Determinants of generics' market growth

Determinants of generics’ market growth
Bruno Martins Pedro Pita Barros Lu´ıs Catela Nunes
Nova School of Business and Economics
January 2012
Abstract
In the last ten years, the Portuguese governments have made several policies aimed at developing the generic pharmaceutical market, which was nearly nonexistent. In fact, more than fifty measures were taken with this purpose. The goal of the government relates to decreasing the costs with pharmaceuticals both to consumers and to the National Health System, without undermining the quality of the treatment.
The fact that such a high number of measures have been taken suggests that there is no exact solution to boost this market. However, no formal analysis of how effective these were ha s ever been made, which may lead to wrong policymaking, the adoption of policies that have no effect on the market and, therefore, are a waste of resources.
In this paper we propose to study the impact of all the policy measures adopted. Using information for generics’ sales and market share (in retail prices and volume), we estimate a diffusion curve using a parametric approach for the period from January 2000 (January 2003 for market share information) to
October 2010. This curve is estimated using logistic regression in which policy measures are included in the diffusion rate using dummy variables, one for each measure. The logistic function allows us to estimate both the impact of time, accounting for the natural development of the market, and the impact of the measures on the diffusion rate of the generics’ market, creating an additional boost to the diffusion, while taking into account the seasonal effect. Moreover, this method also allows us to estimate two more parameters of interest, namely the upper asymptote, which represents the maximum dimension of the market, and the inflection point that represents the period of maximum growth.
Our results show that, in a general way, the development of the generics’ market has been following its own dynamic, due to the natural flow of time. Indeed, only a small part of the measures had an impact in the market. Moreover, this impact was not always positive as some of them seem to decrease the diffusion rate. In addition, statistically significant effects are more easily found when the market is considered in prices rather than in volume, as expected, since several policies address specifically pharmaceutical drugs
1
prices. Additionally, the generics’ market in terms of value was found to be already reaching its limit while in terms of volume it is still in expansion.
All in all, there is no single policy measure that has an unquestionable impact on the generics’ markets.
Nevertheless, the large numbers of measures taken by governments in the last ten years do not seem to be fulfilling its objective.
1 Introduction
A generic pharmaceutical drug can only be sold after having its legal patent time expired. By definition, it contains the same active ingredients and is bioequivalent to the original brand. Bioequivalence means that it has to release the active ingredient at the same speed and amount than its branded counterpart.
In the last ten years, the successive Portuguese governments have been adopting policy measures aiming at promoting the market for generics. In fact, it has been included as one of the objectives for the national drug
To the Government, using these medicines has the advantage of decreasing the public expenditure with pharmaceuticals and improving the financial sustainability of the National Health System (NHS), since, typically, generic prices are lower than those of brand drugs. Consumers gain as well by using generic in the sense that they can use a medicine which serves for the same therapeutic purpose at a lower price, without undermining the quality of the treatment. Adoption of generics is, then, a win-win situation for governments and consumers.
In the beginning of the 21st century, the generics’ market was nearly nonexistent. Since then, at least fifty-six policy measures were adopted with the purpose of expanding it. The fact that such a high number of policies were taken suggests that there is no right solution to boost the market. However, no formal analysis of how effective these were has ever been made, which may lead to wrong policymaking. The adoption of policies that have no effect on the market is a waste of resources.
This paper aims at studying the impact of the policy measures adopted in the expansion of the market for generics.
The market will be defined as sales and market share.
In the case of generic expansion, however, success should not be thought only in terms of these variables. It is important as well to study the impact on prices, of both brand drugs and generics. Even so, several policies aim specifically at increasing the generics’ market share and, therefore, this will be the main criterion to assess the success of the generic market penetration. Furthermore, we consider only as successful measures those which had, indeed, statistical impact on the diffusion of the generics’ market. We do not intend to assess the costs and benefits of each measure nor if they are desirable from the society point of view. We assess only if a given objective (market
1
Available at http://www.infarmed.pt/portal/page/portal/INFARMED/PERGUNTAS_FREQUENTES/MEDICAMENTOS_USO_HUMANO/
MUH_POLITICA_MEDICAMENTO
2
share or sales) is reached. The desirability of the objective is not assessed as well.
We characterise the market by the following variables, which will be the subject of study:
• Total value of generics’ sales, current prices;
• Total value of generics’ sales, January 2001 prices;
• Market share of generics’ sales to total pharmaceuticals, in value;
• Generics’ sales, in number of packages;
• Market share of generic packages to total pharmaceutical packages.
The last two variables give us a proxy for the quantity sold in the market. We acknowledge that it is not a perfect representation since it depends on the number of units contained in each package and on the adequacy of the size to the therapeutic necessity. Moreover, some consumers may not be using the full contents of the package and may be wasting some resources. Therefore, a package sold has no direct translation to the quantity of medicine sold or used.
Our methodology is, by design, optimistic. In case there is some bias in our estimates, it will be positive, meaning that we are more likely to find policy measures with a significant impact.
We may, then, be overestimating the number of measures with a significant impact. However, our results show that there are a very limited number of policies that had, in fact, some impact on the market. Therefore, the eventual positive bias does not change the conclusion that most policies failed to statistically affect the diffusion rate of the generics’ market.
Overall, our results show that the development of the generics’ market has been following its own dynamic, due to the natural flow of time. Indeed, only a small part of the measures had an impact on the market.
Moreover, this impact is not always positive as some of them seem to decrease the diffusion rate. In addition, statistically significant effects are more easily found when the market is considered in prices rather than in volume. This is expected, since several policies address specifically pharmaceutical drugs prices. Additionally, the generics’ market in terms of value is found to be already reaching its limit while in terms of volume it is still in expansion.
2 Data and Methodology
We study the generics’ market for the period between January 2000 and October 2010. For the variables defined in terms of sales, the analysis starts in January 2000 while in the variables defined as market shares the analysis starts only in January 2003. Data regarding the generics’ market was collected from the INFARMED,
3
I.P. website, which is publicly available. Consumer Price Index data was gathered from Banco de Portugal.
Media coverage was made available through the Pfizer press review platform, with data from November 2008 to December 2010.
the data, which is traditionally used to estimate diffusion curves. We define it as:
K y =
1 + exp { ( − b
1
+ b
2
D t
)( t − a ) }
(1)
Where y our dependent variable (sales or market share), K the upper asymptote, which represents the maximum dimension of the market, t is time (monthly), a the inflection point, which represents the month of maximum growth, b
1 and b
2 are parameters for the diffusion rate, b
1 being the diffusion rate due to the natural flow of time while b
2 concerns the policy measure, and Dt is a dummy variable which takes the value 0 for the months prior to the policy adoption and 1 for the period afterwards. In case the policy had a positive effect in the generics’ diffusion rate, b
2
> 0. If the impact is negative, then b
2
< 0. It has no statistical impact if b
2
= 0.
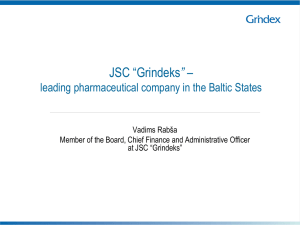
Figure 1: The effect of a structural break in the diffusion rate
Note, however, that if a policy measure does have an impact, the transition to the “new” diffusion curve
(with diffusion rate b
∗
= b
1
+ b
2
) is not smooth. In the month the adoption takes place, a jump will occur in
the direction of the jump depends not only on the sign of the parameter b
2 but also on the point in time
parameters b
2 and a .
4
Table 1: Relation between the inflection point and the coefficient b
2 t < a t > a b
2
> 0 Negative jump Positive jump b
2
< 0 Positive jump Negative jump
Note: t < a refers to the period before the inflection point, while t > a refers to the period after.
Basically, before the inflection point the direction of the jump is contrary to the parameter b
2
, while after that point the estimated curve jumps in the same direction as the impact on the diffusion rate. This interesting aspect happens because, when comparing two different diffusion curves that are distinct only in the diffusion rate, the one with the higher parameter will be below the other before the inflection point and above it after this point. Although counter intuitive at first, this result may be interpreted in the following way: In order for the market growth to be more concentrated over fewer months, it has to drop at some point, given that its maximum dimension is constant.
The interpretation of the coefficients should not be done, therefore, independently from the point in the diffusion curve at the time the policy was taken. Furthermore, the policy impact may be analysed differently depending on the time horizon we are considering. In terms of the instant effect, it is seen by the direction of the jump. Concerning the impact on the diffusion spread along time, it is seen by the coefficient b
2
.
The clear presence of heteroscedasticity motivates us to use some data series in logarithmic form, thus obtaining a growth curve instead of a diffusion curve. The impact is given in relative terms, rather than absolute terms. It may happen that some policies do not have an impact in absolute terms but do have in relative terms, and vice-versa. When no logarithmic is used and there is evidence of heteroscedasticity, we use robust standard-errors. Seasonality is also tested and taken into account, when necessary.
A potential source of bias in our estimates is the effect of news disclosure by the mass media. New policy measures receive, usually, some media coverage, which introduces uncertainty on whether the impact on the generics’ market is due to the policy itself or the spread of information coming from the news. It is necessary, then, to take into account these sources of information. We use three different media sources newspapers, television and radio using as independent variables the number of news released by each (as well as the aggregate) in the last two months. We choose to use two months in order to capture a higher number of
develop on this particular subject, by separating news disclosure between those that refer to policy adoption and those that do not.
At the individual level, the mass media information disclosure does not have an impact on our quantity variables, and therefore they will not be included in our regressions. The variables in prices, though, seem
5
to be influenced by these sources of information and as such, we include them in our analysis.
The breakdown of our methodology follows:
1. Each policy measure is first tested individually against the data series;
2. All policies with an individually statistically significant impact are tested aggregately against each data series. Moreover, we add the impact of media news disclosure.
We follow this methodological path twice per data series, first with a 5% significance level for the hypothesis tests and then with 10%. This choice of significance level allows us to be more permissive with the significance of each policy impact.
Some policies have been simultaneously adopted in the same month. This represents a drawback on this methodology, as it is not able to discern the individual impact of each policy. Only their aggregate effect is observed.
3 Empirical results
A simple analysis of the market variables across time allows us to take some interesting conclusions.
The generics’ market was nearly non-existent before mid-2001. Only then it started to develop, though slowly at first, but eventually picking up its pace until halfway of the decade. From then on, the growth clearly slowed down, until it halted, or even began to decrease, by 2008. This seems to be the story independently of the variables used in terms of prices. The quantity variables, however, still maintain their rising trend.
In the sales variables the variance of the data towards the trend increases with time (presence of heterocedasticity), bringing additional noise and making our estimates less reliable. Nevertheless, this also the most interesting period. We find some outliers in the data. The first one appears in September and October, 2008, when the series plunges in the former month and soars in the latter. This outlier represents a consumer anticipation effect towards government policies. More specifically, in October 2008 policy measure was adopted that reduced generic drugs’ prices (those exceeding 5 Euros) by 30%. In fact, this measure was published in August of the same year. Therefore, the exceptional negative variation in September represents the consumers’ decision of postponing the consumption of drugs to October in order to take advantage of lower prices.
The second outlier, detected mainly in the package sales, appears in September 2010, when it value rises suddenly above the trend. Although not as obvious as the previous one, this outlier may also represent an anticipation effect of a policy that decreases government’s coverage, published in October 2010, to be adopted in 2011. This measure had already been announced by the media before its publishing in the Di´
6
da Rep´ , confirming it as a reason for the outlier. The fact that the outlier shows only in one month may be due to a lower reduction in coverage than expected, annulling the effect after it had been published.
Note, however, that at the same time, another policy aimed at lowering drug prices, which should have the opposite effect on the market. Nevertheless, according to the calculations made by the media, it was announced that the coverage reduction effect would be stronger, making generic drugs overall more expensive.
Another explanation for this outlier may be one policy measure, adopted in October 2010, which rearranges pharmaceutical categories for different coverage. This measure can explain the outlier since it may have changed the NHS coverage in several drugs.
3.1
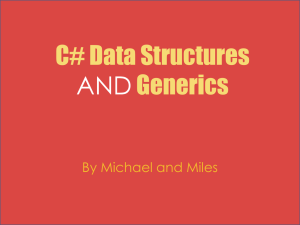
Development of total value of generics’ sales, current prices
Figure 2: Development of total value of generics’ sales, current prices
The results show that, except in a single case in 2000 (where it is found a negative effect in the growth rate), changes to the coverage regime and on the price-definition rules do not seem to have a significant and permanent impact on the total value of generics sales.
Governmental increases in pharmaceutical prices appear to have a positive impact on the growth rate.
The first increase, occurring in December 2001, raised it by 0.19 percentage points in the growth rate while the second, in January 2003, increased it by 0.8p.p. This result may reflect a mechanical effect of accounting due to the variation in prices and may not be a sign of a truly expansion of the generics’ market. A careful look into the progress of the market in terms of quantity is necessary in order to understand more deeply the effect of these price variations.
7
Price reductions of 6% in all pharmaceuticals (September 2005 and January 2007) do not have a statistical impact. Nonetheless, the 30% cut in generics’ prices in October 2008 had a negative impact on the growth rate with magnitude approximately of 0.07p.p. Two reasons may explain this finding. First, the 6% cuts were common to all pharmaceutical, which does not modify relative prices and, as such, should not change consumers’ choice between generics and branded drugs. Second, patients can simply react more intensively to greater cuts in prices, such that a 6% cut is not enough to have a significant response. Note also those prices variations may change total expenditure, but do not change necessarily the underlying growth rate
(the growth is only modified in the moment that they take place).
The market liberalization of over-the-counter (OTC) drugs covered by the NHS in 2007 had a negative impact of 0.3p.p. Typically, branded drugs are more widely used. Therefore, the liberalization may have had a greater effect in these types of pharmaceuticals, which should explain why the impact on generics was negative. Alternatively, sales may have been driven to outside of pharmacies, reducing, as a by-product, the growth of generics’ market.
The aggregate media disclosure does not appear to have an overall impact, but in one equation the impact of newspapers was negative. Nonetheless, the newspapers media impact is not significant enough to make the aggregate effect stand out, though it is significant at the individual level.
Expanding the analysis to the 10% significance level gives us additional results.
In this case, price reductions of 6% do seem to have an impact, although of unclear sign (possibly due to other measures occurring at September 2005). The use of the reference pricing scheme in the ADSE (civil servants) subsystem, starting in March 2004, had a positive effect in the growth rate.
The number of homogeneous groups, defined by governmental law, does not appear to have a statistically significant impact, except when analysed jointly with the media news and with a 10% significance level, where it had a negative impact on the growth rate.
In terms of the market maximum dimension, our estimates point at approximately 55.5 million Euros, not far from its current value.
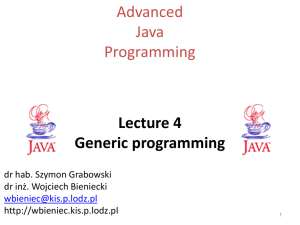
3.2
Development of total value of generics sales, January 2001 prices
The data analysed in January 2001 prices shows a very similar pattern to the one in current prices, as shown
number of homogeneous groups do not seem to have an impact as well. Nevertheless, and contrary to the data in current prices, OTCs liberalization had no impact in this case.
Expanding the analysis to a 10% significance level does not give new results and validates the above-
8
Figure 3: Development of total value of generics’ sales Structural breaks
Figure 4: Development of total value of generics sales, January 2001 prices mentioned ones.
The market maximum dimension of this series was estimated at around 45.2 million Euros, at January
2001 prices. In any of the total sales estimations, in current or constant prices, the market appears to be reaching its maximum value of penetration, since growth rates have been decreasing significantly.
9
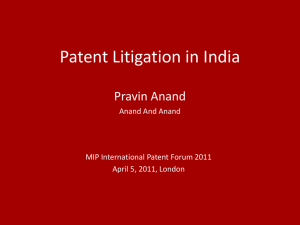
Figure 5: Development of total value of generics’ sales, January 2001 prices Structural breaks
Figure 6: Development of the market share of generics, in value Structural breaks
3.3
Development of the market share of generics’ sales to total pharmaceuticals, in value
This series was analysed in levels since there was no evidence of heteroscedasticity, and its results are reported
in Table 5. Some of them are similar to the total value of sales.
Policy measures reducing the price of all drugs by 6% do not have a statistical impact (as it is expected, since these measures affect both the numerator and denominator of the market share in the same proportion) while reduction of 30% in the generics price negatively affect the market share diffusion by 2.3p.p/month. This
10
may be simply an accounting consequence. Reducing generics’ price implies a reduction in its market share, other things constant. Nonetheless, a lower price should produce an increase in the consumption of generic drugs, for two reasons. First, patients may consume a higher quantity of generics, replacing brand drugs’ consumption (intensive adjustment). Second, new consumers may enter the market for generics (extensive adjustment). The increase in consumption would be dominant if the growth rate of the number of generic drugs sold (packages) had increased. In the absence of this increase, as shown infra, it is not possible to distinguish each of these potential effects. An additional one may also occur. Such a strong price decrease reduces the incentives for pharmaceutical companies to promote generics’ consumption. The information comprised in this type of data does not allow discriminating the role of each of these elements. The first two effects may be captured through the analysis of the market share in terms of quantity (packages sold), and as such, we shall return to this subject later on. In any case, for all the above-mentioned reasons, it is reasonable to conclude that demand price elasticity of generics is below the unity in aggregate terms.
Results show also that changes to the coverage regime and the number of homogenous groups do not have a significant impact on the generics’ market share in value.
It was found a negative impact of the mass media, when the total number of news released in aggregate by the press, television and radio was included in the analysis. Note that the fact that the impact was negative depends ultimately on the type and contents of the disclosed information.
The use of the reference pricing system for the NHS coverage in its subsystems has a positive impact on the market share diffusion, of about 1.4 p.p. per month. Remember that an increase of the diffusion rate
2003. A 10% significance level does confirm the above-mentioned hypothesis, by showing the same positive effect for the ADSE (civil servants) subsystem. Moreover, there is a set of three simultaneously measures that had a negative impact on the diffusion, though we are not able to disentangle each one’s effect. According to our estimates, the market share, in value, is reaching its limit of 19.45%, given the historical background.
3.4
Development of generics’ sales, in number of packages
The evolution of generic packages sold is the dataset most sensitive to the type of analysis performed conclusions do change significantly if we consider levels or logarithms. This means that there are several policy measures that may have a significant impact in absolute terms, but not in relative terms, and vice-
versa. The results can be found in Table 6.
In relative terms, that is, in logarithms, we find that the obligation of the prescriber to mention the
11
International Non-proprietary Name (INN) of the drug had a positive impact on the growth rate of the market. This policy was adopted in September 2000. Nevertheless, since we find no impact on the market share in value, it is likely that there was a shift towards cheaper generics. Graphically, this impact is captured by means of a drop of the diffusion curve, in order to allow for higher growth rates.
The price increase in December 2001 and January 2003 appears to have had a positive impact on the growth rate. Note, however, that the second increase coincides with a measure that forces physicians to inform patients of the existence of a generic alternative, meaning that the positive effect found in 2003 may have come from this measure. We found a quantity reaction to price variations, though of opposite direction to the usually found in economic analysis. Nevertheless, in this particular market, the quantity consumed does not depend only on consumer choice, but also on the physicians’ decisions and advertising campaigns towards generics. The adjustment of these agents may have been relevant for the development of this market.
More specifically, the element of information disclosure towards consumers may have produced an effect that compensated the one created by price variations. Moreover, in 2001 and 2003, the generics market was still in the very beginning. It is natural that, at this stage, the market expansion effect due to higher information available exceeds the reduction in consumption due to an increase in prices.
This interpretation suggests that the increasing coverage during the early stage of the market was less relevant than either letting prices be relatively higher, stimulating pharmaceutical industries to enter the market, or making generics information widely available to consumers.
The reference pricing system, adopted in March 2003, had a negative impact on the generics growth rate.
of total pharmaceutical sales and stimulated price reductions much more striking in branded pharmaceuticals than in generics. In turn, this increases the relative prices of generics making them less appealing compared
to branded products thus leading to a lower growth rate of generics.
In absolute terms, instead of using logarithms, we obtain some similar results but also distinct ones. The number of homogeneous groups has a positive effect in the diffusion rate (with a 10% significance level). That is, the enlargement of the drugs for which the reference pricing system is applied contributed positively for the development of the market.
A set of three measures that were taken at the same time, January 2005, appear to have a negative impact of around 0.03p.p per month: (i) The redefinition of pharmaceutical groups according to a new classification;
(ii) New rules for package dimension of pharmaceuticals covered by the NHS; (iii) application of the reference pricing system to coverage in ADMG (health subsystem for national republican guards) and SAD (health subsystem for police agents).
2
Note that a price decrease is considered as a beneficial effect. The generics market share, however, is not the suitable data to capture it.
12
Figure 7: Development of generics’ sales, in number of packages Structural breaks
Remember that the interpretation of the coefficients must have into account the point on the curve at the time of adoption. Whenever it is in the early stage of the curve, a reduction of the diffusion rate is associated with an upward shift in the curve.
It is not clear the mechanism and the relative importance of each of these measures for the negative impact found. The fact they occurred at the same time makes it impossible to discriminate each individual effect, given the information available. Regarding the market maximum dimension, we found a limit ranging
Figure 8: Development of generics’ sales, in number of packages Structural breaks from 4.4 to 4.8 million packages, depending on whether we use logarithms or absolute value.
13
3.5
Market share of generics’ packages to total pharmaceutical packages
Figure 9: Market share of generics’ packages to total pharmaceutical packages Structural breaks
The analysis of the market share in packages concludes that almost all measures did not have an impact
level considered, we find that only the set of three measures adopted in 2005, the same as in the previous case, have had a negative impact on the diffusion rate of 1.09p.p. per month.
From the above-mentioned three measures, it is likely that the effect has come from the one related to the size of packages. This measure was adopted in order to reduce the waste produced by the lack of fit between the number of units contained in each package and therapeutic needs. As such, the new size rules aimed at improving the rationing of pharmaceuticals through a better adequacy between size of packages and patients’ needs.
Moreover, this data series appears to have a behaviour such that, when fit to the diffusion curve, the diffusion rate is considerably lower than the other series. In fact, it seems almost linear. According to our estimates, the inflection point occurred only in November 2007, while in the other series it occurred around
2003 and 2004. Therefore, the series is still far away from its upper limit, estimated at 36.66%, but being highly uncertain.
Our findings, while not being particularly interesting, should be interpreted while understanding that our measure of quantity is rather limited. The number of packages does not take into account differences in the dimension of each package (it would be more appropriate use DDD doses dirias definidas (ingles?) and even that makes an implicit comparison between therapeutics, which is discussable). It is not surprising, therefore, that the market share in packages has limited capability of grasping any changes in the market
14
functioning resulting from policy measures.
4 Conclusion
In the last ten years, the successive Portuguese governments have been adopting policy measures aiming at promoting the market for generics. From a set of more than twenty measures, not even half of them had a statistically significant impact in the data that was analysed. There is no single policy that we can say that affects globally the market for generics. However, it is possible to specify some measures that somewhat systematically affected the market, either in value or in quantity.
Policy measures were found to be more likely to have impact in data defined in value than in volume and, in some cases, the direction of the impact was negative, decreasing the diffusion rate of sales. However, it is not surprising that it is easier to find effects in the data defined in value since several policy measures aim specifically at pharmaceutical drug prices (even due to the mechanical method of computing this type of data).
Though price reductions of 6% in all pharmaceuticals did not have impact in any data, the reduction in generic prices of 30% had a negative impact in all data defined in value. However, the effect was only in prices, since that no impact was found quantity-wise, as conveyed by the data defined in packages. This means that patients are not sensitive to generic prices, that is to say, the own-price demand elasticity is lower than the unity and the effect in the expenditure is mostly mechanical. Note however that although there was no effect on the diffusion rate, there was an anticipation effect, as seen by the outlier. That is, the measure did not change the dynamics of the market, but it had a very large impact in the moment it was adopted, but with a counter-reaction in the following month of opposite direction, making the overall effect nearly zero.
In the market defined in volume, there is no policy measure that had an indisputable impact, as already mentioned. Nevertheless, we stress two measures whose impact was somewhat more consistent in our different regressions. The first one is the obligation of the prescribing physicians to indicate the INN of the pharmaceutical and to notify the existence of the generic counterpart and the same obligation by pharmaceutical workers. It seems to imply that the increase of information available to patients regarding the existence of generics does impact its consumption. The second is the set of three measures taken at the same time already discussed, from which we cannot separate the statistical effect attributed to each one individually. However, the policy that makes more sense to have the impact is the definition of new rules to the packages dimension.
All in all, considering that the Government’s objective is to promote the use of generics in terms of consumption (measured by quantity) and not in terms of value and that the analysis was optimistic, this objective is not being fulfilled.
15
The growth in the market for generics has followed mainly its own dynamic, while public policies had little effect, or, at least, not immediately strong enough for it to be clearly visible.
It is worth noticing that the generics’ market, relative to the total pharmaceutical market, is reaching a stability stage, even in the presence of mechanisms whose objective is to induce competition between firms.
One can speculate that the policies aimed at increasing the appeal for generics that were carried out in the early stages, such as the entering price or the extra coverage, eventually led to a comfortable life for generics, with little competition among themselves.
This possibility may be weakened due to the reaction of branded drug producers to decrease their prices, which take away some of the room for the generics growth. However, this effect should not be dominant since the decrease in branded prices was not followed by a decrease in generics prices, for drugs competing in the
same market. (See Portela, 2009).
One of the most debated issues in the last decade regarding the generics market was the existence of a market share in value higher than in quantity. This relation, apparently turned around recently, suggests that generic prices in Portugal are higher, on average, that the remaining products sold in pharmacies.
The reason for this feature of the Portuguese market is not entirely clear. In the early stage, the development of the generics market was achieved through higher generic prices and higher coverage by the NHS.
The initial objective was to attract generic producers to operate in the Portuguese market. After this initial boost, it would be desirable to stimulate competition between generic producers. However, for reasons that are far from clear, competition has not been developing as desired.
The first reason, and probably the main one, relates to the encouraging conditions that generic producers encountered, which created focal points for prices, such that no producer has an incentive to decrease its price while others do not. Thus, there is no individual incentive to engage in price wars.
The second reason may have to do with the attractiveness of the Portuguese market, which may attract only generics of higher value, being the average composition of generics different across countries. In this case, the comparison of generic prices should be done product by product, and not through the average value of generics, which is affected by the set of products available in each country.
survey of a Portuguese sample, find that from 2001 to 2008 there is an increase in the number of respondents that accepts well the prescription of generics (ver novo estudo da Carlota quintal?). The mistrust regarding generic quality is nearly residual, though it exists ever since the beginning of the market (only 2.8% lacked trust in the quality of generics in 2001, against 2.3% in 2008).
All things considered, the crucial elements for the development of generic consumption deal with physicians decision to prescribe (given the role of trust between doctors and patients) and with the economic advantage
16
of generics, which may be taken into account by physicians by considering the economic situation of the patient in the moment of prescription.
In the context of the Portuguese national drug policy, and considering the policy measures associated with reduction in pharmaceutical drug prices, promotion of generics and promotion of the rational use of drugs and the objective of guarantee the sustainability of the NHS, our results point to a moderate success: generic consumption did increase, though independently of the price policies adopted. Actions of information disclosure and persuasion to its use were more relevant.
Administrative price reductions were the main source of the decrease in prices. These last years show a stabilization of generics share to total pharmaceuticals. The notion of moderate success is due to some measures that contributed to the expansion of generics, though the effects of many other measures fall short of what was proposed.
References
Pedro Pita Barros.
Economia da sa´ . Almedina, Coimbra, 2009.
Pedro Pita Barros and Luis Catela Nunes. The impact of pharmaceutical policy measures: An endogenous structural-break approach.
Social Science & Medicine , 71(3):440–450, August 2010. URL http://ideas.
repec.org/a/eee/socmed/v71y2010i3p440-450.html
.
Pedro Pita Barros and Lu´ıs Catela Nunes. 10 anos de Poltica do Medicamento em Portugal, 2011.
ao portuguesa perante as prescri¸ oes m´ Imprensa de Ciˆ ,
2009.
Maria da Concei¸ ao Portela.
Regimes de comparticipac˜ cos de referˆ . PhD thesis, Escola Nacional de Sa´
Universidade nova de lisboa, 2009.
A List of measures
Table 2: List of measures
17
ID
Publish
Date
Date of effect
Legal document
Content Valores
1
08-08-2000
2
01-09-2000
3
05-09-2000
4
07-06-2001
5
14-11-2001
6
07-03-2002
7
02-12-2002
08-09-2000
Law 14/2000
Obligation of physician to prescribe by
INN Obligation of pharmaceutical worker to notify to the patient the existence of the cheapest generic
1 between
2000m8 e
2002m12
02-09-2000
Law-Decree
205/2000
New class of NHS coverage Extra coverage for low-income elderly Extra coverage for generics (10% more)
06-09-2000
Ordinance
713/2000
Price Rules for OTCs Profit margins
1 between
2000m9 e
2005m8
1 between
2000m9 e
2005m8
08-06-2001
Ordinance
577/2001
Generic prices must be, at least, 35% lower then the branded pharmaceutical Profit margins
1 between
2001m6 e
2007m3
01-12-2001
Ordinance
1279/2001
Govermental price increase (2 to 3% depending on its price)
1 since
2001m12
08-04-2002
Despacho n.
7145/2002, 7 de Maro
Rules for savings generated in hospitals and primary care centers due to presciption by INN
1 between2002m4 e 2003m1
01-01-2003
Law-Decree
271/2002
. Obligation of physician and pharmaceutical worker to notify to the patient of the existence of the cheapest generic covered by the NHS;
1 since
2003m1
18
8
02-12-2002
9
05-12-2002
10
05-12-2002
11
13-12-2002
12
23-01-2003
13
01-09-2003
01-03-2003
Law-Decree
270/2002
Establishes the reference pricing system for coverage purposes. The reference price in each homogeneous group of pharmaceutical products is determined by the highest generic price. Extra 25% coverage of the reference price for patients under the specia coverage regime
Establishes the list of homogeneous groups
06-12-2002
Despacho conjunto n.
865-A/2002, de 5 de
Dezembro
01-01-2003
Ordinance
1492-A/2002
Govermental price increase (1.5 or 5% depending on its price)
1 between
2003m3 e
2010m5
1 since
2003m1
04-01-2003
Deliberao n.
4/2003, de
13 de
Dezembro de
2002
Approves the list of homogeneous groups
24-01-2003
Despacho n.
1389/2003, de 6 de
Janeiro
. Revoga o despacho n. 7145/2002, de
7 de Maro
02-09-2003
Ordinance
914/2003
Establishes that new generic products cannot enter the market with a price above the reference price
1 between
2003m9 e
2007m3
19
14
27-09-2003
15
11-10-2003
16
06-02-2004
17
23-02-2004
18
10-04-2004
19
20-04-2004
20
26-05-2004
21
21-12-2004
22
21-12-2004
28-09-2003
Law-Decree
234/2003
Applies the reference pricing system to coverage to the NHS subsystems
1 since
2003m10
12-10-2003
Law-Decree
249/2003
. Facilita a passagem a medicamentos genricos de especialidades farmacuticas j existentes no mercado
1 between
2003m10 e
2006m8
01-01-2004
01-03-2004
Law-Decree
31/2004
Extends the extra 25% coverage applied in the Law-Decree 270/2002 until 31-12-2004
Ordinance
172/2004
Applies the reference pricing system to coverage to the ADSE subsytem
1 since
2004m3
11-04-2004
Law-Decree
81/2004
Establishes that updates in homogeneous groups composition and reference price is taken every three months
Deliberao n.
669/2004, de
26 de Maro
Updates the list of homogeneous groups
01-01-2005
22-12-2004
22-12-2004
Ordinance
561/2004
Applies the reference pricing system to coverage to the ADMG and SAD subsytems
Ordinance
1474/2004
Ordinance
1471/2004
Redefines pharmaceutical producst groups according to a new classification. Does not changes coverage between groups or products
Establishes new rules for packages dimension
1 since
2005m1
1 between
2005m1 e
2010m9
1 since
2005m1
20
23
18-01-2005
24
26-01-2005
25
15-03-2005
26
27-07-2005
27
11-08-2005
28
16-08-2005
29
03-01-2006
30
10-02-2006
01-01-2005
Deliberao n.
53/2005, 13 de Dezembro
Updates the list of homogeneous groups
01-01-2005
Law-Decree
23/2005
01-04-2005
Despacho conjunto n.
358/2005, 15 de Maro
Extends the extra 25% coverage applied in the Law-Decree 270/2002 until 31-12-2004
Updates the list of homogeneous groups
15-09-2005
Ordinance
618-A/2005
Price reduction of 6% in all pharmaceuticals Defines profit margins
10-09-2005
Law-Decree
129/2005
Reduction in coverage for pharmaceuticals in Group A Ends extra 10% coverage in generics gives extra 5% coverage for pharmaceuticals in group A for low-income pensioneers.
15-09-2005
Law-Decree
134/2005
Liberalizes OTC sales (expect those under goverment coverage)
01-01-2006
Law-Decree
6/2006
Extends the extra 25% coverage applied in the Law-Decree 270/2002 until 31-12-2004
01-01-2006
Protocol
7/2006
Methodology of price definition revised
Objectives of promoting OTC and generics Maximum allowed expenditure growth defined
1 since
2005m9
1 since
2005m9
1 since
2005m9
1 since
2006m1
21
31
26-06-2006
32
04-07-2006
33
29-07-2006
34
30-08-2006
35
29-09-2006
36
29-12-2006
37
29-12-2006
38
05-01-2007
01-07-2006
Despacho n.
15978/2006, de 26 de
Junho
Updates the list of homogeneous groups
01-07-2006
Law-Decree
127/2006
Reduces and extends the extra of 25% coverage to 20% applied in the
Law-Decree 270/2002 until 31-12-2004
01-01-2007
Law
53-A/2006 -
Article 150
1 since
2006m7
31-01-2007
Law
53-A/2006 -
Article 147
Price decrease of 6% in all pharmaceutical under NHS coverage
31-08-2006
Law-Decree
176/2006
Changes the statute of pharmaceutical defines the legal regime for pharmaceuticals
1 between
2006m9 e
2009m7
01-10-2006
Despacho n.
21787/2006, de 29 de
Setembro
Updates the list of homogeneous groups
01-01-2007
Law-Decree
242-A/2006
Extends the extra coverage of 20% applied in the Law-Decree 127/2006
Coverage reduction
1 since
2007m1
31-01-2007
Ordinance
30-B/2007
Price decrease of 6% in all phamaceutical under NHS coverage
1 since
2007m2
22
39
31-01-2007
40
14-03-2007
01-02-2007
Despacho n.
4130/2007, de 31 de
Janeiro
Updates the list of homogeneous groups
15-03-2007
Law-Decree
65/2007
Establishes the international reference pricing regime Establishes price reduction of generics as a function of its market share Defines profit margins
Establishes that generics ought to be
35% lower than the branded counterpart (or 20% if less than 10 euros)
41
19-03-2007 01-05-2007
Ordinance
300-A/2007
Details the rules for Law-decree
65/2007
42
19-03-2007
43
19-06-2007
44
28-12-2007
45
27-06-2008
01-04-2007
Despacho n.
6434/2007, de 19 de
Maro
Updates the list of homogeneous groups
20-06-2007
Law-Decree
238/2007
Liberalizes OTC sales, with no coverage outside pharmacies
01-01-2008
Law-Decree
392-B/2007
Extends the extra coverage of 20% applied in the Law-Decree 127/2006
01-07-2008
Law-Decree
110/2008
Extends the extra coverage of 20% applied in the Law-Decree 127/2006
1 between
2007m5 e
2010m6
1 since
2007m7
23
46
08-08-2008
47
18-12-2008
48
29-05-2009
49
12-06-2009
50
07-08-2009
51
15-01-2010
52
13-05-2010
01-10-2008
Ordinance
1016-A/2008
Price reduction of 30% for all generic above 5-
01-01-2009
Law-Decree
247/2008
Extends the extra coverage of 20% applied in the Law-Decree 127/2006
1 since
2008m10
01-06-2009
Law-Decree
129/2009
Establishes 100% coverage to generics for low-income pensioneers.
1 between
2009m6 e
2010m5
13-06-2009
Ordinance
650/2009
. Extende o regime especial de comparticipao do Estado no preo dos medicamentos aos pensionistas beneficirios da Assistncia na Doena aos Militares das Foras Armadas
(ADM), cujo rendimento total anual no exceda 14 vezes a retribuio mnima mensal garantida (RMMG).
1 since
2009m6
1 since
2009m8
08-08-2009
Law-Decree
182/2009
Simplifies pharmaceuticals imports
01-01-2010
Law-Decree
6/2010
Extends the extra coverage of 20% applied in the Law-Decree 127/2006
01-06-2010
Law-Decree
48-A/2010
Establishes 100% coverage to 5 lowest-price generics for low-income pensioneers. The price of new pharmaceuticals to be covered has to be 5% lower than the lowest-price generic with at least 5% of market share
1 between
2010m6 e
2010m12
24
53
11-06-2010
54
17-09-2010
55
01-10-2010
56
07-10-2010
01-07-2010
Ordinance
312-A/2010
Revises the rules for price defntion of pharmaceuticals
01-10-2010
Ordinance
924-A/2010
Redefines the pharmaceutical grous for coverage
01-01-2011
Law-Decree
106-A/2010
Reduces coverage for Group A to 90%
Reduces coverage for generics to low-income pensioneers to 95%
Redefines the reference price for homogeneous groups (average of the 5 cheapest prices in the market) Defines electronic prescription
15-12-2010
Ordinance
1041-A/2010
Price reduction of 6% in pharmaceuticals under coverage
1 since
2010m7
B Regressions
Table 3: Total value of generics sales, current prices
Date ID log(pvp) a=5%
Separated media impact log(pvp) a=5%
Aggregated media impact log(pvp) a=10%
Separated media impact log(pvp) a=10%
Aggregated media impact
08-09-00 (1)
02-09-00 (2) (3)
01-12-01 (5)
0.0000118
0.00123*
-0.00191*
0.0000296
-0.00000511
0.00000898
0.00111*
-0.00219*
0.00130*
-0.00181*
0.00127*
-0.00190*
25
01-01-03
01-03-03
02-09-03
(7) (10)
(8)
(13)
-0.00893* -0.00875*
0.000144
-0.00800*
-0.000631
-0.00786*
-0.000805
28-09-03
12-10-03
(14)
(15)
0.000115
-0.0000905
-0.000102
-0.000151
-0.000165
0.00135
0.00262
-0.000811
-0.000436
-0.00000866
-0.0000431
0.00000233
-0.00000779
0.00207* 0.00233* 01-03-04 (17)
01-01-05
(21) (22)
(20)
15-09-05
(26) (27)
(28)
0.000813
01-01-06 (30) -0.000367
0.000686
0.000304*
0.000842*
0.000358**
0.00081*
-0.000261
-0.000325
-0.000255
-0.000235
-0.000181
-0.000218
01-07-06
31-01-07
31-01-07
20-06-07
(32)
(33)
(38)
(43)
-0.000329
0.000355
-0.000634
-0.000377*
0.000437
-0.000593
-0.000336
0.000377
-0.000568*
0.000418
-0.000533
-0.000326* -0.000301*
01-10-08
01-06-09
13-06-09
08-08-09
(46)
(48)
(49)
(50)
-0.000719* -0.000719* -0.000695* -0.000692*
0.000357*
-0.000333*
0.000226
-0.000132
0.000651
-0.000267
-0.000236
0.000836
-0.000542
-0.00011
26
Homogeneous groups
-0.000000619
-0.00000235
-0.00000216
-0.00000319
Press news
-0.00000377* -0.00000231
Radio news
0.0000107
0.0000127
TV news
-0.00000401
Total news
-0.000000161
-0.00000562
Inflection point
2003m6 2003m7 2003m6
-4.37E-08
2003m7
* means the coefficient is statistically significant
Table 4: Total value of generics sales, January 2001 prices
Date ID log(deflac) a=5%
Separated media impact log(deflac) a=5%
Aggregated media impact log(deflac) a=10%
Separated media impact log(deflac) a=10%
Aggregated media impact
02-09-00
08-09-00
(2) (3)
(1)
-0.000159
0.000307
01-12-01 (5) -0.00225*
01-01-03 (7) (10) -0.00356*
01-03-03
02-09-03
28-09-03
(8)
(13)
(14)
0.000396
0.0000859
0.00147
-0.000162
0.000307
-0.00226*
-0.00311*
0.000392
0.0000326
27
0.00159
0.000533
0.000746
-0.00173*
-0.00797*
-0.00105
0.000109
0.000659
0.000528
0.000744
-0.00174*
-0.00781*
-0.00102
0.0000846
0.000776
01-07-06
31-01-07
31-01-07
01-05-07
20-06-07
12-10-03 (15) -0.000605
01-03-04 (17)
01-01-05
(21) (22)
(20)
0.00149
-0.00986*
15-09-05
(26) (27)
(28)
0.00103
01-01-06 (30) 0.000339
(32)
(33)
(38)
(41)
(43)
-0.000898
0.00112
-0.00124
-0.000701
0.00175
-0.00886*
0.000957
0.000354
-0.000782
0.00114
-0.00116
-0.000324
0.00166
0.000795
0.0000601
-0.000257
-0.000518
0.000593
-0.000712
0.000182
-0.000326
-0.000363
0.00184
0.00088
0.0000968
-0.000326
-0.000197
01-10-08
01-06-09
08-08-09
(46)
(48)
(50)
-0.000753*
0.00037
-0.000668*
0.000243
-0.000582*
0.000352*
-0.000557*
0.000279
-0.000521
-0.000232
-0.000159
-0.0000336
01-06-10 (52) 0.000557
0.000389
-0.000843
-0.000914
01-07-10 (53) 0.0000348
0.0000964
0.000244
0.00028
Homogeneous groups
0.00000501
Press news
-0.00000368
0.00000168
-0.00000284
-0.00000406
-0.00000187
-0.000232
-0.000469
0.000605
-0.000688
0.000182
-0.000277
28
Radio news
0.000038
0.0000152
TV news
-0.0000189
Total news
-0.00000026
-0.00000727
Inflection point
2005m1 2005m1 2003m7
-8.51E-08
2003m7
* means the coefficient is statistically significant
Table 5: Market share os generic’s sales to total pharmaceuticals, in value
Date ID
Sharepvp a=5%
Separated media impact
Sharepvp a=5%
Aggregated media impact
Sharepvp a=10%
Separated media impact
Sharepvp a=10%
Aggregated media impact
28-09-03 (14)
01-03-04 (17)
01-01-05
(21) (22)
(20)
0.0141*
0.00545
0.0135*
0.0029
0.0170*
0.0398*
-0.0802*
31-01-07
31-01-07
(33)
(38)
0.00174
-0.00038
-0.000803
-0.00187
01-10-08 (46) -0.0234*
Homogeneous groups
-0.0000214
Press news
-0.0000528
-0.0242*
-0.0000142
-0.0294*
0.0000642
-0.000114
0.0178*
0.0370*
-0.0787*
0.000209
-0.00264
-0.0319*
0.0000617
29
Radio news
-0.00232
TV news
0.00123
Total news
-0.0000183*
Inflection point
2005m1 2005m2
* means the coefficient is statistically significant
-0.00186
0.00102
2004m11
-0.0000165*
2004m12
Table 6: Generics’ sales, in number of packages
Date ID
08-09-00 (1)
02-09-00 (2) (3)
08-06-01
01-12-01
08-04-02
(4)
(5)
(6) log(package) log(package) a=5% a=10%
-0.00347*
0.000588
0.00426*
01-01-03 (7) (10)
01-03-03 (8)
0.00232
-0.00284*
02-09-03 (13)
28-09-03
12-10-03
(14)
(15)
-0.00188*
0.00112*
0.00289*
0.00206*
0.00416*
-0.00159* package a=5%
0.00168
-0.000205
-0.0018
-0.00303
-0.00187
0.00113
package a=10%
-0.0130*
0.0239*
0.000124
-0.0398*
-0.00302
0.0045
0.018
-0.01
30
01-03-04 (17)
01-01-05
(21) (22)
(20)
15-09-05
(26) (27)
(28)
0.0000743
01-01-06
01-07-06
(30)
(32)
-0.000634
-0.000732
31-08-06
31-01-07
(34)
(33)
-0.000418
0.00299
0.0000726
-0.000673
-0.000657
-0.000396
0.00271
-0.00114
-0.00316*
-0.0135*
-0.0284*
-0.0333
-0.000859
31-01-07
01-05-07
(38)
(41)
-0.00212
-0.00207
0.000879
20-06-07 (43) -0.000103
Homogeneous groups
-0.00000337
-0.00000177
-0.00000444
Inflection point
0.000308
1998m9 1998m6 2011m7
0.000139*
2005m10
* means the coefficient is statistically significant
Date
01-03-04
Table 7: Market share of generic’s packages
ID
(17)
Sharepackage a=5%
-0.00316
Sharepackage a=10%
-0.00317
31
01-01-05
(21) (22)
(20)
15-09-05
(26) (27)
(28)
01-01-06 (30)
-0.0109*
-0.000254
-0.0109*
-0.000236
-0.0000379
31-08-06 (34) -0.000761
-0.000754
01-05-07 (41)
Homogeneous groups
-0.00092
-0.000916
0.0000129
0.0000129
Inflection point
2007m11
* means the coefficient is statistically significant
2007m11
32