clinical governance strategy
advertisement

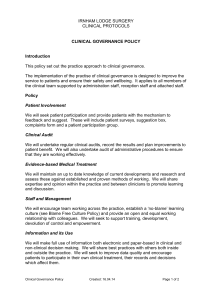
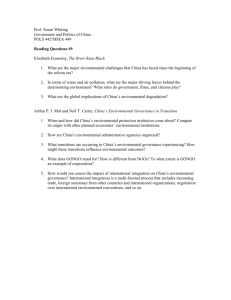
DRAFT ROYAL BERKSHIRE AMBULANCE NHS TRUST A CLINICAL GOVERNANCE STRATEGY 2002 - 2007 TABLE OF CONTENTS INTRODUCTION ……………………………………………………………………………………3 BACKGROUND ……………………………………………………………………………………..4 CLINICAL GOVERNANCE AND RISK MANAGEMENT STATEMENT ……………….………5 CG MANAGEMENT ORGANISATION AND RESPONSIBILITIES …….………….6 4.1 Executive Responsibility………..…………….. ……………………………………………….6 4.2 Board Committee Structure ……………………………………………………………………....9 4.2.1 Clinical Governance responsibilities under the Service Directors……..……….9 4.3............................................................................... Clinical Governance and Risk Committee 9 4.4.......................................................................................... Trust Clinical Effectiveness Group 11 4.5........................................................................................... Local Ambulance Advisory Panel 11 4.6.......................................... Patient Advice and Liaison Service (PALS) - under development 12 4.7........................................................................................................................ Caldicott Group 13 4.8........................................................................................... Health and Safety Working Group 13 4.9....................................................................Vehicle, Equipment and Uniform Working Party 14 4.10.................................................................................................................... Audit Committee 14 4.11..........................................................................................................................................BSI 14 4.12...................................................................................... People and Organisation Committee 15 4.13.............................................................................. Line Managers and Heads of Department 15 4.14.................................................................................................................................. All Staff 16 5. CLINICAL GOVERNANCE ACTIVITIES AND TARGETS ……………………………………..16 6. MONITORING CLINICAL GOVERNANCE ACTIVITIES ………………………………………16 7. ROYAL BERKSHIRE AMBULANCE TRUST REFERENCES …………………………………..16 7.1 Acknowledgements……………………………………………………………………………...17 1. 2 3. 4. APPENDICES Appendix 1 THE SEVEN PILLARS OF CLINICAL GOVERNANCE ..................................................... 18 1 Consultation and Patient Involvement .................................................................... 18 2 Clinical Audit Activity ............................................................................................ 18 3 Clinical and Non-Clinical Risk Management ......................................................... 19 4 Research and Effectiveness ..................................................................................... 22 5 Staffing and Staff Management ............................................................................... 22 6 Education and Training ........................................................................................... 25 7 Use of Information to Support Clinical Governance and Healthcare Delivery ...... 26 Appendix 2 THE TARGETS AGREED FOR 2002-2003 FOR THE NINE PILLARS OF CLINICAL GOVERNANCE SET OUT FOR THE SOUTH EAST REGION OF THE NHS. ............. 28 a) Clinical Governance Strategies ............................................................................... 28 b) Consultation And Patient Involvement ................................................................... 29 c) Clinical Audit Activity ............................................................................................ 30 d) Clinical and Non-Clinical Risk Management ......................................................... 31 e) Research and Effectiveness ..................................................................................... 32 f) Staffing and Staff Management ............................................................................... 33 g) Education and Training ........................................................................................... 34 h) Use of Information to Support Clinical Governance and Healthcare Delivery ...... 34 Appendix 3 GLOSSARY OF TERMS ......................................................................................................... 35 2 ROYAL BERKSHIRE AMBULANCE NHS TRUST A CLINICAL GOVERNANCE MANAGEMENT STRATEGY 1. INTRODUCTION 1.1 This strategy outlines the plan for the continued implementation of Clinical Governance at the Royal Berkshire Ambulance NHS Trust. We have drawn on experiences of other Trusts, both locally and nationally, inside and outside the ambulance services, who have participated in the first wave of reviews undertaken by the Commission for Health Improvement. 1.2 While recognising that this strategy for quality is ambitious, it is built on a foundation of continued achievement both in performance and financial control of which the Trust, and those working within it are rightly proud. This document provides an understanding both of how Clinical Governance is organised within the Trust and what the Trust’s priorities are, during the forthcoming five years and outlines goals for the next two years. 1.3. The key objectives addressed by the Strategy to deliver quality in the organisation are to: integrate Clinical Governance and risk management activity in both the clinical and non-clinical areas; ensure there is an effective and comprehensive system for untoward incident and near misses review and complaints management; ensure a process for appropriate learning which leads to quality improvements; ensure that patients and other service users contribute to the development of the Trust’s clinical and non-clinical services assist with statutory compliance in all areas of the Trust’s activities; provide a mechanism to assure the Trust Board that appropriate and necessary control systems are in place to reduce and control risks; encourage financial benefits from improving quality and minimising risk. 1.4 The Trust Board believes that by approaching the control of risks in a strategic and organised manner, the risks can be reduced to an acceptable level. This will result in better quality care for patients and service users, a safer environment and a reduction in unnecessary expenditure. 1.5 The Trust promotes the right of the individual to be informed and consulted on pertinent issues. It recognises that inadequate communication is a major risk factor, with perceived withholding of information potentially resulting in lowered staff morale and subsequent reduction in the quality of service provision. 1.6 The involvement of all staff in Clinical Governance will be encouraged by promoting an open, ‘blame-free’ culture, in which individuals are empowered to voice their concerns in the knowledge that due attention will be paid to these, as evidenced by 3 feedback on how these issues have been addressed. The Trust recognises that in the majority of adverse incidents there is an organisational failure leading up to the event1. 2 BACKGROUND 2.1 Since the advent of clinical governance as set out in the Government’s white paper The new NHS Modern. Dependable2 and in A First Class Service. Quality in the new NHS Health Services Circular 19983, organisations have been struggling with the concept of clinical governance and how to put it into practice. It is clear that Clinical Governance is the cornerstone of the Government’s strategy for the NHS, which is to ensure that quality care is the driving force for the development of health services. The overall aim is to improve standards of care by reducing and understanding variations, improving outcomes and access to services. The clinical decisions taken will be based on up-todate evidence to ensure its effectiveness. 2.2 The framework that emerges for the implementation of Clinical Governance requires local interpretation. Central to this is the use of a multi-professional, multi-disciplinary and multi-agency approach, in addition to building on current systems for ensuring quality care already in use, eg, clinical audit, risk management, quality assurance, clinical effectiveness and staff and organisational development. Local ownership and a shared interpretation of Clinical Governance are viewed as essential for successful implementation. 2.3 The key to the success of Clinical Governance within each health organisation rests on maximising and developing a culture based not only on collaboration, teamwork and the sharing of expertise, but one in which innovation and learning are nurtured against a backdrop of openness, trust and public discussions. 2.4 In considering the challenges for providing quality-driven healthcare for the 21st century such as that envisaged in A First Class Service. Quality in the new NHS4, central to this thinking is the desire reflected in this strategy of involving patients as active partners in their own health care, thereby underpinning the Trust’s vision of the clinical governance strategy. 1 Organisation with a Memory, Department of Health 2000 The stationary office Ltd. 1997 The new NHS Modern. Dependable. London 3 Department of Health 1998 A First Class Service. Quality in the new NHS Health Services Circular 1998 4 Department of Health 1998 A First Class Service. p113 2 4 3. CLINICAL GOVERNANCE AND RISK MANAGEMENT STATEMENT 3.1 The following Clinical Governance and Risk Management Statement has been distributed to all staff throughout the Trust as part of the Trust's Strategic Plan. CLINICAL GOVERNANCE AND RISK MANAGEMENT STATEMENT The vision of the Royal Berkshire Ambulance NHS Trust is: “To be a model ambulance service” The Trust recognises that the management of Clinical Governance and risk is a key factor in achieving this aim, as is controlling any potential risk to staff and general public. It is also the duty of the Trust to safeguard the assets and reputation of the Trust. The trust will ensure that quality improvement processes are in place, leadership skills are developed at clinical team level, evidence based practice is in day-to-day use and good practice, ideas and innovations are systematically disseminated. Problems of poor clinical performance will be recognised and dealt with at an early stage. All professional development programmes will reflect the principles of clinical governance . Quality data will be collected to monitor clinical care & will be of a high standard A systematic approach will be taken to the on-going identification and assessment of risk, with prompt action initiated to eliminate or control those risks identified. The management of Clinical Governance and risk is the responsibility of all managers and staff throughout the Trust. This will be achieved within a progressive, honest and open environment, where mistakes and untoward incidents are identified quickly and acted upon in a positive and constructive way. Staff will be provided with the necessary education, training and support to enable them to meet this responsibility. 5 4. CLINICAL GOVERNANCE ORGANISATION AND RESPONSIBILITIES 4.1. Executive Responsibility 4.1.1 Whilst ultimate responsibility for quality lies with the Chief Executive and the Trust Board, the overall executive responsibility for Clinical Governance has been delegated to the Medical Director. He is a member of the Clinical Governance and Risk Committee. 4.1.2 While the Directors are assisted in this role by several managers within the Trust, whose departments support the various aspects of Clinical Governance, the Trust believes that clinical governance will only develop if there is full ownership and collaboration from staff at all levels of the organisation and its structure reflects the importance the Trust places on the involvement of staff included in direct patient care. 4.1.3 The Medical Director provides board level leadership. The Clinical Governance and Risk Committee (CGRC) provide the strategic direction that feeds into the Trust Board. This is then cascaded down through the Trust Clinical Effectiveness Group and Operations Committee to Operational staff via their Clinical Supervisors and Work-based Assessors. These groups act as the drivers for change and development. They are multi-professional representing the services they provide. At present the Clinical Effectiveness Group, Operations Committee and the Clinical Governance and Risk Committee take responsibility for clinical governance elements such as: risk, clinical audit, information, staffing, education & continuing professional development, clinical governance strategy and the clinical governance organisation & responsibilities. 4.1.4 A key principle in the Trusts’ policy is that the Clinical Governance and Risk Committee and the Clinical Effectiveness Group reports using an agreed format on specific clinical governance issues. Of the ‘pillars of clinical governance’ the groups are responsible for patient experience & involvement, risk management, clinical audit, research & effectiveness and also consider items of information management, staffing, education and continuous professional development which may impact directly on their projects. Otherwise, these topics are considered in the relevant departments / meetings outlined later in this document. The Clinical Effectiveness Group is responsible for developing an agreed forward plan including patient experience, clinical audit and clinical guidelines focussing on high risk or high volume procedures. The programme is informed by claims and complaints and by national initiatives such as the NSF standards and NICE guidance. 4.1.5 To support the staff and ensure the co-ordination and development of Clinical Governance activity the Trust has in place the Clinical Governance and Risk Committee and Clinical Effectiveness Group who provide expertise, facilitation and training in the following areas; complaints, litigation, clinical risk, clinical audit and research and development. An important role for the Clinical Effectiveness team is that a senior member attends all Clinical Governance and Risk Committee meetings to ensure a common approach and provide feedback both to and from the Clinical Effectiveness Group. 4.1.6 The organisation for clinical governance with respect to risk, audit and effectiveness and complaints is well developed in terms of structure. However, clinical governance, 6 incorporating all elements, is currently in its infancy and supporting structures and processes continue to be refined and developed . 7 4.2 BOARD COMMITTEE S T R U C T U R E EXECUTIVE TEAM MEETING CAPITAL MANAGEMENT AUDIT COMMITTEE CHARITABLE COMMITTEE M E E T I N G S DIRECTORS’ REMUNERATION COMMITTEE APPOINTMENTS COMMITTEE STAFF COUNCIL PEOPLE & ORGANISTION COMMITTEE B O A R D JOINT NEGOTIATING GROUP T R U S T VEHICLE, EQUIPMENT & UNIFORM WORKING PARTY OPERATIONS COMMITTEE LOCAL AMBULANCE ADVISORY PANEL MEETING CLINICAL EFFECTIVENESS GROUP RISK MANAGEMENT & CLINICAL GOVERNANCE COMMITTEE Meeting Structure 1 April 2002 HEALTH & SAFETY WORKING GROUP CALDICOTT GUARDIANS 8 4.2.1 Clinical Governance responsibilities under the Emergency Services, Customer Services and Medical Director Medical Director LAAPs Emergency Services and Customer Services Directors Corporate Services Manager Claims Complaints Critical incidents analysis & reporting CNST Controls Assurance Health & Safety CHI preparation and Project Plan Public Involvement Co-ordination (RCGC) Clinical Effectiveness Manager Co-ordination (Clinical Effectiveness Group) Clinical Audit Research and Development Clinical Guidelines / Document Review Clinical Governance Management Project management Trust Lead for NHS Plan Trust Lead for NSFs (Coronary Heart Disease and the Older Patient) Trust lead for Category "C" projects Trust lead for Electronic Patient Report Forms Representation on: Audit Committee VEHICLE, EQUIPMENT & IM&T UNIFORM WORKING Caldicott PARTY Vehicle, Equipment and Uniform Working Party People and Organisation Committee Staff Council Negotiating Group 9 4.3 Clinical Governance and Risk Committee Role The Clinical Governance and Risk Committee (CGRC) is established under the Trust Board. It has a strategic role in the co-ordination and monitoring of the Trust’s Clinical Governance and Risk Management Strategies ensuring there are processes for risk assessment in place, so that risk is managed pro-actively and that there is no unnecessary duplication of effort or information gathering, but equally making it clear where final responsibility lies for dealing with individual issues. The operational functions will be devolved as appropriate to sub-committees. Terms Of Reference 1. To ensure in light of information available that there are adequate risk assessment processes in place throughout the Trust. The committee will set targets for Clinical Governance and risk management where appropriate. 2. The CGRC will promote a culture of continuous quality improvement. 3. The Committee will receive reports at each meeting from the following subcommittee. The Trust Clinical Effectiveness Group The Local Ambulance Advisory Panel The Health and Safety Working Group Caldicott Guardians Management Review Groups (BSI Quality Systems) Major Incident Planning Officer The Trust Patient Advisory Liaison Panel (when formed) - and review Claims against the Trust presented by Marsh UK Limited The Committee will devolve responsibility for action to one of these groups as is felt appropriate. 4. The Committee will ensure that risk management objectives remain in line with the objectives of the Controls Assurance initiative within the NHS and the Controls Assurance Statements in the Annual Accounts. However, the Committee will also remain aware of its relationship with The Audit Committee whose function is to assure The Board that Financial Controls are sound. 5. The group will report to the Board quarterly 10 4.4 Trust Clinical Effectiveness Group Role The Clinical Effectiveness Group is established as a working group of the Trust’s Clinical Governance and Risk Committee with the responsibility to ensure all operational staff maintain and improve clinical standards. This aim is achieved by providing a multidisciplinary structure to support clinical effectiveness and by promoting an evidencebased practice culture throughout the Trust. Improving clinical effectiveness will have a major impact in improving standards of care, better use of resources and reducing clinical risk in the organisation in accordance with the principles of Clinical Governance being adopted within the Trust. Key points from Terms of Reference 1. Identify priority areas, taking into account both local and national priorities and initiatives 2. Develop knowledge of Evidence-Based Practice (EBP) and Critical Appraisal Skills within the Trust 3. Develop facilities to enable widespread and easy access to knowledge 4. Identify and improve current facilities within the Trust for information and knowledge-acquisition within the Trust relevant to clinical effectiveness (CEf) including record keeping 5. Encourage the development of a systematic approach to CEf e.g. - Identify priority area Identify current practice Critical appraisal of best practice Develop evidence-based guidelines, protocols and procedures Compare current with best practice Change practice if necessary Monitor 6. Review and recommend remedial action for adverse clinical incidents to the CGRC and the management team for implementation 4.5 Local Ambulance Advisory Panel RBAT have observed the Rules and Regulations for Paramedic Training, by establishing the mandatory Local Paramedic Steering Committee. 11 Principal Objective Composed of specialist consultants in fields related to ambulance work, the Local Ambulance Paramedic Steering Committee oversee the training of Paramedics and review the clinical policies and protocols under which they work. Functions: 1. To advise on and approve Drug Protocols for use by RBAT staff 4.6 2. To advise on and approve clinical procedures undertaken by RBAT staff 3. To provide specialist Consultant advice in each member’s clinical area and keep the Ambulance service appraised of developments in clinical practice 4. To consider the application of National Ambulance Guidelines within the local area taking into account the local Health Care structure 5. To approve the arrangements for the Paramedic course and re-assessment process 6. Chairman or Deputy to oversee Paramedic Training course and determine that the training has been carried out in accordance with the Rules, Regulations and Syllabus. To sign the certificate application form of successful candidates Patient Advice and Liaison Service (PALS) - under development Proposed Role Within the structure of Quality and Clinical Effectiveness the group to take responsibility for all aspects of quality relating to patient care including complaints management. The PALS will be established as a subcommittee of the Trust’s Clinical Governance and Risk Committee with the responsibility to report on all significant matters which come to their attention during the execution of their duties. The PALS will operate within the limits of authority delegated to it by the Risk and Clinical Governance Committee. Proposed Terms of Reference for Discussion 1. To establish and monitor the effectiveness of a problem resolution system linking this to systems of incident reporting to ensure that action is taken to address any trends identified 2. To establish a system of co-ordinating and quality-assuring all standard information for patient use 3. To develop systems in which a culture of continuous quality improvement can be developed. In the first instance this structure and function of the proposed group will be developed 4. To lead the development of systems of patient involvement in clinical decision making 12 4.7 Caldicott Group Role Chaired by the Director of Finance and Business Services, this group advises and supports the Trust in all issues concerned with confidentiality Functions 1. Members of the group ensure confidentiality standards are being met 2. Members of the group have powers to monitor how standards are being met, identify reasons why if they are not being met and ensure implementation of changes in practice to meet those standards 3. To regulate and monitor the use of patient identifiable information (on an individual and broader basis, for example information held in large databases) 4. To ensure that training in the ethical and legal issues around confidentiality is provided for both clinicians and non-clinicians in the Trust 5. To advise on security issues, including, for example, how information should be protected from direct access or browsing by anyone who is not treating the patient to whom the information relates 6. To oversee training in the use of IT within the service and the protection of the confidentiality of information held by the Trust. 4.8 Health and Safety Working Group Role The Health and Safety Working Group is established as a subcommittee of the Trust’s Clinical Governance and Risk Committee with the responsibility to report on all significant matters which come to their attention during the execution of their duties as described in the Terms of Reference. This will include ensuring that systems are in place for reporting accidents/non – clinical incidents and monitoring identified trends (including patients and visitors). Terms of Reference To provide a staff consultation and discussion forum on all matters relating to health, safety and the relational issues of Risk Management. Such matters will include: - the study of accident and risk report statistics and trends the examination of safety reports and workplace inspections the consideration of reports from appointed Safety Representatives to consider & monitor the adequacy of safety and health communication and awareness in the workplace the development, introduction and monitoring of work safety rules and safe systems of work. 13 4.9 Vehicle, Equipment and Uniform Working Party Principal Objective: To develop, evaluate and recommend to the Clinical Effectiveness and Operations Committee the most appropriate type of vehicles, equipment and uniform which are cost efficient, effective and fit for the purpose. Appropriate items are also taken to the CGRC. Areas of Activity: To oversee trials of medical equipment To monitor equipment and uniform effectiveness and suitability and recommend the most cost effective solutions. To examine different vehicle and stretcher opportunities and take account of user views when recommending appropriate capital purchases. Monitor performance of existing vehicles, equipment and uniforms and their ongoing developments. 4.10 Audit Committee The Audit Committee, chaired by a non-executive director, will continue to have responsibility for the management of financial risk. It will also co-ordinate activity in accordance with the guidance given in HSC 1998/070 with regard to controls assurance, set out in the NHS Executive Directions EL97/55. The Finance Director has the responsibility for maintaining a sound system of internal control that supports the achievement of the organisation’s objectives and for reviewing its effectiveness. The system of internal control is based on an on-going risk assessment process designed to identify the principal risks to the achievement of the organisation’s objectives; to evaluate the nature and extent of those risks and to manage them effectively and economically. The system of internal control is underpinned by compliance with the requirements of the core Controls Assurance standards: Governance Financial Management Risk Management (Risk Management System standard for 2001/2002-10-15 This Committee reports through the Chair to the Trust Board. 4.11 BSI On the recommendation of the Board the Trust agreed to attain the standards set out by the BSI organisation. The BSI Manager sets the agenda and timetable for the audits. Progress 14 and performance are monitored against the targets set, through individual department Management Review Groups. Regular reviews and reports should be presented to CGRC and Operations Committee by the BSI Manager 4.12 People and Organisation Committee The People and Organisation Committee reports directly to the Board Role To develop and recommend to the Board for approval, Organisational and Human Resources Strategies and Policies to support the Trust’s business objectives and plans. Areas of Activity: 4.13 Organisational development Human Resources Policies and Procedures Remuneration and reward systems Manpower and planning and development Employee relations Communications Training and Personal Development Recruitment and Retention Line Managers and Heads of Department In conjunction with the Trust-wide Clinical Governance initiatives and systems, it is essential that all managers accept that Clinical Governance is a part of their line management responsibility. This will be reflected in the job descriptions and appraisal objectives of all managers. Their responsibilities include: active participation in the implementation of the Clinical Governance Strategy and making any necessary changes and improvements; implementation of specific Trust-wide Clinical Governance policies and procedures; ensuring attendance of staff at Clinical Governance training sessions; raising Clinical Governance Awareness at operational level; encouraging staff to identify and report hazards and risks and responding positively when they do so; ensuring that all adverse incidents are reported through the incident reporting system; seeking advice on Clinical Governance issues as required; facilitation of the Clinical Governance Assessment process and reporting the risks identified to the Clinical Effectiveness Group or the Health and Safety Manager, as appropriate. 15 4.14 All Staff All Trust staff have responsibility to: maintain general risk awareness at all times; participate in Clinical Governance education and training; comply with policies, procedures and protocols; notify line managers of any identified risks or Clinical Governance issues; adhere to the adverse incident reporting procedures. 5. CLINICAL GOVERNANCE ACTIVITIES AND TARGETS 5.1 Clinical Governance is managed according to the nine pillars of clinical governance which have been set out by the NHS and are the basis for monitoring by the South East Regional Office. These activities are: Clinical Governance Strategy, Organisation and responsibilities for Clinical Governance, consultation and public involvement, clinical audit, clinical risk management, research and effectiveness, staffing and staff management, education and training, use of information. 5.2 The targets that have been agreed are set out in appendix 1 and an annual forward plan is attached (appendix 2). 5.3 A glossary of terms has been added for clarity and this appears in appendix 3. 6. MONITORING CLINICAL GOVERNANCE ACTIVITIES 6.1 Clinical Governance activities will be reported to the Board on a monthly basis by the Emergency Services Director, Customer Services Director, Medical Director and the Corporate Services Manager 6.2 The Clinical Governance Action Plan and Outcomes will form a part of the Annual Report. 6.3 The Clinical Governance and Risk Committee will be the forum for discussion and development of Clinical Governance projects. 7. ROYAL BERKSHIRE AMBULANCE TRUST REFERENCES J:\Clinical Effectiveness\Clinical Governance\Strategy\RBAT Clinical Governance Strategy.doc Controlled document: CEf 45 August 2002 Review due: August 2003 16 7.1 Acknowledgements Written by: C Breen Clinical Effectiveness Officer Approved by: S Brown Medical Director 10/09/02 Accepted by: Debbie Dunning Emergency Services Director 7/10/02 Approved by: Ken Sealy Non-Executive and Chairperson At Clinical Governance and Risk Meeting: TBA Ratified by: Ian Ferguson Chief Executive At Board Meeting: TBA 17 APPENDIX 1 THE NINE PILLARS OF CLINICAL GOVERNANCE Overall seven pillars of clinical governance were set out these have now been supplemented by two additional requirements based on Clinical Governance strategy and clear organisational structures with lines of responsibility, these latter two have been dealt with in the main strategy document. Below is a discussion in more detail on the remaining seven pillars. 1 Consultation and Patient Involvement 1.1 The NHS Plan sets out the Government’s ambitions to create a patient-centred NHS. The involvement of users and external agencies in the development, delivery and evaluating of health care services is an important aspect of the Clinical Governance Agenda. The Trust recognises the need to involve and integrate users, carers and the public at all levels of service delivery. With the aim of ensuring that they can act as a powerful lever for change and improvement. 1.2 The Trust recognises that a considerable amount of work needs to be done to achieve the targets of developing and implementing a public involvement policy, establishing a PALS service and ensuring that there is organisational learning from claims and complaints. 1.3 At the centre of patient involvement is the issue of informed consent to procedures, treatment and personal care. The Trust is committed to implementing Good practice in consent5, 6. 2 Clinical Audit Activity 2.1 Clinical Audit is an essential part of improving health services, through the accurate and relevant measurement of practice against agreed standards. It is most effective when applied to priority areas, where improvements in practice can be made if required. Increasingly this agenda is defined nationally with standards set, for example, within the National Service Frameworks (NSF) and ASA/JRCALC guidelines. 2.2 The Trust must strive to provide detailed and accurate information on which clinical decisions can be made and practice compared. 5 HSC 2001/023, Good Practice in consent; Achieving the NHS Plan commitment to patient-centred consent practice, NHS Executive 2001 6 Good Practice in consent implementation guide: consent to examination or treatment. DOH 2001 18 3 Clinical and Non-Clinical Risk Management 3.1 Managing risks in clinical settings is a challenge to all those who deliver healthcare. Recent reports7, 8 demonstrate the complexity of this process and make recommendations to improve the situation. 3.2 The integration of Clinical and Non-Clinical Risk Management with Clinical Audit, Research and Development, Complaints and Claims has been an important step in managing a cycle of identification, assessment, action and evaluation. 3.3 The baseline assessments for the CNST and Controls Assurance have provided valuable information on both the understanding and present compliance of issues relating to both clinical and non-clinical risk. 3.4 Many of the risk targets discussed build on transferring existing, exemplary good practice that flourishes within the organisation. These all have their roots within the audit cycle and are concerned with the prevention of service failure. 3.5 Risk identification is crucial to the success of the Trust’s risk management programme. This will be addressed through an ongoing programme of risk reviews. The assessments will be undertaken by managers and staff, who will be provided with education and training in risk management techniques relevant to the area in which they are working. 3.6 Clinical risks identified will be analysed by the Clinical Effectiveness Group to determine the potential for frequency of occurrence and severity of outcome. A copy of all assessments undertaken will be passed to the CGRC, which will prioritise them for action. A quarterly summary of actions will be forwarded to the Clinical Governance and Risk Committee. 3.7 It is recognised that it is not possible to completely eliminate all risks. It is necessary therefore to have control measures in place to reduce the likelihood of an adverse occurrence or outcome. This will be addressed through the adoption of some or all of the following measures: 7 8 the development of a comprehensive risk assessment process; the development of a risk management training and education programme; the utilisation of policies, protocols, procedures and guidelines; risk acceptance (i.e. assuming the potential loss and allocating resources to cover the financial consequences); risk avoidance (i.e. utilising alternatives); risk transfer (e.g. use of insurance, membership of the CNST); contingency and disaster planning to reduce the effects of major internal incidents (e.g. loss of utilities). contingency and disaster planning for external Major Incidents for which the Trust may respond Organisation with a Memory, Department of Health 2000 Building a Safer NHS for Patients, Department of Health 2001 19 3.7 The risk control processes will be monitored regularly by the Clinical Governance and Risk Committee. The Chief Executive and the Trust Board will be informed regularly of the effectiveness of the systems in place, and whether these comply with the changing requirements of the Controls Assurance Project. 3.8 The reporting of untoward incidents and near misses is one of the most essential parts of Clinical Governance and risks management. It is also, in relation to clinical incidents, one of the risk management standards of the CNST9, and will be an important issue with regard to clinical governance. 3.9 The Trust will establish a unified system throughout the Trust for reporting all types of incidents, including accidents and near misses, as a matter of priority. The Glossary section describes what constitutes an incident, and these will be supplemented by a Trust-wide awareness-raising and education programme for all staff. This subject will also be included in the Trust induction programme for new staff. 3.10 Staff will be encouraged to report incidents by the Trust’s commitment to the establishment of an open and ‘blame-free’ culture. They will also be given feedback by their line managers on the action taken (or not) as a result of the incidents they have reported. Such feedback makes staff feel valued and encourages them to report incidents. 3.11 The data collected will be collated and used to track and trend incidents. As such it becomes a useful predictive and analytical risk management tool. 3.12 The provision of computer terminals on Resource Centres provides an excellent opportunity for the use of immediate e-mailed risk management information. Information can be entered directly onto the risk assessment form, thus making it instantly available for analysis. 3.13 In the longer term risk assessments can be linked to the management of complaints and claims, thus facilitating the exchange of information between these areas. 3.14 The Trust has developed a procedure for following up major clinical incidents. The Trust will continue to develop procedures for reporting all incidents and accidents 3.15 High priority will be given to reducing the risks to patient, staff and all organisations involved in Major Incidents within the operating area of the Royal Berkshire Ambulance NHS Trust. This will be achieved by 9 Continued risk assessment of the operational area to identify high profile sites and the development and continuous review of specific plans for those areas identified Ensuring all staff are trained in their potential roles in a Major Incident and that all staff are exercised in those roles Continued development of key relationships in other response organisations and the wider health economy aimed at disseminating good practice. Clinical Negligence Scheme for Trusts, (Standard Number 4) 20 3.16 Adequate control of the potential for, and actual, cross infection reduces risk to both patients and staff. The Health and Safety Working Party will report to the Clinical Governance and Risk Committee. 3.17 The over-riding principles throughout this strategy document are those of risk assessment, adequate training, control and monitoring. The Trust has addressed these by delegating responsibility for health and safety risk assessments to line managers, with the assessments being audited by the Health and Safety Manager. Health and Safety guidance notes are produced which include forms to be used for risk assessments. 3.18 All managers will ensure that they understand their responsibility for undertaking health and safety risk assessments and health and safety is included in the induction programme for all new staff, with updates planned as part of the Trust mandatory refresher programmes. 3.19 High priority will be given to reducing the risks to staff from manual handling of both patients and loads. The following initiatives have been undertaken to ensure that all appropriate staff receives the necessary training: training in manual handling techniques, commensurate with their roles, is provided to all new staff, including bank staff, as part of their induction before they commence their duties; follow up training will be provided for all staff in the future, including bank staff, on a regular basis; records will be kept by the training department on the Promis database of all training given and the names of staff attending Managers are responsible for the manual handling risk assessments in their work areas. 3.20 Regular reviews will be undertaken of the compliance with the Control of Substances Hazardous to Health Regulations 1994 (COSHH). The results of these audits, together with any recommendations for further action, will be reported to the Clinical Governance and Risk Committee via the Health and Safety Working Party. 3.21 The Trust is committed to fire safety and has a Fire Officer advising. The overall objective is to achieve compliance with Firecode, and where there are deficiencies these are known, and are being addressed. The Trust recognises the importance of building upon the good work already undertaken to ensure that fire safety remains a high priority agenda item. The introduction of mandatory bi-annual fire lectures for staff is being considered; The Trust has addressed the risk of fire resulting from smoking by initiating a no smoking policy within Trust buildings. 3.22 The security of staff, patients and visitors, is a high priority for the Trust. To this must be added the need to address an on-going problem of break-in theft and theft of computer equipment in particular. 3.23 In order to address the various issues in a systematic way, a security strategy is being drafted by the Estates Manager and the Emergency Services Directorate to be 21 approved by the Clinical Governance and Risk Committee before being presented for ratification by the Trust Board. The Strategy will include: an education programme to raise staff awareness of security measures and the need for vigilance; security risk assessments; security marking and securing of equipment; access control; use of closed circuit television (CCTV) system or dummies in lower risk areas; continued training for staff in the management of aggression and breakaway techniques; continuous review of the lone worker policy and procedures for staff working in the community or otherwise alone in Trust buildings. prevention of theft of personal / trust / patients’ property 3.24 The Trust is dependent upon reliable equipment, safe and suitable buildings and vehicles and continuous power and supply services to carry out its responsibilities of caring for patients. Buildings and vehicles will be regularly maintained so as to minimise any risks to health and safety. This will be achieved following safe systems of work, with contingency plans in place to deal with any emergencies. 3.25 All equipment will be adequately maintained, with maintenance records kept and the case for replacement equipment identified through the business planning process. 4 Research and Effectiveness 4.1 Increasing knowledge about health interventions and service delivery provides a basis for increasing the effectiveness of services. Encouraging an inquiring, research base culture provides focus for clinically important questions. The implementation of research findings, including Health Technology Assessments, NICE guidance and work carried out by groups such as the Centre for Reviews and Dissemination, underpins Clinical Governance. In order to support staff involved in these activities we need to continue to develop our research capacity. 4.2 Research in the Trust is in its infancy and while we remain a small organisation, will struggle to be of significant value. Collaboration with other ambulance services and inter-sectoral institutions has most potential to deliver on the recently announced research governance agenda10. The minimum we must ensure is that all healthcare professionals have the skills to access and use information to inform their practice. 5 Staffing and Staff Management 5.1 The Trust Board recognises that staff who feel valued, supported and informed in their work practice will have an enhanced sense of pride and loyalty to the Trust. Consequently the risk profile of the Trust will be reduced and the quality of clinical services enhanced. The Trust is committed to the welfare and development of its staff in Improving Working Lives, as evidenced by its Pledge to achieving a Top 10 Research Governance Framework for Health and Social Care, Department of Health 2001 22 Performing People Organisation. This commitment is demonstrated by the Chief Executive and managers continuing to take action to ensure: staff are provided with a safe and pleasant environment in which to work; staff are consulted to identify what their needs are; staff are asked to feed back on the extent to which they consider their needs are being met; staff development and education needs are met; staff are offered help, support and counselling when required; staff are provided with satisfactory occupational health services, which include access to help in dealing with work-related stress; staff are regularly trained in such techniques as manual handling, resuscitation skills, infection control, fire training and recognising and dealing with aggression; staff are fully informed regarding Trust-wide developments and have the opportunity to provide feedback. 5.2 The Trust will continue to develop the induction programme for all grades and disciplines of staff. These will include training in health and safety issues, as well as other aspects of risk management. The programme will be mandatory and line managers will be responsible for ensuring that all staff complete the course provided by the HR department, as soon as possible after appointment. 5.3 Individual departments are encouraged to develop their own orientation programmes to follow on from the Trust induction. These will incorporate specific objectives to be achieved within a specified timeframe. (See example Appendix 4) 5.4 The Trust supports the professional development of its staff, whose education and training needs are identified through its individual performance appraisal and professional development review. Systems of clinical supervision will continue to be developed, which will provide support and guidance for all clinical staff. At Resource Centres the Clinical Supervisors and members of the Training Department will play key roles in the development of a culture of clinical effectiveness and the use of evidence-based clinical care. 5.5 The Trust will address the risks associated with the use of bank, agency and locum staff through the implementation of the following control measures: 5.6 the introduction of an appropriate appraisal system for bank staff who do not also hold a substantive post. a review of the robustness of Trust and supplying agencies’ systems with regard to ensuring the quality, authenticity and experience of bank, agency, or locum staff. the orientation of all agency staff when first employed within the Trust, by the line-manager; the provision of on-going supervision for all agency staff. The Trust will address the risks associated with the use of outside contractors by the appointment of only appropriate suppliers of services registered with quality accreditation systems or approved by the Finance Department of the Royal Berkshire Ambulance NHS Trust 23 5.6 The Health and Safety at Work etc.: Act 1974 and subsequent legislation oblige all members of staff to accept some responsibility for maintaining a safe workplace environment. Staff have a right to highlight their concerns about any health and safety issue, either directly to their manager, or through their appointed health and safety representative, or other members of the Trust Health and Safety Working Party. 5.7 Staff involvement and development are the cornerstones on which the success of Clinical Governance will depend. The Trust is committed to developing sound partnership working across all staff groups, ensuring there is clear ownership, responsibility and accountability through established management development programmes, workforce planning and Improving Working Lives. 5.8 These and other management training programmes facilitate: Clear team goal and objectives Clear lines of accountability and authority Diversity of skills and personalities Clear individual roles for staff Shared tasks Regular internal formal and informal communication Staff participation The ability to change and develop The confronting of crisis and conflict Feedback to individuals Team and individual rewards and awards Monitoring of team/individual objectives Outside recognition of achievement Two way external communication Feedback on team performance 5.9 The Trust recognises the significance of the contribution made by individual staff members (e.g. through the Trust newsletter – the RBAT Times, an at the annual “Awards Night”. 5.10 The targets therefore, have been developed to reflect the growing need to ‘manage’ professional life in today’s NHS and attempt to reconcile infinite demand with finite resources in a disciplined manner. 5.11 The Trust will continue to work towards an understanding of the work life balance in line with the demands of personal and professional lives. 5.12 The management of Clinical Governance is the responsibility of every staff member. This will be reflected in all job descriptions and job plans, which will emphasise the importance of the individual’s contribution to ensuring that Clinical Governance practices underlie their various duties and responsibilities on an on-going basis. 24 6 Education and Training 6.1 Central to achieving Clinical Governance is the creation of an environment, which enables and encourages the best clinical practice and performance, ensuring that we have staff with the right skills at the right time to perform to their best. The Trust believes that this will be delivered ultimately through a multi-professional approach and over the next 5 years, will work towards ensuring a fully integrated education programme is in place. The appraisal process is seen as the focus to be built on to provide this. 6.2 The Trust also values the importance of ensuring that staff are supported and provided with clear direction and leadership. The fundamental part of Clinical Governance is centred on changing behaviour towards safer patient care. This change can only be maintained through promoting a culture of continued learning. 6.3 The targets discussed build on an analysis having completed the baseline assessments for Controls Assurance and CNST. The Trust endorses the principles of ‘lifelong learning’ for all individuals and teams to meet the needs of patients, deliver good health outcomes and Trust priorities, while enabling professionals to expand and fulfil their potential. 6.4 To be successful, education and training need to operate on two dimensions to support the clinical governance strategy. First, the education and training needed to generate the organisational awareness and commitment and support for systems and procedures. Second, the education and training needed to develop continuously the individual professionals’ level of knowledge and skill. 6.5 The Clinical Governance Strategy will only be successful if supported by education and training, at varying levels, for all staff. Programmes will be designed to maintain awareness of Clinical Governance and to continue to provide all employees with the necessary level of knowledge of the procedures for clinical governance and for identifying and reporting risk situations. 6.6 The programmes will include an element of education about the necessary culture change for all staff, and, to varying degrees, specific technical and practical training for those involved at the different levels of the clinical governance management structure. 6.7 Clinical Governance is an essential part of the staff induction programme. Attendance will be mandatory for all new staff, and the process will be monitored to ensure effectiveness and attendance. The programme will include information on clinical risk management where appropriate, as well as health and safety and organisational risks. 6.8 The following subjects will be included in an on-going annual education programme. an overview of the general principles and objectives of Clinical Governance management; a definition of the role of staff in the Clinical Governance management process; 25 raising awareness of the reporting requirements and indicators for each work area; the Trust’s strategic Clinical Governance management objectives; the Trust Clinical Governance management structure. 6.9 The ongoing education programme will be enhanced through the provision of literature, posters, Trust newsletter and the Trust Intranet, which allows access to the Internet, including both local and Trust-wide Clinical Governance management standards. 6.10 The acquisition of a portable information system (a suitable E-PRF) will considerably enhance our ability to deliver training and information on amended policies and procedures, etc and the Trust is actively involved in investigation of procurement. 7 Use of Information to Support Clinical Governance and Healthcare Delivery 7.1 The Trust recognises the importance of timely and accurate information to inform Clinical Governance. This information needs to be comprehensive, routinely available, relevant, up to date and accurate and capable of comparison with national data. 7.2 The use of external peer review and clinical benchmarking will enable comparisons to be made to identify scope for improvements and the Trust demonstrates its acceptance of this by involvement with Regional audits directed and designed by the South-east Clinical Governance Ambulance Group (SECGAG) and the South-east Ambulance Clinical Audit Group (SEACAG) 7.3 The Trust recognises that a considerable amount of work is required to develop this area, ensuring that the Trust has robust, user-friendly information available, most effective and efficient being an electronic mobile data system. Clinical governance strategy must seek to create health systems that are able to routinely adopt good practice and electronic systems enhance this capability, particularly in an ambulance service where the staff are scattered in pairs or individually across the county 7.4 The challenge of good clinical governance, is also to ensure that heath organisations develop the information systems, the infrastructure and the training to enable access and use of clinical information and research evidence to become part of routine clinical practice. 7.5 Not infrequently, a major cause of risk is that members of staff are individually uncertain as to what is expected of them, particularly in emergency situations. This uncertainty can be compounded when other members of the same team have different understandings of the actions to be taken in such circumstances. Up-to-date, easily understood policies, protocols, procedures and guidelines are an essential part of Clinical Governance and risk reduction. 7.6 There is adherence to a clear Trust format for policies and procedures, which are indexed and annotated with a review date and authorship. A central record will be kept of all documents, and an index compiled, updated at regular intervals and circulated throughout the Trust. This will also be available on the Intranet to ensure 26 that different areas do not each draft their own document on the same subject. An archive of obsolete or superseded policies will also be maintained for possible use in the future defence of cases of alleged negligence against the Trust. 7.7 The Clinical Effectiveness Group will agree standards and procedures for the definition, format, drafting and review of all clinical policies, protocols, procedures and guidelines across the Trust. This will ensure that such documents are researchbased and follow any existing, relevant national guidelines. They will also have a section identifying risk issues and how to minimise exposure. 7.8 Systems are in place for formulating, ratifying and circulating the policies, protocols, procedures and guidelines. These will ensure that the documents are distributed to the relevant clinical area(s), read and understood by the staff to whom they apply and acted upon appropriately. Regular audits will be undertaken to ensure staff awareness of and compliance with the content. 7.9 The Trust will support the Caldicott Group and Business Services Department in their systems for the tracking, storage and retrieval of patient report forms. These will be audited on an on-going basis, with the results of the audits monitored by the Caldicott Group and reported to the Clinical Effectiveness Group. 7.10 The content of patient report forms will be subject to on-going audit both by the Clinical Supervisors and the Clinical Effectiveness Department. The results of such monitoring will be correlated by the Clinical Effectiveness Groups, with key findings disseminated to appropriate staff groups and reported to the Board on a monthly basis. 7.11 High priority is given by the Trust to information management and technology (IM&T) with the Finance Director being responsible for Information Services. A comprehensive strategy will be produced for the development of systems and services. A review of the existing systems, services and processes has taken place. The focuse will now be on the procurement and implementation of an electronic information management system which includes an E-PRF with the potential of interactive e-learning. The Strategy will include standards and policies which address the majority of risk issues relating to its implementation. The risks intrinsic to the Trust will also be assessed and any necessary action taken to control them. These risks include: the recruitment and retention of specialist staff; the risks associated with out-sourcing; the location and security of the network equipment and other hardware. 7.13 The development of a Trust-wide Intranet has resulted in there being at least one computer terminal in each Resource Centre. From the risk management perspective, this will provide easy access to clinical guidelines, which will be accessible through the network, as well as other Trust policies and protocols. These will include risk management policies and procedures. The system also allows completion of electronic versions of several Trust proformas. The eventual delivery of a portable electronic information system (includes an E-PRF) will enable more timely access to these documents. 27 APPENDIX 2 The Targets Agreed For 2002-2003 For The Nine Pillars Of Clinical Governance Set Out For The South East Region Of The NHS. a) Clinical Governance Strategies Targets CNST level 1 and achieve level 2 o Level 1 – 2001 o Level 2 - 2003 Maintain Controls Assurance accreditation o Level 2 milestones – March 2003 o Level 3 milestones – March 2005 CHI visit, mid 2002 o Project group, including stakeholders, to agree action plan and subsequent delivery Maintain progress against Trust strategy objectives 28 b) Consultation And Patient Involvement Targets To implement a patient, carer and public involvement Strategy by February 2003 The Trust will move towards the establishment of a PALS service by April 2003 The Clinical Effectiveness Group will identify and implement ways to ensure patients, carers and the public are involved in their development To achieve a coordinated approach to the development of patient information o To build on existing good practice (e.g.: the Ethnic and Cultural Awareness Handbook and the Multilingual Phrase Book) and implement ways to ensure that minority groups have fair access to services. o Improving advice for patients/users to obtain additional information about their condition when not transported Good Practice will be shared across the Trust through Clinical Supervisors and training programmes Identify groups for patient / user involvement by March 2003 Ensure reports on complaints and claims demonstrate (document/evidence) changes which have reduced risk as a consequence. CEfD to report on and draw up action plans where appropriate on patient experience evaluation The continued development of links into primary and secondary healthcare and social care systems within the local health economy. 29 c) Clinical Audit Activity Targets Ensure regular meetings of multi-disciplinary Clinical Effectiveness Group Clinical Effectiveness Group will monitor outcomes and improvements from its clinical audit programme Clinical Effectiveness Group will agree priorities and set standards which will monitor clinical outcomes The Trust Clinical Effectiveness Group will work to ensure that all audit activity undertaken closes the loop and follows through with actions and implementation Resources required to support clinical audit will be reviewed November 2002 Conduct CHD multi-agency audit July 2003 Support national / regional audits o Continue National MI audit begun August 2002 (pilot completed) o Conduct 6 agreed performance indicator audits per year for benchmarking with the South-east ambulance trusts o Support the development of a cardiac arrest database with the South-East Ambulance Clinical Audit Group (SEACAG) Ensure patient input into July 2003 Develop annual report to include improvements made, actions taken, multidisciplinary working and patient involvement Audit support to validate progress being made towards risk management objectives o Standardised accident/near miss/adverse incident reporting - 2002 o Compliance with 19 Controls Assurance Standards for level 2/3 milestones 2002 30 d) Clinical and Non-Clinical Risk Management Targets Ensure staff are trained in all aspects of clinical and non-clinical risk assessment – March 2003 Continue the rolling clinical and non-clinical risk assessment process building on existing best practice, linking in work commenced to meet the requirements identified for Controls Assurance, CNST and CHI – December 2002 Build on existing good practice linking the function of health & safety into the agreed programme of clinical & non-clinical risk assessment for controls assurance – March 2003 To ensure the management of clinical and non-clinical risk is integrated into the Trust’s business planning process Continue the investigation of clinical and non-clinical incidents Continue the development, review, training and dissemination of good practice in Major Incident Planning, including other response organisations and organisations in the wider health economy of the Operating Area of Royal Berkshire Ambulance NHS Trust, where appropriate Develop and publish quarterly Clinical Governance Newsletter – From April 2003 Develop a security strategy by March 2003 31 e) Research and Effectiveness Targets Implement Research Governance focusing on: o improving patient involvement o monitoring of R&D activity o implementing intellectual property strategy o improving liaison with LREC Provide regular training in Critical Appraisal Skills – annual programme to be produced by July 2003 Ensure dissemination of results of pre-hospital research both within and external to the Trust Promote Internet website on research information e.g. KA24 Ensure that all healthcare professionals have access to evidence through electronic and hard copy media 32 f) Staffing and Staff Management Targets Develop strategies for protected time for on-going professional development which are in balance with operational staffing levels required to deliver a quality service – 2004. Continue provision of access to training management development programmes for staff in management positions The provision of a portfolio of evidence over a wide range of policies and procedures that improve the working lives of NHS staff – Accreditation required April 2003 o A policy on harassment and bullying was implemented in Nov 2000 o A strategy for zero tolerance to protect NHS staff from violence has been produce – April 2002 - and will continue to be enforced o Produce and implement strategy for improving diversity o Ratify the draft procedure for monitoring equal opportunities by 2003 o Produce a policy on recruitment and selection of black and ethnic minorities by 2004 o Produce and implement strategy for flexible retirement (e.g. HDU for A&E staff) – April 2003 Improve the use of the established appraisal system with quantifiable aims and objectives, which promote best practice while identifying accountability to deliver the overall clinical governance strategy. Aims and objectives identified may include: o How best practice is identified o How practice can be monitored effectively o What is meant by clinical risk management o How complaints can be used to influence changes in clinical practice o The individuals role within the clinical governance framework 33 g) Education and Training Targets Scope and develop training needed to generate cultural change, knowledge and awareness of the concept of clinical governance and the supporting infrastructure of systems needed to support it Continue provision of the education and training needed to sustain and continuously develop the individual professional’s knowledge and skill, which will ultimately determine the quality of care provided. Develop and facilitate ‘self-learning into practice’ through Continuing Professional Development (CPD) schemes Improve mandatory Trust induction programmes for non-clinical staff, which includes an introduction to clinical governance and clinical/non-clinical risk management All staff to attend a department specific induction programme appropriate to the specialty in which they are working Develop the training of non-clinical staff in the Trust in the use of AEDs All clinical staff to have attended CPR/AED training in any 12 month period, 90% of eligible non clinical to have attended CPR/AED training in any 6 month period – November 2003 h) Use of Information to Support Clinical Governance and Healthcare Delivery Targets Maintain improvements in PRF completion Develop a comprehensive strategy for IM&T Procure an electronic mobile data system (includes an E-PRF) - April 2004 Identify standards, calibration and audit for medical equipment Implement drug audit system (Audit commission report ‘A Spoonful of sugar’ 2002) 34 APPENDIX 3 GLOSSARY OF TERMS Accident Any untoward or unexpected event which results in injury to or adverse effect on the physical or mental health of an individual. Adverse Clinical Incident An incident causing injury where a clinician is directly responsible for the management of the person injured. Blame Free Culture Where individuals may feel free to raise matters of concern without fear of retaliation. It does not allow for wilful neglect. Clinical Negligence A breach of a duty of care by Health Care professionals or by others consequent on the decisions or judgements made by Health Care professionals. Clinical Governance A framework through which NHS organisations are accountable for continuously improving the quality of their services and safeguarding high standards of care by creating an environment in which excellence in clinical care will flourish Clinical Waste Waste arising from investigation, treatment, care or research which is toxic, infectious or otherwise potentially dangerous. Clinician Those directly involved in the care and treatment of patients including Ambulance Care Assistants. Continuing Professional Development See Lifelong Learning. Corporate Governance The framework through which the Trust is held accountable for the way in which it conducts its corporate business including meeting its statutory financial duties. CNST Clinical Negligence Scheme for Trust. A mutual of over 400 Trusts nationwide subscribing to a central pool to cover Clinical Negligence costs. The CNST is part of the NHS Litigation Authority - a Special Health Authority. 35 Incident Any untoward or unexpected event which interferes with the orderly progress of activity and which resulted, or could have resulted, in one or more of the following: injury to, or adverse effect on, the physical or mental health of any person; damage to or loss of any property, including buildings, equipment, vehicles or materials; a “near miss” which could have resulted in the above Lifelong Learning A process of continuing development for all individuals and teams which meets the needs of patients and delivers the healthcare outcomes and healthcare priorities of the NHS and which enables professionals to expand and fulfil their potential. Medical Devices Agency Assesses the safety and performance of healthcare products. National Institute for Clinical Excellence (NICE) A Special Health Authority established to promote clinical and cost-effectiveness by producing clinical guidelines and audits for dissemination throughout the NHS. NHS Executive The NHS Executive is part of the Department of Health, with offices in London and Leeds and eight Regional Offices across the country. It supports Ministers and provides leadership and a range of central management functions to the NHS. NHS Trusts Public bodies providing NHS hospital and community health care. Personal Development Plan (PDP) Developed by individual health professionals as part of lifelong learning. Special Health Authority Health Authorities with unique national or supra-regional functions which cannot be effectively undertaken by other kinds of NHS bodies (for example, the Prescription Pricing Authority). 36