This article was originally published in a journal published by
Elsevier, and the attached copy is provided by Elsevier for the
author’s benefit and for the benefit of the author’s institution, for
non-commercial research and educational use including without
limitation use in instruction at your institution, sending it to specific
colleagues that you know, and providing a copy to your institution’s
administrator.
All other uses, reproduction and distribution, including without
limitation commercial reprints, selling or licensing copies or access,
or posting on open internet sites, your personal or institution’s
website or repository, are prohibited. For exceptions, permission
may be sought for such use through Elsevier’s permissions site at:
http://www.elsevier.com/locate/permissionusematerial
Author's Personal Copy
Manual Therapy 14 (2009) 579–582
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier.com/math
Professional Issue
The convex–concave rule and the lever law
Jochen Schomacher
Dorfstr. 24, CH-8700 Küsnacht ZH, Switzerland
a r t i c l e i n f o
Article history:
Received 11 January 2009
Received in revised form
23 January 2009
Accepted 23 January 2009
1. Introduction
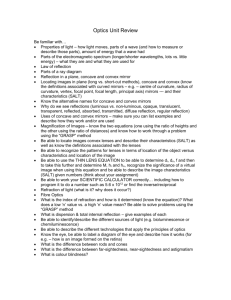
The convex–concave rule is considered an important theory
during treatment decision-making (Kirby et al., 2007). According to
this rule (Fig. 1) the therapist moves a bone with a convex joint
surface opposite to the direction of restricted movement of the
distal aspect of the bone (e.g. the head of humerus inferiorly for
restricted shoulder abduction). However, a concave joint surface is
mobilized in the same direction as the direction of the restricted
bone movement (e.g. the tibia condyles anteriorly for restricted
knee extension) (Kaltenborn, 2002: p 34).
Recent studies are questioning this principle. On 3D reconstructions of helical CT data of 3 asymptomatic shoulders Baeyens
et al. (2000) for example observed a posterior translation of
humeral head during external rotation in 90 abduction. However,
the convex–concave rule predicts an anterior glide for external
rotation. This observation could also be made in 3 symptomatic
shoulders with minor instability (Baeyens et al., 2001). The same
method of 3D reconstructions of helical CT data was used in the
analyses of pro- and supination of the forearm (Baeyens et al.,
2006). It was found for example a posterior translation of the radial
head during supination in the proximal radio-ulnar joint, while the
convex–concave rule predicts anterior gliding of the radial head’s
joint surface on the radial notch of ulna.
Cattrysse et al. (2005) used an electromagnetic tracking device
to study coupled motions of the acromioclavicular, glenohumeral
and humero-ulnar joints on cadavers. With mathematical calculations they deduced intra-articular kinematics which were not
according to the convex–concave principle. Brandt et al. (2007)
found in their literature review inconsistent evidence, poor methodological quality, and heterogeneity of the studies, so that no clear
E-mail address: jochen-schomacher@web.de
1356-689X/$ – see front matter Ó 2009 Elsevier Ltd. All rights reserved.
doi:10.1016/j.math.2009.01.005
conclusion could be drawn on the direction of translation of the
humeral head.
Johnson et al. (2007) evaluated the effect of the gliding mobilization in 20 patients with adhesive capsulitis (frozen shoulder).
Half of the patients were mobilized anteriorly and the other half
posteriorly. They found pain alleviation in both groups, but the
posterior mobilization group had better results in range of motion –
although the convex–concave rule predicts anterior gliding of the
humeral head during external rotation.
The aim of this paper is to explain the mechanics of the convex–
concave rule and then to discuss possible misinterpretations in the
above mentioned studies.
2. Mechanics of the convex–concave rule
During the movement of a bone around an axis
(¼osteokinematics), its joint surface is doing complex movements
described by arthrokinematics (Williams et al., 1989: p 478). The
form of the joint surface has been considered to induce its gliding/
fixated bone
moving bone
Gliding of the joint surface
(= arthrokinematics)
Movement of the distal
bone (= osteokinematics)
fixated bone
moving bone
Direction of the gliding
mobilization
Fig. 1. Convex–concave rule (Kaltenborn, 2002: p 35).
Author's Personal Copy
580
/ Manual Therapy 14 (2009) 579–582
FForce
F Force
F Weight
F Weight
a
F Weight
F Force
b
c
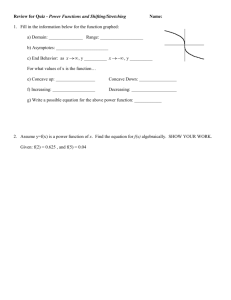
Fig. 2. The three types of levers. (a) lever with two arms: Weight and force are acting on both sides of the axis. Example: hip joint standing on one leg and seen in the frontal plane
(scale of Pauwels). (b) lever with one arm: Weight is acting between axis and force on one side of the axis. Example: metatarsofalangeal joint standing on the forefoot seen in the
sagittal plane. (c) Lever with one arm: Force is acting between axis and weight on one side of the axis. Example: flexion in the ellbow joint seen in the sagittal plane.
sliding movement: a female (¼concave) joint surface glides in the
same direction as the bone movement, while a male (¼convex)
surface is gliding in the opposite direction of the bone movement
(MacConaill and Basmajian, 1977: p 36 and 37; Williams et al., 1989:
483). Kaltenborn (2002: p 34) has described these mechanics in
terms of the convex–concave rule.
The mechanical basis of the convex–concave rule is the lever law.
A lever is a body (mostly a bar) which can be moved around an axis
(Brockhaus, 1993). The bones of the locomotor system represent
such levers which are moved by muscles or weight forces around the
axis of a joint. There are levers with two arms, where weight and
force are acting both sides of the axis (e.g. a seesaw; Fig. 2 a), and
levers with one arm, where weight and force are acting on the same
side of the axis (e.g. a wheelbarrow and a shovel; Fig. 2 b and c).
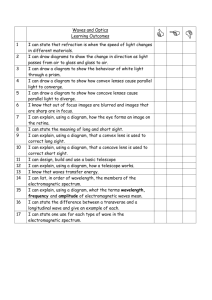
Movement of a bone with a convex joint surface like the
humerus represents movement of a lever with two arms (Fig. 3a).
The axis is roughly in the middle of humeral head. One lever arm is
the shaft of humerus moving cranially during abduction. The other
lever arm is between the axis and the joint surface of humeral head
and is moving caudally during abduction.
When moving a bone with a concave joint surface like the
scapula, the lever system is a lever with only one arm (Fig. 3b). The
axis of motion remains in roughly the middle of the humeral head.
The bone of scapula and its joint surface are moving in the same
direction, because both are on the same side of the axis and
therefore on the same lever.
The convex–concave rule is a simplification of these mechanics
describing the movements of the joint surfaces using their form.
However, there are variations of joint surfaces where this simplification is no longer useful. For example during a cadaver study,
Lazennec et al. (1994) found in 150 proximal tibiofibular joints the
fibular joint surface to be plane in 40%, convex and concave in 57%
and round and convex in 3%. The tibial joint surface was not always
reciprocally formed, as one would expect, but in 55% plane, in 40%
convex and in 5% concave. This illustrates the difficulty in applying
a
humerus moves
scapula is fixated
the convex–concave rule according to the form of the joint surfaces
in this joint. The joint mechanics are determined by the position of
the axis of motion and the type of lever (one or two arms).
Therefore, Lazennec et al. (1994) suppose an axis in the frontal
plane between the lower third and the upper two thirds of the
fibula, which represents a lever with two arms. So when the fibular
malleolus moves posteriorly during dorsal flexion in the ankle, the
head of fibula is moving anteriorly and the other way round
(Lazennec et al., 1994).
3. Discussion: movements of the centre of the humeral and
radial head or of the joint surface
Having the lever law as a mechanical basis, the convex–concave
rule can hardly be contradicted. So why is it questioned in different
studies?
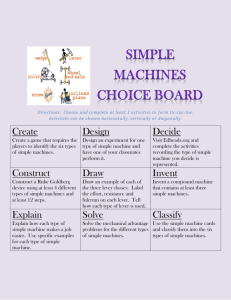
The explanation is a misunderstanding! Baeyens et al. (2000,
2001) described the translation of the centre of the humeral head
during external rotation in 90 abduction. Fig. 4a shows a similar
movement – horizontal abduction – which is easier to represent
graphically. The humerus moves physiologically as a lever with two
arms and therefore its joint surface is gliding anteriorly while the
bone shaft is moving posteriorly – according to the convex rule.
When gliding is restricted, rolling predominates (Kaltenborn,
2002: p 27). Rolling shifts the axis of motion towards the contact
point of the joint surfaces. For simplification this is exaggerated in
Fig. 4b. This transforms the humerus nearly into a lever with one
arm. In this case the joint surface of the humerus is mostly rolling
posteriorly and its anterior gliding is restricted. The centre of the
head of humerus is now moving posteriorly. The observation of
Baeyens et al. (2000, 2001) is, therefore, correct, but they do not
describe the movement of the joint surface as does the convex–
concave rule.
The described shift of the axis of motion happens especially in stiff
joints and it has been known for a long time (Fig. 5; Jordan,1963: p 22).
b
humerus is fixated
scapula moves
Abd.
Abd.
Fig. 3. The lever system applied to abduction in the shoulder joint. (a) Abduction of the shoulder with humerus moving: the convex rule as a lever with two arms. (b) Abduction of
the shoulder with scapula moving: concave rule as a lever with one arm.
Author's Personal Copy
/ Manual Therapy 14 (2009) 579–582
a
581
b
Fig. 4. The lever system applied to horizontal abduction in the shoulder with physiologic and restricted gliding of the humeral joint surface. (a) Horizontal abduction in a horizontal
section: in a physiological joint a lever with two arms exists and the humeral joint surface is gliding anteriorly according to the convex rule. (b) Shift of the axis of motion towards
the contact point of the joint surfaces because of restricted gliding. Humerus is becoming a lever with one arm and the centre of head of humerus is moving posteriorly. Note the
absence of gliding in this extreme example.
The same explanation applies to the study of pro- and supination of Baeyens et al. (2006). In supination the radial head rotates
on its axis. This is a two arm lever system. During supination the
lateral aspect of the radial head moves posteriorly, while its medial
aspect – the articular surface – moves anteriorly on the radial notch
of ulna. This is according to the convex–concave rule! However,
rolling of the joint surface causes posterior displacement of the
centre of the radial head, which was the correct observation of
Baeyens et al. (2006).
The simplification of the convex–concave rule describes only the
gliding of the joint surface of the moving bone. It should be noted
that human joints surfaces not only glide but simultaneously roll
upon the opposite joint surface (Williams et al., 1989: p 483), which
is never fully congruent to the other one (MacConaill and Basmajian, 1977: p 33). In the reasoning model of the convex–concave rule
the axis of motion is considered stationary for simplification.
However, the rolling component in human joints shifts the axis.
This is responsible for the displacement of the centre of the
humeral and radial head observed by Baeyens et al. (2000, 2001,
2006).
Stiff joints are thought to have restricted gliding and predominant rolling between the joint surfaces (Kaltenborn, 2002: p 27).
The cause of this gliding restriction is unclear and may be an
increased articular pressure as a consequence of shortening of the
joint capsule or increased tension in periarticular muscles. Other
causes are possible such as an altered synovial liquid or loosening
of periarticular ligaments or insufficiency of periarticular muscles
as in hypermobile joints. Shortening of the joint capsule and
muscles is also mentioned by Brandt et al. (2007) as a factor
having an influence on arthrokinematic movements. These
authors confuse, like Baeyens et al. (2000, 2001, 2006), the
displacement of the centre of the humeral head with the movement of the joint surface described by the convex–concave rule
(Schomacher, 2008).
The increased external rotation after posterior gliding mobilization in the shoulder joint (Johnson et al., 2007) might be
explained by the frequently observed anterior positional fault of the
humeral head in relation to the acromion (Schomacher, 2007;
Bryde et al., 2005). There was no significant difference between
anterior and posterior gliding mobilization regarding pain (Johnson
et al., 2007). This indicates, that respecting mechanical principles is
seen mainly in mechanical parameters like range of motion, while
for pain relief many techniques might be done – even ignoring joint
mechanics!
Finally, it should be mentioned, that the convex–concave rule
describes gliding in physiological joints. It is valid also in pathological ones in which the physiological gliding becomes restricted.
However, the physiotherapist should not mobilize a pathological
joint according to a rule, but treat pathological clinical findings,
which are in correlation with the patient’s complaints.
axis of
motion
starting
position
adhesions
starting
position
final position
final position
Fig. 5. Extension of the knee with physiological gliding and with restricted gliding due to adhesions. Note the shift of axis of motion (after Jordan 1963: 22).
Author's Personal Copy
582
/ Manual Therapy 14 (2009) 579–582
4. Conclusion
The convex–concave rule, introduced by Kaltenborn into
manual therapy, is a didactic simplification of the lever law, during
rotatory movements of the joints. Movement of a convex bone
corresponds to movement of a lever with two arms (¼convex rule)
and movement of a concave bone to a movement of a lever with
one arm (¼concave rule).
The convex–concave rule describes the movement of a pair of
mating joint surfaces (arthrokinematics) and not the movement of
the bone e.g. the centre of humeral head (osteokinematics), which
is often analyzed in biomechanical research.
In practice it is important not to transfer the gliding direction
from physiological joints to pathological ones for mobilization
without a prior examination. Restricted gliding and the associated
dysfunctions may have different causes. They must be assessed
individually in an examination and the findings must be interpreted in a thorough clinical reasoning process.
Acknowledgements
The author likes to thank Freddy Kaltenborn for revision of the
text and Ola Grimsby for the help with the English language.
References
Baeyens J-P, van Roy P, Clarys JP. Intra-articular kinematics of the normal glenohumeral joint in the late preparatory phase of throwing: Kaltenborn’s rule
revisited. Ergonomics 2000;43(10):1726–37.
Baeyens J-P, van Roy P, de Schepper A, Declercq G, Clarijs J-P. Glenohumeral joint
kinematics related to minor anterior instability of the shoulder at the end of the
late preparatory phase of throwing. Clinical Biomechanics 2001;16:752–7.
Baeyens J-P, van Glabbeek F, Goossens M, Gielen J, van Roy P, Clarys J-P. In vivo 3D
arthrokinematics of the proximal and distal radioulnar joints during active
pronation and supination. Clinical Biomechanics 2006;21:S9–12.
Brandt C, Sole G, Krause MW, Nel M. An evidence-based review on the validity of
the Kaltenborn rule as applied to the glenohumeral joint. Manual Therapy
2007;12(1):3–11.
Brockhaus. Der Brockhaus in fünf Bänden. Mannheim – Leipzig: F.A. Brockhaus;
1993. und 1994.
Bryde D, Freure BJ, Jones L, Werstine M, Briffa NK. Reliability of palpation of
humeral head position in asymptomatic shoulders. Manual Therapy
2005;10(3):191–7.
Cattrysse E, Baeyens J-P, van Roy P, van de Wiele O, Roosens T, Clarys J-P. Intraarticular kinematics of the upper limb joints: a six degrees of freedom study of
coupled motions. Ergonomics 2005;48(11–14):1657–71.
Johnson AJ, Godges JJ, Zimmermann GJ, Ounanian LL. The effect of anterior versus
posterior glide joint mobilization on external rotation range of motion in
patients with shoulder adhesive capsulitis. Journal of Orthopaedic and Sports
Physical Therapy 2007;37(3):88–99.
Jordan HM. Orthopedic appliances. Springfield: Charles C. Thomas Publisher; 1963.
Kaltenborn FM. Manual mobilization of the joints. In: The extremities, vol. I. Oslo
(Norway): Norlis; 2002.
Kirby K, Showalter C, Cook C. Assessment of the importance of glenohumeral
peripheral mechanics by practicing physiotherapists. Physiotherapy Research
International 2007;12(3):136–46.
Lazennec JY, Besnehard J, Cabanal J. L’articulation péronéo-tibiale supérieure, une
anatomie et une physiologie mal connues: Quelques réflexion physiologiques et
thérapeutiques. Annales de Kinésithérapie 1994;21(1):1–5.
MacConaill MA, Basmajian JV. Muscles and movements, a basis for human
kinesiology. Huntington, New York: Robert E. Krieger Publishing Company;
1977.
Schomacher J. Response to: Brandt C, Sole G, Krause MW, Nel M. An evidencebased review on the validity of the Kaltenborn rule as applied to the
glenohumeral joint. Manual Therapy 2007;12(1):3–11. Manual Therapy
2008;13(1):e1–2.
Schomacher J. Letter to the editor in response to: Johnson AJ, Godges JJ, Zimmermann GJ, Ounanian LL. The effect of anterior versus posterior glide joint
mobilization on external rotation range of motion in patients with shoulder
adhesive capsulitis. Journal of Orthopaedic and Sports Physical Therapy
2007;37(7):413 (Authors reply on pp. 414–415).
Williams PL, Warwick R, Dyson M, Bannister LH. Gray’s anatomy. Edinburgh:
Churchill Livingstone; 1989. pp. 476–485.