplc.indiana.edu/ohp/clinicalobservation.shtml https://www.aamc.org/download/181690/data/guidelinesforstudentsprovidingpatientcare.pdf http://www.ama-assn.org/ama/pub/physician-resources/solutions-managing-your-practice/coding-billinginsurance/hipaahealth-insurance-portability-accountability-act.page? http://www.ama-assn.org/ama/pub/physician-resources/legal-topics/patient-physician-relationshiptopics/patient-confidentiality.page? http://fmignet.aafp.org/online/fmig/index/resources/hipaaresources.html Appendix A Code of Conduct for Premedical Students Participating in Shadowing When shadowing a physician, I will: 1. Arrive promptly. 2. Accurately represent my position and role. 3. Appreciate the limits of my role as an observer. 4. Respects patients’ rights to refuse to have students present. 5. Treat all patients and staff with respect and dignity, regardless of age, gender, race, ethnicity, national origin, religion, disability, or sexual orientation. 6. Maintain strict confidentiality about patient information. 7. Maintain honesty and integrity by being forthright in my interactions with patients, peers, physician supervisors and staff. 8. Ensure patient safety by remaining at home if I am ill; and will notify physician of my planned absence 9. Report concerns about patient safety to the physician who is being shadowed. 10. Behave in an appropriate, professional, courteous manner at all times. 11. Not initiate or accept patients’ invitations to engage in social or social media relationships. 12. Dress and act professionally. 13. Not abuse drugs or alcohol. 14. Be aware of and follow the guidelines of my sponsoring institution and of the setting in which I am an observer. I agree to follow the Code of Conduct described above: Print name_______________________________Signature______________________Date________ Appendix B Confidentiality and Privacy of Patient Information Dear Student, As a student who is rotating in this health care setting and office practice, you have an ethical and legal duty to keep patient information confidential. Federal law known as the Health Insurance Portability and Accountability Act of 1996 (HIPAA) allows health care providers to use and disclose patient information for certain reasons, such as treatment, but at times it is necessary for the patient to agree to have his/her information used or disclosed. Health care providers also must consider who has access to the information and how much they need to see. Allowing a student observe an encounter between a provider and a patient requires patient authorization. Failure to maintain the confidentiality of patient information as required by HIPAA is considered a violation of the law and may have serious consequences. Some general guidelines: • • • • • Access patient information only under the direction and supervision of the health care provider you are shadowing. Share or discuss patient information only when necessary and only in locations where the confidentiality of that information can be maintained. Patient information should never be disclosed in any form of social media. Be familiar with and follow the health care system and provider’s policies on confidentiality and privacy. Should you have any questions or concerns, discuss them with the physician you are shadowing. Student Agreement I have received and reviewed all information that I was given about patient privacy and confidentiality. I understand there are rules regarding the use and disclosure of patient protected healthcare information, and I agree to abide by such rules and keep protected healthcare information confidential. I understand there are both educational and legal punishments if I violate this policy. I recognize that I may be immediately removed and excluded from this program, if I do not comply with this Confidentiality and Privacy Agreement. Print name Signature (Adapted from American Academy of Family Physicians, 2011) Date________ Admissions Initiative Pathways for Tomorrow’s Doctors The Situational Judgment Test (SJT) Prototype Project Committee on Admissions July 10, 2013 What is the Admissions Initiative? Our goal: to support medical schools as they work to identify and select the applicants that are the best fit for their institutions in the most informed and efficient manner possible. Admissions Initiative Pathways for Tomorrow’s Doctors What are we working on? • Supporting the implementation of holistic admissions • Establishing core competencies and exploring ways to ease transition to competency-based admissions • Refining existing tools and investigating and developing new tools to evaluate the whole applicant Admissions Initiative Pathways for Tomorrow’s Doctors Core competencies for entering medical students Admissions Initiative Pathways for Tomorrow’s Doctors What is a competency? • Observable behavior that combines knowledge, skills, values, and attitudes related to a specific activity Admissions Initiative Pathways for Tomorrow’s Doctors What are the core competencies for entering medical students? Thinking & Reasoning Critical Thinking Quantitative Reasoning Science Living Systems Human Behavior Scientific Inquiry Interpersonal Service Orientation Ethnical Responsibility to Self & Others Social Skills Reliability & Dependability Cultural Competence Resilience & Adaptability Teamwork Capacity for Improvement Written Communication Oral Communication Admissions Initiative Pathways for Tomorrow’s Doctors Intrapersonal What new tools are we developing to move us forward in assessing the inter- and intrapersonal competencies? Admissions Initiative Pathways for Tomorrow’s Doctors Situational Judgment Test (SJT) • Standardized instrument used to measure interpersonal/intrapersonal competencies • Presents scenarios and requires applicants to describe how s/he would respond • Commonly used in organizational settings (e.g., executive selection) • Used in medical education in Canada, Belgium, Israel, and the UK Admissions Initiative Pathways for Tomorrow’s Doctors What is an SJT? Note to COA: We will show a very short SJT demo at the meeting. Admissions Initiative Pathways for Tomorrow’s Doctors How might an SJT work in medical school admissions? • Provide information about inter- and intrapersonal competencies for use in pre-interview screening • Scale to the number of examinees who take the MCAT • Use live action or animation to present scenarios • Online administration • 90 minutes or less of testing time • Result in one overall or two (inter- and intra-personal) scores Admissions Initiative Pathways for Tomorrow’s Doctors How are we testing our thinking about SJTs? • Multi-stage project to investigate the viability and appropriateness of SJTs • Includes several phases of research • Multiple decision points built in along the way • Gather input from constituents throughout the process Admissions Initiative Pathways for Tomorrow’s Doctors Project timeline Stage Timeline 1. Develop SJT prototype Jan. 2013 – Sept. 2013 2. Research Jan. 2014 - Dec. 2015 (multiple years may be needed) 3. Pilot testing No earlier than 2016 (multiple years may be needed) 4. Operational No earlier than 2017 After the conclusion of each stage, AAMC will analyze data and make a decision about whether or not to continue to the next stage. Admissions Initiative Pathways for Tomorrow’s Doctors Stage 1: Develop SJT Prototype • AAMC wanted to learn more about the viability of SJTs for use in medical school admissions • Conducted an “environmental scan” and indentified several vendors with expertise • Background research on vendor capabilities • Input from national-recognized experts Admissions Initiative Pathways for Tomorrow’s Doctors Stage 1: Develop SJT Prototype (contd.) • Selected 4 vendors to develop SJT prototypes • • Example of a fully-developed, operational SJT Propose a plan to address technical and operational issues • Partnered with 33 constituent “subject matter experts” to develop the SJT • • Admissions officers, pre-health advisors, medical school faculty Represented a diverse array of medical schools (public/private, USA/Canada, HBCU, different missions) Admissions Initiative Pathways for Tomorrow’s Doctors Stage 1: Develop SJT Prototype (contd.) • Prototypes will be delivered on July 15th • At the conclusion of this phase, AAMC will evaluate the proposal and prototypes and determine whether to continue to the next stage Admissions Initiative Pathways for Tomorrow’s Doctors Stage 2: Initial Research (January 2014-December 2015) • Conduct research in three primary areas: • Psychometrics • Validity • Coaching and Faking • At the conclusion of this phase, AAMC will analyze data and determine whether to continue to the next stage Admissions Initiative Pathways for Tomorrow’s Doctors Stage 3: Pilot testing (no earlier than 2016) • Work with a small sample of medical schools to use the SJT in admissions • Psychometrics • Validity • Coaching and Faking • At the conclusion of this phase, AAMC will analyze data and determine whether to continue to operational development Admissions Initiative Pathways for Tomorrow’s Doctors Questions • What other research questions should we investigate? • Currently, the SJT is being designed to measure inter- and intra-personal competencies. What feedback do you have about this scoring approach? • What are your thoughts about administering the SJT in an online, unproctored environment? • What other feedback do you have about the SJT? Admissions Initiative Pathways for Tomorrow’s Doctors Admissions Initiative Pathways for Tomorrow’s Doctors ©