Non-OR Procedural Safety - Institute for Clinical Systems Improvement
advertisement

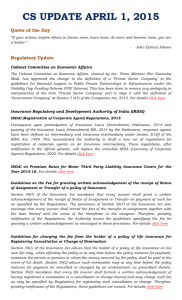
Health Care Protocol Non-OR Procedural Safety How to cite this document: Farris M, Anderson C, Doty S, Myers C, Johnson K, Prasad S. Institute for Clinical Systems Improvement. Non-OR Procedural Safety. Updated September 2012. Copies of this ICSI Health Care Protocol may be distributed by any organization to the organization’s employees but, except as provided below, may not be distributed outside of the organization without the prior written consent of the Institute for Clinical Systems Improvement, Inc. If the organization is a legally constituted medical group, the ICSI Health Care Protocol may be used by the medical group in any of the following ways: • copies may be provided to anyone involved in the medical group’s process for developing and implementing clinical Protocols; • the ICSI Health Care Protocol may be adopted or adapted for use within the medical group only, provided that ICSI receives appropriate attribution on all written or electronic documents and • copies may be provided to patients and the clinicians who manage their care, if the ICSI Health Care Protocol is incorporated into the medical group’s clinical Protocol program. All other copyright rights in this ICSI Health Care Protocol are reserved by the Institute for Clinical Systems Improvement. The Institute for Clinical Systems Improvement assumes no liability for any adaptations or revisions or modifications made to this ICSI Health Care Protocol. www.icsi.org Copyright © Year by Institute for Clinical Systems Improvement Health Care Protocol: Non-OR Procedural Safety Text in blue in this algorithm indicates a linked corresponding annotation. 1 Pre-procedure evaluation, planning and communication Fourth Edition September 2012 2 * No mark required due to patient refusal, midline structure, diagram used, imaging assistance, etc. Pre-procedure verification of patient, procedure and site 3 * Provider marks site with initials if required 4 Confirmation that all verification steps are completed; is discrepancy identified? yes no 10 6 5 Repeat verification process; is discrepancy identified? Has time, team or location changed after verification? yes no yes Able to resolve discrepancy? no no yes 7 11 Able to resolve discrepancy? Active Time-Out process with all team members; is discrepancy identified? yes no no yes 8 no Able to resolve discrepancy? yes 9 ** Complete procedure and create appropriate documentation prior to patient leaving area ** For multiple procedures: 1. Same procedure at different sites: confirm next site after completion of each. 2. Different procedures at multiple sites: reverify with the formal Time-Out process. 3. For multiple teams: Time-Out process for each team at beginning of their procedure. 12 Cancel procedure Return to Table of Contents Copyright © 2012 by Institute for Clinical Systems Improvement www.icsi.org 1 Non-OR Procedural Safety Fourth Edition/September 2012 Table of Contents Work Group Leader Marietta Farris, BSN Nursing, Fairview Health Services Work Group Members Chippewa County – Montevideo Hospital & Clinic Christina E. Anderson, MD Family Medicine HealthPartners Medical Group and Regions Hospital Stephanie Doty, MSN, MBA, RN Patient Safety & Quality University of Minnesota Shailendra Prasad, MBBS, MPH Family Medicine ICSI Kari Johnson, RN Clinical Systems Improvement Facilitator Cassie Myers Systems Improvement Coordinator Algorithm and Annotations........................................................................................... 1-14 Algorithm..............................................................................................................................1 Evidence Grading..................................................................................................................3 Foreword Introduction......................................................................................................................4 Scope and Target Population............................................................................................5 Aim..................................................................................................................................5 Clinical Highlights...........................................................................................................5 Implementation Recommendation Highlights.................................................................6 Related ICSI Scientific Documents.................................................................................6 Definitions.................................................................................................................... 6-7 Special Considerations.....................................................................................................8 Annotations..................................................................................................................... 9-14 Quality Improvement Support. ................................................................................. 15-21 Aims and Measures.............................................................................................................16 Measurement Specifications.................................................................................... 17-18 Implementation Recommendations.....................................................................................19 Implementation Tools and Resources..................................................................................19 Implementation Tools and Resources Table.................................................................. 20-21 Supporting Evidence..................................................................................................... 22-32 References...........................................................................................................................23 Appendices.................................................................................................................... 24-32 Appendix A – List of Invasive, High-Risk or Non-Surgical Procedures.......................24 Appendix B – Sample Checklists.............................................................................25-28 Appendix C – Body Diagrams................................................................................. 29-32 Disclosure of Potential Conflicts of Interest........................................................... 33-34 Acknowledgements. ....................................................................................................... 35-36 Document History and Development....................................................................... 37-38 Document History...............................................................................................................37 ICSI Document Development and Revision Process..........................................................38 www.icsi.org Institute for Clinical Systems Improvement 2 Non-OR Procedural Safety Fourth Edition/September 2012 Evidence Grading Literature Search A consistent and defined process is used for literature search and review for the development and revision of ICSI protocols. The literature search was divided into two stages to identify systematic reviews (stage I) and randomized controlled trials, meta-analysis and other literature (stage II). Literature search terms used for this revision are below and include literature from January 1, 2010, through May 1, 2012. The PubMed database was searched for literature. Limited searches included universal protocol for wrong site in radiology, endoscopy or catheter labs, bedside procedures, and clinics. Other search terms included wrong site and outside the OR/operating room, wrong site and non-OR, near-miss events, true events, wrong procedure, wrong site and surgical safety. Individual research reports are assigned a letter indicating the class of report based on design type: A, B, C, D, M, R, X. Evidence citations are listed in the document utilizing this format: (Author, YYYY [report class]; Author, YYYY [report class] – in chronological order, most recent date first). Class Description Primary Reports of New Data Collections A Randomized, controlled trial B Cohort-study C Non-randomized trial with concurrent or historical controls Case-control study Study of sensitivity and specificity of a diagnostic test Population-based descriptive study D Cross-sectional study Case series Case report Reports that Synthesize or Reflect upon Collections of Primary Reports M Meta-analysis Sytematic review Decision analysis Cost-effectiveness analysis R Consensus statement Consensus report Narrative review X Medical opinion Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 3 Non-OR Procedural Safety Fourth Edition/September 2012 Foreword Introduction The purpose of this safety protocol is to eliminate events involving the wrong patient, wrong site or wrong procedure during high-risk invasive or high-risk procedure performed in the non-operating room setting. Please see the Definitions section for key terms used throughout the protocol. This protocol is consistent with and based heavily on The Joint Commission's Board of Commissioners approved Universal Protocol for Preventing Wrong Site, Wrong Procedure, and Wrong Person Surgery (Joint Commission, The, 2012 [NA]; Siddiqui, 2007 [R]). The Universal Protocol was created in an attempt to address the continuing occurrence of these medical events. The Universal Protocol became effective July 1, 2004, for all accredited hospitals, ambulatory care and office-based surgery facilities, and drew upon, expanded and integrated a series of requirements under The Joint Commission's National Patient Safety Goals (Joint Commission, The, 2012 [NA]). The Universal Protocol is endorsed by nearly 50 professional health care associations and organizations including the American Medical Association, American Hospital Association, American College of Physicians, American College of Surgeons, American Dental Association and American Academy of Orthopedic Surgeons. As part of the Minnesota Adverse Health Event law which can be found at http://www.revisor.leg.state.mn.us/ stats/144/sections 144.706 through 144.7069 – wrong site, procedure and patient events are reported directly to the Minnesota Department of Health and are disclosed to the public on an annual basis. Fortunately, while these events are very rare (1:50,000 invasive procedures including the operating room), facilities in Minnesota continue to work hard at preventing wrong site, wrong patient and wrong procedure events outside of the operating room. The Eighth Annual Public Report of Adverse Events in Minnesota states that 36% of the total wrong site, patient or procedure events occurred in non-operating room settings (Minnesota Department of Health, Eighth Annual Public Report, 2012 [NA]). In addition to providing guidance on implementing the elements of Universal Protocol as defined by The Joint Commission, this protocol addresses other components such as purposeful team communication, that are important in fostering a culture of patient safety in a health care setting. An observational study has shown that ineffective team communication is often a root cause for a medical event, and ineffective team communications can have immediate, negative effects on patient safety (Lingard, 2004 [D]). The work of implementing this protocol requires coordination among the provider, the patient/legal guardian, the patient's nurse, the procedural team, radiology personnel, emergency department staff and anesthesia practitioners, as well as many others. All staff/providers involved must take an active role in participating with this protocol to ensure its effectiveness. Patients or surrogates should be encouraged to participate, if able, as essential members of the health care team and should be engaged in processes designed to reduce the risk of adverse events. Participation may include the patient or surrogate in the pre-procedure verification process. Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 4 Non-OR Procedural Safety Fourth Edition/September 2012 Foreword Scope and Target Population There are clinical reasons for a procedure to take place outside of an operating room. This protocol is applicable for all patients having an invasive, high-risk, diagnostic or therapeutic procedure performed not in the operating room but in an office, procedural area, emergency department or at the bedside. The protocol, while similar in process to safety measures used in operating room, takes into consideration the unique work of the different patient care areas listed, e.g., image-guided biopsies and procedures such as PICC line placement where the insertion site is not predetermined. It covers the processes of patient consent; identification; verification of procedure, site and patient; and the indications for site-marking. A diagram may be used as an alternative to marking; see Appendix C, "Body Diagrams," for examples. Discussion of laterality, levels, multiple sites and multiple procedures is also included. The goal of the Universal Protocol is "to improve patient safety and prevent procedural errors." Institutional consistency may improve overall compliance and safety, and institutions may consider a more broad application of this algorithm rather than a more limited one (e.g., inclusion of electroconvulsive therapy [ECT], dialysis and radiation). Much of the evidence used to derive these recommendations is from studies involving adult patients. However, the work group has made the assumption that the benefit derived from these practices also applies to pediatric patients. Return to Table of Contents Aim 1. Eliminate wrong site, side, patient or procedure events performed outside of the operating room. Return to Table of Contents Clinical Highlights • Procedure sites will be marked with the initials of the provider. The provider will confirm the patient's identity, procedure(s) and site(s) prior to initialing the site. For bilateral procedures, both sides will be marked. (Annotation #3) • A Time-Out will be performed just prior to the start of the procedure, with active verbal confirmation by all the caregivers involved in the care of the patient. The patient should be involved if possible. (Annotation #7) • If site determination is done at the time of the procedure using imaging, verbal confirmation should occur with team/patient, and documentation should reflect use of imaging for site determination. (Annotation #3) • The Time-Out procedure will be repeated for each different anatomically distinct procedure. (Annotation #9) Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 5 Non-OR Procedural Safety Fourth Edition/September 2012 Foreword Implementation Recommendation Highlights The following system changes were identified by the protocol work group as key strategies for health care systems to incorporate in support of the implementation of this protocol. • For ongoing success of this protocol, leadership support, a local/unit-based champion and a multidisciplinary steering team are absolutely essential. • Establish pre-procedure and intra-procedural communication standards in the form of structured handoffs, huddles, pre-procedure briefings, etc. • Create a process that addresses how to document completion of each step and ensure that all elements of the protocol are completed. A checklist may be used (see Appendix B, "Sample Checklists," for a sample Pre-Procedure hard copy checklist, and for a sample checklist within an electronic medical record [EMR]). • A visual reminder to complete the Time-Out is recommended. Return to Table of Contents Related ICSI Scientific Documents Protocols • Perioperative Protocol Return to Table of Contents Definitions Clinician – All health care professionals whose practice is based on interaction with and/or treatment of a patient. Discrepancy is any disagreement over the plan for the patient. A discrepancy in the plan of care could develop or be found at any point in the Safe Site Process. The discrepancy could be found with what the patient/legal guardian states is being done, patient identification, consent, site, site-marking, medical record, imaging, procedure scheduled, team members and/or lack of available equipment. Hard stop is a cessation of activity. It is performed when the verification process has not been followed completely and/or there is a discrepancy identified. High-risk invasive procedure is any procedure that is known to expose a patient to the risk of serious harm or permanent loss of function or injury. Generally, this includes procedures requiring consent by the patient. Refer to Appendix A, "List of Invasive, High-Risk or Non-Surgical Procedures," for examples. Intra-procedure pause is a pause during the procedure(s); the provider will indicate verbally: • level(s), • internal laterality after a midline or orifice entry, or • implant information. Laterality refers to any anatomical structure that occurs on both sides of the body, either internally or externally (e.g., right, left or bilateral). Reference to laterality is always with respect to the patient (e.g., the patient's right or left, not the provider's). Return to Table of Contents Institute for Clinical Systems Improvement www.icsi.org 6 Non-OR Procedural Safety Fourth Edition/September 2012 Foreword Level refers to any anatomical structures that include multiples occurring linearly (e.g., spinal vertebrae, ribs). Patient identifiers are used first, to reliably identify the individual as the person for whom the service or treatment is intended: second, to match the service or treatment to that individual. Acceptable methods for identifying a patient include the individual's name, an assigned identification number, telephone number or other person-specific identifier. Provider is a member of the team performing the procedure who is credentialed and privileged as defined by the institution's medical staff bylaws or who is a physician in residency training. Position refers to the placement or angle of the patient for the procedure (e.g., supine, prone). Reference to position is important when determining laterality. Possibles refer to possible sites and/or procedures listed on the patient consent, and the decision whether to perform the additional procedure is based on the findings of the initial procedure. These should follow this same process for site-marking and verification as predetermined procedures. Site is defined as the specific anatomic location of the procedure site (incision, insertion or injection) as indicated by a description of the body part(s), levels (e.g., spine level or ribs), and digits (for hands, use thumb, index, long, ring, small; for toes, use great toe, second, third, etc.) to be subjected to intervention. Midline not associated with laterality or level need not be marked. However, if the internal target site involves laterality, and laterality is specified on the consent, the provider should verbally state site upon entry. For spinal procedures, the incision site – anterior or posterior – and general level (cervical, thoracic or lumbar) are marked. Single provider one and only person involved in performing an invasive procedure. Source document refers to an original radiology or pathology report that identifies laterality and/or specifies anticipated procedural location. Structured hand-off is a standardized method of communication used to improve the exchange of information during care transitions. The purpose of a structured hand-off is to promote patient safety by ensuring that critical pieces of information are conveyed to the next individual assuming care responsibilities, including such things as critical test results, patient status, recent/anticipated changes in patient condition, plan of care/ goals, what to watch for in the next interval of care, etc. This should be a process used by all caregivers and should be done during a patient transition from one caregiver to another. This should be done face to face to encourage discussion and questions. Time-Out is the full verification that is performed immediately prior to the start of the procedure and is the final safety stop before the procedure is begun. Every Time-Out must include the following standard elements: • Patient's identity, using a minimum of two patient identifiers • Procedure(s) to be performed (including internal and/or external laterality, multiples and/or level) • Patient positioning if not already verified • Procedure side, site and/or level including visualization of the provider's initials if applicable • As appropriate, imaging, equipment, implants or special requirements (e.g., pre-procedure antibiotic administration) Verification is defined as checking for consistency between the: • informed consent documentation; • diagnostic studies if applicable; and • response of the patient/legal guardian, if able. Return to Table of Contents Institute for Clinical Systems Improvement www.icsi.org 7 Non-OR Procedural Safety Fourth Edition/September 2012 Foreword Special Considerations Anatomical Variation: When a patient is known to have anatomical variation involving the procedure site, this information should be shared with the care team and additional steps taken to confirm the correct procedure site. This may include additional imaging or a second physician confirming the procedure site. Single Provider: There are invasive procedures that may involve only one provider. If possible, engage the patient or surrogate in the pre-procedure verification process by asking the patient or surrogate to state the procedure to be performed. This pre-procedure verification is especially important if the provider leaves the patient's room/bedside before performing the invasive procedure. Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 8 Non-OR Procedural Safety Fourth Edition/September 2012 Algorithm Annotations 1. Pre-Procedure Evaluation, Planning and Communication Verification of the consistency of all patient/procedural information (patient's name, date of birth, medical record number, planned procedure, procedural site and laterality, as applicable) ideally begins at the point of scheduling. It is recommended that facilities establish a process to verify the consistency of all patient/procedural information upon receipt of procedure-related documents. Potential sources include: • procedural consent, • radiology reports, • pathology reports, • laboratory results, • procedural orders, • medical records, and • physician referrals. This could take the form of a checklist including the date and signature of the individual who receives and verifies that data are consistent on each document as received. All documentation should be provided by paper, fax or electronic format (not by phone or verbal communication) except in emergent/urgent situations. Ideally, the patient should be provided the same information in hard copy form to bring to the appointment/procedure. Discrepancies in the consistency of patient name, date of birth, medical record number, planned procedure, procedural site or laterality should be: • addressed immediately upon discovery, and • guided by a process (e.g., unit supervisor informed). Planning for the procedure must not continue until the discrepancy is resolved. Return to Algorithm Return to Table of Contents 2. Pre-Procedure Verification of Patient, Procedure and Site With the patient awake the providers/clinicians involved in the care, along with the patient/legal guardian and/or family member will confirm the patient's identity, procedure and site by comparing the following: • Patient's identity, using two patient identifiers. • Procedure name and site in the informed consent documentation. Multiple procedures are numbered on the consent form with corresponding numbers marked on the patient's skin. • Information in the medical record. • Diagnostic studies. • Discussion with the patient/legal guardian. Return to Algorithm Return to Table of Contents Institute for Clinical Systems Improvement www.icsi.org 9 Non-OR Procedural Safety Fourth Edition/September 2012 Algorithm Annotations • Interventional radiology: the lesion/site may be identified using intra-procedural imaging, in which case it cannot be marked on the skin. The use of intra-procedural imaging for site verification will then be recorded in the Time-Out documentation. The ultimate responsibility for procedure and site verification lies with the provider performing the procedure. See Appendix B, "Sample Checklists," for examples of process documentation. Return to Algorithm Return to Table of Contents 3. Provider Marks Site with Initials if Required The provider performing the procedure holds the responsibility for following the correct site-marking process. See the definition of "Site" in the "Definitions" section for more information. General exceptions to site-marking include but are not limited to: • Emergency procedures • Midline structures • Single organ cases (cardiac procedures) Site-marking has the following characteristics and expectations: • Site-marking is done following the identification of the patient, review of the consent and other related images as required, and with the patient/family taking part in the process, if able. • The procedure site will be initialed by the provider using his/her initials with an indelible marker and will be placed such that it is visible when the patient is positioned, prepped and draped. • Both sites will be marked for bilateral procedures as noted on the consent form. • For multiple sites/digits on the same anatomical site: each procedure must be numbered independently on the informed consent documentation and each site marked with the appropriate corresponding number. • For independent procedures on paired anatomical sites (e.g., ears): each procedure must be numbered independently on the informed consent documentation and each site marked with the appropriate corresponding number. • For procedures involving level (spine or ribs) – The informed consent documentation will indicate the laterality and level, and the site will be marked in a way to indicate anterior or posterior and general level (cervical, thoracic, lumbar, or rib number). • For imaging-guided procedures, if the side or individual structure is known prior to the procedure start, the site should be marked on the skin. • Site-marking is also necessary when direct puncture into the area of interest is done based on external landmarks, history or prior studies (rather than intra-procedural imaging) and there is a possibility for left/right or level events. • For procedures performed by anesthesia – When an anesthesiologist is performing a nerve block or epidural that involves laterality or spine levels, the site should be marked with an "A" with a circle around it to differentiate it from the proceduralist's initials even when the only procedure being performed is by the anesthesiologist. • For some procedures, the entry site, best approach or treatment site is determined during the first phase of the procedure using radiologic imaging. Verbal confirmation of the final site selection Return to Algorithm Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 10 Non-OR Procedural Safety Fourth Edition/September 2012 Algorithm Annotations should take place between the provider, the team and the patient (if possible), and documentation following the procedure should reflect the use of imaging to determine the site. Procedures and situations requiring the use of site-marking diagram: There should be a written process providing direction on when and how to use the site-marking diagram and how to record this information in the medical record. Guidelines for the use of the diagram include: • When the site is technically or anatomically impossible to mark, (such as a mucosal surface or perineum). • Teeth – Indicate operative tooth name(s) on informed consent documentation, or mark the operative tooth (teeth) on the dental radiographs or dental diagram. • Premature infants for whom the mark may cause a permanent tattoo. No infants under the corrected gestational age of 38 weeks should be marked. • Patient refusals to have skin marked – A defined procedure should be in place for documentation of a patient refusal of site-marking, along with the use of the site-marking diagram. • The use of the diagram should be considered for patients with tattoos at the operative site and the site mark may not be clearly visible. • The use of the diagram should be considered for patients with anatomical abnormalities that may lead to confusion as to the correct site. Other situations: Site-marking is not required when the provider performing the procedure is in continuous physical presence with the patient from arrival for the procedure to conclusion of the procedure. Continuous physical presence means the provider does not leave the room where the procedure will be preformed. All the essential patient identifiers, consents, medical records, x-rays and the necessary equipment must be present in the room, and the provider does not leave the room for any reason. • Interventional procedures where the insertion site is not predetermined (e.g., cardiac catheterization, peripherally inserted central catheters, central lines, arteriogram). • Procedures that enter through an orifice where the target organ is not associated with laterality (e.g., endoscopies, cystoscopy, laryngoscopy). • Site-sensitive areas that may be marked above or lateral to the procedure site (e.g., scrotal sites will be marked on the groin area on the appropriate side of the body; breast sites will be marked on the breast or above the breast on the upper chest area). Sample diagrams are provided in Appendix C, "Body Diagrams." Return to Algorithm Return to Table of Contents 4. Confirmation That All Verification Steps Are Completed; Is Discrepancy Identified? A discrepancy is any disagreement over the plan for the patient. A discrepancy in the plan of care could develop or be found at any point in the Safe Site Process. The discrepancy could be found when the patient/ legal guardian states what is being done during patient identification/consent/site-marking, medical record, imaging, when the procedure is scheduled, and from team members and/or lack of available equipment. If any part of the verification process is not followed and/or a discrepancy is discovered, the procedure is halted and will not continue until the discrepancy is resolved. Return to Algorithm Return to Table of Contents Institute for Clinical Systems Improvement www.icsi.org 11 Non-OR Procedural Safety Fourth Edition/September 2012 Algorithm Annotations Resolution of discrepancies will include: • • • • • Reverification of patient identification, with at least two patient identifiers (name/medical record number or name/date of birth) Review of the information in the informed consent documentation Review of the medical record Review of diagnostic studies Discussion with the patient/legal guardian/family member (if appropriate) Return to Algorithm Return to Table of Contents 5. Able to Resolve Discrepancy? When a discrepancy is found, the procedure and/or preparation is halted and will not continue until the discrepancy is resolved. This may include a hard stop, meaning the scalpel, needle or cutting/incising device is not handed to the provider until the discrepancy is resolved. The complete process for resolution of discrepancies must include the following items: • Reverification of patient identification with at least two patient identifiers • Review of the information in the informed consent documentation • Review of the medical record • Discussion with the patient/legal guardian/family member • Review of diagnostic studies Conversations related to solution of discrepancies will be held in a quiet location, away from activity and distractions. After the discrepancy has been resolved, the procedure and site verification process will be repeated. If the steps of the verification process cannot be completed and/or a discrepancy cannot be resolved, the procedure is cancelled and rescheduled. Return to Algorithm Return to Table of Contents 6. Has Time, Team or Location Changed After Verification? There are any number of reasons for the care team to change. If any staff changes or additions (such as handoff, tech-to-tech, observers, lab personnel, etc.) take place, the team member(s) involved in procedure and procedural support should confirm the patient's information including the verification of the patient, procedure and the site. All hand-offs in care before, during or after the procedure should follow a standard process/ format that has been agreed upon by the facility. See the "Definitions" section for "Structured Hand-Off." Return to Algorithm Return to Table of Contents 7. Active Time-Out Process with All Team Members; Is Discrepancy Identified? The Time-Out is to be performed immediately prior to the start of the procedure and is the final safety step before the procedure is begun. Every Time-Out must include the following elements: • Patient identity, using a minimum of two patient identifiers • Patient positioning if not already verified • Procedure(s) to be performed (including internal and/or external laterality, multiples and/or level) Return to Algorithm Return to Table of Contents Institute for Clinical Systems Improvement www.icsi.org 12 Non-OR Procedural Safety Fourth Edition/September 2012 Algorithm Annotations • • Procedure side, site and/or level including visualization of the provider's initials if applicable As appropriate, imaging, equipment, implants or special requirements (e.g., pre-procedure antibiotic administration) The Time-Out is to be initiated by the provider and includes active verbal acknowledgment by all members of the team. During the Time-Out, each person in the procedure room must stop what he or she is doing and actively participate in the process. No individual is exempt from the process. Active participation requires each individual to state clearly and loudly that he or she agrees with the elements of the Time-Out. The scalpel, needle or other cutting/incising device is not to be handed to the provider until the Time-Out has been completed. Environmental distractions are to be eliminated as much as possible during the Time-Out. For example, music is turned off, pagers are set on vibrate, talking other than participation in Time-Out ceases, and no staff are permitted to enter or exit the room. If during the Time-Out an interruption or distraction occurs (pager goes off or an individual enters the room), the Time-Out must be restarted. While it is desirable to actively include the patient in the Time-Out, it is not always possible, particularly if the patient is under the influence of sedating medications or is otherwise unable to participate. It is recommended that a visual memory aid be used to trigger the initiation of the Time-Out. For example, a "Time-Out" sign or towel can be used to cover the scalpel, needle or cutting/incising device as a reminder to conduct the Time-Out. The provider may delegate the Time-Out elements to the nurse or other member of the team, but the initiation of the Time-Out should be the responsibility of the provider. The nurse or other team member may refer to the patient consent for the Time-Out elements. However, prior to its use, the consent must have been validated against other documents such as history and physical, radiology or pathology reports, progress notes, etc. See Appendix B, "Sample Checklists." Additional Time-Outs are to be performed when there are two or more different procedures performed on the same patient during the same procedure period, whether or not the procedures involve a new procedure team. The process and elements of the Time-Out as described above must occur prior to the start of the next procedure. Additional patient identification should be conducted when there is a change in team composition. If the patient needs to be repositioned during the procedure and this repositioning affects the patient's presentation (e.g., the patient is turned prone), an abbreviated Time-Out including the site, side, level and/ or visualization of the provider's initials will be conducted. The Time-Out process will be the same as described above (e.g., elimination of distractions, active participation). The Time-Out process is a final check prior to the actual procedure being performed. It is recommended that the process be documented in the medical record as a marker of safety procedures. The documentation should reflect the person initiating the Time-Out process; the identification by the second provider of the patient, the site and the procedure being performed, and the completeness of the consent process. Return to Algorithm Return to Table of Contents 8. Able to Resolve Discrepancy? See Annotation #5, "Able to Resolve Discrepancy?" Return to Algorithm Return to Table of Contents 9. Complete Procedure and Create Appropriate Documentation Prior to Patient Leaving Area When the provider is starting a new procedure at a different site, the procedure number is referenced on the consent form and verified with the number marked on the patient. A member of the team will read Return to Algorithm Return to Table of Contents Institute for Clinical Systems Improvement www.icsi.org 13 Non-OR Procedural Safety Fourth Edition/September 2012 Algorithm Annotations the procedure and number from the consent form. Each member of the team will verbally acknowledge the procedure being performed prior to starting. This process is completed every time the location and/or procedure changes. Examples include: • Multiple procedures – different sites - • Biopsy of atypical lesions: face, scalp and right forearm Different procedures – multiple sites - Cryosurgery actinic keratoses: right cheek, nose, left ear, right forearm, right hand. Incision and drainage cyst at upper back, biopsy of atypical lesion right lower back - Cryosurgery verruca at right heel. Biopsy atypical lesion at right leg - Cryosurgery actinic keratoses at left arm, right arm, nose and left ear. Biopsy lesion at left cheek and dorsal left hand At the completion of the procedure, the provider will create an immediate post-procedure note into the medical record. If the procedure note is being dictated, an abbreviated note will suffice. A final note should include a notation that a Time-Out had been completed. Return to Algorithm Return to Table of Contents 10.Repeat Verification Process; Is Discrepancy Identified? If the procedure time changes, if the provider or care team changes, or if the patient is moved, a repeat verification is required. Refer to verification components in Annotation #2, "Pre-Procedure Verification of Patient, Procedure and Site." Return to Algorithm Return to Table of Contents 11.Able to Resolve Discrepancy? See Annotation #5, "Able to Resolve Discrepancy?" Return to Algorithm Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 14 Quality Improvement Support: Non-OR Procedural Safety The Aims and Measures section is intended to provide protocol users with a menu of measures for multiple purposes that may include the following: • population health improvement measures, • quality improvement measures for delivery systems, • measures from regulatory organizations such as Joint Commission, • measures that are currently required for public reporting, • measures that are part of Center for Medicare Services Physician Quality Reporting initiative, and • other measures from local and national organizations aimed at measuring population health and improvement of care delivery. This section provides resources, strategies and measurement for use in closing the gap between current clinical practice and the recommendations set forth in the protocol. The subdivisions of this section are: • Aims and Measures • Implementation Recommendations • Implementation Tools and Resources Copyright © 2012 by Institute for Clinical Systems Improvement 15 Non-OR Procedural Safety Fourth Edition/September 2012 Aims and Measures Outcome Aim and Measure 1. Eliminate wrong site, side, patient for invasive or high-risk procedure events performed outside of the operating room. Measures for accomplishing this aim: a. Wrong invasive or high-risk procedure events per month. b. Rate of wrong invasive or high-risk procedure events per month. c. Rate of observational compliance. Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 16 Non-OR Procedural Safety Fourth Edition/September 2012 Aims and Measures Measurement Specifications Measurement #1a/1b 1a. Wrong invasive or high-risk procedure events per month. 1b. Rate of wrong invasive or high-risk procedure events per month. Population Definition Patients of all ages who have an invasive or high-risk procedure done outside of the operating room (any non-OR setting). Data of Interest 1a. Number of wrong invasive or high-risk procedures events per month. 1b. # of wrong events Total # of procedures per month Numerator and Denominator Definitions Numerator: Number of wrong invasive or high-risk procedure events per month. Note: a wrong event is defined as a wrong invasive or high-risk procedure performed on the wrong patient, or a procedure performed on the wrong side, site or level. Denominator: Total number of non-OR procedures per month. Method/Source of Data Collection Collect the number of total invasive or high-risk procedures done monthly. Determine from chart audits or event data whether any of these were wrong events. Event data should be reported through an incident or sentinel event report or per the organization's policy for reporting. Data Collection Time Frame The suggested time period is a calendar month, but three months could be consolidated into quarterly data points if case load and/or event numbers are small. Notes This is an outcome measure, and the improvement goal is no wrong events. Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 17 Non-OR Procedural Safety Fourth Edition/September 2012 Aims and Measures Measurement #1c Rate of observational compliance. Population Definition Patients of all ages who have an invasive or high-risk procedure done outside of the operating room (any non-OR setting). Data of Interest # of invasive or high-risk procedures that met observational compliance Total # of invasive or high-risk procedures outside of OR Numerator and Denominator Definitions Numerator: Number of invasive or high-risk procedure that met observational compliance. Denominator: Total number of non-OR procedures per month. Method/Source of Data Collection Collect the number of total invasive or high-risk procedures done monthly. Determine from chart audits or event data the number that met observational compliance. Event data should be reported through an incident or sentinel event report or per the organization's policy for reporting. Data Collection Time Frame The suggested time period is a calendar month, but three months could be consolidated into quarterly data points if case load and/or event numbers are small. Notes This is an outcome measure, and improvement is noted as an increase in the rate. Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 18 Non-OR Procedural Safety Fourth Edition/September 2012 Implementation Recommendations Prior to implementation, it is important to consider current organizational infrastructure that address the following: • System and process design; • Training and education; and • Culture and the need to shift values, beliefs and behaviors of the organization. The following system changes were identified by the protocol work group as key strategies for health care systems to incorporate in support of the implementation of this protocol: • For ongoing success of this protocol, leadership support, a local/unit-based champion and a multidisciplinary steering team are absolutely essential. • Establish pre-procedure and intra-procedural communication standards in the form of structured handoffs, huddles, pre-procedure briefings, etc. • Create a process that addresses how to document completion of each step and ensure that all elements of the protocol are completed. A checklist may be used (see Appendix B, "Sample Checklists," for a sample Pre-Procedure hard copy checklist, and for a sample checklist within an electronic medical record [EMR]). • A visual reminder to complete the Time-Out is recommended. Return to Table of Contents Implementation Tools and Resources Criteria for Selecting Resources The following tools and resources specific to the topic of the protocol were selected by the work group. Each item was reviewed thoroughly by at least one work group member. It is expected that users of these tools will establish the proper copyright prior to their use. The types of criteria the work group used are: • The content supports the clinical and the implementation recommendations. • Where possible, the content is supported by evidence-based research. • The author, source and revision dates for the content are included where possible. • The content is clear about potential biases and when appropriate conflicts of interests and/or disclaimers are noted where appropriate. Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 19 Non-OR Procedural Safety Fourth Edition/September 2012 Implementation Tools and Resources Table Author/Organization American College of Radiology Audience Health Care Providers Web Sites/Order Information http://www.acr.org/Quality-Safety The ACS is a scientific and educational association of surgeons established to improve the quality of care for surgical patients by setting high standards for surgical education and practice. Health Care Providers; Patients and Families http://www.facs.org Agency for Healthcare Research and Quality (AHRQ) Safety and quality tips for consumers. Patients and Families http://www.ahrq.gov/consumer/ The Centers for Medicare and Medicaid Services (CMS) Quality initiatives overview and links to Health Care specific information. Providers American College of Surgeons Institute for Healthcare Improvement (IHI) Title/Description The principal organization of radiologists, radiation oncologists, and clinical medical physicists in the United States, with more than 30,000 members. Provides links for quality and safety. The Web site provides information for health care providers and patients. 5M Lives Campaign IHI is a not-for-profit organization for improvement of health care throughout the world. http://www.cms.gov/QualityInitiativesGenInfo Health Care Providers http://www.ihi.org/IHI/Programs/ Campaign/Campaign.htm The 5 Million Lives Campaign is an initiative to engage U.S. hospitals to implement changes to improve patient care and prevent avoidable deaths. Surgical Infection Prevention is one of the initiatives of the 5M Lives Campaign. There are tools and kits in the "Prevent Surgical Site Infection" section. Institute for Safe Medication Practices (ISMP) Alerts patients to frequent medication events and how to avoid them, and general medication safety advice. Patients and Families http://www.ismp.org/newsletters/ consumer/consumeralerts.asp The Joint Commission Site includes The Joint Commission's Universal Protocol Health Care Providers http://www.jointcommission.org The Leapfrog Group Quality and safety information about hospitals that consumers can search. Patients and Families http://www.leapfroggroup.org/ for_consumers Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 20 Non-OR Procedural Safety Fourth Edition/September 2012 Resources Table Author/Organization The Minnesota Alliance for Patient Safety (MAPS) Minnesota Department of Health Title/Description Award winning partnership advancing patient safety in MN. Audience Health Care Providers Web Sites/Order Information http://www.mnpatientsafety.org The site provides patient safety information that includes adverse event reporting and information for consumers and patients. Health Care Providers; Patients and Families http://www.health.state.mn.us/ patientsafety/index.html Minnesota Health Information Hyperlinks to variety of Web sites related to cost and quality, information about managing chronic health conditions and staying healthy. Patients and Families http://www.minnesotahealthinfo. org Minnesota Hospital Association Safe Site Call to Action Health Care Providers http://www.mnhospitals.org National Academy for State Health Policy (NASHP) Assists states in achieving excellence in health policy and practice, resources compare patient safety initiatives and approaches. Health Care Providers http://www.nashp.org Physicians, Scientists, Allied Health Professionals http://www.sirweb.org/medicalprofessionals/ Health Care Providers; Patients and Families http://www.stratishealth.org/expertise/safety/ Web site includes tools that address procedures outside the OR. Society of Interventional National organization of physicians, Radiologists scientists and allied health professionals dedicated to improving public health through disease management and minimally invasive, image-guided therapeutic interventions. Stratis Health NCPS – VA National Center for Patient Safety Minnesota's Medicare Quality Improvement Organization, provides health literacy information and project / quality improvement opportunities. United States Veteran's Administration Health Care Providers http://www.patientsafety.gov Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 21 Supporting Evidence: Non-OR Procedural Safety The subdivisions of this section are: • References • Appendices Copyright © 2012 by Institute for Clinical Systems Improvement 22 Non-OR Procedural Safety Fourth Edition/September 2012 References Links are provided for those new references added to this edition (author name is highlighted in blue). Joint Commission, The. The universal protocol for preventing wrong site, wrong procedure, and wrong person surgeryTM. Available at http://www.jointcommission.org/standards_information/standards.aspx. (Class Not Assignable) Lingard L, Espn S, Whyte S, et al. Communication failures in the operating room; an observation classification of recurrent types and effects. Qual Saf Health Care 2004;13:330-34. (Class D) Minnesota Department of Health. Adverse health events in Minnesota. Eighth Annual Public Report. Available at: http://www.health.state.mn.us/patientsafety/ae/2012ahereport.pdf. (Class Not Assignable) Siddiqui MT. Pathologist performed fine needle aspirations & implementation of JCAHO universal protocol and "time out." Cytojournal 2007;4:19. (Class R) Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 23 Non-OR Procedural Safety Fourth Edition/September 2012 Appendix A – List of Invasive, High-Risk or Non-Surgical Procedures * • Any procedures involving skin incision • Injections of any substance into a joint space or body cavity • • • • • • • • • • • • • • • • Any procedures involving general or regional anesthesia, monitored anesthesia care, or conscious sedation Percutaneous aspiration of body fluids or air through the skin (e.g., arthrocentesis, bone marrow aspiration, lumbar puncture, paracentesis, thoracentesis, suprapubic catheterization, chest tube) Biopsy (e.g., bone marrow, breast, liver, muscle, kidney, genitourinary, prostate, bladder, skin) Cardiac procedures (e.g., cardiac catheterization, cardiac pacemaker implantation, angioplasty, stentimplantation, intra-aortic balloon catheter insertion, elective cardioversion) Endoscopy (e.g., colonoscopy, bronchoscopy, esophagogastric endoscopy, cystoscopy, percutaneous endoscopic gastrostomy, J-tube placements, nephrostomy tube placements) Invasive radiological procedures (e.g., angiography, angioplasty, percutaneous biopsy) Dermatology procedures (biopsy, excision and deep cryotherapy for malignant lesions – excluding cryotherapy for benign lesions) Invasive ophthalmic procedures including miscellaneous procedures involving implants Oral procedures including tooth extraction or gingival biopsy Podiatric invasive procedures (e.g., removal of ingrown toenail) Skin or wound debridement Electroconvulsive therapy Radiation oncology procedures Central line placements or PICC Kidney stone lithotripsy Colposcopy and/or endometrial biopsy Procedures NOT considered surgical, high-risk or invasive include: • Electrocautery of lesion • Manipulation and reduction • • • • • • • Venipuncture Chemotherapy/oncology procedures Intravenous therapy Nasogastric tube insertion Foley catheter insertion Flexible sigmoidoscopy Vaginal exams * This list is not meant to be comprehensive. It partially draws from the United States Department of Veterans Affairs. The PDF version of VHA Directive 2010-023 was last accessed on September 1, 2012, at http://www1.va.gov/vhapublications/publications.cfm?pub=1. Return to Table of Contents Institute for Clinical Systems Improvement www.icsi.org 24 Non-OR Procedural Safety Fourth Edition/September 2012 Appendix B – Sample Checklists Pre-Procedure Verification Checklist Invasive Procedures Outside the Operating Room If at any time during this process, there is a discrepancy of information, call for a “Hard Stop” – all activity ceases until information is reconciled. Pre-Procedure – Verification 1. Patient identification verified using two indicators ....................................................................... 2. Accurate and complete informed consent verified....................................................................... 3. Procedure verified using at least two independent source documents • Provider order, diagnostic images, radiology/pathology reports, patient understanding of the procedure, informed consent ....................................................................................... 4. Site marked, as appropriate*, by person performing the procedure with initials: ...................... *Refer to provider policy for site marking exclusions • Multiple sites marked and identified in the informed consent .............................................. • Diagram marked by person performing the procedure if unable to mark on patient…….. o Site was not marked due to: ( ) Site marking not required per policy ( ) Provider is in continuous attendance with the patient ( ) Refused by patient Health Care Provider Signature: _________________________________________________________________ Pre-Procedure – Communication 1. Team communication completed .................................................................................................. Team reviewed relevant case information including: o - Images and diagnostic/pathology/lab reports ......Yes ( ) - Anticipated equipment is available ......................Yes ( ) - Antibiotics or fluids for irrigation ...........................Yes ( ) - Positioning .............................................................Yes ( ) - Additional safety precautions, e.g. allergies ........Yes ( ) • N/A ( N/A ( N/A ( N/A ( N/A ( ) ) ) ) ) Just Prior to Procedure (Time-out) 1. Person performing the procedure initiated the time-out verbally ................................................ 2. All other activity ceased ................................................................................................................. 3. 2 nd health care provider verbally: • Verified patient and procedure including side/site......................................................... • Verified visualization and location of the site mark, if applicable ................................. 4. Person performing the procedure verbally: • Verified procedure including side/site ............................................................................. Health Care Provider Signature: Used with permission. Minnesota Hospital Association Safe Site Call-To-Action Toolkit, 2009. Return to Table of Contents Institute for Clinical Systems Improvement www.icsi.org 25 Appendix B – Sample Checklists Non-OR Procedural Safety Fourth Edition/September 2012 Electronic Checklist of Pre-Procedure Assessment, Pre-Procedure Verification and Time-Out Sample electronic format used by Hennepin County Medical Center. Return to Table of Contents Institute for Clinical Systems Improvement www.icsi.org 26 Appendix B – Sample Checklists Sample electronic format used by Hennepin County Medical Center. Return to Table of Contents Institute for Clinical Systems Improvement Non-OR Procedural Safety Fourth Edition/September 2012 www.icsi.org 27 Appendix B – Sample Checklists Non-OR Procedural Safety Fourth Edition/September 2012 Sample electronic format used by Hennepin County Medical Center. Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 28 Non-OR Procedural Safety Fourth Edition/September 2012 Appendix C – Body Diagrams Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 29 Appendix C – Body Diagrams Return to Table of Contents Institute for Clinical Systems Improvement Non-OR Procedural Safety Fourth Edition/September 2012 www.icsi.org 30 Appendix C – Body Diagrams Return to Table of Contents Institute for Clinical Systems Improvement Non-OR Procedural Safety Fourth Edition/September 2012 www.icsi.org 31 Appendix C – Body Diagrams Return to Table of Contents Institute for Clinical Systems Improvement Non-OR Procedural Safety Fourth Edition/September 2012 www.icsi.org 32 Disclosure of Potential Conflicts of Interest: Non-OR Procedural Safety ICSI has long had a policy of transparency in declaring potential conflicting and competing interests of all individuals who participate in the development, revision and approval of ICSI protocols and protocols. In 2010, the ICSI Conflict of Interest Review Committee was established by the Board of Directors to review all disclosures and make recommendations to the board when steps should be taken to mitigate potential conflicts of interest, including recommendations regarding removal of work group members. This committee has adopted the Institute of Medicine Conflict of Interest standards as outlined in the report, Clinical Practice Protocols We Can Trust (2011). Where there are work group members with identified potential conflicts, these are disclosed and discussed at the initial work group meeting. These members are expected to recuse themselves from related discussions or authorship of related recommendations, as directed by the Conflict of Interest committee or requested by the work group. The complete ICSI Policy regarding Conflicts of Interest is available at http://bit.ly/ICSICOI. Funding Source The Institute for Clinical Systems Improvement provided the funding for this protocol revision. ICSI is a not-for-profit, quality improvement organization based in Bloomington, Minnesota. ICSI's work is funded by the annual dues of the member medical groups and five sponsoring health plans in Minnesota and Wisconsin. Individuals on the work group are not paid by ICSI, but are supported by their medical group for this work. ICSI facilitates and coordinates the protocol development and revision process. ICSI, member medical groups and sponsoring health plans review and provide feedback, but do not have editorial control over the work group. All recommendations are based on the work group's independent evaluation of the evidence. Return to Table of Contents Copyright © 2012 by Institute for Clinical Systems Improvement 33 Non-OR Procedural Safety Fourth Edition/September 2012 Disclosure of Potential Conflicts of Interest Christina Anderson, MD (Work Group Member) Family Physician, Family Medicine, National, Regional, Local Committee Affiliations: None Guideline-Related Activities: ICSI Rapid Response Team Protocol Research Grants: None Financial/Non-Financial Conflicts of Interest: None Stephanie Doty, MSN, MBA, RN (Work Group Member) Director of Patient Safety, Patient Safety and Quality Department, Regions Hospital National, Regional, Local Committee Affiliations: None Guideline-Related Activities: ICSI Rapid Response Team Protocol; ICSI Prevention of Retained Foreign Objects During Labor and Delivery Protocol; ICSI Perioperative Protocol; ICSI Committee on EvidenceBased Practice Research Grants: None Financial/Non-Financial Conflicts of Interest: holds stock in 3M Marietta Farris, BSN, MAN (Work Group Leader) Nurse Manager, Medical/Surgical, Fairview Health Services, University of Minnesota Medical Center National, Regional, Local Committee Affiliations: None Guideline-Related Activities: None Research Grants: None Financial/Non-Financial Conflicts of Interest: None Shailendra Prasad, MBBS, MPH (Work Group Member) Assistant Professor, Family Medicine, University of Minnesota National, Regional, Local Committee Affiliations: None Guideline-Related Activities: None Research Grants: None Financial/Non-Financial Conflicts of Interest: None Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 34 Acknowledgements: Non-OR Procedural Safety All ICSI documents are available for review during the revision process by member medical groups and sponsors. In addition, all members commit to reviewing specific documents each year. This comprehensive review provides information to the work group for such issues as content update, improving clarity of recommendations, implementation suggestions and more. The specific reviewer comments and the work group responses are available to ICSI members at http://bit.ly/NonOR0912. Return to Table of Contents Copyright © 2012 by Institute for Clinical Systems Improvement 35 Non-OR Procedural Safety Fourth Edition/September 2012 Acknowledgements Invited Reviewers During this revision, the following medical groups reviewed this document. The work group would like to thank them for their comments and feedback. Gillette Children's Specialty Healthcare, St. Paul, MN Minnesota Gastroenterology, St. Paul, MN Planned Parenthood of Minnesota, North Dakota, South Dakota, St. Paul, MN Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 36 Document History and Development: Non-OR Procedural Safety Document Drafted June – July 2008 First Edition Oct 2008 Second Edition Oct 2009 Third Edition Aug 2010 Fourth Edition Begins Oct 2012 The next revision will be no later than October 2017. Original Work Group Members Kristy Enger, CMA Clinic Chippewa County – Montevideo Hospital & Clinic Marietta Farris, BSN Nursing, Co-Work Group Leader Fairview Health Services Karin K. Fjeldos-Sperbeck, RN Nursing Sanford Health Joann Foreman, RN Facilitator ICSI Lisa Hurt, RN Home Health Services Ridgeview Medical Center Nancy Jaeckels Measurement/Implementation Advisor ICSI Janet Jorgenson-Rathke, PT Measurement/Implementation Advisor ICSI Loree Kalliainen, MD, FACS Plastic Surgery, Co-Work Group Leader HealthPartners Regions Hospital Stephanie Lach, MSN, MBA, RN Patient Safety & Quality HealthPartners Regions Hospital Karen Landeen, RN Radiology Hennepin County Medical Center Neal C. Rucks, PA-C Clinic Chippewa County – Montevideo Hospital & Clinic Cally Vinz, RN Facilitator ICSI Document History In response to ICSI hospital member's patient safety activities aimed at advancing efficient surgical process flow and creating safe and reliable practices that reduced the number of adverse events in surgery, in 2007 ICSI developed surgical protocols to allow for standardization in surgical processes such as safe site-marking, retained foreign objects and reduction of surgical site infection. In recognizing the many differences that exist specifically for safe site-marking for procedures outside of the operating room, a separate protocol was created in 2008 addressing just safe site-marking for procedures outside of the operating room. This protocol was consistent with the requirements set forth at that time by the The Joint Commission National Patient Safety Goals. Additionally, in 2007-2008 ICSI facilitated a Reliability Centered Surgical Care Redesign Collaborative, which provided a collaborative learning environment for participants to become knowledgeable in reliability theory and principles. This collaborative provided an opportunity for participants to share their learnings as they worked to implement this and other surgical related protocols. Return to Table of Contents Contact ICSI at: 8009 34th Avenue South, Suite 1200; Bloomington, MN 55425; (952) 814-7060; (952) 858-9675 (fax) Online at http://www.ICSI.org Copyright © 2012 by Institute for Clinical Systems Improvement 37 Non-OR Procedural Safety Fourth Edition/September 2012 ICSI Document Development and Revision Process Overview Since 1993, the Institute for Clinical Systems Improvement (ICSI) has developed more than 60 evidence-based health care documents that support best practices for the prevention, diagnosis, treatment or management of a given symptom, disease or condition for patients. Audience and Intended Use The information contained in this ICSI Health Care Protocol is intended primarily for health professionals and other expert audiences. This ICSI Health Care Protocol should not be construed as medical advice or medical opinion related to any specific facts or circumstances. Patients and families are urged to consult a health care professional regarding their own situation and any specific medical questions they may have. In addition, they should seek assistance from a health care professional in interpreting this ICSI Health Care Protocol and applying it in their individual case. This ICSI Health Care Protocol is designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients, and is not intended either to replace a clinician's judgment or to establish a protocol for all patients with a particular condition. Document Development and Revision Process The development process is based on a number of long-proven approaches and is continually being revised based on changing community standards. The ICSI staff, in consultation with the work group and a medical librarian, conduct a literature search to identify systematic reviews, randomized clinical trials, meta-analysis, other protocols, regulatory statements and other pertinent literature. This literature is evaluated based on the GRADE methodology by work group members. When needed, an outside methodologist is consulted. The work group uses this information to develop or revise clinical flows and algorithms, write recommendations, and identify gaps in the literature. The work group gives consideration to the importance of many issues as they develop the protocol. These considerations include the systems of care in our community and how resources vary, the balance between benefits and harms of interventions, patient and community values, the autonomy of clinicians and patients and more. All decisions made by the work group are done using a consensus process. ICSI's medical group members and sponsors review each protocol as part of the revision process. They provide comment on the scientific content, recommendations, implementation strategies and barriers to implementation. This feedback is used by and responded to by the work group as part of their revision work. Final review and approval of the protocol is done by ICSI's Committee on Evidence-Based Practice. This committee is made up of practicing clinicians and nurses, drawn from ICSI member medical groups. Implementation Recommendations and Measures These are provided to assist medical groups and others to implement the recommendations in the protocols. Where possible, implementation strategies are included which have been formally evaluated and tested. Measures are included which may be used for quality improvement as well as for outcome reporting. When available, regulatory or publicly reported measures are included. Document Revision Cycle Scientific documents are revised every 12-24 months as indicated by changes in clinical practice and literature. Each ICSI staff monitors major peer-reviewed journals every month for the protocols for which they are responsible. Work group members are also asked to provide any pertinent literature through check-ins with the work group mid-cycle and annually to determine if there have been changes in the evidence significant enough to warrant document revision earlier than scheduled. This process complements the exhaustive literature search that is done on the subject prior to development of the first version of a protocol. Return to Table of Contents www.icsi.org Institute for Clinical Systems Improvement 38