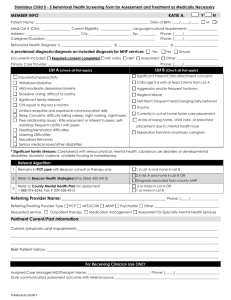
COGNITIVE IMPAIRMENT Clinical Action Plan (Flow Sheet)
advertisement
")
COGNITIVE IMPAIRMENT Clinical Action Plan (Flow Sheet) website: www.BCGuidelines.ca NAME OF PATIENT SEX M DIAGNOSIS CARE OBJECTIVES Diabetes HTN CAD Atrial fib Asthma COPD Renal disease Depression Baseline Investigations (pwhen done; normal or add values prn) FBG ECG TSH Other GFR CBC B12 Ca Other: HbA1c EDUCATION DATE OF DIAGNOSIS OCCUPATION SELF MANAGEMENT (discuss with patient & caregiver) RISK FACTORS AND COMORBID CONDITIONS Obesity Smoker Alcohol DATE OF BIRTH F SMMSE Score Date: MoCA Score Date: Define management goals (risk factor reduction; treat co-morbid conditions; case management) Functional status (baseline & review at each visit) ADLs: IADLs: •Bathing/toileting •Housework •Dressing •Meal prep •Mobility •Shopping •Transportation •Finances •Managing meds Supports (home care, family, case manager, living situation) Caregiver issues (behaviour/sleep/mood) Advance care planning/DNR discussion VISITS DATE BP HR WEIGHT Lbs Kg SMMSE SCORE (Review care objectives, management goals, functional status, symptoms, medications/polypharmacy) BASELINE REVIEW CLINICAL ACTION PLAN VACCINATIONS Annual Flu: Date: Date: Pneumovax: Date: DIAGNOSTIC CODE (Dementia): 290 For information on billing complex care incentive fees, please visit: www.GPSCbc.ca. 1 Cognitive Impairment – Recognition, Diagnosis and Management in Primary Care: Cognitive Impairment Clinical Action Plan (Flow Sheet) (2014)