8949,"heroin essay",2,,,40,http://www.123helpme.com/search.asp?text=heroin,5,470000,"2015-12-21 07:34:17"
advertisement

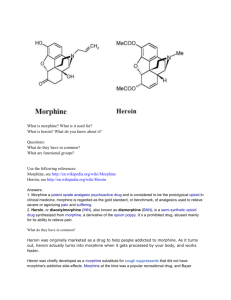
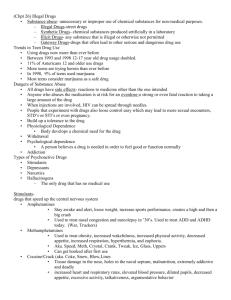
A5, Page 1 Essay Code: A5 CHEM 151 9 February 2014 Morphine: Its history, chemistry, and uses Morphine was the first alkaloid to ever be isolated from any plant. It is the main psychoactive chemical in opium. The recreational use of morphine and its semi-synthetic derivative, heroin, have taken a great toll on society since their discovery. However, it has important medical use as an analgesic to relieve intense pain especially for terminally ill patients and during child birth. Common synthetic derivatives of morphine include dextromethorphan (over the counter cough suppressant), codeine (cough suppressant and antidiarrheal), hydromorphone (narcotic analgesic), and diacetylmorphine (recreational drug). This paper will exemplify the value of morphine and its derivatives by discussing its chemical properties, clinical uses, and abuse potential. Opium, also known as poppy tears, is the milky exudate of the opium poppy papaver somniferum. Opium contains approximately 20 alkaloids including codeine, thebaine, and morphine among other non-analgesic alkaloids. (Might want to introduce morphine first and how it is present in opium instead of introducing opium first since this paper should mainly be focused on morphine.) Morphine, the active constituent in the opium poppy, was first isolated from opium in 1804 by German pharmacist Friedrich Wilhelm Sertürner. He named the yellowish-white crystalline powder morphium, after Morpheus, the Greek god of dreams because the substance had a tendency to cause sleep. He reported that the substance had effects of euphoria and pain relief at low doses and nausea, vomiting, cough suppression, slowed breathing, constipation, and psychiatric effects at high doses (“Morphine”, Encyclopedia Britannica). In 1925, J.M Gulland and R. Robinson proposed the structure for morphine, which was confirmed by its total synthesis in 1952 by M. Gates and G. Tschudi. (Might be worded better if said: In 1925, J.M Gulland and R. Robinson proposed the structure for morphine, which was confirmed by M. Gates and G. Tschudi in 1952 when they completely synthesized it.) The synthesis had 31 steps with a 0.06% yield. One of the most efficient syntheses was proposed in 1980 by K. Rice; it had a 30% yield in 14 steps. Morphine’s chemical formula is C₁ ₇ H₁ ₉ NO₃ with a molecular weight of 285.34 g/mol. Morphine has a melting point of 255℃, a boiling point of 190℃, and solubility of 0.15g/L at 20℃ (“Morphine”, Pub Chem). The structure is shown below: (Might want to put this paragraph towards the end of the essay since it is the least interesting.) A5, Page 2 Based on its structural backbone, morphine is classified as a benzylisoquinoline alkaloid (with two additional rings). The rigid pentacyclic structure consists of a benzene ring and two partially unsaturated cyclohexane rings, which are part of a phenanthrene ring system that has little conformational flexibility. In addition, it had a piperidine ring and a tetrahydrofuran ring. The functionality of morphine consists of two hydroxyl functional groups (phenolic and allylic), an ether linkage, a basic tertiary amine, and five centers of chirality. More than 250 morphine derivatives have been developed. Its derivatives include opioid agonists, antagonists, agonistantagonists, partial agonists, and inverse agonists, which range from 2% to 2,000% the strength of morphine. Morphine is the precursor for semi-synthetic opioids such as hydromorphone, oxymorphone, and diacetylmorphine (Weill, “The Structure of Morphine”). (Might want to put this paragraph more towards the end of the essay as well.) Opioids are exogenous substances that bind to endogenous opioid receptors throughout the brain. Endogenous opioids are neurotransmitters called endorphins, enkephalins, and dynorphins that bind to mu, delta, and kappa receptors in the brain, moderating reactions to painful stimuli. Opioids also disinhibit dopamine neurons by reducing the amount of GABA (inhibitory neurotransmitter) released. As a result, opioids increase the amount of dopamine produced, causing a feeling of euphoria. The effects of opioids include: pain relief, cough suppression, anxiety relief, shallow breathing, slowing of the digestive tract, histamine release. Some side effects include drowsiness, nausea or vomiting, sweating, dysphoria, constipation, and respiratory depression. Opioids can be clinically used for diarrhea, pain management, and cough control. Due to their effects, opioids are highly addictive and have a high overdose potential. However, they have the least toxic effects at the cellular level compared to other drugs (Dubuc, “How Drugs Affect Neurotransmitters”) (Start off paragraph by explaining how opioids are related to morphine; remember that morphine is the main subject here.) Diacetylmorphine is one of the most notorious semi-synthetic derivatives of morphine. It is created by treating morphine with acetic anhydride via an acetylation reaction (Bedford, et al). A5, Page 3 The drug was first synthesized from morphine in 1874 by C. R. Alder Wright. It was introduced as a commercial product by the Bayer Company in 1898. The company marketed the drug under the trademark name of Heroin due to its perceived “heroic” effects. At this (the) time, morphine had become a popular recreational drug and Heroin was marketed as a non-addictive morphine substitute and cough suppressant. In addition, it was marketed as a cure for morphine addiction before it was discovered that it metabolizes (metabolized) into morphine once it is (was) absorbed by the body. However, contrary to advertising (advertisement), heroin soon had the highest dependence rates among its users (“Heroin”, Ecyclopedia Britannica). (Interesting paragraph that kept my attention while being informative at the same time.” Morphine is able to cross the blood brain barrier but it does not cross easily due to its poor lipid solubility. Heroin, on the other hand, is much less soluble in water than morphine but more lipid soluble. As a result, it crosses the blood brain barrier more easily, making it more potent than morphine. Heroin can be injected (intravenous or intramuscular), smoked, snorted, or ingested. The most common routes of administration are subcutaneously (skin popping) and intravenously (mainlining). Although all routes of administration are addictive, the pleasurable effects of the drug are proportional to the rate at which the drug concentration increases in the blood. Intravenous injections cause blood concentrations to rise most quickly, providing the most rapid onset of euphoria after 7-8 seconds, followed by an intramuscular injections (5 to 8 minutes) and smoking or snorting (10-15 minutes). Therefore, IV heroin injections produce an intense rush that is fast and dramatic but with shorter lasting effects than morphine (“Heroin: Abuse and Addiction”). Due to its effects, heroin produces a profound degree of tolerance and (as well as) physical and psychological dependence, which are motivating factors for compulsive use of the drug. Heroin is the second most addictive drug after nicotine. (Awkward place for this sentence, A5, Page 4 maybe think about moving it elsewhere or explaining more.) Withdrawal from opioids is more dramatic than withdrawals from other illicit drugs. Symptoms include but are not limited to anxiety, insomnia, cold sweats, severe muscle and bone ache, fever, involuntary limb spasms, nausea, vomiting, and hypersensitivity to pain and stress. Heroin withdrawal is not fatal to healthy adults, however, the user feels as if it is. Treatments for heroin withdrawal include methadone as a replacement drug (methadone maintenance) and buprenorphine (opioid partial agonist). Both of these drugs prevent withdrawal without causing positive reinforcing effects (“Drug Use”). Although morphine and its derivatives are highly addictive. They do serve important clinical purposes. Morphine is medically used in its hydrochloride, sulfate, acetate, and tartrate salts. [Wording is confusing.] One of its most common uses in the medical field is to treat severe pain. It is effectively treats acute or chronic severe pain, postoperative pain, and labor pain. [Sentence flows better without the “is” between “it” and “effectively”.] Outpatient analgesia is usually administered orally or transdermally (via a patch). Inpatient analgesia is administered intravenously via a titration or through patient-controlled analgesia. The doses of the selfadministered morphine are smaller than those administered orally, however, they both provide effective recovery. [Sentence flows better without “the” in “the doses of the selfadministered…”.] Oral administration of morphine provides analgesia that lasts about 3-6 hours while intravenous, intramuscular, and subcutaneous administrations last 3-4 hours (“Morphine”, Encyclopedia Britannica). Morphine is commonly used to treat pain in terminally ill patients. The National Cancer Institute states that symptoms commonly experienced at the end of life for cancer patients include pain, delirium, fatigue, cough, dyspnea (shortness of breath), and rattle (the accumulation of saliva and other fluids in the upper airways of the patient who is to weak to clear their throat). Morphine can be administered to control pain especially during the patient’s final hours. Several studies refute associations between hastened death and opioid use. However, cancer patients are not free of the substance’s addictive properties. Patients that develop an addiction are given adequate amounts without reluctancy to avoid withdrawal. The use of intermittent injections or infusions are increased as a patient approaches death. High doses may produce myoclonus (involuntary muscle twitching), acute confusion, restlessness, hallucinations, and hyperalgesia. These symptoms may be treated with the administration of an opioid antagonist (“Last Days of Life”). [Good paragraph that is interesting, maybe think about moving this paragraph higher in the essay.] The many uses of morphine and its derivatives make[s] morphine a controversial drug. On one hand it is an effective pain reliever, cough suppressant, and antidiarrheal. [Sentence is not completely, usually is “On one hand……on the other hand…”.] It is especially beneficial for postoperative analgesia. Its use on terminally ill patients provides them with relief of [from] fear of uncontrollable pain that many patients face as they approach death. However, morphine’s side effects are often a concern for family members and health care providers. The use of the semisynthetic morphine derivative, heroin, is very detrimental to the user and to society. According to the National Institute on Drug abuse, an estimated 4.2 million Americans aged [ages] 12 or older had [have] used heroin at least once in their lives. (“Heroin: Abuse and Addiction”). Heroin is one of the most addictive drugs due to its intense withdrawal symptoms and euphoric effects; This makes it almost impossible for users to quit and for society to eradicate its use. Heroin is linked to increases in crime, domestic violence, child abuse, and infectious diseases like HIV and hepatitis. Since its discovery, morphine has changed the life of its users, whether it is through A5, Page 5 beneficial medical uses or through addiction. [Paragraph changes from talking about heroin to ending with morphine, needs to flow better.] Works Cited Bedford, K. R., S. L. Nolan, R. Onrust, and J. D. Siegers. "The Illicit Preparation of Morphine and Heroin from Pharmaceutical Products Containing Codeine: 'Homebake' Laboratories in New Zealand." N.p., 1987. Web. 02 Feb. 2014. <https://www.erowid.org/archive/rhodium/chemistry/ codeine.homebake.labs.html>. "Drug use." Encyclopaedia Britannica. Encyclopaedia Britannica Online. Encyclopædia Britannica Inc., 2014. Web. 10 Feb. 2014. <http://www.britannica.com/ EBchecked/topic/172024/drug-use>. Dubuc, Bruno. "How Drugs Affect Neurotransmitters." The Brain From Top to Bottom. Institute of Neuroscience, Mental Health, and Addiction, Jan. 2002. Web. 01 Feb. 2014. "Heroin." Encyclopaedia Britannica. Encyclopaedia Britannica Online. Encyclopædia Britannica Inc., 2014. Web. 10 Feb. 2014. <http://www.britannica.com/ EBchecked/topic//>. "Heroin: Abuse and Addiction." National Institute on Drug Abuse. Research Report Series, May 2005. Web. 02 Feb. 2014. Mandal, Ananya. "Morphine History." News Medical. N.p., n.d. Web. 01 Feb. 2014. < http://www.news-medical.net/health/Morphine-History.aspx>. "Morphine." Encyclopaedia Britannica. Encyclopaedia Britannica Online.Encyclopædia Britannica Inc., 2014. Web. 10 Feb. 2014. <http://www.britannica.com/ EBchecked/topic//>. "Morphine." Pub Chem Compound. National Center for Biotechnology Information, n.d. Web. 01 Feb. 2014. <http://pubchem.ncbi.nlm.nih.gov/summary/ summary.cgi?cid=5288826>. "Last Days of Life." National Cancer Institute. National Institutes of Health, 10 Dec. 2013. Web. 02 Feb. 2014.<http://www.cancer.gov/cancertopics/pdq/ supportivecare/lasthours/healthprofessional/page2/AllPages>. Weill, Paul B. "The Structure of Morphine." United Nations Office on Drug and Crime. N.p., 01 Jan. 1950. Web. 01 Feb. 2014. <https://www.unodc.org/unodc/en/dataand-analysis/bulletin/bulletin_1950-01-01_2_page004.html>. A5, Page 6 Comments -introductory paragraph was very interesting, drew in my attention -work more on the thesis, be more specific about what you’re going to be talking about in the essay -the essay seemed to be more focused on heroin and opium than on morphine -there was a lot of interesting information in the essay -missing a conclusion paragraph