EUROPEAN UROLOGY 66 (2014) 898–905
available at www.sciencedirect.com
journal homepage: www.europeanurology.com
Surgery in Motion
Robot-assisted Laparoscopic Adrenalectomy: Step-by-Step
Technique and Comparative Outcomes
Luis Felipe Brandao, Riccardo Autorino, Homayoun Zargar, Jayram Krishnan,
Humberto Laydner, Oktay Akca, Maria Carmen Mir, Dinesh Samarasekera,
Robert Stein, Jihad Kaouk *
Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
Article info
Abstract
Article history:
Accepted April 8, 2014
Background: Recent evidence supports the use of robotic surgery for the minimally
invasive surgical management of adrenal masses.
Objective: To describe a contemporary step-by-step technique of robotic adrenalectomy
(RA), to provide tips and tricks to help ensure a safe and effective implementation of the
procedure, and to compare its outcomes with those of laparoscopic adrenalectomy (LA).
Design, setting, and participants: We retrospectively reviewed the medical charts of
consecutive patients who underwent RA performed by a single surgeon between April
2010 and October 2013. LA cases performed by the same surgeon between January 2004
and May 2010 were considered the control group.
Surgical procedure: The main steps of our current surgical technique for RA are
described in this video tutorial: patient positioning, port placement, and robot docking;
exposure of the adrenal gland; identification and control of the adrenal vein; circumferential dissection of the adrenal gland; and specimen retrieval and closure.
Outcome measurements and statistical analysis: Demographic parameters and main
surgical outcomes were assessed.
Results and limitations: A total of 76 cases (RA: 30; LA: 46) were included in the
analysis. Median tumor size on computed tomography (CT) was significantly larger in
the LA group (3 cm [interquartile range (IQR): 3] vs 4 cm [IQR: 3]; p = 0.002). A
significantly lower median estimated blood loss was recorded for the robotic group
(50 ml [IQR: 50] vs 100 ml [IQR: 288]; p = 0.02). The RA group presented five minor
complications (16.7%) and one major (Clavien 3b) complication (3.3%), whereas four
minor complications (8.7%) and one major (Clavien 3b) complication (2.3%) were
observed in the LA group. No significant difference was noted between groups in terms
of malignant histology ( p = 0.66) and positive margin rate ( p = 0.60). Distribution of
pheochromocytomas in the LA group was significantly higher than in the RA group
(43.5% vs 16.7%; p = 0.02).
Conclusions: The standardization of each surgical step optimizes the RA procedure. The
robotic approach can be applied for a wide range of adrenal indications, recapitulating
the safety and effectiveness of open surgery and potentially improving the outcomes of
standard laparoscopy.
Patient summary: In this report we detail our surgical technique for robotic removal of
adrenal masses. This procedure has been standardized and can be offered to patients,
with excellent outcomes.
# 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Keywords:
Adrenalectomy
Laparoscopy
Surgical technique
Robotic surgery
Please visit
www.europeanurology.com and
www.urosource.com to view the
accompanying video.
* Corresponding author. Center for Laparoscopic and Robotic Surgery, Glickman Urological and
Kidney Institute, Cleveland Clinic, 9500 Euclid Avenue/Q-10, Cleveland, OH 44195, USA.
E-mail address: kaoukj@ccf.org (J. Kaouk).
http://dx.doi.org/10.1016/j.eururo.2014.04.003
0302-2838/# 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.
EUROPEAN UROLOGY 66 (2014) 898–905
1.
Introduction
899
monitored intraoperatively to ensure hemodynamic stability during the
procedure and specifically during tumor manipulation.
To date, robotic surgery in urology remains mainly used for
extirpative procedures including significant reconstructive
components such as radical prostatectomy and partial
nephrectomy, whereas its use for purely extirpative
procedures such as nephrectomy and adrenalectomy is
more limited mainly because of cost issues [1].
Since the report of initial cases in 2002 [2], da Vinci
robot-assisted laparoscopic adrenalectomy (RA) has been
shown to be safe and feasible [3]. Recent evidence supports
the use of robotic surgery for minimally invasive surgical
management of adrenal masses and suggests that RA can be
effectively performed with operative time and complication
rates similar to laparoscopy, but with potential shorter
hospital stay and less blood loss [4].
The aim of the study is to describe a contemporary stepby-step technique of RA, to provide tips and tricks to help
ensure a safe and effective implementation of the procedure, and to compare its outcomes with those of laparoscopic adrenalectomy (LA) in the experience of a single
surgeon at a high-volume center.
2.
Methods and patients
2.1.
Study design
2.3.
Surgical technique
A detailed illustration of the surgical technique for RA can be found in the
accompanying video material.
2.3.1.
Robotic instrumentation
The da Vinci Surgical System (Intuitive Surgical Inc., Sunnyvale, CA, USA)
is used in a three-arm configuration, and the following robotic
instruments are used: 308 down scope, ProGrasp forceps, Hot Shears
(monopolar curved scissors), and a robotic clip applier. A monopolar
cautery hook and Harmonic ACE curved shears (Ethicon Endo-Surgery
Inc., CA, USA) can be also used when deemed helpful by the surgeon. We
do not routinely use a bipolar energy source.
Laparoscopic instruments are handled by the bedside assistant
including a Weck Hem-o-Lok clip applier (Teleflex Medical) and a
suction device.
2.3.2.
Patient positioning, port placement, and robot docking
The patient is placed in a 608 flank position. Extreme care is taken with
pressure points and correctly padding them with pillows and foams.
Tapes are used to secure the patient to the surgical table, which is mildly
flexed and positioned in a slight Trendelenburg position. The patient’s
arms are in a comfortable position, either both over a double arm board
or one placed along the side of the body.
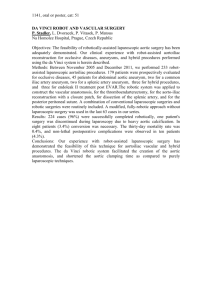
Similar to laparoscopy, precise port placement is essential to
maximize exposure and ease of surgery. Right- and left-side port
We retrospectively reviewed the medical charts of consecutive patients
configurations are shown in Figure 1. After creating pneumoperitoneum
who underwent transperitoneal RA performed by a single surgeon (J.K.)
by using a Veress needle, a 12-mm port is inserted above and lateral to
in our center between April 2010 and October 2013. Data were acquired
the umbilicus, at the lateral border of the abdominal rectus muscle
from our institutional review board–approved prospectively maintained
across from the 12th rib. Through this first port, the robotic scope is
database.
inserted and the abdomen is carefully inspected to rule out any
Transperitoneal LA cases performed by the same surgeon between
accidental injuries. Then the remaining ports are placed under vision
January 2004 and May 2010 were considered as the control group. The
including an 8-mm robotic port at the lateral border of the ipsilateral
two groups were compared in terms of surgical indications and
rectus muscle about 1 in below the costal margin, a second 8-mm robot
perioperative outcomes.
port about 2 in cephalad to the anterosuperior iliac spine, and a 12-mm
assistant port along the lateral border of the rectus muscle, halfway
2.2.
Preoperative assessment and surgical indication
[(Fig._1)TD$IG]
Indications for RA parallel those for LA including hormone-secreting
tumors (ie, aldosteronomas, glucocorticoid, androgen- and estrogenproducing adenomas), solitary small pheochromocytomas, hormoneinactive lesions >3 cm demonstrating growth over time on serial
imaging studies or >5 cm without observation, and rare lesions such as
myelolipomas.
Special indications are the removal of malignant tumors or
metastases. Increasing size and the suspicion of malignancy increase
the difficulty of the procedure. Contraindications include infiltrative
adrenal masses, involvement of large vascular structures or significant
involvement of adjacent organs, and large tumors. General contraindications include serious cardiac conditions, severe cardiac insufficiency, and uncorrected coagulopathy.
In general, a multidisciplinary management plan involving an
endocrinologist is followed in a patient presenting with an adrenal
mass. The adrenal gland is evaluated with a computed tomography
(CT) or magnetic resonance imaging to assess the location, size,
and functional characteristics of the mass. Metabolic parameters
(serum levels of aldosterone, cortisol, and catecholamines, as well as
urine levels of metanephrines) are assessed to identify functional
masses.
In cases of pheochromocytoma, patients are prescribed a preoperative 2-wk course of oral adrenergic blockade. Blood pressure is carefully
Fig. 1 – Port configuration for (a) right and (b) left robot-assisted
laparoscopic adrenalectomy.
900
EUROPEAN UROLOGY 66 (2014) 898–905
[(Fig._2)TD$IG]
[(Fig._3)TD$IG]
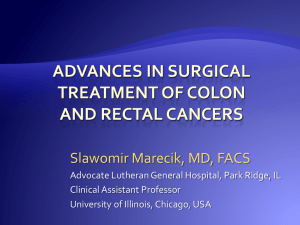
Fig. 2 – Operating room setup: The robot is docked over the shoulders of
the patient.
between the camera port and the lower robotic port. For the right-side
cases, an additional 5-mm port is placed below the xiphoid process in the
midline, to help retract the liver by using an Allis locking clamp.
To avoid clashing between the robotic arms, the ports must be
appropriately spread, about 8–10 cm distant from each other. In case of
obese patients, ports need to be shifted laterally and cephalad to
appropriately access the adrenal gland. This move is to avoid abdominal
contents obstructing the view.
Similar to a robotic partial nephrectomy procedure [5], the robot is
docked over the patient’s shoulder so its axis makes an obtuse angle in
relation to the patient’s axis (Fig. 2).
2.3.3.
Exposure of the adrenal gland
On the left side, complete medial bowel mobilization is needed to allow
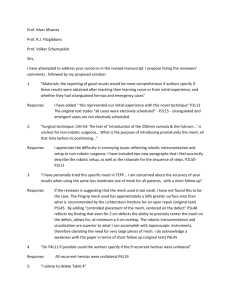
Fig. 3 – Left-side robot-assisted laparoscopic adrenalectomy. (a)
Intraoperative image showing the left adrenal vein emerging from the
left renal artery and tail of the pancreas medially; (b) illustration
showing the left adrenal vein emerging from the left renal artery.
gland exposure. The lateral attachments of the spleen, as well as
splenorenal ligaments, are divided. The spleen, bowel, and the pancreas
are mobilized medially until the adrenal gland is clearly visualized.
2.3.5.
Attention must be paid to the tail of the pancreas because it can be
Once the adrenal vein is properly controlled, the adrenal gland is
Circumferential dissection of the adrenal gland
mistaken for the adrenal gland.
circumferentially mobilized, beginning at the upper pole of the kidney,
On the right side, the triangular liver ligament is divided as cranially
progressing to the medial surface of the diaphragm, and finding a plane
as possible to release the liver, and the locking grasper (placed through
between the posterior surface of the adrenal and the psoas muscle. Care
the subxyphoid trocar) is used as a liver retractor. The posterior
must be taken during this step to control arterial blood supply (Fig. 5a
peritoneum overlying the upper pole of the adrenal can also be incised to
and 5b), which can be done using clips or the Harmonic ACE. Layers of fat
release the liver, which can then be retracted more superiorly. After
are left on the surface of the adrenal gland to use as a handle, thereby
properly retracting the liver, the right adrenal can be accessed with
minimizing manipulation of the gland and avoiding fracturing it.
minimal colon mobilization. For a better exposure of the inferior vena
cava (IVC), the duodenum can be medially mobilized as well. If this is the
2.3.6.
case, the use of cautery needs to be minimized to avoid duodenal
After checking the hemostasis by lowering the pneumoperitoneum, a
Specimen retrieval and closure
injuries.
laparoscopic entrapment sac is introduced by the assistant and the
specimen is placed into the sac. After undocking the robot, the bagged
2.3.4.
Identification and control of the adrenal vein
specimen is extracted by extending the incision at the level of the
On the left side (Fig. 3a and 3b), the renal hilum is identified, either
assistant port. A Carter-Thomason device (Inlet Medical Inc., Eden
by accessing it directly or after identifying and following the gonadal
Prairie, MN, USA) is used to close the 12-mm incisions. No drain is left in
vein cephalically. It is necessary to identify and dissect the left renal vein
place.
because the adrenal vein is a tributary branch of it. Then the adrenal
vein is carefully dissected and clipped by using the robotic clip applier,
2.4.
Postoperative care and follow-up
when available, or standard laparoscopic Hem-o-Lok clips placed by the
bedside assistant.
Intravenous fluids, analgesics, antibiotics, and prophylaxis for deep vein
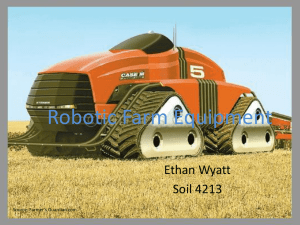
On the right side (Fig. 4a and 4b), after the duodenum is kocherized,
thrombosis are given per institutional protocol. Hemoglobin levels and
the lateral border of the IVC and the renal vein are identified. Dissecting
hematocrit are monitored. The patient is encouraged to ambulate
cranially along the lateral border of the IVC, the right adrenal vein is
gradually, and diet is advanced. The patient is discharged on the first or
encountered, dissected, clipped, and resected.
second postoperative day.
EUROPEAN UROLOGY 66 (2014) 898–905
[(Fig._4)TD$IG]
901
time, estimated blood loss, length of hospital stay, transfusions and
complications, total of morphine equivalents used, visual analog scale
(VAS) score on the first postoperative day and on discharge, and 30-d
readmissions. Postoperative complications were graded using the
Clavien-Dindo system. Pathology findings were analyzed including
pathologic tumor size, type of histology, and margin status.
Continuous variables were described as median and interquartile
range (IQR), and the categorical variables were reported as count
(percentage). Comparable analyses were performed using the Student t
test for parametric continuous variables; the Mann-Whitney U test was
used for nonparametric continuous variables. Chi-square tests were used
to compare categorical parameters. The Fisher exact test was performed
when required. Statistical significance was considered at p < 0.05.
3.
Results
3.1.
Demographics
Overall, 85 patients were identified. Nine LA patients were
excluded because a retroperitoneal approach had been
used. Thus 76 patients were ultimately included in the
analysis (Table 1). There was no difference between groups
in terms of age, BMI, gender, race, Charlson Comorbidity
Index, history of past abdominal surgery, and tumor
laterality. The RA group presented a significantly higher
number of patients with an ASA score 3 (80% vs 50%;
p = 0.015). However, the median tumor size on the CT was
significantly larger in the LA group (3 cm [IQR: 3] vs 4 cm
[IQR: 3]; p = 0.02).
3.2.
Fig. 4 – Right-side robot-assisted laparoscopic adrenalectomy. (a)
Intraoperative image showing the right adrenal vein emerging from the
lateral wall of the inferior vena cava (IVC); (b) illustration showing the
right adrenal vein emerging from the IVC.
2.5.
Data analysis
Collected demographics parameters were age, body mass index (BMI),
gender, Charlson Comorbidity Index, American Society of Anesthesiologists (ASA) score, history of past abdominal surgery, and incidental
[(Fig._5)TD$IG]
diagnosis. Main surgical outcomes were assessed including operative
Perioperative outcomes
Table 2 presents a comparative analysis of the perioperative
outcomes. No significant differences were noted in terms of
operative times between the two groups, whereas significantly lower estimated blood loss was recorded for the
robotic group (50 ml [IQR: 50] vs 100 ml [IQR: 288];
p = 0.02). Length of hospital stay and 30-d readmission rate
were comparable between groups. Median follow-up time
was significantly longer for the conventional laparoscopic
group (46 mo [IQR: 53.7] vs 4.5 mo [IQR: 6.5]; p < 0.001).
There was no significant difference in the use of
morphine equivalents per day during hospitalization
Fig. 5 – (a) Left-side and (b) right-side robot-assisted laparoscopic adrenalectomy. Illustration showing the circumferential mobilization of the adrenal
gland taking special care with arterial blood supply in either side.
902
EUROPEAN UROLOGY 66 (2014) 898–905
Table 1 – Demographic parameters
Characteristic
Age, yr
BMI, kg/m2
Race, white
Male gender
Charlson Comorbidity Index 4
ASA score 3
Past abdominal surgery
Tumor size, CT, cm
Incidentaloma
Side, left
Table 3 – Pathology findings
RA
(n = 30)
LA
(n = 46)
p value
62 (18)
29.5 (11.25)
27 (90)
12 (40)
5 (16.7)
24 (80)
8 (26.7)
3.0 (3)
15 (50)
18 (60)
54.5 (22)
29 (8.25)
40 (87)
25 (54.3)
11 (29.9)
23 (50)
22 (47.8)
4.0 (3)
30 (65.2)
12 (40)
0.09
0.67
0.49
0.24
0.56
0.015
0.09
0.02
0.23
0.24
ASA = American Society of Anesthesiologists; BMI = body mass index;
CT = computed tomography; LA = laparoscopic adrenalectomy; RA = robotassisted adrenalectomy.
Values expressed as median (interquartile range) and count (percentage).
( p = 0.42), as well as in VAS pain score assessment on
postoperative day 1 ( p = 0.64) and on discharge ( p = 0.78).
3.3.
Finding
Tumor size, cm
Malignant histology
Positive margin
Histology type
Adrenocortical adenoma
Pheochromocytoma
Myelolipoma
Metastasis
Adrenocortical carcinoma
Other
RA
(n = 30)
LA
(n = 46)
p value
3 (3)
2 (6.7)
0 (0)
4 (3)
3 (6.5)
1 (2.3)
0.02
0.66
0.59
18
5
2
2
0
3
(60)
(16.7)
(6.7)
(6.7)
(0)
(10)
13
20
2
2
1
8
(28.3)
(43.5)
(4.3)
(4.3)
(2.3)
(17.4)
0.009
0.02
0.64
0.64
0.59
0.51
LA = laparoscopic adrenalectomy; RA = robot-assisted adrenalectomy.
Values expressed as median (interquartile range) or count (percentage).
hyponatremia, and a pancreatic fistula that was treated
conservatively. Both major complications were extensive
postoperative bleeding that required surgical intervention
under general anesthesia.
Complications and transfusion rates
3.4.
There were no significant differences between groups in
terms of intraoperative complication rate ( p = 0.23), intraoperative transfusion rate ( p = 0.64), postoperative complication rate ( p = 0.32), and postoperative transfusion rate
( p = 0.64).
The RA group presented five minor complications
(16.7%) and one major (Clavien 3b) complication (3.3%),
whereas four minor complications (8.7%) and one major
(Clavien 3b) complication (2.3%) were observed in the LA
group. Minor complications in the RA group encompassed
one case of hyponatremia, an episode of nausea and
vomiting, a postoperative bleed requiring blood transfusion,
a wound infection, and an atrial fibrillation. The minor
complications from the LA group were a wound infection,
a postoperative bleed requiring blood transfusion,
Pathology findings are reported in Table 3. Median
pathologic size of the tumor was 3 cm (IQR: 3) in the RA
group and 4 cm (IQR: 3) in the LA group ( p = 0.02). There
were no differences between groups in terms of malignant
histology ( p = 0.66) and positive surgical margin rate
( p = 0.60).
The positive surgical margin in the LA group was
diagnosed as a pheochromocytoma on final pathology.
Overall, 66% of the robotic masses were adenomas, which
was significantly higher when compared with the LA group
(32.7%; p = 0.009). Nevertheless, the total amount of
pheochromocytomas in the LA group was significantly
higher than in the RA group (43.5% vs 16.7%; p = 0.02).
4.
Table 2 – Surgical outcomes
Outcome
Operative time, min
Blood loss, ml
Length of stay, d
Intraoperative complication
Intraoperative transfusions
Postoperative complications
Minor (Clavien 1–2)
Major (Clavien 3)
Postoperative transfusions
Conversion
Morphine equivalents, mg
VAS
POD 1
At discharge
30-d readmissions
Follow-up, mo
RA
(n = 30)
120
50
2
1
1
6
5
1
2
0
145
(33)
(50)
(1)
(3.3)
(3.3)
(20)
(16.7)
(3.3)
(6.7)
(0)
(171)
7 (3)
1 (3)
1 (3.3)
5.7 (6.5)
LA
(n = 46)
p value
120 (60)
100 (288)
2.5 (1)
6 (13)
4 (8.7)
5 (10.9)
4 (8.7)
1 (2.3)
2 (4.3)
1 (2.3)
52.9 (167)
0.59
0.02
0.17
0.23
0.64
0.32
0.30
0.63
0.64
0.59
0.42
6
0
3
46
(3)
(3)
(6.5)
(53.7)
0.64
0.78
0.48
<0.001
LA = laparoscopic adrenalectomy; POD = postoperative day; RA = robotassisted adrenalectomy; VAS = visual analog scale.
Values expressed as median (interquartile range) or count (percentage).
Histopathology
Discussion
Here we describe in a step-by-step fashion a standardized
technique of transperitoneal RA by providing tips and tricks
for a safe and effective implementation of this procedure.
As for any other robotic procedure, careful case selection
is of utmost importance for RA, especially during a surgeon’s
early experience. Indications include hormone-secreting
tumors, adrenal masses >5 cm, smaller lesions suspicious
for malignancy, and lesions increasing in size on serial
imaging [3]. Contraindications include infiltrative adrenal
masses and tumors of extremely large size because size of
adrenal lesions correlates with the potential for adrenal
carcinoma [6]. A known (or suspected) diagnosis of
adrenocortical carcinoma is better managed with open
surgery because there might be an increased risk of
recurrence and death compared with laparoscopy [7].
However, authors have advocated the feasibility of RA for
adrenocortical carcinoma [8].
In the present RA series, no adrenocortical carcinoma
was treated, and most of the masses were adenomas (60%),
with pheochromocytoma representing the second most
EUROPEAN UROLOGY 66 (2014) 898–905
common indication (16.7%). The lack of tactile feedback can
be of concern during dissection of pheochromocytoma
because inappropriate tumor manipulation can lead to
catecholamine release. Aliyev et al. recently reported a first
study focusing on RA for pheochromocytoma with a
comparison to the laparoscopic technique [9]. They found
similar perioperative outcomes, although larger tumors
were removed in the robotic group. Intraoperative hemodynamic parameters were also similar between the two
approaches. In our series, smaller tumor sizes were
observed in the RA group (median: 3 vs 4 cm; p = 0.02),
likely reflecting more careful selection criteria adopted in
the early robotic experience.
Morbidly obese patients have been considered at higher
risk of complications when undergoing LA [10]. Aksoy et al.
did not found any difference in perioperative outcomes
between RA and LA in obese patients, suggesting that
difficulties in maintaining exposure and dissection in obese
patients nullify the advantages of robotic articulating
versus rigid laparoscopic instruments in adrenal surgery
[11]. Notably, our RA population included obese and
morbidly obese patients with a high median BMI of
29.5 kg/m2, which reflects the referral pattern for our
tertiary care institution.
In laparoscopy, both the transperitoneal and retroperitoneal approach can be used effectively [12]. According to a
recent meta-analysis, the transperitoneal approach is the
preferred one for RA [4]. The larger operative field of this
approach aids in a better orientation and visualization of
familiar anatomic landmarks, which is particularly helpful
during the early learning curve. A larger working space is
useful for removal of larger adrenal masses. For RA, other
approaches to the adrenal gland also exist. Retroperitoneoscopy for RA was first described by Ludwig et al. [13]. This
approach offers direct access to the adrenal gland without
the need for visceral mobilization or lysis of adhesions from
prior abdominal operations and the ability to perform
bilateral adrenalectomy without repositioning the patient
[14].
As for laparoscopy, trocar configuration remains a key
factor in the operative setup for RA. In this study we
describe a port configuration similar to that we routinely
use for any robotic upper urinary tract surgery (ie, partial
nephrectomy, nephrectomy, or pyeloplasty) [5]. This is
based on the rationale of offering an effective and practical
disposition of the trocars in the setting of a teaching
hospital, where different residents and fellows are involved
in the case. Since the initial cases done at our institution in
2002 [2], we have modified the port setup so the upper
robotic port, the camera port, and the assistant port are
along the same line, but instead of this line being from the
umbilicus to the costal margin, it now corresponds to the
lateral edge of the ipsilateral abdominal rectus muscle.
Berber et al. suggested placing the first optical 12-mm
trocar midway between the umbilicus and the costal
margin, and two 8-mm robotic trocars 2 fingerbreadths
beneath the costal margin, and one 15-mm port for
the assistant, which is the most medial port for right-side
adrenalectomy and the most lateral port for left-side
903
procedures [15]. A similar configuration was suggested
by Brunaud et al. [16]. Krane et al. detailed their technique
for right-side RA and suggested placing the patient in the
full flank position, with 158 flexion of the table and using a
12-mm camera port placed 5 cm below the costal margin,
midway between the midclavicular and anterior axillary
line, and two 8-mm robotic ports placed to form an isosceles
triangle pointing toward the right adrenal, each about 8 cm
from the camera port. They also used an additional 8-mm
robotic port placed below the xyphoid to use the fourth
robotic arm and a 12-mm periumbilical port for the
assistant [17]. A four-arm approach was also described
by Giulianotti et al. [18], who placed the optical camera on
the lateral side of the pararectal line above the umbilical
transverse line and three robotic ports along a concave line
focusing on the adrenal fossa plus a 12-mm assistant port
placed near the umbilicus. In general, in our experience,
similar to robotic partial nephrectomy [5], there is no need
to use the third robotic arm, which translates into a cost
reduction.
Based on the same rationale, we minimize the number
of robotic instruments, so that we routinely use only a
ProGrasp forceps and monopolar Hot Shears for the
dissection of the adrenal gland as well as controlling the
vessels. Only if strictly needed, we selectively use other
tools such as the robotic clip applier, the monopolar cautery
hook, and Harmonic ACE curved shears. Others advocated
routine use of the Harmonic scalpel [19]. Taskin and
Berber suggested the use of the Harmonic energy also for
the division of the adrenal vein when <4 mm [15]. An
alternative way of controlling the vein is the use of a robotic
clip applier, which—thanks to the EndoWrist technology—
allows the console surgeon to achieve the best working
angle whenever the access is challenging for the bedside
assistant.
Identification of vascular structures represents the most
crucial and technically demanding step during adrenal
surgery. The dissection of the adrenal vein can be challenging
because of the unique anatomic location of the adrenal
gland. Understanding variant adrenal venous anatomy is
important to avoid bleeding, particularly in patients with
large tumors or pheochromocytomas [20]. In this regard,
extra attention to the venous anatomy is advised during right
adrenalectomy. The left adrenal vein is easier to divide
because it is longer and narrower; conversely, the right
adrenal vein is easier to identify but shorter and more
difficult to control. Adrenal arteries tend to be small and
indistinct, and they usually can be easily cauterized [21].
Recognizing the main anatomic landmarks during both
right- and left-side procedures is the best way to prevent
inadvertent intraoperative complications. On the left side,
the left renal vein, the tail of the pancreas, the superior pole
of the kidney, and the psoas muscle can be very helpful to
have a better exposure of the surgical field. On the right side,
it is important to visualize the edge of the IVC, the right
renal vein in addition with the superior pole of the kidney,
and, not less important, the psoas muscle. During our
adrenal dissection, the psoas muscle can be seen when
mobilizing the gland circumferentially.
904
EUROPEAN UROLOGY 66 (2014) 898–905
Regarding the surgical outcomes of RA, we observed a
low intraoperative complication rate (3.3%), which is in line
with other reported robotic series [22] and comparable with
LA [4]. The only statistical difference between RA and LA in
the present analysis was the blood loss, although it was of
limited clinical significance (D = 50 ml). We did not observe
any difference in terms of length of hospital stay, as
reported by Brunaud et al. [23] and confirmed by a recent
meta-analysis reported by our own group [4].
The learning curve represents an intriguing issue when
approaching a newly introduced surgical procedure. A
widely used surrogate parameter as a measure of the
learning curve is the operative time. Brunaud et al. observed
in their series of 50 RA procedures that ‘‘operative time was
reduced from 116 minutes for the first 20 patients to
87 minutes for the most recent RA group of patients
( p < 0.0003)’’ [23]. When performing the same kind of
analysis in our study population, we found that the last 20
RA cases presented better mean (standard deviation [SD])
operative time (131 31 min vs 150 104 min; p = 0.62),
less mean (SD) estimated blood loss (87 87 ml vs
312 771; p = 0.96), and shorter mean (SD) hospital stay
(2.6 1.2 d vs 2.2 1 d; p = 0.36); nevertheless, none of
the differences was significant. This might be related to the
limited sample size itself and by the fact that the console
surgeon had extensive previous experience with other robotic
surgical procedures including upper urinary tract and pelvic
surgery.
This study was intended to focus on our surgical
technique for RA and to report comparative outcomes
with LA performed by the same surgeon. In general, our
results are consistent with the studies available in the
recent literature and in line with a recent systematic
review and meta-analysis suggesting that RA could result
in a lower blood loss [4]. The small sample size and the
retrospective design of the study might be regarded as the
limitations of the study. It was outside our scope to provide
a formal cost analysis. Few studies have attempted to
assess the cost of RA compared with the laparoscopic or
open approach. Brunaud et al. estimated RA to be 2.3 times
more costly than LA [23]. Winter et al. compared median
operative charges and overall hospital charges for robotic,
laparoscopic, and open adrenalectomy. Although they
found that operative charges were over twice as much
for robotic versus open adrenalectomy, median hospital
charges were $1600 more for open adrenalectomy than for
RA or LA because of shorter hospitalizations for patients
who underwent minimally invasive surgery [22]. Contemporary prospective randomized studies are needed to
compare LA and RA conclusively. As robotic systems
become more widely used and the volume of robotic
surgery increases, maintenance, preparation, and cost
issues will become less burdensome, and the role of
robotics in adrenal surgery will be clarified.
recognition of main anatomic landmarks and the knowledge
of potential intraoperative complications, allow an optimization of this procedure. The robotic approach can be safely
and effectively applied for a wide range of adrenal indications, potentially improving the outcomes of the standard
laparoscopic approach.
Author contributions: Jihad Kaouk had full access to all the data in the
study and takes responsibility for the integrity of the data and the
accuracy of the data analysis.
Study concept and design: Brandao, Autorino, Kaouk.
Acquisition of data: Brandao, Laydner, Akca, Mir.
Analysis and interpretation of data: Brandao, Autorino, Zargar.
Drafting of the manuscript: Brandao, Autorino.
Critical revision of the manuscript for important intellectual content: Zargar,
Krishnan, Mir, Samarasekera, Stein, Kaouk.
Statistical analysis: Brandao, Zargar.
Obtaining funding: None.
Administrative, technical, or material support: None.
Supervision: Kaouk.
Other (specify): None.
Financial disclosures: Jihad Kaouk certifies that all conflicts of interest,
including specific financial interests and relationships and affiliations
relevant to the subject matter or materials discussed in the manuscript
(eg, employment/affiliation, grants or funding, consultancies, honoraria,
stock ownership or options, expert testimony, royalties, or patents filed,
received, or pending), are the following: Jihad Kaouk is a paid consultant/
speaker for Intuitive Surgical Inc.
Funding/Support and role of the sponsor: None.
Appendix A. Supplementary data
The Surgery in Motion video accompanying this article
can be found in the online version at http://dx.doi.org/
10.1016/j.eururo.2014.04.003 and via www.europeanurology.com.
References
[1] Merseburger AS, Herrmann TR, Shariat SF, et al. EAU guidelines
on robotic and single-site surgery in urology. Eur Urol 2013;64:
277–91.
[2] Desai MM, Gill IS, Kaouk JH, Matin SF, Sung GT, Bravo EL. Roboticassisted laparoscopic adrenalectomy. Urology 2002;60:1104–7.
[3] Hyams ES, Stifelman MD. The role of robotics for adrenal pathology.
Curr Opin Urol 2009;19:89–96.
[4] Brandao LF, Autorino R, Laydner H, et al. Robotic versus laparoscopic adrenalectomy: a systematic review and meta-analysis. Eur Urol
2014;65:1154–61.
[5] Kaouk JH, Khalifeh A, Shahab H, et al. Robot-assisted laparoscopic
partial nephrectomy: step-by-step contemporary technique and
surgical outcomes at a single high-volume institution. Eur Urol
2012;62:553–61.
[6] Kebebew E, Siperstein AE, Clark OH, et al. Results of laparoscopic
adrenalectomy for suspected and unsuspected malignant adrenal
neoplasms. Arch Surg 2002;137:948–53.
5.
Conclusions
[7] Mir MC, Klink JC, Guillotreau J, et al. Comparative outcomes of
laparoscopic and open adrenalectomy for adrenocortical carcinoma:
Our contemporary technique for RA is detailed in this study.
The standardization of each surgical step, based on the
single, high-volume center experience. Ann Surg Oncol 2013;20:
1456–61.
EUROPEAN UROLOGY 66 (2014) 898–905
905
[8] Zafar SS, Abaza R. Robot-assisted laparoscopic adrenalectomy for
[16] Brunaud L, Germain A, Zarnegar R, Cuny T, Ayav A, Bresler L. Robot-
adrenocortical carcinoma: initial report and review of the litera-
assisted adrenalectomy. Surg Laparosc Endosc Percutan Tech 2011;
ture. J Endourol 2008;22:985–9.
21:248–54.
[9] Aliyev S, Karabulut K, Agcaoglu O, et al. Robotic versus laparoscopic
[17] Krane LS, Shrivastava A, Eun D, Narra V, Bhandari M, Menon M. A
adrenalectomy for pheochromocytoma. Ann Surg Oncol 2013;20:
four-step technique of robotic right adrenalectomy: initial experi-
4190–4.
[10] Dancea HC, Obradovic V, Sartorius J, Woll N, Blansfield JA. Increased
complication rate in obese patients undergoing laparoscopic adrenalectomy. JSLS 2012;16:45–9.
[11] Aksoy E, Taskin HE, Aliyev S, Mitchell J, Siperstein A, Berber E.
Robotic versus laparoscopic adrenalectomy in obese patients. Surg
Endosc 2013;27:1233–6.
[12] Rubinstein M, Gill IS, Aron M, et al. Prospective, randomized
comparison of transperitoneal versus retroperitoneal laparoscopic
adrenalectomy. J Urol 2005;174:442–5.
[13] Ludwig AT, Wagner KR, Lowry PS, Papaconstantinou HT, Lairmore
TC. Robot-assisted posterior retroperitoneoscopic adrenalectomy.
J Endourol 2010;24:1307–14.
[14] Dickson PV, Alex GC, Grubbs EG, Jimenez C, Lee JE, Perrier ND.
Robotic-assisted retroperitoneoscopic adrenalectomy: making a
good procedure even better. Am Surg 2013;79:84–9.
[15] Taskin HE, Berber E. Robotic adrenalectomy. Cancer J 2013;19:
162–6.
ence. BJU Int 2008;101:1289–92.
[18] Giulianotti PC, Buchs NC, Addeo P, et al. Robot-assisted adrenalectomy: a technical option for the surgeon? Int J Med Robot 2011;7:27–32.
[19] Agcaoglu O, Aliyev S, Karabulut K, Siperstein A, Berber E. Robotic vs
laparoscopic posterior retroperitoneal adrenalectomy. Arch Surg
2012;147:272–5.
[20] Scholten A, Cisco RM, Vriens MR, Shen WT, Duh QY. Variant adrenal
venous anatomy in 546 laparoscopic adrenalectomies. JAMA Surg
2013;148:378–83.
[21] Joel AB, Rubenstein JN, Arredondo S, Meng MV, Duh QY, Stoller ML.
Laparoscopic appreciation of the adrenal artery: fact or fiction?
J Endourol 2005;19:793–6.
[22] Winter J, Talamini M, Stanfield C, et al. Thirty robotic adrenalectomies: a single institution’s experience. Surg Endosc 2006;20:
119–24.
[23] Brunaud L, Bresler L, Ayav A, et al. Robotic-assisted adrenalectomy:
what advantages compared to lateral transperitoneal laparoscopic
adrenalectomy? Am J Surg 2008;195:433–8.