Assessment of the Pelvis Handout PPT
advertisement

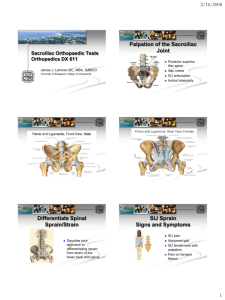
assessment of the pelvis Prepared and presented by Nichole Hamilton, Physiotherapist for Clinical Edge Assessment of the Pelvis Anatomy Review Bony Landmarks Function of the pelvis and SIJ Tests of Dysfunction Directions and ideas for treatment www.clinicaledge.com.au Anatomy Review ! Ligaments of the SIJ • Anterior SI ligament • Interosseous and Posterior L shaped joint with shorter vertical arm and longer horizontal arm ligaments • Sacrotuberous ligament • Sacrospinous ligament • Iliolumbar ligament • Long dorsal ligament ! Innominate: Ischium, pubis and ilium ! Sacrum: sacral base and apex Palpation Innominate: ! ASIS ! PSIS ! Ischial Tuberosity Sacrum: ! Sacral base ! Sacral apex and hiatus ! Sacral Sulcus ! Inferior lateral angle Copyright Clinical Edge 2011 Physiological movements of the SIJ • Innominate anterior rotation • Innominate posterior rotation www.clinicaledge.com.au 1 SIJ and pelvis: function Physiological movements of the SIJ ! SIJ: ! Functions to transmit forces between the lumbar spine and lower limb Sacrum • Nutation and Counternutation • Torsion- combined rotation and contralateral side flexion SIJ Stability • Vertical orientation makes the SIJ’s susceptible to to shear forces in the vertical plane (Snijders et al 1993) • Therefore requires adequate lateral compression to stabilise and transfer load efficiently (Lee 1999) SIJ Stability ! The closed packed position for optimal stability is a combination of: • Sacral Nutation • Innominate Posterior Rotation ! (Sturesson et al 1989, 2000, Hungerford et al 2004) Factors improving SIJ compression Examination and Testing for SIJ dysfunction • Form Closure (Sturesson et al 1989, 2000, Hungerford et al 2004) • Force Closure • Ability to achieve closed packed position Copyright Clinical Edge 2011 To test for SIJ and pelvic dysfunction we need to analyse its ability to achieve normal function: • Functional tests of SIJ load transfer ability • Tests of force closure • Tests of form closure www.clinicaledge.com.au 2 Functional Tests of Load Transfer Functional Tests of Load Transfer Forward Flexion Test: • Palpate PSIS bilaterally and flex forward at hips • Positive when one PSIS raises superiorly (anterior innominate rotation and unlock SIJ) • Can retest one SIJ at a time Stork Test: Stance Phase • Palpate PSIS and S2 spinous process • Ask patient to stand on one leg and flex contra-lateral hip • Positive for SIJ dysfunction if innominate anteriorly rotates (or unlocks) relative to sacrum (Stuerrson et al 2000, Hungerford et al 2004) SIJ Dysfunction Tests of Force Closure ! Active Straight Leg Raise • Tests ability to maintain LP stability during load transfer • Patient Supine • Actively raise one leg off plinth, then repeat on opposite side • Differences in subjective effort noted and compensation strategies observed !Positive functional and load transfer tests indicate a failure to efficiently transfer load between the trunk and lower limb through the pelvis Why? (Mens et al 1999, 2001, 2004) Tests of Force Closure Tests of Form Closure ! If intra-articular glide is restricted in the SIJ, the ability to efficiently achieve form closure and load transfer can be compromised • Squish test (Buyruk et al 1995) • Articular Glide test (Lee 1999) ASLR Test with Compression • Retest ASLR with compression around the pelvis • Does this improve or change patients ability to ASLR? • Can also test PHE (Lee 1999) Copyright Clinical Edge 2011 www.clinicaledge.com.au 3 Directions for Treatment 1 Passive Joint Glide Test (Squish) !"#$#%$&'()&#%*(+()&+#,'&-. ! !"#$%%&'$!"#$()*+,$! -./0#1$0*.1$)+.23-#+$/2$4#0"/3$5)6.)$ 2##13$-7+)6#+$#8.9/2.)/*2: ! (;<$=+)/>70.+$?0/1#$)#3)3$#@7.0 ! =(AB$)#3)$;CDBEFG($H/)6$>*94+#33/*2 • Glide the ilium on the sacrum along the joint line (posteriorly and slightly superiorly) • Compare left and right feeling for R1 and R2 symmetry in resistance $ /0121#2!342#!45!67/1#/0!2#87/!14/#41152#9:;1# 6:98;122!:4#!4#/01#81<=!2#/:#>?46/!:4@## # /0!2#674#6:91#>;:9#;107A#1B1;6!212#/7;31//!43# >?46/!:47<#145?;7461#!4#/;742=1;2?2C# 9?</!>!5!2#745D:;#3<?/17<2@ Directions for treatment 2 directions for treatment 3 !"#$#%$&'()&#%*(+()&+#,'&-. ! G8.940#3$*-$9.27.0$)6#+.4I$-*+$#.>6$/21/"/17.03$K+#3)+/>)#1$ ! !"#$%%&'$!"#$()*+,$! -./0#1$0*.1$)+.23-#+$/2$4#0"/3$5)6.)$2##13$-7+)6#+$ #8.9/2.)/*2: ! =+)/>70.+$?0/1#$)#3)3$=33I9#)+/> ! =(AB$)#3)$)6.)$1*#3$JE&$/94+*"#$H/)6$>*94+#33/*2 )/337#L$>.2$/2>071#$9.33.M#'$2##10/2M'$3)+#)>6#3'$)+/MM#+$4*/2)$ +#0#.3#'$CG&$N$)6/3$H/00$1#4#21$*2$I*7+$3,/00$.21$)+./2/2M ! G8#+>/3#$)*$/94+*"#$3).O/0/)I$>.2$/2>071#$4/0.)#3'$4*3)7+.0$ .H.+#2#33'$-72>)/*2.0$>*+#$#217+.2>#$#8#+>/3#3'$-72>)/*2.0$ M07)#.0$3)+#2M)6#2/2MP $ /0!2#97E#!45!67/1#/01#87/!14/#!2#7<;175E#F/::#6:98;12215G#745# 41152#974?7<#/01;78E#5!;16/15#7/#;12/;!6/15#2!H#:;#/!30/# 9?26<12@ # # /0!2#;1I?!;12#!45!=!5?7<#722122914/C#A?/#674#!46<?51# 8!;!>:;9!2C#/><C#I<#:;#0792/;!432 # 6JKKJ)LM#%$&'()&+#,'LL#)((N#$#OJKP')$&'J)#J"#K$)Q$L# &-(*$%M#"J*#*(+&*'O&(N#&'++Q(DRJ')&#$)N#+&$P'L'+$&'J)# (S(*O'+(+#"J*#J%&'K$L#*(OJT(*M#J"#"Q)O&'J) References • • • • • • Buyruk H M, Stam H J, Snijders C J, Vleeming A, Lameris J S, Holland W P J 1997 Measurement of sacroiliac joint stiffness with color doppler imaging and the importance of asymmetric stiffness in sacroiliac pathology. In: Vleeming A, Mooney V, Dorman T, Snijders C, Stoeckart R (eds) Movement, Stability and Low Back Pain. Churchill Livingston, Edinburgh, p 297 Damen L, Buyruk H, Guler-Uysal F, Stam H 2001 Pelvic pain during pregnancy is associated with assymetrical laxity if the sacroiliac joints. Obs Gynae Scand 80: 1019-1024 DonTigny R 1985 Function and Pathomechanics of the Sacroiliac Joint A Review. Physical Therapy 65(1): 35Hungerford B, Gilleard W, Hodges P 2003 Evidence of altered lumbo-pelvic muscle recruitment in the presence of sacroiliac joint pain. Spine 28(14) 1593-1600 Hungerford B, Gilleard W, Lee D 2004. Altered patterns of pelvic bone motion determined in subjects with posterior pelvic pain using skin markers. Clinical Biomechanics. Hungerford B, Gilleard W, Hodges P, Lee D 2004 Paper presented at the 5th World Congress on Low Back and Pelvic Pain. Altered Lumbo-Pelvic muscle recruitment occurs in the presence of sacroiliac joint pain. References • • • • • • • Copyright Clinical Edge 2011 Lee D 1999 The Pelvic Girdle; An approach to the examination and treatment of the lumbo-pelvic-hip region. Churchill Livingston, Edinburgh, pp145-151. Mens J, Vleeming A, Snijders C, Stam H, Ginai A 1999 The active straight leg raise test and mobility of the pelvic joints. European Spine 8:468 Mens J, Vleeming A, Snijders C, Koes B, Stam H 2001 Reliability and Validity of the active straight leg raise test in posterior pelvic pain since pregnancy. Spine 27(2):196 O’Sullivan P, Beales D, Beetham J, Cripps J, Graf F, Lin I, Tucker B, Avery A 2002 Altered motor control strategies in subjects with sacroiliac joint pain during the active straight leg raise test. Spine 1:21(1): E1-8 Snijders C, Vleeming A, Stoeckart R 1993 Transfer of lumbosacral load to the iliac bones and legs. 1: Biomechanics of self bracing of the sacroiliac joints and its significance for treatment and exercise. Clinical Biomechanics 8: 285-294 Sturesson B, Uden A, Vleeming A 2000 A radiosteriometric analysis of movements of the sacroiliac joints during the standing hip flexion test. Spine 25(3): 364 Vleeming A, Mooney V, Dorman T, Snijders C (eds) 1995b Second Interdisciplinary world congress on low back pain: The intergrated function of the lumbar spine and sacroiliac joint, San Diego. www.clinicaledge.com.au 4