Influence of Health Care Reform on the Availablity and Quality of
advertisement

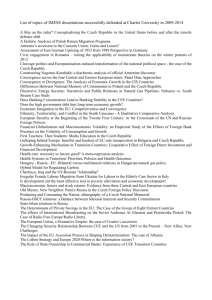
_________________________________________________________________________ Influence of Reforms on Availability and Quality of the Czech Health Care _________________________________________________________________________ Irena Jindrichovska1 and Ivana Funkova2 Abstract: Health care sector is essentially a very important industry in every developed democratic country, especially in Europe. This paper concentrates on assessment of the impact of ongoing reforms of Czech health care system on patients. The empirical part of this study concentrates on the core hospitals providing medical services in every statutory district across the country. We assess the changes after 2003 when the reform started to be implemented in practice, and in particular we consider the recent changes in legal status and ownership of hospitals in 2011. The paper comes to the conclusion that services for population are reduced and are becoming more costly at the same time. As to the availability of health care, health care is still available, but the on-going reforms make it less accessible. We suggest that this result is a combination of bureaucracy and ill-management of the process. Keywords: Health care, reform, public sector, privatization, hospitals JEL classification: I11, I18, H41 1. Introduction Health care as part of national economy is one of the most closely monitored followed sectors. Health issues affect all age groups. Even though the health care is not the only factor that determines the health of population the availability of drugs and good treatment can significantly affect the quality of human life. The health care system in the Czech Republic is the only sphere traditionally dominated by the state that went through radical reform after the political changes at the end of 1989 (Vyborna, 1994; Uldrichova, 1996; Anderson, 2009). The new health care system is strongly orientated towards the private provision of health care and is striving to introduce a sense of personal responsibility of individuals for the status of their health. It is possible to conclude that this fact is explicable by the strong support and active co-operation of health care providers in the preparation and realization of health care reform. Each country has its own specific system of health care with different institutions and relationships among them. Ideal system does not exist. Although the reform must be based on the specific situation of the state we can observe similar tendency in all countries. Different systems are analyzed by international health organizations (Matl et al., 2009). University of Economics and Management, Nárožní 9a, 150 09 Praha 5, Czech Republic, e-mail: irena.jindrichovska@seznam.cz 2 University Hospital Motol, V Úvalu 84, 150 06 Praha 5 – Motol, Czech Republic, e-mail: ivana.funkova@fnmotol.cz 1 In the Czech Republic the new system suffers from the common problem of all health care systems – the difficulty of controlling increasing costs. The reform of the health care system contributed to cost increases by imposing an additional administrative cost for the creation of a system of health insurance companies, by technical mistakes in the system of price regulation, and by introducing a pure fee-for-service reimbursement system in combination with of new fee-for- service price list. Nevertheless the new system is compatible with new market orientation of the whole economy and did not distort the accessibility or quality of health care in the interim transitory period. In the future, the Czech health care system will most likely follow the path on which it has embarked during 1990s. It will concentrate on improvements in the structure of health insurance and price regulation, and on introducing cost-combating modifications of the feefor-service system (Vyborna, 1994). All Eastern European countries of post communist block have gone through a period of rapid and major change in every sector, including health, since the revolutions of 1989. Major reforms were executed since 1989 and by 1998 the previously centralized, tax-based system had been transformed into a decentralized and pluralistic social health insurance system with contractual relationships between purchasers, health insurance funds and health care providers (Cosoveanu et al., 2009). In the Czech Republic the healthcare program is based on a model of a welfare state. This concept is a heritage given by the historical development after the Second World War that was maintained and developed for several decades until the Velvet Revolution in 1989. After the 1989 the system has changed. There was not a steady flow of financial resources directly from the state budget but hospitals and other medical facilities started to be reimbursed for health care provided by newly established health insurance companies. Stream of revenues that goes to health care institution is a combination of direct payments and payments in form of reimbursement by the Ministry of Health established by legislation (Jindrichovska et al., 2011). The structure of our paper is as follows: The first part is the introduction and motivation. To gain some more perspective on this issue the second part provides a short summary of previous literature. The third part presents brief characteristic of health-care funding in the Czech Republic and approaches to health care funding in Eastern Europe. The fourth part characterises changes of the health care system in the Czech Republic and explained recent changes especially in regional hospitals that serve the widest part of population. The fifth part presents a discussion of recent development – issues of availability and quality. The last part provides conclusion and recommendations. 2. Previous literature In the Eastern Europe the health care was under the scrutiny several times. The work of selected authors, which have recently explored this topic, is summarized in the following table. 2 Table 1. Recent literature on health care in Czech Republic and Eastern Europe Author(s) (year) Vyborna, O. (1994) Uldrichova, V. (1996) Jevcak, A. (2006) Anderson, L. S. (2009) Country Czech Rep. Czech Rep. Slovakia Czech Rep. Cosoveanu, G., Dlouhy, M., Czech Rep., Hinkov, H. and Cizmarik, P. Slovakia, (2009) Romania and Bulgaria Matl, O., Pavlokova, K., Czech Rep. Roubal, T. and Vachek, S. (2009) Sova, A. (2010) Czech Rep. Jindrichovska, I., Peskova, Czech Rep. R., Funkova, I. and Nesladkova, E. (2011) Research question The Reform of the Czech Health Care System Liquidation of state monopoly of Health care Unpopularity of Health Reforms in Slovakia Political issues related to the Czech Health Care Reforms Mental Health Financing in several East European countries Sustainability models of Czech health care Long term care in the Czech Republic Efficiency Management of the Czech Health Care To ease the classification we have grouped the literature into several blocks. Goals of Health Care reform To summarize the bulk of recent work we start with Vyborna (1994) who claims the health care system is the only sphere traditionally dominated by the state that went through radical reform after the political changes at the end of 1989. The following new health care system is strongly orientated towards the private provision of health care and it is striving to introduce a sense of personal responsibility in individuals for their own health. Therefore the strong support and active co-operation of health care providers in preparation and realization of health care reform is needed for successful end result. The reform of the Czech public health system started in 1991. The main goals were the liquidation of the state's monopoly on health services and creation of non-state health care that would include private facilities. Another goal was the introduction of multi-resource financing for health care that respected the principle of social solidarity (Uldrichova, 1996). International Experience – post socialist block Situation in Slovakia was characterized by Jevcak (2006), who claims that although many painful reforms have been adopted in Slovakia over the last couple of years, the only one, which is clearly disliked by the public, is the reform of the healthcare system. The reform introduced profit-making and hard budget constraints into the system in an effort to increase efficiency. However, up to these days the reform did not significantly increase choice or responsiveness in insurance coverage and medical treatment. Four country characteristic was summarized by Cosoveanu et al. (2009), who assert that all the four countries have started mayor changes in their systems of purchasing and financing mental health care. The diversities due to different context as well starting points in the reforms could be overcome. The information gap identified is a challenge for the countries (Cosoveanu et al., 2009, p. 1). In the Czech Republic and Slovakia a compulsory public health 3 insurance system replaced the tax-financed system in 1993. In Slovakia, as a part of social insurance; public health insurance was separated from the social insurance in 1994. Public health insurance is the major source of health financing in the country; the direct expenditures of the national and local governments are low, but stable. Altogether, public financing covers 90 percent of health expenditures in the Czech Republic and 80 percent in Slovakia; the share of private spending is relatively low, but growing (Cosoveanu et al., 2009). Political issues and sustainability of reforms Anderson (2009) characterizes the transition as the fundamentals transformation from a Soviet-style health system in which the government paid for and provided all healthcare to citizens free at point of service to a new system with compulsory health insurance provided by multiple, quasi-private health insurance funds and a mix of public and private providers. Although costs had been low under the old system, healthcare expenditures rose dramatically under the new social insurance model and by the mid 1990s the financial sustainability of the post-communist health system was in question. Matl et al. (2009) concentrated on the long term viability of the Czech healthcare system and models of financial sustainability of Czech healthcare. Their study offers detailed information about the possibilities and limits of forecasting and predicting revenues and expenditures of the public healthcare sector. Sowa (2010) studied the problem of ageing and explored a question, how to develop an efficient and sustainable long-term care systems for elderly responsive to needs. This question is imminent, due to rising demographic pressures and becomes an urgent matter all over the Europe. Czech Republic is among the countries that have redesigned long-term care system according the principles of accessibility, quality and fiscal tenacity in the past couple of years. The reform process was well rooted in the practice of local governments and social sector empowering institutions that existed before 2006, when the reform was introduced, but were insufficiently anchored in legal regulations. Health care quality and efficiency Jindrichovska et al. (2011) concentrated on health care efficiency management and funding in the Czech Republic. In their study they were exploring how both the financial and non-financial measures operate in two representative Czech university hospitals. The general recommendations for efficiency improvements in health care sector in the Czech hospitals are to significantly reduce their costs, with use of outsourcing and lowering costs of medical materials with the use of auctions. The system of control can be used as a non-financial indicator, which can serve in evaluation of medical institutions. The system of control which is used in organisations contributes to reducing inefficiencies and improves quality of provided medical services and also efficient use and allocation of financial resources 3. Funding of health care in the Czech Republic In Czech Republic health insurance funds receive their budgets by directly collecting contributions from the insured inhabitants. Contribution rates amount to 13.5% of the gross income, paid by employers and employees in a 9% to 4.5% ratio. Self employed contribute 13.5% from profit. For pensioners, students, children, the state budget allocates a capitation payment for each non-waged person. About 53% of the population is insured through the state. There is a yearly minimum and maximum health insurance contribution. There is a risk 4 pooling procedure. The collected contributions are redistributed among funds on the basis of risk of age groups – there are different weights for different age groups (Cosoveanu, 2009, p. 4). The health care legislation in the Czech Republic is regulated mainly by the Act No 48/1997, on Public Health Insurance. This law gives an opportunity to every Czech citizen to use any medical institution supplying urgent care (emergency and ambulance) or to institution with a valid contract with Insurance Agency to provide medical treatment. There is an element of solidarity and equity in the Czech health care. In the Czech Republic the healthcare program is based on a model of a welfare state. This concept has been inherited from the historical political development after the Second World War. This system developed for several decades until the Velvet Revolution in 1989. Both funding and budgeting systems in medical care are specific due to particularities of the sector. This means that a patient does not pay directly for medical services provided. The health care system is set up for the public provision of treatment. Therefore, it has been very difficult to implement private medical facilities that could by the scope of provided services be similar to established public hospitals. The impossibility to compete basically gradually divided the market into services which are almost exclusively provided by the private clinics (e.g. laser eye surgery, aesthetic surgeries, assisted reproduction etc.) and the overwhelming majority of the rest of medical services is provided by public hospitals. Private clinics provide particular medical services, because the level of reimbursement is making them profitable and these services are almost solely provided by them. Private medical facilities provide services mostly for direct cash payments. This system of funding makes them independent on the insurance companies, and thus leaves them the space for standard non-regulated way of competition. The public hospitals cover all other types of medical treatments. Even though the standard of supplied services differs vastly among the public facilities across the Czech Republic, the providers are basically not allowed to compete. The reimbursement for particular treatment is specified by the Ministry of Health and it is the same for everybody. In other words, hospitals always get the same contribution, no matter the quality provided. This aspect is recently changing with new reforms that bring more concentration in the sector and closures of regional medical facilities. This is very different from the approach of private commercial entity and it also partially explains why at the same market there is usually no space for both public and private medical facilities. In the Czech Republic the health care expenditures represented about 6.9–7.5 per cent of the GDP total expenditures in the period from 2004 to 2010. This is comparable to European standard, as it can be seen in Figure 1. As it concerns the budgeting of individual hospitals and health care institutions the current reimbursement system in the Czech health care is unfavourable to the private medical facilities in the sense that the amendments to the contracts with insurance companies are signed retroactively for the given year. Funding of health care is provided from two major sources firstly by cost-sharing as part of health insurance and secondly by direct payments for private health services. In Czech Republic prior to January 1, 2008: 1. Cost-sharing was a part of public insurance: reference pricing for drugs, some dental services, and some other really marginal services. 5 2. Direct payments were executed for private services: medical examinations not directly related to health (e.g. certificates for issue of driving licences, or for life insurance), over-thecounter drugs and some private services (plastic surgery, above-standard dental services etc.) or any services provided by provider without a contract with the public insurance (which is rather exceptional). New payments provisions were introduced in January 1, 2008. Patients pay 30 CZK for each outpatient visit; they also pay 30 CZK for drug prescription, 60 CZK per inpatient day, and 90 CZK for emergency treatment. This is all added to all payment services that were instituted prior to January 2008 as mentioned above. There are no differences between physical and mental health (Cosoveanu et al., 2009, p. 6). Starting December 1, 2011 there was also an increase of the fee for an overnight stay in hospital to CZK 100 per night. Figure 1. Health care expense as a percentage of GDP per country 20,0 18,0 16,0 2004 14,0 2005 12,0 2006 10,0 2007 8,0 2008 6,0 2009 4,0 2010 2,0 USA Turkey Switzerland Spain Sweden United Slovakia Austria Greece Poland Portugal New Norway Netherlands Mexico Germany Hungary Korea Luxembourg Canada Italy Japan Ireland Iceland France Finland Belgium Denmark Czech Australia 0,0 Proportions of health care expenditures on country GDP (Europe in years 2004–2010), http://www.oecd.org/els/healthpoliciesanddata/oecdhealthdata2012-frequentlyrequesteddata.htm, cited on 22-082012. This graph shows the health care expenditures of the Czech Republic in comparison with OECD countries. The expenses of Czech Republic are reasonably low about 6.9–7.5 per cent of total GDP in comparison with other developed countries both in and outside Europe. 4. Changes in the network of district hospitals and impact on health care availability After 1989 the Czech health care has undergone extensive transformation. Prior to 1989 health care was managed centrally by the state and it was financed from taxes. Subsequently, the hospitals and equipment was transferred to the public health care system and health insurance companies have been established to take responsibility for organization and funding3. In the Czech Republic all health care facilities initially belonged to state. After 1989, the introduction of a new system was accomplished and the Regional Institutes of National Health were abolished and associated equipment in them was transferred under the administration of 3 http://www.uzis.cz/katalog/mimoradne-publikace/vyvoj-zdravotnictvi-ceske-republiky-po-roce-1989, 31-01-2012]. [cited 6 the Ministry of Health. In 1991 the Ministry of Health issued a new the Decree No. 242/1991 Coll., on the system of health care facilities established by district authorities and municipalities, which governed the decentralization of the district national institutes of health into smaller, economically separate and distinct legal entities. In connection with the approval of the new health care system there was an amendment to Act No. 20/1966 Coll. by the Health Care Act No. 548/1991 Coll. issued in 1991. The Act No. 551/1991 Coll., on the General Health Insurance Company of the Czech Republic established set up the concept of health insurance and the General Health Insurance Company was established. In 1992 the Act No. 280/1992 Coll. set up further departmental, professional, and business health insurance companies. Health insurance market is not regulated by the state, and at the beginning there was a gradual decline, which caused a collapse of several health insurance companies. Currently, there are nine well-functioning health insurances on the Czech market. The health system that has been in existence since 1996 was funded by performance payment, which led for chasing points. Since 1997 the funding for health insurance was changed to capitation payments for physicians and advance payments derived from the previous period in hospital inpatient care. The performance system remained in power only for outpatient specialists. In 1992 the Act No. 160/1992 Coll. was adopted. This has transferred the healthcare into private health care institutions and privatization of healthcare facilities started. Creating a network of medical facilities in the territory is subject to Law No. 20/1966 Coll. about the care and health of people, as amended. Significant changes occurred in the inpatient care in 2002. Then in accordance with the Act No. 290/2002 Coll. further transfer of other equipment, rights and obligations of the Czech Republic to the regions and municipalities was executed. This reorganisation started in 2003, and a total of 82 hospitals were transferred to regions and municipalities. At that time many health facilities were running huge debts and regional authorities were faced with the possibility of failure of medical facilities. At the same tome they had a difficult task to guarantee health care to the extent and quality that the patient was a Czech patient was accustomed. Nowadays, region is the only shareholder in 17 facilities. In 2004, further transfers to regional and later urban hospitals were executed. In 2005 the parliament managed to push through a law that does not allow the transfer of governmental organizations and companies. Due to the gap in the law regions managed to further transform the hospitals. The parliament of the Czech Republic failed to enforce the law on public or non-profit organizations and law on university hospitals, which would regulate common workplace learning in teaching hospitals. This enabled the transfer of certain other things, the rights and obligations of the Czech Republic to the regions and municipalities, civic associations active in the field of physical education and sport and related changes and amendments to Act No. 157/2000 Coll., on the transfer of certain assets, rights and liabilities from the Czech Republic, as amended by Act No. 10/2001 Coll., and Act No. 20/1966 Coll. on Health Care, as amended. The region was transferred 1 to 1. In the year 2003 medical institutional care facilities (district hospitals and other medical institutions) with the exception of state contributory organizations whose functions founder passes from district offices to the Ministry of Health – Annex 3 cit. law. 7 The health care regional network is regulated by the Act No. 290/2002 Coll., which is ensuring the availability of outpatient health care, and which is entrusted the jurisdiction of the regions with regard to the local conditions of the area – population density, transport services, geographic conditions of the region and its demographic indicator. Creation of the network of healthcare facilities is also ensured by announcing tenders, where the is director is region with delegated powers for the purpose of entering into contractual relations for the provision of health care to non-medical facilities and health insurance companies. 4.1 Current state of Czech regional health care network For our purposes we have concentrated on district hospitals which form the spinal network of primary health care in the Czech Republic. Our research sample-population consisted of 63 hospitals. We have run research on the network of previously district hospitals, tat were subsequently transferred to regions as of December 1, 2011. The research concerned their activity, ownership structure and financial results. There were 63 district hospitals under consideration, out of which 49 hospitals were transferred to regions, either in the form of joint stock company – plc or contributory organizations (příspěvkové organizace). Three hospitals were run by municipalities, one hospital was managed by the town and 11 hospitals were run by other legal persons (jiná právnická osoba – JPO). Table 2: List of districts and corresponding hospitals Transfer Region/district from Region Central Bohemia Mladá Boleslav OÚNZ Mělník OÚNZ Kladno OÚNZ Rakovník OÚNZ Beroun OÚNZ Příbram NsP Benešov OÚNZ Kutná Hora Kolín OÚNZ Nymburk OÚNZ Plzeňský Region Plzeň KÚNZ Tachov N/A Domažlice N/A Klatovy N/A Rokycany N/A Karlovarský Region Karlovy Vary N/A Sokolov N/A Cheb OÚNZ Ústecký Region Děčín N/A Ústí nad Labem N/A Teplice N/A New Institution Form Founder Scope of care Result in 2010 Klaudiánova hospital Hospital Mělník Area hospital Kladno Masaryk hospital Hospital Beroun and Hospital Hořovice Area hospital Příbram Hospital Rudolfa and Stefanie Part of hospital Kolín Area hospital Kolín Hospital Nymburk plc plc plc s.r.o. Region JPO Region JPO 4 Int.,g.,surg. 4 4 undisclosed undisclosed undisclosed undisclosed plc plc plc plc plc s.r.o. JPO Region Region Region Region JPO 4 4 4 Int.,g.,surg. 4 Int.,g.,surg. undisclosed undisclosed undisclosed undisclosed undisclosed undisclosed Stodská hospital NNP Sv. Anna Domažlická hospital Klatovská hospital Rokycanská hospital plc s.r.o. plc plc plc Region JPO Region Region Region 4 0 4 4 4 profit undisclosed undisclosed undisclosed loss Karlovarská regional hospital Karlovarská regional hospital Karlovarská regional hospital plc plc plc Region Region Region 4 4 4 loss loss loss Regional healthcare, a.s. plc Region 4 profit 8 Most OÚNZ Chomutov OÚNZ Litoměřice OÚNZ Town hospital v Litoměřicích Louny OÚNZ Hospital Louny South Bohemian Region Písek OÚNZ Hospital Písek Strakonice OÚNZ Hospital Strakonice Prachatice OÚNZ Hospital Prachatice Český Krumlov N/A Hospital Český Krumlov České Budějovice OÚNZ Hospital České Budějovice Jindřichův Hradec OÚNZ Hospital Jindřichův Hradec Tábor OÚNZ Hospital Tábor Liberecký Region Liberec KÚNZ Regional hospital Liberec Česká Lípa OÚNZ Hospital with polyclinic Turnov OÚNZ Panochova hospital Jablonec nad Nisou N/A Hospital Jablonec Královehradecký Region Jičín OÚNZ Area hospital Jičín Trutnov OÚNZ Area hospital Trutnov Rychnov nad K. OÚNZ Area hospital Rychnov n/K. Náchod OÚNZ Hospital Náchod Pardubický Region OÚNZ, Pardubice KÚNZ Pardubická regional hospital formerly Chrudim LDN Chrudimská hospital Svitavy OÚNZ Svitavská hospital Ústí nad Orlicí OÚNZ Orlickoústecká hospital Region Vysočina Jihlava OÚNZ Hospital Jihlava Pelhřimov OÚNZ Hospital Pelhřimov Havlíčkův Brod OÚNZ Hospital Havlíčkův Brod Žďár nad Hospital Nové Město na Sázavou OÚNZ Moravě Třebíč OÚNZ Hospital Třebíč South Moravian Region Znojmo OÚNZ Hospital Znojmo Břeclav N/A Hospital Břeclav Hodonín N/A Hospital TGM Hodonín Vyškov N/A Hospital Vyškov Blansko OÚNZ Hospital Blansko Zlínský Region Zlín KÚNZ Regional hospital T. Bati Vsetín N/A Vsetínská hospital Kroměříž OÚNZ Kroměřížská hospital Uh. Hradiště OÚNZ Uherskohradištská hospital Moravian and Silesian Region Ostrava OÚNZ Municipal hospital Ostrava Hospital and polyclinic Karviná OÚNZ Karviná-Ráj p.o. plc Municipality 4 JOP LNP profit undisclosed plc plc plc plc Region Region Region Region 4 4 4 4 profit profit profit loss plc Region 4 plc plc Region Region 4 4 profit Loss in 2009. 2010 missing profit plc plc s.r.o. Region Region JPO 4 4 int.,g.,surg. profit profit loss p.o. Municipality 4 profit plc plc plc plc Region Region Region Region 4 4 4 4 undisclosed undisclosed undisclosed undisclosed plc Region 4 loss plc plc plc Region Region Region 4 4 4 loss loss loss p.o. p.o. p.o. Region Region Region 4 4 4 profit loss profit p.o. p.o. Region Region 4 4 profit loss p.o. p.o. p.o. p.o. p.o. Region Region Region Region Town 4 4 4 4 Int. undisclosed undisclosed profit undisclosed profit plc plc plc plc Region Region Region Region 4 4 4 4 undisclosed loss loss profit p.o. Municipality 4 undisclosed p.o. Region undisclosed 4 9 Opava OÚNZ Nový Jičín N/A Bruntál OÚNZ Frýdek Místek OÚNZ Olomoucký Region Prostějov OÚNZ Přerov OÚNZ Šumperk N/A Jeseník new district N/A Sources of data: ÚZIS. Legend: OÚNZ NsP s.r.o. plc Slezská hospital p.o. Lease from the region Region 4 undisclosed plc p.o. Lease from the region AGEL, plc 4 int.,g., Agel, JPO surg.. Region 4 Středomoravská nemocniční Středomoravská nemocniční Šumperská hospital plc plc plc Agel, JPO Agel, JPO Agel, JPO 4 4 4 undisclosed undisclosed undisclosed Jasenická hospital s.r.o. JPO 4 loss Hospital s pol. Nový Jičín Podhorská hospital Rýmařov,Bruntál Hospital ve Frýdku-Místku undisclosed undisclosed profit Own research based on web pages of individual hospitals, districts and regions, and data from District institute of national health, KÚNZ Regional institute of national health, Hospital with Polyclinics LDN Hospital for long-term aftercare Small public limited company p.o. Contributory organization Big public limited company – joint stock company 5. Discussion of the health care quality and availability 5.1 Issues of Availability In all hospitals under study maintained the core departments, which represent: internal medicine, surgery, gynaecology, and paediatric departments, Only 5 hospitals did not maintain the system and have only 3 fields of specialization. From one hospital became a hospital for aftercare. Previously, the district hospitals were in each district. At present, the former districts of Prague-East, Pilsen-North, Plzeň-city, Tachov, Louny, Litoměřice, Hradec Kralové, Brno and Brno-Country are without regional hospitals. The network structure is based on the benchmarks for Health care facilities of the World Health Organisation (WHO). The organisation recommends that there should be a hospital with all basic specializations per each hundred thousand inhabitants. In the Czech Republic this unit was a district. Hospitals of higher type should concentrate on more complex cases mainly because of patient’s safety, and also because the physician needs to have appropriate conditions to be able to provide high quality of complicated treatment. Czech Government at its meeting on 29 August, 2012 approved the Regulation on driving distances to a GP, dentist and gynaecologist. Patients should be able to reach their physicians within a maximum of 35 minutes. Driving time to outpatient care also applies to childcare practitioner, dentist, gynaecologist and pharmacy. The time limit of 45 minutes will be available to more specialized care such as surgery, neurology, internal care and orthopaedics. Even this can lead to further reduction of an access to health care because it can be enforced by health insurance companies to reduce not only the outpatient departments, but also hospitals 10 5.2 Issues of quality Quality and safety of hospitals is becoming a hot topic even in facilities managed regionally. For this reason the coordination groups have been created to promote the accreditation process awarded by the Joint Accreditation Commission as a measure to reduce costs and at the same time to improve quality. The accreditation process is a guarantee that a systematic analysis will be performed in all hospitals. To minimize the risks, that could lead to of any patients’ damage. Accreditation increases the work safety even for the medical staff and helps the hospital in concern in orientation in complex system of legislation. Another positive element of accreditation is that hospitals will be ready to comply with requirements of health insurance companies which will favour the accredited bodies’ to unaccredited in payments for rendered services. The accreditation process is a useful tool for comparison of services provided by individual hospitals During the accreditation process common quality indicators are established and due to this procedure it will be possible to compare the individual hospitals and individual results. Hospitals that have been transferred to regions individual hospitals are preparing to accreditation process or they are already completed.4 The general health insurance company is also interested in the process, because they negotiate the contracts with providers, which highlight the need for gradual optimisation of the health care network and the need for optimising the bed fund. This is done preliminary because of the need to create financial reserves. According to the strategy5 the assessment of impatient healthcare facility in its restructuring depends on several criteria, e.g. filling material, technical and staffing, bed occupancy of at least 75%, the minimum number of five key performance procedures. And last but not least the quality and efficacy of health care provided. The main goal of the General insurance company in addition to establish and guarantee the financial sustainability and improve the quality of health care is to align the requirements of patients, healthcare insurance providers and health insurance companies. The General health care insurance company sees this evidence that accredited hospitals are providing a high standard medical care. 6. Conclusion The move from controlled socialist structure to an insurance-based, fee-for-service model has been institutionalized in a short time. Health care spending increased 50% in 2 years at the beginning of 1990s. This development now resembles many industrialized nations. Claims for reimbursements are increasing at a rate of 5% to 7% per quarter. Market incentives have changed the behaviour within the medical community. Newly privatized physicians generate greater volume and consume more resources than those continuing as state employees. Policy issues requiring further evaluation include supply, distribution, and relative valuation of physician services; clinical resource allocation; and cost containment (Massaro et al., 1994). In accordance with previous findings (Vyborna, 1994 and Uldrichova, 1996) the new system suffers from the common problem of all health care systems – the difficulty of controlling SAK ČR [online]. SAK-standardy-nemocnice-2009.pdf. Dostupný z http://www.sakcr.cz/czmain/dokumenty/akreditace [cit 2012-08-31]. 5 SAK ČR [online]. Akreditace zařízení zlepšuje pozici při jednání s VZP. Dostupný z http://www.sakcr.cz/czmain/archiv-aktualit/akreditace-zarizeni-zlepsuje-pozici-pri-jednani-s-vzp-.488/ [cit 2012-08-31]. 4 11 increases in costs. The reform of the health care system initially contributed to cost increases by imposing additional administrative charges associated with the creation of a system of health insurance companies and by introducing a pure fee-for-service reimbursement system in combination with an amateur fee for-service Price List. Decentralization of state facilities has gone extremely quickly. In the future, the Czech health care system will most likely follow the path on which it has embarked during 1990s. According to Anderson (2009) the most significant reform was a 1997 temporary bill passed by an interim government. Efforts to contain healthcare costs through legislative reform proved difficult to achieve. Until 2007, no other significant healthcare reformed aimed at financing was passed. Cosoveanu, at al. (2009), have established that in the Czech Republic and Slovakia a compulsory public health insurance system replaced the tax-financed system in 1993. Altogether, public financing covers 90 percent of health expenditures in the Czech Republic and 80 percent in Slovakia; the share of private spending is relatively low, but growing. In the previous study Jindrichovska et al. (2011) claimed that providing health care is not only a budgeting question, but it is related to many ethical issues. Up to now, the Czech state and municipal hospitals were not really forced to be cost effective and to be responsible for their results. Thus, on a more general level, patients in the Czech Republic need to be aware of the costs of medical care they receive. As we have learned in the case of Germany, patients receive a bill summarizing the cost of their treatment. Therefore they have an opportunity to become cost conscious. Our current study contributes to the stream of previous literature of transformation of health care system and health care reforms with providing detailed study of changes in the spinal network of district hospitals distributed across the Czech Republic. We have found that there are changes in ownership of hospitals in their structure and expertise. The WHO recommendations are much looser than the arrangement under the previous Czech system. To perform a thorough analysis of influence of on –going health care reforms more quantitative data need to be employed and features of population ageing need to be taken in consideration. On the other hand the influence of new technologies together with witty cost conscious management should bring the overall health-care costs to optimal level. References Anderson, L. S., 2009, “Health Policymaking in the Contemporary Czech Republic”, APSA 2009 Toronto Meeting Paper, Available at SSRN: http://ssrn.com/abstract=1449446 Cosoveanu, G., Dlouhy, M., Hinkov, H. and Cizmarik, P., 2009, “Mental Health Financing and Purchasing in Four Eastern European Countries”, Available at SSRN: http://ssrn.com/abstract=1810080 or http://dx.doi.org/10.2139/ssrn.1810080 Jevcak, A., 2006, “Healthcare reform – unpopular even in Slovakia”, Economic analysis from the European Commission’s Directorate-General for Economic and Financial Affairs, Volume 3, Issue 2, available at SSRN: http://ec.europa.eu/economy_finance/publications/publication11312_en.pdf cited on 11.9.2012 12 Jindrichovska, I., Peskova, R., Funkova, I., Nesladkova, E., 2011, “Efficiency Management of the Czech Health Care“, ACC JOURNAL 3/2011, vol. XVII, Issue C, Social sciences and economy, pp. 64–75. Matl, O., Pavlokova, K., Roubal, T., Vachek, S., 2009, “České zdravotnictví v roce 2050: modely finanční udržitelnosti zdravotnictví v ČR”, (Praha: Kulatý stůl k budoucnosti financování zdravotnictví v ČR). Massaro, T. A., Nemec, J., Kalman, I., 1994, “Health system reform in the Czech Republic. Policy lessons from the initial experience of the general health insurance company”, (The Journal of the American Medical Association, Jun 15, 271(23), pp. 1870–4). OECD Health care policies, Available at SSRN: http://www.oecd.org/els/healthpoliciesanddata/oecdhealthdata2012frequentlyrequesteddata.htm, [cited on 22-08-2012]. SAK ČR [online], “SAK-standardy-nemocnice-2009.pdf”, Available http://www.sakcr.cz/cz-main/dokumenty/akreditace, [cited 2012-08-31]. at SSRN: SAK ČR [online], “Akreditace zařízení zlepšuje pozici při jednání s VZP”, Available at SSRN: http://www.sakcr.cz/cz-main/archiv-aktualit/akreditace-zarizeni-zlepsuje-pozici-prijednani-s-vzp-.488/ [cit 2012-08-31]. Sowa, A., 2010, “The System of Long-Term Care in the Czech Republic”, (CASE Network Studies & Analyses, No. 415/2010), Available at SSRN: http://ssrn.com/abstract=1710618 or http://dx.doi.org/10.2139/ssrn.1710618 Uldrichova, V., 1996, “Current Problems in the Financing of the Czech Public Health System”, (CASE Network Studies and Analyses No. 83), Available at SSRN: http://ssrn.com/abstract=1475187 or http://dx.doi.org/10.2139/ssrn.1475187 UZIS, “Vyvoj-zdravotnictvi-ceske-republiky-po-roce-1989”, Available at SSRN: http://www.uzis.cz/katalog/mimoradne-publikace/vyvoj-zdravotnictvi-ceske-republiky-poroce-1989 [cited on 31-01-2012]. Vyborna, O., 1994, “The Reform of the Czech Health Care System”, (CERGE-EI Working Paper Series No. 64), Available at SSRN: http://ssrn.com/abstract=1557425 or http://dx.doi.org/10.2139/ssrn.1557425 13