Lipid Metabolism: Chapter 25 – Sections 25.1
advertisement

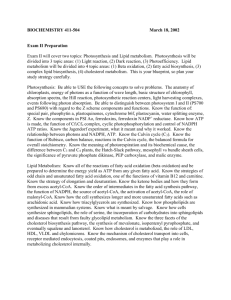
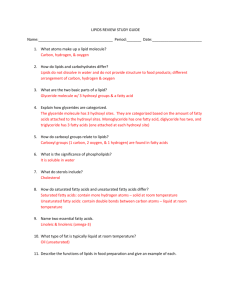
Physiological Chemistry Lipid Metabolism Chapter 25 Digestion • 98% of total dietary lipids are triacyglycerols (fats and oils) • Stomach: – Mostly physical changes take place (i.e., formation of lipid droplets) – high fat meals have a longer transit time through the stomach since it takes longer to “disperse” lipids in this manner – Gastric lipases carry out ~10% hydrolysis Digestion • Small Intestines – As chyme enters the duodenum, intestinal cells secrete cholecystokinin (CCK), which stimulates contraction of the gall bladder and release of bile into the small intestine – bile salts serve to emulsify triacylglcerols, which allows pancreatic lipase to hydrolyze them to two fatty acids and monoacylglycerols, which eventually form “micelles”, which are readily absorbed through intestinal cell membranes Digestion (hydrolysis) of a triacylglycerol A micelle Products of Lipid Digestion • Smaller components – Free fatty acids (short, medium and long chain) – Monoacylglycerols – Phospholipids and lysophospholipids – Free cholesterol – Fat soluble vitamins – Bile acids Absorption • Micelles are absorbed by passive diffusion through the cell membrane of small intestinal cells • Nearly all dietary fat and 50% of dietary cholesterol are absorbed • About 80% of bile acids are reabsorbed Metabolism of Absorbed Lipid • Free fatty acids (FA) absorbed in small intestinal cell: – Short-chained FA go directly into blood and bind to albumin • Transported through portal circulation to liver for “chain elongation” or catabolism – Other FA are re-esterified to triacylglycerols, phospholipids, and cholesterol esters • Newly formed triacylglycerols, cholesterol esters, free cholesterol, and phospholipids are assembled with proteins to form chylomicrons Chylomicrons • Lipoprotein made by small intestinal cells • Move from small intestines to lymphatic system and then to blood stream • Removed from blood by lipoprotein lipases in tissues (mostly adipose and muscle), which break them down to free fatty acids and glycerol before absorbing them to use either as sources of fuel or to store them as triacylglycerols (TAGs) • Appear in blood within 2 hours, peak at about 5-6 hours and are completely cleared in about 10 hours post meal (dependent upon fat content of meal) – May take up to 16 hours Chylomicrons Digestion and Absorption Figure 25.3: The events that must occur before triacylglycerols can reach the bloodstream through the digestive process. CCK Triacylglycerol (TAG) Storage • • • • TAG stored in adipocytes (adipose tissue) mostly Provides insulation and protection TAG droplet occupies most of cell As TAG accumulates, cell enlarges and then splits into 2 cells • TAG can be stored virtually limitlessly! • Obesity can result from either an increased number of fat cells or an enlargement of existing fat cells Adipocytes Figure 25.4: Structural characteristics of the adipose cell. Triacylglycerol Mobilization • Release of free fatty acids and glycerol from fat cells by hydrolysis of TAGs, stimulated by epinephrine and norepinephrine (fasting or physical activity) • Hormone binds to external receptor and activates adenyl cyclase, causing production of cAMP in the inside of the adipocyte • cAMP activates hormone sensitive lipase (HSL) in adipocyte, which hydrolyzes TAGs to produce free fatty acids (FFAs) and glycerol that are released into blood and go to the muscle tissue (FFAs are transported bound to plasma albumin) • Relatively slow process (~10% replaced daily) Epinephrine Action Figure 25.5 Triacylglycerol Mobilization • TAGs represent the largest energy reserve in the body, and are the SECOND type of compound to be utilized as energy after carbohydrates Glycerol Metabolism • Occurs in the cytosol • Involves phosphorylation and oxidation • Consumes one ATP and produces one NADH • DHAP enters glycolysis to produce glyceraldehyde-3-P Fatty Acid -Oxidation • Occurs in mitochondria • Makes acetyl-CoA, ATP, and NADH/FADH2 • Involves three steps – “activation” of the fatty acid – transport into mitochondrial matrix – repeated -Oxidation: sequence of FOUR reactions Activation and Transport of FA A. Conversion to acyl-CoA on the outer mitochondrial space Process consumes TWO high energy phosphate bonds B. A transporter then facilitates translocation of acyl-CoA into mitochondrial intermembrane space Activation and Transport of FA C. Acyl-CoA is converted to acyl-carnitine by carnitine palmitoyltransferase, which then translocates acyl-carnitine into the matrix, and regenerates acyl-CoA from free CoA from within the matrix as carnitine is recycled back into the intermembrane space Activation and Transport of FA -Oxidation • Sequential removal of 2 C (acetyl) units from the carboxyl end of FA in a repetitive FOUR-step cycle 1. Oxidation (dehydrogenation) 2. Hydration -Oxidation 3. Oxidation (dehydrogenation) 4. Cleavage Unsaturated Fatty Acids • Two additional enzymes are needed – Epimerase: converts D--hydroxyacyl-CoA that results from hydration of a cis double bond (the most abundant) to the L isomer Unsaturated Fatty Acids • Two additional enzymes are needed – Cis-trans isomerase: converts cis double bonds at oddnumbered positions to trans double bonds at evennumbered positions, which is required for the hydratase enzyme Complete Oxidation and ATP Production • For C18 (Stearate): 8 cycles occur – 32 ATPs from 8 NADH (× 2.5) and 8 FADH2 (× 1.5) – 90 ATPs (via Citric Acid Cycle) from 9 Acetyl-CoAs (9×3×2.5 + 9×1×1.5 + 9×1) – 2 ATPs are used to form acyl CoA (initially) – Total Net = 120 ATP from C18 Fatty Acid!! Energy Comparison Comparing equal masses: • 1 g stearic acid (18:0) x 1 mole x 120 ATP = 0.423 moles of ATP 284 g 1 mole • 1 g glucose x 1 mole x 30 ATP = 0.17 moles ATP 180 g 1 mole • You get 2.5 times more energy (0.423/0.17) from 1 g fat than from 1 g carbohydrate; thus: • 1 g carb = 0.17 × 24.5 ~ 4 kcal • 1 g fat = 0.43 × 24.5 ~ 9 kcal Energy Comparison • Both carbs and fats are useful “body fuels” • Skeletal muscle: prefers glucose when active and fatty acids when resting • Cardiac muscle: prefers fatty acids then ketone bodies, glucose, lactate • Liver: prefers fatty acids • Brain: prefers glucose (fatty acids can’t cross BBB) then ketone bodies • RBC: needs glucose (no mitochondria) Energy in Exercise The initial stages of exercise are fueled primarily by glucose (glycogen); within about 20 – 30 minutes, triacylglycerols become the primary fuel Ketone Bodies • Produced via alternative pathway of acetyl-CoA metabolism when it accumulates – acetoacetate → acetone – β-hydroxybutyrate • Caused by high rate of fat catabolism relative to glucose catabolism in liver mitochondria • When glucose catabolism decreases and/or fat catabolism rises, there is not enough pyruvate to synthesize oxaloacetate (by carboxylation), so Krebs cycle cannot consume all the acetyl-CoA Ketogenesis Pathway • Step 1: Self-condensation of acetyl-CoA • Step 2: Hydrolysis of acetyl-CoA and condensation of acetate with acetoacetyl-CoA Ketogenesis Pathway • Step 3: Fragmentation of HMG CoA to acetoacetate (ketone body) + acetyl CoA • Step 4a: Reduction of acetoacetate to β-hydroxybutyrate Ketogenesis Pathway • Step 4b: Spontaneous decarboxylation of acetoacetate to acetone (ketone body) + CO2 (acetone is then expired from the lungs and excreted via skin pores and urine) Figure 25.8 How do ketone bodies provide energy? • β-hydroxybutyrate can be reversibly converted to acetoacetate, which produces NADH that can be used in the electron transport chain to produce ATP • Acetoacetate can be “activated” by transfer of a CoA group from succinyl-CoA (from Krebs cycle), and the resulting acetoacetyl-CoA can be cleaved to two acetylCoA molecules that can enter Krebs cycle • Thus, β-hydroxybutyrate and acetoacetate represent water-soluble transportable forms of acetyl-CoA that can be used to generate energy as needed CoA‒SH succinate succinyl-CoA How do ketone bodies provide energy? • Heart muscle and the renal cortex use acetoacetate in preference to glucose • The brain adapts to utilization of acetoacetate with starvation or diabetes (75% of brain fuel needs are obtained from acetoacetate during prolonged starvation) Ketosis vs. Ketoacidosis • The presence of significant levels of acetoacetate, βhydroxybutyrate, and acetone is called ketosis • Acetone gives a “sweet smell” to breath and urine • Acetoacetate and β-hydroxybutyrate can decrease plasma pH (by decreasing plasma bicarbonate), which if left uncontrolled can lead to metabolic acidosis, also called ketoacidosis • Increased solutes in plasma can cause a fluid shift from ICF to ECF if left uncontrolled Ketosis vs. Ketoacidosis • This can initially lead to extracellular edema, and ultimately to intracellular dehydration – Loss of solutes in the urine causes loss of water as well (by osmotic diuresis), eventually leading to total body dehydration • Occurs when glucose metabolism is not occurring at a reasonable rate compared to fat metabolism for a prolonged period of time • Common in: uncontrolled type I diabetes, and extended low carbohydrate diets, fasting, or starvation Lipogenesis • Synthesis of fatty acids from acetyl CoA – Occurs in the cytosol, mostly in liver, adipose tissue, and mammary glands – NOT the exact reverse of fatty acid degradation – Carried out by the “Fatty Acid Synthase Complex” – Fatty acid is bonded to acyl carrier protein (ACP) – Requires NADPH as a reducing agent – Acetyl-CoA initially forms malonyl CoA (3 carbons) – Converts “excess caloric intake” from carbohydrates, protein, and alcohol (i.e., excess acetyl CoA) to fats Lipogenesis • Humans can convert both glucose and fats to acetyl CoA, but acetyl-CoA can only be converted back to fatty acids (via lipogenesis), NOT to glucose (acetyl-CoA cannot be converted to pyruvate or oxaloacetate) • Thus to lose extra fat, humans must burn fat as an energy source (being physically active before and/or after meals) Lipogenesis • The major steps or lipogenesis are: – Translocation of acetyl-CoA from the mitochondrial matrix to the cytosol (via citrate-malate shuttle) – Formation of malonyl CoA – Formation of acyl-ACP – Chain elongation Citrate-Malate Shuttle • Acetyl CoA is produced in the mitochondria and lipogenesis occurs in the cytosol, so acetyl CoA needs to be transported out of the mitochondria • Acetyl CoA + oxaloacetate → citrate (via Krebs) • Citrate is then transported out of the matrix through a protein called the citrate transporter Citrate-Malate Shuttle • Once in the cytosol – citrate → acetyl CoA + oxaloacetate – consumes one ATP • acetyl CoA goes into lipogenesis • oxaloacetate + NAD+ → malate + NADH • malate transported into the matrix by a protein called the malate transporter • malate + NADH → oxaloacetate + NAD+ • Oxaloacetate is used to react with more acetyl CoA to form citrate (cycle repeats) Formation of Acetyl & Malonyl ACP 1. Transfer of acetyl group from CoA to ACP 2. Conversion of acetyl-CoA to malonyl-ACP (Only occurs where ATP levels are high; requires Mn2+ and biotin) Chain Elongation 1. Attachment of acetyl- and malonyl-ACP to the Fatty Acid Synthase Complex 2. Much like β-oxidation, a sequence of FOUR steps then take place, which are the reverse of βoxidation A. condensation B. hydrogenation C. dehydration D. hydrogenation Chain Elongation 1. Condensation (with decarboxylation) 2. Hydrogenation (requires NADPH, from pentose phosphate pathway) Chain Elongation 3. Dehydration 4. Hydrogenation (requires NADPH, from pentose phosphate pathway) Further elongation requires other enzyme, but still result in fatty acids with an even carbon number Synthesis of Unsaturated Fatty Acids • Requires molecular oxygen and NADPH • In humans, points of unsaturation can only occur at carbon atoms 4 through 9 in fatty acid – Thus fatty acids with points of unsaturation initially beyond carbon 10 (e.g., linoleic acid and alpha linolenic acid) cannot be synthesized Cholesterol Synthesis • Essential structural component of all cell membranes • Precursor to steroid hormones (progestins, estrogens, androgens, glucocorticoids, and mineralcorticoids), vitamin D, and bile acids/salts • Occurs primarily in the liver and small intestines from 18 acetyl CoA molecules, which ultimately yield a structure with 27 carbons • Approximately 1.5 – 2.0 g/day is synthesized and nearly 0.30 g/day is consumed in the diet Cholesterol Synthesis • Five major stages Key enzyme: HMG-CoA reductase [target of anti-cholesterol drugs called “statins”, e.g., atorvastatin (Lipitor), lovastatin (Mevacor), simvastatin (Zocor)] Cholesterol Synthesis ×6 Cholesterol Synthesis Several steps Statin Structure Steroid Synthesis Relationship between Lipids and Carbohydrates • Acetyl CoA is primary link • Both fat and carbohydrates produce acetyl-CoA for citric acid cycle for energy • Excess acetyl-CoAs from carbohydrate metabolism can produce fatty acids and eventually lead to fat storage (they cannot be used to regenerate glucose because they cannot be converted to pyruvate or oxaloacetate) Relationship between Lipids and Carbohydrates • Ketosis occurs when there is an increase in fatty acid metabolism relative to glucose metabolism • Ketoacidosis occurs when there is excessive fat metabolism that is not well controlled • Fatty acid and cholesterol synthesis occurs when the body is in an acetyl CoA-rich state Lipoproteins (Chapter 20) • Chylomicrons – carry exogenous (dietary) fat and other lipids from the small intestine into the blood and ultimately to tissue sites (mostly adipose tissue and muscle) • VLDL – carry mostly endogenous (synthesized) fat, from the liver through the blood to adipose tissue Lipoproteins • LDL – carry fats and larger amounts of cholesterol from the liver through the blood to the peripheral tissues (made from VLDL) (< 100 mg/dL is optimal) • HDL – carry fats and larger amounts of cholesterol from the peripheral tissues through the blood to the liver for metabolism to bile acids followed by excretion in bile via the gall bladder (> 60 mg/dL is optimal) – Ratio of total cholesterol to HDL cholesterol is better of < 3.5 is optimal ©2001 Brooks/Cole, a division of Thomson Learning, Inc. Thomson Learning™ is a trademark used herein under license. Size and Compositions of the Lipoproteins Lipoprotein Electrophoresis • Sample (serum) is applied to a support medium • Placed in a chamber with a buffer and electrodes • Negatively charged particles move to the anode • After the development period, the strip is removed and stained (Oil Red O) • This sticks to the lipids and they can be quantified in several ways Lipoprotein Electrophoresis • A normal (fasting for > 8 hours) lipoprotein electrophoresis pattern should contain prominent HDL (alpha) and LDL (beta) bands, and a weak VLDL (prebeta) band • Chylomicrons are cleared from the blood within 8-12 hours anode cathode Hyperlipidemia • Type I Hyperlipidemia (Frederickson Classification) is the inability to clear chylomicrons from the plasma in a normal time – Results from a deficiency in lipoprotein lipase (breaks down chylomicrons) or low HDL levels – People with this condition display significantly elevated TAG levels in the blood (> 600 mg/dL; normal is < 150 mg/dL) – Must severely restrict fats from diet, which may result in essential fatty acid and fat-soluble vitamin deficiency Hyperlipidemia • Restricted diet may be supplemented with a “medium-chain TAG” mixture (recall that smaller fatty acids escape the re-esterification into TAG and incorporation into chylomicrons – they are carried as FFAs by albumin) • Instead, these (and shorter chain fatty acids) are transported to the liver for “chain elongation” Familial Hypercholesterolemia • Genetic disorder characterized by high cholesterol levels, specifically very high levels of low-density lipoprotein (LDL, “bad cholesterol”), in the blood and early cardiovascular disease • Many patients have mutations in the LDLR gene that encodes the LDL receptor protein, which normally removes LDL from the circulation, or apolipoprotein B (ApoB), which is the part of LDL that binds with the receptor Familial Hypercholesterolemia • Patients who have one abnormal copy of the LDLR gene (i.e., heterozygous) may have premature cardiovascular disease at the age of 30 to 40. • Having two abnormal copies (being homozygous) may cause severe cardiovascular disease in childhood. • Heterozygous FH is a common genetic disorder, occurring in 1:500 people in most countries; homozygous FH is much rarer, occurring in 1 in a million births. Familial Hypercholesterolemia • Heterozygous FH is normally treated with statins, bile acid sequestrants, or other hypolipidemic agents that lower cholesterol levels. • New cases are generally offered genetic counseling • Homozygous FH often does not respond to medical therapy and may require other treatments, including LDL apheresis (removal of LDL in a method similar to dialysis) and occasionally liver transplantation Familial Hypercholesterolemia • High cholesterol levels normally do not cause any symptoms early on. • Cholesterol may be deposited in various places in the body that are visible from the outside, such as in yellowish patches around the eyelids (xanthelasma palpebrarum), the outer margin of the iris (arcus senilis corneae) and in the form of lumps in the tendons of the hands, elbows, knees, and feet, particularly the Achilles tendon (tendon xanthoma). Familial Hypercholesterolemia Xanthelasma palpebrarum, yellowish patches consisting of cholesterol deposits above the eyelids. These are common in people with FH. Familial Hypercholesterolemia Patient’s hands showing multiple xanthoma tendinosum Familial Hypercholesterolemia • Accelerated deposition of cholesterol in the walls of arteries leads to atherosclerosis, the underlying cause of cardiovascular disease. • The most common problem in FH is the development of coronary artery disease (atherosclerosis of the coronary arteries that supply the heart) at a much younger age than would be expected in the general population. • This may lead to angina pectoris (chest tightness on exertion) or heart attacks. Familial Hypercholesterolemia • Less commonly, arteries of the brain are affected; this may lead to transient ischemic attacks (brief episodes of weakness on one side of the body or inability to talk) or occasionally stroke. • Peripheral artery occlusive disease (obstruction of the arteries of the legs) occurs mainly in people with FH who smoke; this can cause pain in the calf muscles during walking that resolves with rest (intermittent claudication) and problems due to a decreased blood supply to the feet (such as gangrene) Familial Hypercholesterolemia • If lipids start infiltrating the aortic valve (the heart valve between the left ventricle and the aorta) or the aortic root (just above the valve), thickening of these structures may result in a narrow passage called aortic stenosis. • Aortic stenosis is characterized by shortness of breath, chest pain, and episodes of dizziness or collapse. • Atherosclerosis risk is increased further with age and in those who smoke, have diabetes, high blood pressure, and a family history of cardiovascular disease. Familial Hypercholesterolemia • Cholesterol levels may be determined as part of health screening for health insurance or occupational health, when the external physical signs such as xanthelasma, xanthoma, arcus are noticed, symptoms of cardiovascular disease develop, or a family member has been found to have FH. • Hyperlipoproteinemia type IIa on the Fredrickson classification is typically found: – raised level of total cholesterol – markedly raised level of low-density lipoprotein (LDL) – normal level of high-density lipoprotein (HDL) – normal level of triglycerides Summary of HyperLipoproteinemia Phenotypes Type metabolic defect LP abnormality predominant hyperlipidemia I deficient fasting hypertriglyceridemia lipoprotein lipase chylomicrons IIa floating creamy layer over clear serum hypercholesterolemia clear serum increased LDL IIb deficient apoB receptors deficient apoB receptors and deficient HDL III defective apoE IV deficient HDL increased IDL and hypercholesterolemia chylomicron remnants hypertriglyceridemia increased VLDL hypertriglyceridemia V deficient lipoproteinlipase and deficient HDL increased LDL fasting chylomicrons and increased VLDL appearance hypercholesterolemia hypertriglyceridemia hypertriglyceridemia clear (if trig < 500 mg/dl) lipemic (if trig > 600 mg/dl) lipemic clear (if trig < 500 mg/dl) lipemic (if trig > 600 mg/dl) floating creamy layer over lipemic