Pelvic Tilt - PTJ - American Physical Therapy Association
advertisement

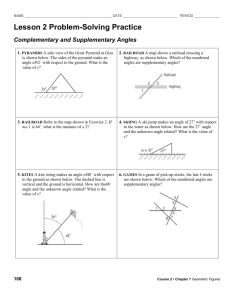
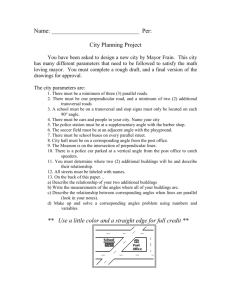
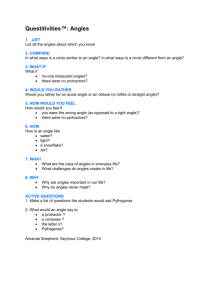
Pelvic Tilt Intratester Reliability of Measuring the Standing Position and Range of Motion RICHARD GAJDOSIK, RALPH SIMPSON, RICHARD SMITH, and RICHARD L. DONTIGNY The purpose of this study was to examine intratester reliability of a test designed to measure the standing pelvic-tilt angle, active posterior and anterior pelvic-tilt angles and ranges of motion, and the total pelvic-tilt range of motion (ROM). After an instruction session, the pelvic-tilt angles of the right side of 20 men were calculated using trigonometric functions. Ranges of motion were determined from the pelvic-tilt angles. Intratester reliability coefficients (Pearson r) for test and retest measurements were .88 for the standing pelvic-tilt angle, .88 for the posterior pelvic-tilt angle, .92 for the anterior pelvic-tilt angle, .62 for the posterior pelvic-tilt ROM, .92 for the anterior pelvic-tilt ROM, and .87 for the total ROM. We discuss the factors that may have influenced the reliability of the measurements and the clinical implications and limitations of the test. We suggest additional research to examine intratester reliability of measuring the posterior pelvic-tilt ROM, intertester reliability of measuring all angles and ROM, and the pelvic tilt of many types of subjects. Key Words: Pelvis, Range of motion, Reliability tests, Physical therapy. Physical therapists (PTs) routinely administer therapeutic procedures that either directly or indirectly affect the standing position and active range of motion (ROM) of the pelvic tilt in the sagittal plane. The effects of the procedures are rarely quantified, however, because noninvasive clinical tests that isolate pelvic motion as an independent functional movement are unavailable. Physical therapists should consider clinical tests designed to provide objective and reliable pelvic-tilt data because such tests would permit documenting change in the pelvic tilt after a specific physical therapy regimen. The effects of therapeutic procedures could then be quantified and changes in the procedures could be made accordingly. Numerous techniques for measuring trunk motions in the sagittal plane have been reported in the literature. The techniques include using radiography,1-4 photography,3, 5, 6 spondylometry,7, 8 flexible rules that conform to trunk curves,9, 10 tape measures to record the change in centimeters between skin marks11-14 or bony landmarks,15 and variations of goniometry.6,1 0 , 1 4 ,6-18 Although interest has been widespread in measuring trunk movements, none of these published papers reported measuring active ROM of the pelvic tilt as an Mr. Gajdosik is Associate Professor, Physical Therapy Program, University of Montana, Missoula, MT 59811. He is currently doing graduate work at the University of North Carolina at Chapel Hill, Chapel Hill, NC. Address correspondence to 612 Hibbard Dr, Chapel Hill, NC 27514 (USA). Mr. Simpson was a senior physical therapy student when this study was conducted. He is currently Staff Physical Therapist, The Sports Medicine Clinic, Seattle, WA. Mr. Smith is Visiting Assistant Professor, Physical Therapy Program, University of Montana, Missoula, MT. Mr. DonTigny is a physical therapist at the Havre Clinic, Havre, MT. This paper was adapted from a presentation at the Spring Meeting of the Montana Chapter of the American Physical Therapy Association, Missoula, MT, May 21, 1983. This article was submitted January 12, 1984; was with the authors for revision 11 weeks; and was accepted August 16, 1984. Volume 65 / Number 2, February 1985 isolated movement. Radiographic methods for measuring the standing pelvic-tilt (SPT) position have been reported,2, 3 and these methods could be used to measure ROM, but radiographic examination is generally regarded as expensive, potentially harmful, and not always available to PTs. We found one study that reported measuring the SPT angle, the posterior pelvic-tilt (PPT) angle, and the anterior pelvic-tilt (APT) angle with a noninvasive computerized method, the Iowa Anatomical Position System (IAPS).19 Even so, the IAPS, as with radiography, is not readily available to PTs. Recently, Sanders and Stavrakas suggested a noninvasive clinical technique for measuring the SPT angle relative to the horizontal plane.20 The reliability of the technique, however, was not reported. We postulated that the test suggested by the authors could be used reliably to measure the SPT angle, and by modifying the test and standardizing testing procedures, the test could also be used reliably to measure the PPT and APT angles after active movement. These angles could then be compared with the SPT angle to determine the PPT-ROM and the APT-ROM. The total pelvic tilt (TPT) ROM could be calculated as the difference between the PPT and APT angles. The purpose of this study was to investigate intratester reliability of measuring the angles of SPT, PPT, APT, and the active ROM of pelvic tilting in the sagittal plane. METHOD Subjects and Instructions Twenty healthy men ranging in age from 19 to 34 years, with a mean age of 25.2 years, volunteered to participate in this study. Their mean weight was 75 kg (range, 61-91 kg), and their mean height was 179 cm (range, 170-195 cm). Subjects were limited to men who had Normal muscle strength and normal ROM of the back and lower extremities 169 and who had no history of orthopedic or neurologic disorders. All subjects were instructed to restrict excessive physical activity on the day of testing, such as recreational running and bicycling, and to wear gym trunks for the tests. On the day of testing, all subjects reviewed and signed informed consent forms for the study that had been approved by the University of Montana Institutional Review Board for Use of Human Subjects in Research. We then taught the subjects how to perform the PPT and the APT. After learning the movements, they were required to perform the movements for approval by the researchers. In addition, we encouraged all subjects to relax and told them that the movements would not be judged as "good" or "bad." We believed these verbal cues decreased subjects' anxiety and, therefore, helped to standardize the testing. Testing Fig. 1. Examiner measuring distance between ASIS and PSIS by compressing depth caliper over adhesive-backed stars. Fig. 2. Standing pelvic tilt: Showing position of examiner measuring distance between PSIS and floor. Note distance from ASIS to floor. 170 We conducted a pilot study to refine instrument placements and testing procedures. As a result, we found that in some subjects the pelvis moved under the skin during active movement. Consequently, when the posterior superior iliac spines (PSISs) and the anterior superior iliac spines (ASISs) were marked with a felt-tip pen as suggested by Sanders and Stavrakas,20 the pelvis moved under the skin and yielded invalid measurements. To ensure that the test was clinically valid, the PSIS and ASIS were palpated and marked with removable, small adhesive-backed stars when the end points of PPT and APT were reached. The actual test session for collecting data included both a test and a retest on the same day between 2 PM and 5 PM. Three subjects were tested each afternoon. After the initial tests, the subjects relaxed supine on beds for 30 minutes before the retests, but neither physical activity nor sleep were allowed during the rest periods. One of us (R. Simpson) administered each test and retest by using bony landmarks on the right side of the subjects. The time required to conduct one complete test of all angles was less than 10 minutes. Standing pelvic tilt. Each subject stood erect with his feet approximating a designated line on a tile floor. The right ASIS and right PSIS were palpated and marked with the adhesive-backed stars. We then placed a depth caliper over the stars, which were compressed to "firm resistance," and observed and recorded the distance between the spines to the nearest millimeter (Fig. 1). This point to point measurement on one innominate bone should remain constant with any change in position of that bone. The measurement was, therefore, used to calculate the PPT and APT angles. After measuring the distance from the right ASIS to the right PSIS, we used a sliding pointer on a meter stick mounted on a wood base to measure the distances from the floor to the right ASIS and from the floor to the right PSIS (Fig. 2). We then recorded the measurements to the nearest millimeter and removed the stars. Posterior pelvic tilt. While the subject stood erect as in the SPT measurements, we instructed him to keep his knees straight, to tighten the abdominal and gluteal muscles, and to move the top of the pelvis back to initial resistance without causing pain or discomfort (Fig. 3). The subject held this position while the right PSIS was palpated, marked, and the distance to the floor measured, and the right ASIS was palpated, marked, and the distance from the star to the floor measured. The subject then relaxed to the SPT position, and we removed the stars. Anterior pelvic tilt. From the SPT position, the subject was reminded to stand erect and instructed to arch the low back PHYSICAL THERAPY RESEARCH and move the top of the pelvis forward to initial resistance without causing pain or discomfort (Fig. 4). Again, the iliac spines were palpated, marked, and the distances from the stars to the floor measured. The subject relaxed to the SPT position, and we removed the stars for the last time. Data Analysis We calculated SPT, PPT, and APT angles from the raw data by using a trigonometric calculator to determine angle theta (θ) using the formula: (1) where the side opposite was the height difference between the PSIS and the floor and the ASIS and the floor, and the hypotenuse was the distance between the ASIS and PSIS (Fig. 5).20 Pelvic-tilt angles with the PSIS above the horizontal were assigned positive degree values and those with the PSIS below the horizontal were assigned negative degree values. The PPT-ROM was calculated as the difference between the PPT angle and the SPT angle, and the APT-ROM was calculated as the difference between the APT angle and the SPT angle. We determined the TPT-ROM as the difference between the PPT and APT angles. To check for systematic variation of the pelvic-tilt angles and ROM, paired t-ests were conducted on the test-retest data. The level of significance was set at p ≤ .05. We used the Pearson product-moment correlation coeffi­ cient to determine intratester reliability. To interpret the reliability coefficients, we chose to designate reliability of .90 to .99 as high; .80 to .89 as good; .70 to .79 as fair; and those TABLE Pelvic-Tilt Angles, Pelvic-Tilt Range of Motion, and Reliability Fig. 3. Posterior pelvic tilt: Showing a) contracted abdominal mus­ cles, b) contracted gluteal muscles, and c) extended knees. Note distance from PSIS to floor (A) and distance from ASIS to floor (B). Degrees Tests (N = 20) r s Standing tilt angle Test Retest Posterior tilt angle Test Retest Anterior tilt angle Test Retest Posterior tilt ROM Test Retest Anterior tilt ROM Test Retest Total ROM Test Retest Range less than .69 as poor.21 Tests of significance were calculated for each correlation coefficient to determine if they were significantly different from zero. 8.35 8.53 4.17 4.08 1.99-15.72 1.33-18.57 .88a -0.53 0.19 4.49 4.02 - 6 . 9 7 - 7.55 - 5 . 6 7 - 7.64 .86a 21.21 21.10 5.10 4.84 13.37-29.37 14.02-30.43 .92a 8.88 8.34 3.93 2.32 0.34-14.96 2.43-14.55 .62b RESULTS The pelvic-tilt angles, ROM, and reliability for the tests and retests are reported in the Table. No significant difference was found between the test and retest angles or the test and retest ROM measurements. The most reliable measurements were the APT angle (r = .92) and the APT-ROM (r = .92). The SPT angle (r = .88), the PPT angle (r = .86), and the TPTROM (r = .87) were all measured with good reliability. Poor reliability was demonstrated for the PPT-ROM (r = .62). The correlation coefficients were statistically significant (p < .05). DISCUSSION 12.86 12.57 5.47 5.79 5.85-26.45 5.81-25.28 .92a 21.74 20.91 6.69 6.39 12.34-35.22 10.53-35.94 .87a a p < .001. b p < .005. Volume 65 / Number 2, February 1985 We believe that obtaining high reliability for the APT angle and good reliability for the SPT and PPT angles depended on instruction sessions and testing procedures that were consist­ ently applied to each subject. Before testing, we confirmed that each subject could perform the PPT and the APT. Because the subjects knew the actions, the influence that learning the actions could have had between tests and retests 171 Fig. 5. Schematic diagram of pelvic-tilt measurement. A-B = side opposite and C = hypotenuse. Reprinted with permission from Sanders and Stavrakas. Fig. 4. Anterior pelvic tilt: Showing arched low back and distance from PSIS to floor (A) and distance from ASIS to floor (B). on reliability was decreased. Practicing the movements probably contributed to the stability of the test and retest measurements by decreasing the effect that repeated measurements could have had on the PPT and APT angles. Atha and Wheatley reported that the act of measuring hip flexion increases the ROM of hipflexion,and that most changes take place over the first four trials when testing without a practice motion.22 In our study, the lack of systematic variation between the tests and retests indicates that practicing the movements before testing served as a warm-up and lessened the potential for increases in ROM from early repeated measurements. Consistently applying the same action commands ensured that all subjects performed the same movements and reached similar end points of each motion for both tests and retests. Telling the subjects to stand erect during the actions isolated the motion to the pelvis and limited anterior and posterior leaning that could have affected the pelvic angles. Also, the correlation coefficients indicate no need to use stabilizing devices to prevent swaying movements that may distort the 172 measurements from the iliac spines to the floor by a parallelogram effect. Accurately palpating the iliac spines and accurately placing the adhesive-backed stars over the spines also could have contributed to reliable measurements. Furthermore, the stars provided a precise reference point for placing the depth caliper and the sliding pointer. The depth caliper used in this study provided a relatively large surface area for placing the caliper firmly over the iliac spines. As a result, slipping off the spines was easily prevented. The large surface area also permitted compressing the caliper to "firm resistance" without causing pain. For these reasons, using a caliper with a large surface area may be more reliable than using a bowleg caliper as Sanders and Stavrakas suggested.20 Although measuring the distance between the ASIS and the PSIS yielded reliable measurements of pelvic-tilt angles, the raw measurements do not represent a "true" bone to bone distance because the intervening skin and subcutaneous connective tissue are compressed. We addressed this problem by compressing the caliper to firm resistance in an effort to standardize the force of compression. Even though our results were reliable, measuring this distance on people who are obese or whose body weight changes over time may not be as reliable as reported on the subjects in this study. Variations in subcutaneous connective tissue thickness should be considered because patients may vary in body build from lean to obese; all subjects in our study were lean to medium body build. Moreover, palpating the iliac spines may be difficult in some patients because of obesity or bony variations of the ilium. If the spines cannot be palpated, the test cannot be used. The APT-ROM was determined with high reliability and the TPT-ROM was determined with good reliability, but the PPT-ROM demonstrated poor reliability. The fact that the reliability for the PPT-ROM deviates from that of the PPT angle is likely to be a result of increased noise (fluctuations) PHYSICAL THERAPY RESEARCH because the motion computations involved twice as many raw measurements as for the angle. The noise was apparently much less significant in the APT-ROM and the TPT-ROM. Additional studies should be conducted to examine the reliability of measuring the PPT-ROM. Furthermore, if more than one examiner measures the same person, then the intertester reliability for measuring all angles and ROMs should be studied before the test is used with confidence. Clinical Implications The clinical implications of the test may be far-reaching. Measurements of the APT and the PPT may represent the standing ROM of lumbar trunk extension and flexion, respectively. In a study of the effect of pelvic tilt on standing posture, Day et al documented increased depth of the lumbar curve (extension) with the APT and decreased depth (flexion) of the lumbar curve with the PPT.19 We also observed this relationship of pelvic tilting to lumbar trunk motion (Figs. 3, 4). If the test is used to examine ROM of the lumbar trunk, the possibility that motion or lack of motion in the sacroiliac joints (SIJs) could affect the pelvic-tilt measurements should not be overlooked. Lavignolle et al demonstrated movement in the SIJs with active flexion and extension of the lower limbs.23 Other studies have documented that movement occurs in the SIJs in conjunction with trunk motions in the sagittal plane.2. 24. 25 Accordingly, the SIJs may move during anterior and posterior pelvic tilting and cause either bilateral or unilateral movement of the pelvis in addition to movement of the lumbar spine. Clinical evidence indicates that both bilateral and unilateral SIJ dysfunction can alter the positions and ROM of the pelvis, thus affecting the bilateral symmetry of the pelvic tilt.26, 27 In addition to the possibility of pelvic tilt asymmetry from SIJ dysfunction, asymmetry may result from disorders of the trunk, such as scoliosis or unilateral muscle spasms, and from problems affecting the lower limbs, such as diseases of the hips or leg-length discrepancies. Trunk and pelvic girdle muscle strength-flexibility imbalances and bony anomalies may also contribute to bilateral asymmetry of the pelvic tilt. Although we measured the right side only, we encourage therapists to measure and compare both sides and to conduct further research to examine the effects of therapeutic procedures on the pelvic tilt. Physical therapists should realize that the test is limited to measuring pelvic-tilt angles and ROM in the sagittal plane. We do not imply, however, that the pelvis moves only in the sagittal plane. Gait studies have demonstrated that the pelvis also moves in the transverse plane.28-30 The relationship of pelvic tilting, as measured in our study, to pelvic tilting and transverse pelvic rotation during walking, however, is undetermined and warrants further study. Physical therapists should also consider that the test is limited to persons who can actively tilt the pelvis and hold the end point of each motion while standing. Instruction sessions before testing should, therefore, be considered. Because the PPT is the most complex action, special training may be needed before the action is adequately performed. CONCLUSION Within the limitations of this study, we conclude that the technique suggested by Sanders and Stavrakas20 for measuring the SPT angle is reliable, and that by modifying the test, one examiner can reliably measure the PPT angle, APT angle, APT-ROM, and TPT-ROM. The PPT-ROM was measured with poor reliability. If the test is conducted as described in this article, the test should provide both clinicians and researchers with an objective, reliable, and quick method of measuring pelvic-tilt angles and ROM. Reliable measurements will permit documenting these angles and ROM, and any change in the angles and ROM after a specific physical therapy regimen. The effects of therapeutic procedures can then be quantified and changes in the procedures can be made accordingly. Additional studies are suggested to examine the 1) intratester reliability of measuring the PPT-ROM, 2) intertester reliability of measuring all angles and ROM, and 3) the pelvic tilt of people with normal muscle strength and ROM and of patients with problems affecting the pelvic tilt. Acknowledgments. We thank Kathleen Miller, PhD, the University of Montana; and Phil Witt and Barney LeVeau, PhD, of the University of North Carolina, for their assistance with the statistical analysis. Also, special thanks to Carrie Gajdosik for her editorial suggestions and Betty Stewart for typing the manuscript. REFERENCES 1. Tanz SS: Motion of the lumbar spine: A roentgenologic study. American Journal of Roentgenology, Radium Therapy and Nuclear Medicine 69:399412,1953 2. Clayson GF, Newman IM, Debevec DF, et al: Evaluation of mobility of hip and lumbar vertebrae of normal young women. Arch Phys Med Rehabil 43:1-8, 1962 3. Flint MM: Lumbar posture: A study of roentgenographic measurements and the influence of flexibility and strength, Res Q 34:15-21,1963 4. Hanley EN, Matteri RE, Frymoyer JW: Accurate roentgenographic determination of lumbar flexion-extension. Clin Orthop 115:145-148,1976 5. Davis PR, Troup JDG, Burnard JH: Movements of the thoracic and lumbar spine when lifting: A chrono-cyclophotographic study. J Anat 99:13-26, 1965 6. Troup JDG, Hood CA, Chapman AE: Measurements of the sagittal mobility of the lumbar spine and hips. Annals of Physical Medicine 9:308-321, 1968 Volume 65 / Number 2, February 1985 7. Sturrock RD, Wojtulewski JA, Hart FD: Spondylometry in a normal population and in ankylosing spondylitis. Rheumatology and Rehabilitation 12:135-142,1973 8. Hart FD, Strickland D, Cliffe P: Measurements of spinal mobility. Ann Rheum Dis 33:136-169,1974 9. Israel M: A quantitative method of estimating flexion and extension of the spine—A preliminary report. Mil Med 124:181 -186,1959 10. Anderson JAD, Sweetman BJ: A combined flexi-rule/hydrogoniometer for measurement of lumbar spine and its sagittal movement. Rheumatology and Rehabilitation 14:173-179,1975 11. Macrae IF, Wright V: Measurement of back movement. Ann Rheum Dis 28:584-587, 1969 12. Moll JMH, Wright V: Normal range of spinal mobility. Ann Rheum Dis 30:381-386,1971 13. Moll JMH, Lyanage SP, Wright V: An objective clinical method to measure spinal extension. Rheumatology and Physical Medicine 2:293-312,1972 173 14. FitzgeraldGK,Wynveen KJ, Rheault W, et al: Objective assessment with establishment of normal values for lumbar spinal range of motion. Phys Ther 63:1776-1781, 1983 15. Frost M, Stuckey S, Smalley LA, et al: Reliability of measuring trunk motions in centimeters. Phys Ther 62:1431-1437, 1982 16. Lindahl O: Determination of the sagittal mobility of the lumbar spine. Acta Orthop Scand 37:241-254, 1966 17. Asmussen E, Heeboll-Nielsen K: Posture, mobility and strength of the back in boys, 7 to 16 years old. Acta Orthop Scand 28:174-189, 1959 18. Loebl WY: Measurement of spinal posture and range of spinal movement. Annals of Physical Medicine 9:103-110, 1967 19. Day JW, Smidt GL, Lehmann T: Effect of pelvic tilt on standing posture. Phys Ther 64:510-516, 1984 20. Sanders G, Stavrakas P: A technique for measuring pelvic tilt: Suggestion from the field. Phys Ther 61:49-50, 1981 21. Currier DP: Elements of Research in Physical Therapy. Baltimore, MD, Williams & Wilkins, 1979, p 159 22. Atha J, Wheatley DW: The mobilising effects of repeated measurement on hip flexion. Br J Sports Med 10:22-25, 1976 174 23. Lavignolle B, Vital JM, Senegas J, et al: An approach to the functional anatomy of the sacroiliac joints in vivo. Anatomia Clinica 5:169-176, 1983 24. Weisl H: The movements of the sacroiliac joint. Acta Anat (Basel) 23:8091, 1955 25. Colachis SC, Worden RE, Bechtal CO, et al: Movement of the sacroiliac joint in the adult male: A preliminary report. Arch Phys Med Rehabil 44:490498, 1963 26. Grieve GP: The sacroiliac joint. Physiotherapy 62:384-400, 1976 27. DonTigny RL: Dysfunction of the sacroiliac joint and its treatment. Journal of Orthopaedic and Sports Physical Therapy 1:23-35, 1979 28. Saunders JBdeC M, Inman VT, Eberhart HD: The major determinants in normal and pathological gait. J Bone Joint Surg [Am] 35:543-558, 1953 29. Murray MP, Drought AB, Kory RC: Walking patterns of normal men. J Bone Joint Surg [Am] 46:335-360, 1964 30. Murray MP, Kory RC, Sepic SB: Walking patterns of normal women. Arch Phys Med Rehabil 51:637-650, 1970 PHYSICAL THERAPY