Growth plates have an ordered arrangement
advertisement

Epiphyseal growth plate
- Growth plates have an ordered arrangement of chondrocytes
that reflects the chondrogenic events and processes that lead
to bone growth. From the epiphysis to the metaphysis, they
are arranged as four zones that gradually merge with each
other:
•zone of resting cartilage (attaches growth plate
to epiphyseal bone)
•zone of proliferating cartilage (mitosis of
chondrocytes occurs here)
•zone of hypertrophic (maturing) cartilage
(chondrocytes make matrix and enlarge lacunae)
•zone of calcified (calcifying) cartilage (matrix is
calcifying, chondrocytes are dying or dead attaches the growth plate to the metaphysis)
Undifferentiated or Resting Cell Zone:
- immediately adjacent to epiphysis are irregularly scattered
cartilage cells
- this is germinal layer that supplies the developing cartilage
cells
NB ***- injury to this layer results in cessation of growth
- the groove of Ranvier contains cells which flow into the into
the cartilage in this layer of the growth plate
- the function is to supply chondrocytes for increasing the
width of the growth plate
Zone of Proliferating Cartilage:
- location in which bone length is created by active growth of
cartilage cells
- on metaphyseal side, cartilage cells become aligned into
well-defined columns, known as zone of cellular proliferation
- it is at base of these columns that mitotic activity is found
- in this small area, two or three cells thick, occurs cell division
upon which entire growth in length of bone depends
- failure of these cells to thrive results in cessation of growth at
end of bone
Hypertrophic Cell Zone (Maturation Zone):
- layer in which chondrocytes become swollen and vacuolated
in process of maturation leading to cell death
- they hypertrophy at expense of extracellular matrix, & these
enlarged cartilage cells constitute the third zone, or
hypertrophic zone
- there is no active growth in this layer
- columns of cartilage cells extend toward metaphysis, being
constantly lengthened by cell division occurring at the base cells nearer the metaphysis begin to undergo changes that
ultimately lead to their destruction
- this is weakest portion of the epiphyseal plate (Salter Harris
fractures occur thru this zone)
(NB*** - in rickets, there is failure of calcification which causes
accumulation of cells in the hypertrophic layer
- juncture between epiphyseal plate & metaphysis is secured
by welding of metaphyseal bone to calcified cartilage matrix.
- collagen type X, may play a role in the calcification of this
cartilage
Zone of Provisional Calcification:
- area where, w/ death of chondrocyte & production of AP,
longitudinal bars of cartilage matrix become calcified
- last two cells in column of cartilage cells are in fourth zone, the
zone of provisional calcification. - it is in this area that
extracellular chondroid matrix becomes impregnated with
calcium salt
*** - This calcification of matrix is required for subsequent steps,
including:
- invasion of cartilage cells by blood vessels from metaphysis
- destruction of cartilage cells
- formation of bone along remaining walls of calcified cartilage
matrix
Endochondral ossification is the way in which most
bones form, including the limb bones.
- Small collections of mesenchymal cells cluster together,
become chondroblasts and begin to secrete cartilage
matrix.
- Other cells around them form a perichondrium and a tiny
cartilaginous model of a bone has been formed.
- Chondrocytes within the model grow and divide and
more chondrocytes and matrix is added to the surface by
the perichondrium, so the model gets larger.
•Osteogenic cells are carried in, too, form the
endosteum and begin to lay down bone matrix on
the inner surface of the marrow cavity. (This is the
primary centre of ossification.)
• The marrow cavity expands toward both
epiphyses as the cartilage continues to grow.
•Eventually secondary centres of ossifcation
occur in the epiphyses (at different times) and this
traps a thin plate of cartilage between the primary
centre and each secondary centre. These are the
growth plates of the bone.
- Later, the perichondrium is transformed into a periosteum
and a thin periosteal collar of bone matrix is laid down
around the model's shaft.
- The cartilage mineralises and is invaded by a blood vessel
from the periosteum.
- Cells that accompany the blood vessel erode the now dead
cartilage and form the marrow cavity.
Intramembranous ossification is the way in which
bones like the clavicle, mandible and some skull bones
form.
•Small collections of mesenchymal cells
cluster together, become osteoblasts and
begin to secrete osteoid. Other cells around
them form a periosteum and a tiny bone has
been formed.
•A little later, blood vessels and nerves invade
the bone.
•More bone is deposited on the surface by
osteoblasts of the periosteum, increasing the
size of the bone.
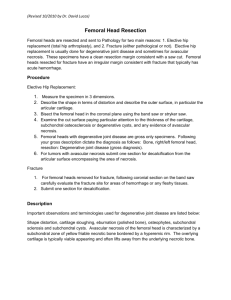
Epiphysial Growth Plate
The epiphysial growth plate, where cartilage is removed and bone is
formed, is marked by four stages (left to right): resting zone,
proliferative zone, hypertrophy zone, ossification zone
This is the normal fetal growth plate demonstrating the process of
endochondral bone formation in a long bone.
Congenital Dislocation of the Hip
Developmental Dysplasia of the Hip
The term "congenital dislocation of the hip" has
traditionally been used to describe abnormal infant hips
that may progress to dislocation.
"Developmental dysplasia of the hip”: denotes the
same range of hip problems but also includes hips that
are never documented to be dislocated but are poorly
developed, as well as hips that are determined to be
abnormal after the newborn period.
This new term is the the currently preferred term but it is
not yet universally employed.
Common risk factors:
- females (80-90%)
- 2/3 are firstborn
- breech presentation
- large baby
- low amniotic fluid
- family history.
***If it is unilateral the LEFT (70%) is usually involved
- bilateral in only 5%
*** But sometimes every one of these factors is absent,
and the baby is still affected
Incidence : one to two cases per 1,000 children
OTHER ASSOCIATED CONDITIONS
•Foot deformities ( club feet, metatarsus adductus)
•Torticollis
•Neuromuscular disorders
•Skeletal dysplasias
The hip is a 'ball and socket' joint.
Various problems can affect the baby's hip as it develops:
“Dislocation” - the ball does not lie safely in the socket
and is displaced from it
“Dislocatable” - although the ball is in the socket it can
slip in and out of place
“Subluxated” - although the hip is in the socket it is not
deeply in place
“Dysplastic”- In some children although the hip is in the right
place the socket does not grow properly and is too shallow
The Ortolani maneuver - the contralateral hip is held still
while the thigh of the hip being tested is abducted and gently
pulled anteriorly.
Positive Test - is the palpable and sometimes audible
"clunk" of the femoral head moving over the posterior rim of
the acetabulum and “ relocating” in the cavity.
The Barlow maneuver - is performed by adducting the hip
while pushing the thigh posteriorly.
Positive Test - If the hip goes out of the socket "dislocatable"
Ortolani and Barlow Maneuvers
(Left) Ortolani
(Right) Barlow
The hips are flexed to 90 degrees; the thumbs of the
examiner are placed on the medial proximal thigh, and the
long fingers are placed over the greater trochanter
These maneuvers cannot be performed in a fussy, crying
infant whose muscle activity may inhibit the movement of
an unstable hip.
The baby must be calm and relaxed . Try any method
available
The more poorly developed the acetabulum (and thus the
more unstable the hip), the less pronounced the "clunk."
The Ortolani maneuver must be performed very gently to
avoid obscuring the sound of the femoral head passing
over a poorly developed posterior acetabulum.
***NB : Audible high-pitched "clicks" without a sensation
of instability have no pathologic significance. They should
simply be re- examined at a later date
NB: If an unstable hip is not detected in the newborn period, a
positive Ortolani's test becomes less common.
- limited abduction is the predominant physical sign as the hip
becomes fixed in the dislocated position.
- other signs: an apparent shortening of the femur, asymmetric
skin folds and telescoping of the affected hip, are also clues to
dislocation.
NB: Xrays taken before four months old - before the head of
the femur starts to convert from invisible-on-xray cartilage to
visible bone (ossification) - are unreliable to rule out hip
dysplasia.
Ultrasound - of the hip is the best under four months.
Coronal sonogram of normal infant hips. (F=femoral head;
A=acetabulum)
RADIOLOGICALLY
1. supero-lateral migration of
femoral head
2. increased acetabular angle
3. small capital femoral epiphysis
Treatment
If an unstable hip is recognized at birth, treatment
consists of maintaining the position of the hip in flexion
(knee up towards the head) and abduction (knee away
from the centerline) for about 1-2 months.
The Pavlik harness is the most widely used device.
- The device maintains proper position of the femoral
head and allows for "tightening up" of the ligamentous
structures as well as for stimulation of normal formation
of the hip socket.
NB *** The treatment must be continued until the hip is
stable and xrays or ultrasound examinations are
normal.
Pavlick Harness
The harness pushes the femoral head toward the socket, and usually,
relocation of the femoral head will occur within 3-4 wk. The Pavlik
harness is approximately 95% successful in dysplastic or subluxated
hips and 80% successful in true dislocations.
If a spontaneous reduction does not occur by splinting, then
a surgical closed reduction (manipulation under anesthesia)
is done and the child is placed in a hip spica cast.
In the older infant from 6-18 Mo, surgical closed reduction
(manipulation under general anesthesia) is the major method of
treatment.
After 18 months of age - the progressive deformities
become so severe that major open surgical intervention
is necessary to realign the hip.
Including; open reduction , tendon releases , pelvic and
femoral osteotomies
***It is important to carefully examine the newborn
child and investigate and refer as needed.
TOE-WALKING
INTRODUCTION
zMay be normal prior to age 3
zAfter age three
{Shortened heel cord
zHabitual toe-walking
{Rule out neurologic causes such as cerebral
palsy as spinal dysraphism
HISTORY
zOften positive family history
zBilateral
{Think of other diagnosis if unilateral
PHYSICAL
z Gait
{Toe-walk
z Standing
{Flat
{Toeing-out
{Forefoot splaying
z Dorsiflexion limited
z Neurologic Exam
{Rule-out other causes
TREATMENT
zNatural History
{Not well delineated
{Many do not resolve spontaneously
{Benign?
treatment
zHeel-cord stretching and gait retraining
{Night splint
zSerial casting
{Ankle-foot orthosis
zSurgery
{Heel-cord lengthening
CLUBFOOT
INTRODUCTION
zCongenital Talipes Equinovarus
{Hindfoot equinus
{Subtalar joint varus
{Cavus
{Forefoot adduction
zMay be unilateral or bilateral
zFamilial tendency
HISTORY & PHYSICAL
z Noted at birth
z If unilateral
{Foot and calf smaller
z Deep creases
z Check for flexibility
z May be associated
with torticollis, and hip
and spine
abnormalities
RADIOLOGY
z Anteroposterior and
lateral weight-bearing
films
TREATMENT
zSerial casting
{+ heel-cord tenotomy
zSurgery for failures
zRecurrence rate not insignificant
{Follow throughout growth
POSITIONAL CALCANEOVALGUS
INTRODUCTION
zMarked dorsiflexion of entire foot at the
ankle joint
zMild and flexible eversion of the subtalar
joint
zLikely due to intrauterine malpositioning
HISTORY & PHYSICAL
zPresent at birth
zUsually able to bring foot out into inversion
and plantarflexion
zRule out congenital vertical talus
{Fixed equinus and valgus of the hindfoot
{Rigid dorsiflexion of midfoot on hindfoot
zRadiographs normal: R/O CVT
TREATMENT
zPassive stretching exercises to hasten
correction may be used
FLATFOOT
INTRODUCTION
zImportant to differentiate flexible from rigid
flatfoot
{Flexible flatfoot not usually problematic
HISTORY
zRigid flatfeet may be painful and can be
associated with increased ankle sprains in
tarsal coalition (abnormal connections
between some of the tarsal bones)
PHYSICAL
z Flexible
{Arch returns with sitting
or tiptoe standing
{Normal subtalar and
midtarsal motion
{Check dorsiflexion with
forefoot supinated
z Locks subtalar joint
z R/O tight achilles
physical
z Tarsal Coalition
{May be painful to move
or palpate subtalar joint
or other tarsal bones
{Subtalar motion often
decreased
{Pes planus and ankle
valgus may not be
striking
RADIOLOGY
z Normal in flexible
flatfoot
z Oblique views and
Harris view may help
view a coalition
TREATMENT
zFlexible flatfoot
{None needed
{May improve spontaneously
{Usually asymptomatic
{May try an orthotic to improve function or
alleviate pain
{Rarely surgery required
treatment
zTarsal Coalition
{Rest/activity modification
{Antiinflammatories
{Physiotherapy
{Orthotics
{Casts
{Surgery: resection or fusion
IDIOPATHIC SCOLIOSIS
INTRODUCTION
zFrontal plane spinal deformity associated
with torsional malalignment of the spinal
column
zFirst rule out other causes of scoliosis
CLASSIFICATION
z Idiopathic
z Neuropathic
z Myopathic
z Congenital
z Associated with
neural tissue defect
z Neurofibromatosis
z Mesenchymal
z Traumatic
z
z
z
z
z
z
Soft tissue contactures
Osteochondrodystrophies
Tumor
Rheumatoid disease
Metabolic
Related to lumbosacral
area
z Thoracogenic
z Hysterical
z Functional
HISTORY
zDeformity
{When noted
{Progression
{Pain
zNeurologic Symptoms
zGrowth Indices
PHYSICAL
z Cutaneous back
lesions
{Pigmentation
{Dimpling/sinuses
{Hair patches
z Thoracopelvic
balance
z Leg length
discrepancy
physical
z Range of motion
z Rotational
prominence
z Neurologic
examination
RADIOLOGY
z Coronal and Sagital
(3 foot standing films)
{Abnormal vertebrae
{Vertebral rotation
{Cobb angle
{Risser Sign
z Convexity determines
sidedness
z Other tests as needed
TREATMENT
zNatural History
{Why we need to treat
{Who we need to treat
PROGRESSION DURING GROWTH
Risser Sign
< 19
degrees
20 – 29
degrees
0–1
22%
progression
68%
progression
2-4
1.6%
progression
23%
progression
PROGRESSION AFTER MATURITY
Thoracic Curves
<60 degrees
Thoracic Curves
60 – 80 degrees
Lumbar Curves
<31 degrees
Lumbar Curves
>31 degrees
6 degrees/24 years
28 degrees/24 years
0 degrees/24 years
18 degrees/24 years
PULMONARY FUNCTION
zThoracic curves >60 degrees
{Decreased vital capacity
zThoracic curves >80 degrees
{Dyspnea
TREATMENT
zThree P’s
{Psychosocial issues
{Progression
{Pulmonary function
treatment
zObservation
{Small curve (<20 degrees?)
{Repeat x-rays every 4 months
zCobb angle
zProgression
treatment
zOrthotics
{Growing child
{>20 degree curve?
{Progression (>5 degrees)
treatment
treatment
z Surgery
{Large curves
{Progression despite
bracing
SCHEUERMANN DISEASE
INTRODUCTION
zStructural kyphosis of the thoracic,
thoracolumbar, and lumbar spine
zEtiology unknown
HISTORY
zAge >10 years of age
zDeformity
zPain
{At deformity or area of compensation
{Worse with sitting, standing, or physical activity
PHYSICAL
z Rounded shoulders
z Angular kyphosis
{Rigid
{pigmentation
RADIOLOGY
z Coronal and Sagital
(3 foot standing films)
{Vertebral wedging
z >50 on 3 consecutive
{Irregular end plates
{Schmorl Nodes
{Decreased disk space
{Cobb angle
TREATMENT
zNatural History
{Rapid progression during growth spurt
{Not clear whether it progresses at maturity
treatment
zObservation
{Mild deformity
{Repeat x-rays every 4 - 6 months
zCobb angle
zProgression
zExercise/physical therapy
{Improve muscle tone/posture and flexibility
treatment
treatment
SPONDYLOLYSIS &
SPONDYLOLISTHESIS
INTRODUCTION
zSpondylolysis: defect in the pars
interarticularis
zSpondylolisthesis: Slipping forward of one
vertebrae on the next
HISTORY
zMay be asymptomatic
zPain usually noted during adolescent
growth spurt
{Worse with activities
{May rarely get radicular pain
zDeformity
{Scoliosis
{Postural changes
PHYSICAL
z Decreased forward bending
{Hamstring tightness
z Tenderness on deep palpation in lumbosacral
area
z Large slips
{Flattening of the buttocks
{Step-off at lumbosacral junction
z Scoliosis
z Neurologic examination may be abnormal
RADIOLOGY
z Standing posteroanterior
and lateral lumbosacral
spine, spot lateral, and
oblique views
{ Pars interarticularis defect
{ Slipping
z Bone scan, CT, or MRI
sometimes needed for Dx
TREATMENT
zNatural History
{Progression usually during the adolescent
growth spurt
zRare at maturity
treatment
zObservation
{Asymptomatic
{Repeat x-rays every year if mild
zReduction of activity/physiotherapy
{Symptomatic
{Orthotic if not settling or if acute injury
treatment
z Surgery
{Repair of the defect
(<L4)
{Arthrodesis
Assessing Limb Alignment In Children
(when to “reassure” and when to “refer”)
GENERAL INTRODUCTION:
• Torsional and angular malalignment are the
most common musculoskeletal complaints
encountered by pediatricians and family
physicians
• Parents and family members have great
concern for the child's appearance and gait
• Spontaneous resolution of these problems is
the norm and the primary care provider can, in
most cases, treat these with careful observation
• Referral to Orthopedic surgeon only when
deformity is severe
NATURAL HISTORY:
During gestation, the lower limb internally rotates,
bringing the great toe to the mid line.
External rotation then occurs in the femur and tibia
throughout the remainder of development to skeletal
maturity.
Some may have a familial tendency and others are
attributable to intrauterine positioning.
NORMAL TORSION OF THE FEMUR:
In the normal adult, the head and neck of the femur are
angulated by 12 degrees relative to the femoral condyles as
noted in the illustration below.
ANTEVERSION: is an increase in the angle of the head and
neck of the femur relative to the frontal plane of the body
This represents a normal femur abnormally positioned in the
acetabulum. The net effect of this positional relationship is an
externally rotated leg.
RETROVERSION: is a decrease in the angle of the head and
neck of the femur relative to the frontal plane of the body.
This represents a normal femur that is abnormally positioned
relative to the acetabulum. The net effect of this positional
relationship is an internally rotated leg.
NB** Average adult has 10° of externally rotated
foot.
- Intoeing of greater than 10° and out-toeing of
more than 30° are considered abnormal, but rarely
with a functional problem.
Complete History
- Pregnancy, birth, and development to rule out pathological
causes for the deformity.
- Type of deformity, onset, progression, and prior treatment.
- Parents concerns regarding future gait, function, and cosmesis
abnormality.
- Family history of musculoskeletal deformities similar and
dissimilar to child's.
Physical Exam:
** Assess from hips to toes
Gait analysis
- check for a heel - toe gait and a limp ( absence of a heel toe gait
may indicate an underlying neurologic disorder such as CP)
Foot progression angle
- the angular difference between the long axis of the foot and the line
of progression the child is moving in
- normal is slightly external ( positive value)
- in toeing of more than 5 degrees is abnormal and is recorded as a
negative value
Imaging
** most rotational problems do not need to be evaluated by xray
** may need to image HIPS if suspect DDH or other congenital or developmental
abnormality
Metatarsus Adductus
Metatarsus
adductus
normal
Tibial Torsion: it is the position of the transmaleolar axis relative to
the coronal plane of the proximal tibia
normal
Medial rotation ( prone hip ROM) Normal = 20 to 60 degrees
- if > than 70 its abnormal
Lateral Rotation - Normal = 30 to 60
- if < 20 its abnormal
- place the child prone to evaluate the hip rotation and tibial torsion
- roughly internal and external rotation of the hip should be equal in the
older child BUT in younger children IR > ER
Metatarsus Adductus: Forefoot is adducted at the tarsal-metatarsal
joint.
- Usually seen shortly after birth and usually resolves with in the
first year of life.
NB **It may be associated with hip dysplasia (10-15%)
- 85% resolve spontaneously.
Treatment:
- Feet that can be actively corrected to neutral do not need any
treatment ( stretching exercises can be given to the parents)
- Feet that can not be possibly corrected need serial casting.
If a child is > I year old and resistant to serial casting Metatarsal
osteotomy and limited medial release may be considered but is
rarely needed
Tibial Torsion:
- Usually presents at 1-2 years of age and resolves by age 3-4 years.
- Operative intervention is seldom required except in severe cases
(supramalleolar osteotomy). Reserved for children with excessive or
asymmetric rotation
*** CRITERIA: indicated if the thigh foot angle remains internally
rotated > 10 or external tibial torsion > 35
Pearls:
- if a child is born with a normal amount of tibial torsion ( often
associated with a calcaneovalgus foot) further external torsion does
not occur
- in kids born with excessive tibial external rotation… spontaneous
correction does not occur
Femoral Anteversion: most common cause of intoeing in kids < 3
- Internal rotation of the femur seen in 3 to 6 year olds that usually
corrects by 10 years of age (F>M).
- Usually symmetric increased medial and decreased lateral rotation is
seen on examination of a child with intoeing and medially rotated
patellae.
-Parents should encourage age child to sit cross-legged.
***NB - Spontaneous resolution occurs in 95% of children
If the child is older than 10 years and has > 90 IR and < 10 ER
femoral derotational osteotomy may be considered for cosmesis only ..
IT DOES NOT CHANGE THE CHILDS FUNCTION!!
****Main complication is the development of a new
rotational problem while trying to treat the first one
Bottom Line: Most cases need only reassurance
VARUS OR VALGUS
Knock-knee (or genu valgum): the legs are bowed
inwards in the standing position. The bowing occurs at or
around the knee, so that on standing with the knees together,
the feet are far apart.
Bowleg (or genu varum): the legs are bowed outwards
in the standing position. The bowing occurs at or around
the knee, so that on standing with the feet together, the
knees are far apart.
Normal Development
Almost all infants have some degree of bowing
There is gradual improvement of the bowing by
18 months and most toddlers do not have
bowing after 2
Knock knees begin to appear between 2 and 3 and
the greatest amount by age 4
Partial straightening occurs at age 6 to 7 at which
time the adult position is reached
Normal evolution: from bowlegs (age 2) to knock-knees (age 3)
to normal valgus (age 5)
2
3
5
History
Family history
Nutritional history
Birth history and milestones
Height and weight chart trends
Does pt have associated pain
Physical Exam
- general ntutritional status and body proportions
- measure the intramalleolar or intrafemoral distance
for your records
- assess for assymetry
Imaging
- single AP xray of both lower extremities ( an
orthoroentnogram without the ruler)
- look for abnormalities of the growth plates such as
widening or growth abnormalities
- can measure the femoral - tibial angle ( 7 degrees of
valgus) and metaphyseal- diaphyseal tibial angle(<
11degrees)
***More detailed work up may be needed under the following
circumstances:
1. If the bowleg or knock-knee appears outside the
age range mentioned above, i.e., bowleg beyond age
3 and knock-knee beyond age 7
2. If it is unilateral
3. If the intercondylar or intermalleolar distance is
more than 6 cm, or is rapidly progressing (more than
11/2 cm within six months)
4. Associated symptoms like pain or limp, or signs of
Blount’s disease, rickets, or other disease syndromes
CAUSES OF VARUS AND VALGUS LEGS
Blount’s disease - a condition of severe bowleg that
occurs usually in obese children who walk early. It is
progressive, and may require surrgery.
Growth disturbance - or epiphyseal dysplasia,
which may be a part of a generalized bone
growth disturbance.
Post-trauma - where injury to the knee causes
damage to the growth plate and abnormal growth
around the knee.
NB*** Metabolic Abnormalities (Rickets etc..) - can cause
growth disturbance of the bones in the body, including the
knee.
Valgus Deformities
Knock-knees can also develop as a result of disease processes.
Most often the precipitating condition has already been diagnosed
and the knock-knees are recognized as a symptom of the condition
Treatment:
The condition is usually not treated. Surgery may be considered
for a condition that persists beyond puberty and in which the
separation between the ankles is approximately 8 cm or greater
You can reassure parents by telling them to take a picture
every 6 months of their child standing to observe the legs
straightening out
Sometimes children reach adolescence but are unhappy that
their 'normal' knock knees have not straightened out enough.
A variety of surgical operations are available to help in these
cases. But such treatment is not foolproof and has to be timed
very carefully.
VARUS DEFORMITIES
Observe the child both lying down, walking and
standing
Physiologic bowing always resolves without treatment.
Bracing is not needed.
****At age 18 months, differentiating physiologic bowing from
tibia vara is important and imaging may be needed.
NB**If a bone metabolic disorder is detected, the underlying
problem should be treated and genu varum usually resolve.
Metaphyseal diaphyseal angle
- this angle is formed by lines between metaphyseal beaks&
perpendicular to the longitudinal axis of the tibia
*** LESS THAN 11 DEGREES IS NORMAL
Metaphyseal dyaphyseal angle > 110
.
Children with a Metaphyseal-Diaphyseal Angle greater
than 11 degrees on a standing radiograph should be
watched!!!
A metaphyseal-diaphyseal angle > than 20 degrees
confirms the diagnosis of Blounts
BUT - angles > than 15 most likely have the disease
Lower Extremity Evolution
Legg Calve Perthes Disease
Definition: - self limiting hip disorder caused by a varying
degree of ischemia and subsequent necrosis of the femoral
head
KEY FEATURES :
- avascular necrosis of nucleus of proximal femoral epiphysis
- abnormal growth of the physis
- and eventual remodeling of regenerated bone are the key
features of this disorder
- usually seen in 4 to 8 yr old boy
- male to female ratio: 4-5 to 1
- increased incidence with a positive family history, low
birth wt, and abnormal pregnancy / delivery
- upto 12% of cases are bilateral but will be at different
stages & are asymmetric
- age is the key to the prognosis - presenting after 8 has a
poor prognosis
Pathogenesis:
- AVN of femoral epiphysis
- articular cartilage is nourished by synovial fluid - continues to
grow
- cartilage columns become distorted with some loss of their
cellular components
- they do not undergoe normal ossification, which results in
excess of calcified cartilage in the primary trabecular bone
- revascularization procedes from peripheral to central
- symptoms occur with subchondral collapse and fracture;
DIFFERENTIAL DIAGNOSIS
bilateral Perthes:
- hypothyroidism
- multiple epiphyseal dyspasia
- spondyloepiphyseal dysplasia tarda
- sickle cell
unilateral Perthes:
- septic arthritis
- sickle cell
- spondyloepiphyseal dysplasia tarda
- gaucher's disease
- transient synovitis
Clinical Presentation:
- pain (often knee pain)
- a limp
Early phase: - limited abduction of hip & limited internal
rotation in both flexion & extension are seen
Late phase - antalgic gait (due to pain
- Trendelenburg gait
Prognosis:
- at least 50% of involved hips do well with no treatment
- many others will do well up until the age of 50 when
anatomic asphericity leads to DJD
Age is the key to prognosis:
- less than 6 years of age: outcome is good
- between 6-8 years of age: results not always
satisfactory with containment
- greater than 9 years of age: questionable benefit from
containment;
- children older than 8-9 yrs at initial onset will have poor
prognosis and may be expected to have significant
symptoms and restricted ROM
Non Operative Treatment:
- principles of treatment are maintenance of ROM &
containment of femoral head through the evolution of healing
of the epiphysis
Containment:
- containment of the femoral head in the normal acetabulum
during repair process may lead to a more sperical head and
congruous joint
- containment is not clearly defined but generally implies 80
% coverage
- prevents extrusion and compression by acetabular rim
- bracing or surgery can achieve containment
Contained “ healed” Perthes
Long Term Consequences:
- coxa magna
- coxa plana
- coxa breva
- hinged abduction: - occurs when an enlarged femoral head
is laterally extruded and impinges against the acetabular rim
when the hip is abducted
Slipped Capital Femoral Epiphysis
ETIOLOGY:
- slip of the captial femoral epiphysis occurs with in a narrow
window of physiologic maturity of the growing child
- arises from mechanical and constitutional factors
- position of growth plate of proximal femur normally
changes from horizontal to to oblique during preadolescence
and adolescence
- wt increase that occurs during adolescent growth spurt
puts extra strain on the growth plate
Clinical Findings:
- it occurs most often in boys 10-17 yrs of age (avg 12 yrs)
- in females, the average age is 12 years
- bilateral involvement in about 1/3 of pts,
NB *** - remember that bilateral involvement is occurs in over
25% of patients
- often within 6 months of the other side, therefore need to
watch for symptoms in opposite hip
- pts may have underlying endocrine disease (such as
hypothyroidism or delayed puberty & bone age)
****- patients who are on or below the 10 percentile for height
at the time of presentation should be screened for
hypothyroidism by measuring thyroid-stimulating hormone
and free thyroxine as a preliminary screening test;
- most common presentation is chronic slip (60 % of cases)
- may cause pain refered to hip, distal medial thigh, or knee
- on exam, look for loss internal rotation, which may be
manifested by observing the extended hip move into external
rotation as hip is flexed
- restricted abduction is found w/ severe slips
Radiographic Findings in SCFE
AP View:
- normal hip shows epiphysis of femoral head projecting above &
lateral to the superior border of the femoral neck
- affected hip shows widening and irregularity of growth plate
Klein's Line: - line drawn along superior border of femoral neck
should cross at least a portion of the femoral epiphysis
- slip must be suspected if a straight line drawn up lateral surface of
femoral neck does not touch the femoral head
KLEIN’S LINE
Lateral View:
***NOTE- AP view may not reveal initial slip, which
explains need for a true lateral lateral which will detect a
posteriorly directed slip
- w/ an acute slip, a frog leg lateral may be contraindicated since it can increase the slip therefore always
order a shoot through lateral
- the most sensitive indicator of a mild slip is the loss of
lateral overhang of the femoral epiphysis;
Classification:
Grade I: displacement of epiphysis less than 30% of width of
femoral neck
Grade II: slip between 30%-60%
Grade III: includes slips of greater than 60% the width of
neck;
SEVERE SCFE
Treatment
- is designed to fuse epiphysis on femoral neck which prevents
further slipping
- this usually involves insertion of one screw into anterior
aspect femoral neck (depending on degree of slip) to enter
center of epiphysis
- this is achieved w/ care to avoid penetration into the hip joint
which can lead to chondrolysis
****No Reduction of the Slip is carried out. The hip is pinned in
situ - to avoid osteonecrosis of the femoral head
GROWTH PLATE CLOSED - no
further risk of slip
Complications:
1) avascular necrosis:
- risk factors: - severity of slip - reduction of slip - location
of pins ( need to avoid anterolateral cortex)
**** risk of AVN is approx 20-50% w/ attempted reduction
vs. less than 5% w/o reduction;
2) Chondrolysis:
- need to monitor for irritation of the hip and
loss of joint space post op