Change Management
advertisement

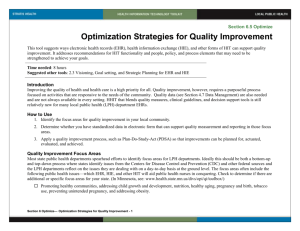
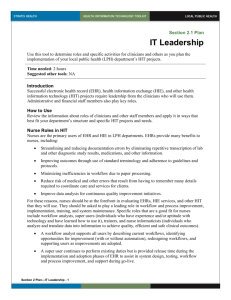
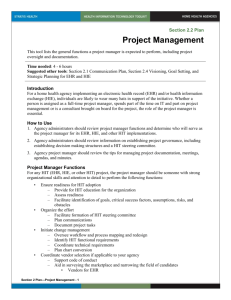
Section 2.5 Plan Change Management This overview describes change management, including change stages, transformation, agents of change, and possible barriers to making changes in your home health agencies. Time needed: 4 hours Suggested other tools: NA Introduction Change is one of the most difficult behaviors to affect. While few people are willing to articulate why change is so difficult for them on a personal level, change is frequently viewed as shifting the balance of power—and no one likes giving up what they perceive as power. An impending change often results in fear, resistance, and even sabotage. How to Use Use this tool to learn about change management strategies. Use the force field analysis tool, described below, to have a discussion about these issues with your staff and prepare for the changes that new health information technology (HIT) may bring. Stages of Change Unfortunately, no magic wand is available to affect change. Some studies suggest that change requires progression through stages, such as the five stages of the grieving process in death (denial, anger, bargaining, depression, and acceptance), where loss of the familiar paper and pen are often accompanied by denying the need to learn to use a computer, becoming angry with those requiring use of HIT, seeking incentives or other means of getting something in return, becoming depressed about one’s own inadequacies, and ultimately accepting that this is the way of the future. Several studies support the idea that change requires pre-contemplation, contemplation, preparation, action, and maintenance—often over a fairly significant amount of time, or at least more time than is often devoted to HIT acclimation. Other change management experts describe a process that entails: unfreezing old habits by pointing out deficiencies in paper records and the value of the new technology in providing clinical decision support; making the change through engagement, education, training, and support; and then refreezing the change into new habits through continual reminders, reinforcement, enforcement, support, and celebration of the new technology’s results. All of these suggest a common theme—that change is complex and people progress through multiple stages before real change occurs. Practice Transformation Practice transformation ultimately means changing the practice of medicine in order to improve the quality and cost of health care. Practice transformation can be achieved without HIT, but usually is improved with use of HIT in general and electronic health record (EHR) and health information exchange (HIE) systems in particular. Regulations, staffing, reimbursement, cost, malpractice, report cards, and other issues have catapulted organizations to seek a significant revamping of their workflows and processes to meet requirements, recruit and retain good staff members, optimize reimbursement, reduce waste, reduce errors, and address public concerns. Clinical quality is now at Section 2 Plan—Change Management - 1 the forefront of all health care organizations’ concerns. Practice transformation suggests some hallmarks that are different from previous approaches to change in health care organizations: Clinically-focused. EHR and HIE have largely been on the periphery of the core business of health care. Financial, administrative, and operational systems have been widely implemented; clinical systems and health information exchange are the next frontier. Clinical information systems focus directly on the core business of health care—taking care of patients. The resulting clinical transformation programs have focused on the effectiveness and efficiency of care delivery. Integrated. Many of the financial, administrative, and operational/departmental systems were largely standalone and sometimes only interfaced to share limited demographic data—not truly integrated. Moving from one application to another is not seamless. To transform clinical processes, all current and new systems must serve as source systems linking directly to one another or through a data repository. Comprehensive. Practice transformation relies on having access to all data for processing into the right presentations of information and into clinical decision making. Although home health agencies may go through a transition period in which they operate with hybrid record systems (some parts on paper and some parts electronic), the ultimate goal is to electronically capture data from all sources for use in care delivery, management, and operations. Knowledge-based. Clinicians are knowledge workers and demand that systems intended to support them be knowledge-based. Financial, administrative, and even operational/departmental systems have primarily addressed clerical and operational tasks. While clinicians would be hard-pressed to function without such systems, they are affected more directly by clinical systems. But if clinical systems do not provide information based on solid evidence, they offer minimal value to the clinician. Further, knowledge is continually evolving and changing. Agencies must recognize that HIT is dynamic and must be continually assessed for accuracy and appropriately supported. Outcome-oriented. Practice transformation is about achieving better outcomes. If there were ways to achieve better outcomes without major investments in information technology, these would be readily adopted. HIT systems are recognized as significant contributors to improving patient safety and quality outcomes. Change Strategies Change management for EHR and HIE is not only about recognizing the stages required to accept change and the clinical transformation, but about applying strategies to support change. One element of developing a change management strategy is understanding the agency’s innate change management style. Every organization has some way of introducing and requiring even moderate amounts of change. Most effective change managers recognize this and either work within the existing organizational culture or attempt to move the organization to a more positive culture. One or more of the following types of change management strategies is typically found in every organization. Although each can be effective, the general school of thought is that the most effective and longest lasting change is achieved through a behavioral norm-based strategy. Behavioral norm-based strategy is when behavioral norms or expectations are changed by organizational leadership and/or external factors. An example is the promotion of EHR and HIE because it is recognized as an important contribution to clinical transformation. There is complete transparency in discussing why change is needed and each stakeholder wants to continuously improve. This approach helps everyone work together to make the change happen. Early adopters of EHR and HIE found themselves using this change management strategy. An excellent example is found in Minnesota where the MN Community Section 2 Plan—Change Management - 2 Measurement project has contributed to competitiveness, with each clinic continuously striving to improve. Incentive-based strategy is one in which conformance is rewarded. This is becoming more popular as payers have announced pay-for-performance incentives for HIT adoption. The most prominent incentive today is the federal meaningful use of EHR incentives for hospitals and physician offices. Still, some experts fear that once the incentive is removed organizations will slip back into old ways, or that forward progress will stop. Sanction-based strategy may be viewed as the opposite of the incentive-based strategy, where nonconformance is penalized. Payers may introduce disincentives, such as Medicare slowing payment of claims that are not filed using the HIPAA-required electronic transactions, withholding some payment from hospitals that do not participate in voluntary quality reporting, or reducing the fee schedule for physicians who do not use e-prescribing. The federal meaningful use incentive program for EHR adoption includes sanctions for not adopting EHR by the specified date. Adoption-based strategy is one in which change happens over time, such as giving nurses the option of whether they will use an EHR to document assessments and notes. This type of strategy may sometimes be useful, but with today’s focus on clinical transformation, most organizations do not have the time or resources to accommodate it. The strategy essentially requires running dual processes—paper records and electronic records— until everyone decides to adopt the new technology. Such a strategy is costly and a hybrid record environment is confusing and poses potential patient safety issues. Agents of Change Another key strategy in managing change is recognizing that the project manager, administrator, director of nursing, or IT staff is not the sole change agent. In fact, everyone involved in the process of HIT adoption needs to be a change agent. Discussing the skills that change agents need with members of the HIT steering committee and all supervisors can be well worth the time. Each person may need to reflect upon the following skill requirements and hone them for the good of the agency: People skills are essential to understand the diversity among all individuals, skill sets, and positions that are impacted by HIT. Effective change managers are able to listen, restate, reflect, clarify without interrogating, draw out the quiet, quiet the verbose, channel discussion, plant ideas, and develop trust and confidence among users. Political skills are needed to understand the various viewpoints and counterpoints that may arise during discussion about HIT. System skills help organize and manage the technology while translating this into language that users will understand and respect. Analytical skills ensure that workflow and processes are not only understood and appropriately improved upon, but also are used to assess and manage the financial impact of change. Business skills are needed to understand the underlying way the health care organization works and the underlying clinical processes. Change agents need be able to “talk the talk” and “walk the walk” related to their roles. MN Community Measurement. http://mncm.org/ Section 2 Plan—Change Management - 3 Recognizing and Responding to Resistance to Change Reading people and preparing to respond to their concerns about change is an important task for change agents. Individuals react and adopt to change in different ways—from threatening to leave to actively supporting the change. Reading reactions and responding appropriately is very important. This is especially true for those known to be “informal leaders” or “opinion leaders” who you want to support change and not sabotage it. Common reactions to change and how to respond include: Leaving. Some clinicians indicate that they will retire before adopting EHR or HIE. Some can be convinced to stay and serve the organization well if their active resistance can be channeled into representing a resister’s viewpoint for the good of the project. However, if this is not possible, simply acknowledge these individuals’ accomplishments and let them make their own decisions. Threats by physicians to take their business elsewhere are generally no longer very effective, as most home health agencies are either adopting EHR and HIE or have them on a future agenda. Young physicians who are interested in geriatrics or using the home health agency to supplement their practices are very interested in EHR. Replacing nurses may not be as easy, so putting effort into education and engagement will be essential for the bulk of your user community. Active resistance. In active resistance, the individuals are clear about how they feel and can benefit an HIT project if their resistance can be channeled into representing a resister’s viewpoint for the good of the project. Once active resisters are turned around, they can be equally active in their support. Active resisters often do not threaten to leave, either because they are not old enough to retire or know other facilities are also adopting EHR and HIE. They are easier to influence than those threatening to leave. It is important to turn them around because their resistance can be infectious. Opposition. A person who opposes EHR and HIE but is not an active resister can be the most difficult to identify and turn around. Often, this is a person who is negative about everything and potentially depressed. Offering life/career counseling to such individuals can yield substantial benefits for the EHR and HIE projects and for the individual. Acquiescence. An individual who grudgingly accepts HIT is someone who who could swing to either opposition or acceptance. Monitor these individuals closely and involve them with specific tasks and recognition for work well done. Acceptance/modification. An individual who claims to accept the project but continuously offers ideas for modifications can put a project at risk for delay or going over budget. Often, a person with such a reaction actually opposes the project and is trying to avoid using the system or any change it may be designed to impose. This exuberance for modifying the new system back to old ways absolutely needs to be managed immediately. Acceptance. A person who quietly accepts change is certainly one to be appreciated. However, such individuals can contribute more to the process of turning others around if they are more actively supportive. They should be encouraged, if not called upon, to describe their interest. Active support. Genuinely active supporters should be greatly appreciated. Their energy and enthusiasm should be channeled into constructive help. Reading People A final consideration is to learn how to read the various responses people may have to an HIT project. Supervisors and managers should try to understand the thoughts of staff people who react with silent opposition or acceptance. One way to do this and start the change management process is to engage these individuals in visioning (see Section 2.4 Visioning, Goal Setting, and Strategic Planning) or to use a force field analysis that helps everyone put driving forces and restraining forces Section 2 Plan—Change Management - 4 for EHR and HIE projects on the table. If done in a way that is not personal, but instructive to the organization, the force field analysis process can be revealing and help to educate everyone. Force Field Analysis Tool The following provides the structure for force field analysis, with some examples of responses you may expect to hear. When using this technique, let participants articulate driving and restraining forces (see tool below) themselves. Avoid filtering or judging any of the comments. Record them as they are described. Capture how people feel about the issues—not whether you think they are right or wrong. Start asking for national/state factors driving HIT and progress down to institutional and personal factors. This helps participants recognize this is not focused just on them or intended to be punitive. Ask the group to describe the strength or importance of the force and illustrate this by the length with which the arrow extends into the Key Factors field. Repeat these steps with the restraining forces. Next, hold a discussion about what the responses mean. Hopefully any myths that surface can be debunked. Reinforce positive forces. Keep the focus positive but realistic, acknowledging risk factors to be addressed. Change is much more likely to be accepted when perfection is not expected. Use the following template to conduct a force field analysis in your agency. Note, you might wish to keep the analysis and periodically review it or even conduct the process afresh to see if change is taking place. Driving Forces Key Factors National/State Factors Institutional Personal Force Field Analysis Example Copyright © 2014, Margret\A Consulting, LLC. Used with permission of author Section 2 Plan—Change Management - 5 Restraining Forces Copyright © 2013 Section 2 Plan—Change Management - 6 Updated 03-10-14