Lecture Name:--
advertisement

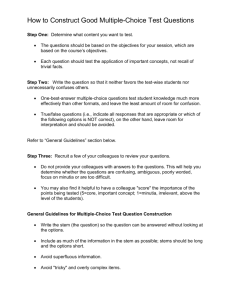
11th-Lec. م حنان ديكان عباس.م The Adrena Gland There are two parts to the adrenals, but there is not much interrelationship between the two: 1. 2. Medulla: The medulla is neurologic tissue; the excess production of the medulla of the adrenal glands causes pheochromocytoma. There is no disease of medullary insufficiency it is perfectly well without the medulla. Cortex: The cortex both has diseases of hyperfunction and hypofunction. Now we have three types of corticosteroids produced by the adrenal cortices: 1. 2. 3. Glucocorticoid, because it has prominently a glucose effect and a moderate amount of salt rentention and other anabolic and catabolic effects. Then we have hyperaldosteronism, which is a mineralocorticoid, it effects mostly although on sodium retention and potassium loss. Then we have the sex steroids, which is characterized in excess by congenital adrenal hyperplasia. Then we have hypofunction of the cortex and that would be the Addison's disease if glucocorticoids are deficient or hyperaldosteronism if glucocorticoid being aldosterone is deficient. The adrenal cortex is controlled largely by the hypothalamus releasing corticotrophic-releasing hormone, stimulating the pituitary to produce ACTH and then stimulating the adrenal cortices. Impacting about the hypothalamus are things like serotonin acetylcholine, norepinephrine and GABA. But the important thing to remember is the hypothalamic pituitary adrenal axis. The cortisone then depresses the pituitary, the hypothalamus and the brain. Now if we have excess of the glucocorticoids it is called Cushing' syndrome. We can also have Cushing's syndrome because of the iatrogenic reasons, the 1 doctors giving the patient corticosteroids. Or we can have bilateral adrenal hyperplasia because of a small pituitary tumor. That is called Cushing's disease. So in some patients there is a small pituitary tumor. In some patient there is pituitary hyperplasia and some patients have a very large and aggressive pituitary tumor called Nelson syndrome. All this is Cushing's disease. So we can have adenoma, which is a benign tumor of the adrenal, there can be carcinoma of the adrenal cortex. ACTH can be produced by cancer, which case is paraneoplastic or CRH can be produced by a cancer. There are many substances with a hydrocortisone effect. This is hydrocortisone or cortisol and this is the active compound. Cortisone is inactive, but as soon it gets in to the body of this oxygen becomes a hydroxyl group and that is activated. On the other hand the synthetic steroids are rather useful because they are much more potent and they have less of an electrolyte effect. They retain sodium less to get less hypertension and less swelling than a patient who was given cortisol or cortisone. This means of course any body with Cushing's syndrome or Cushing's disease will get hypertension. Treatment: Trying the removal of the pituitary microadenoma, if we have adrenal hyperplasia with Cushing's disease. We go for the tumor, we do not find the tumor, and we remove the pituitary gland. Either we can operate, or we can give drugs and all we can use the irradiation of the pituitary. Suppose we operate and we do not find the pituitary adenoma. We go in through the nose, when we are operating a microscope with a fluoroscopic visualization. We can go lateral to the nasal septum or we can temporarily remove the nasal septum and then we cut away though the sphenoid bone and we can see that the tumor very often lies there with normal pituitary around it and we can scoop it out. All of it occupying the whole sella, we can remove the entire lesion pituitary gland and all. So that is for Cushing's syndrome. Now there are other forms of adrenal excess or deficiency. There are two wings to steroid production. We have the wing in which progesterone leads to form a salt retaining steroid, which is aldosterone and then it leads to form 2 cortisone. Then we can have diseases of aldosterone, excess or deficiency. Now hyperaldosteronism is an uncommon lesion in which there is usually a small tumor of the adrenal cortex of the zona glomerulosa region, which produces aldosterone. We have the excess reabsorption of sodium by the kidneys and potassium loss and the mild hypertension because of the sodium retention. Secondary hyperaldosteronism is kind of protective aldosterone production, which can occur, in liver disease or congestive heart failure and it is not associated with hypertension. Now we can have excess sex steroids. We have the glucocorticoids, the mineralocorticoids, and sex steroids. The sex steroid excess is the so-called adrenogenital syndrome, because it is an adrenal disease and it effects the genitalia. We have several variety of it, salt loosing variety, a high blood pressure variety and adrenal insufficiency variety. What happened if we have a blockage in the synthesis of cortisone and the precursors buildup. These progesterone like precursors are transformed by the adrenal gland into sex steroids, which are normally always present, but since the pituitary senses there is not enough cortisone, the pituitary reduces a lot of ACTH. It keeps stimulating the adrenal glands and adrenal glands cannot produce cortisone, so they produce precursors. So the precursor level increases and we have an excess of sex steroid. If we are a female fetus, that female fetus will masculinize, because these are largely androgenic steroids. Thus there will be a so-called female pseudohermaphrodite, which means that they have ovaries, but they look masculinized, because of the excess of sex steroid or we can have in the male a macrogenitosomia precox. Precox means early macro means thing, somia means body, genito, we know what it means, and so it means a male with growth rapidly, has very large genitalia. The symphyses fuse quickly because of all those sex steroid have male hormone in excess and there is no further growth after the fusion of the epiphyses. Hypoadrenalism: Also known as adrenal insufficiency, there is no disease of adrenal sex hormone deficiency, there is a disease of glucocorticoid deficiency. Primarily involving the adrenals we called that Addison's disease. It is the 3 pituitary deficiency causing it, because ACTH is diminished. We call that a secondary hypoadrenalism. And lastly there is hyperaldosteronism. This is the situation in which we get hyperkalemia and hyponatremia, because we do not have the natural salt retaining and potassium losing effect of aldosterone. Aldosterone is produced via the juxtaglomerular apparatus, which releases renin, which then acts on angiotensin in the blood. It induces the formation of Angiotensin I, which we convert it to Angiotensin II and then stimulates the adrenals to produce aldosterone. There are a lot of people are who are hyporeninemic, with hypoaldosteronism in which although, there are stimuli to renin, they are not working. If the renin is low the net result is the decreased formation of aldosterone. There are a lot of weird diseases, which we do not have to worry about, by which our angiotensin for example is produced normally, but can not cause the synthesis of a corticosteroid, corticosterone. Just to point out, but there is several causes of hypoaldosteronism, none of which we have worry about, because it is a rather rare disease. )Synthesis pathways of steroid hormones ( 4 sec retion of adrenocortical hormones by the different zones of the adrenal cortex and secretion of catecholamines by theadrenal medulla Mechanism for regulation of glucocorticoid secretion 5 6