120117-Innov-rounding
advertisement

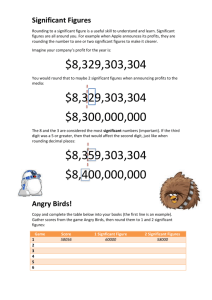
Nursing Practice Innovation Fundamental care Using intentional rounding on a medical assessment unit produced a drop in call bell frequency and improved patient experience. Staff buy-in was essential to the process Engaging staff with intentional rounding In this article... Intentional rounding explained Implementing IR and addressing staff concerns about it Gaining feedback on IR from patients and staff Authors Greg Dix is director of nursing and governance; Jackee Phillips is junior sister, medical assessment unit; Mark Braide is practice development nurse; all at Taunton and Somerset Foundation Trust. Abstract Dix G et al (2012) Engaging staff with intentional rounding. Nursing Times; 108: 3, 14-16. This article describes the introduction of intentional rounding on a busy medical assessment unit and how staff engagement and understanding of the process is essential to its successful rollout. Staff’s reaction to the implementation is highlighted and the benefits to care delivery discussed. E arlier this month, the prime minister called for changes in the way nurses deliver care. This was in response to recent reports drawing attention to care failings (Care Quality Commission, 2011; Health Service Ombudsman, 2011; Department of Health, 2010). One of the recommendations was for nurses to undertake regular rounds to ensure that every hour they will be able to check that each patient is comfortable. This method of systematically reviewing all patients on a regular basis to ensure their fundamental care needs are met is not a new nursing concept. For many years, nurses carried out regular “back rounds”, which had a particular focus on skincare and pressure relief (Fitz-simmons et al, 2011). Anecdotally, nurses believed regular contact with patients had the added value of enabling therapeutic relationships to develop between them. The rounds made patients feel cared for and reassured, knowing that within a couple of hours they would be visited by a nurse and given an opportunity to raise any personal needs. However, while back rounds ensured all patients were reviewed at least every two hours, they were task-orientated and left little room for delivering individualised holistic care. Intentional rounding Intentional rounding (IR) is a more recent development imported from the US that could be described as a modernised back round. It involves nurses carrying out regular checks on individual patients at set intervals to assess and manage their fundamental care needs with respect to six core elements: » Pain; » Hydration and nutrition; » Continence; » Anxiety; » Falls; » Pressure ulcer prevention. IR places the patient at the heart of the ward routine by taking care back to the patient’s bedside. The system improves patients’ experience of care through the reassurance provided by the increased visibility of nursing staff and the knowledge that they can raise any concerns or needs when they are next visited by a nurse so that they can be dealt with promptly. These can range from 14 Nursing Times 17.01.12 / Vol 108 No 3 / www.nursingtimes.net needs that may seem relatively unimportant to ward staff but are hugely significant to patients to potentially serious clinical concerns. Meade and Bursell (2006) noted a significant increase in patient satisfaction and a reduction in pressure ulcer incidence after introducing IR, while the Studer Group’s (2007) work on IR identified similar significant improvements in patients’ experiences of care and clinical outcomes. Musgrove Park Hospital, part of Taunton and Somerset Foundation Trust, has been using IR for a year. The hospital has more than 600 beds, 30 wards and 15 operating theatres. It serves a population of 340,000 and treats more than 450,000 patients each year. IR was just one initiative within the hospital’s Back to Basics campaign. It was championed and led on the medical assessment unit by junior sister Jackee Phillips. IR was initially tested with a bay of patients using rapid cycle testing (plando-study-act (PDSA) cycles) on the medical assessment unit in October 2010. It was rolled out across the unit in January 2011. Every patient receives an hourly or twohourly review by either a nurse or healthcare assistant, with frequency depending on the patient’s clinical condition. Unlike some hospitals using IR, we include all patients rather than just those that are at risk of falling or skin damage. The overarching principle is that all patients, regardless of presentation, have a right to expect their fundamental care needs to be identified and met promptly. Effects of implementation After IR was rolled out, an audit was conducted, typically at weekly intervals on different days of the week but at the same hour (1.00-2.00pm). The audit collected the number and frequency of call bells (Fig 1a), Keywords: Intentional rounding/ Implementation/Personalised care/ Patient experience ●This article has been double-blind peer reviewed 5 key points fig 1. the impact of intentional rounding on call bell usage and complaints 1 Intentional rounding involves nurses checking individual patients at set intervals to assess and manage their fundamental care needs It places the patient at the heart of the ward routine IR reduced the frequency of call bell use Introducing IR requires a cultural change and staff need support to bring in the change IR has a positive effect on patient experience 2 3 4 the completion of the IR form over 24-hours and patient feedback cards. Further metrics are now collected on pressure ulcers, falls and patient satisfaction data. IR has demonstrated a significant reduction in the frequency of call bell usage and the length of time patients wait to have their call bells answered. Fig 1b shows that when IR was performed consistently, call bells use reduced from an average of eight an hour before the system was introduced to one an hour after. It also reduced the time taken to respond to the calls from three minutes to less than one (Fig 1c). Evidence demonstrates that patients frequently use call bells for non-urgent needs as they feel it is the only way to gain nurses’ attention (Tea et al, 2008; Meade and Bursell, 2006). Before IR, call bells were not prioritised due to their frequency (they were typically ringing for 24 minutes in every hour). IR significantly reduced call bell use so now, when a bell is rung, it is usually for a significant reason. The call bell is now more audible because it is used less frequently so not perceived as background noise. Another positive impact demonstrated more recently concerned the early identification of pressure ulcers. The IR tool was amended to include a section on the form to acknowledge the risk of pressure ulcers, followed by a section indicating whether 27 exit card responses, all with the patient’s skin has been positive comments. This cominspected; this was further The number of calls fell pares to just four responses developed so nurses now comdramatically when intentional rounding from the test bay of 12 beds plete the SKIN bundle tool. was introduced as did over a same time period before At times IR activity reduced, their duration. rollout – a significant increase for example when the workload Complaints also reduced of approximately 58%. was particularly demanding; Fig While these numbers are 1a and 1b show that when this small, there has been a noticehappened, the use of the call bell increased, as did call bell duration. IR able rise in the number of thank-you cards activity falling away from time to time coin- received by the ward since the introduccided with a reduction in ward support by tion of IR and a reduction in complaints members of the IR project team. This was and concerns (Fig 1d). fed back to the ward sister and measures put in place to refocus the ward staff. The Staff concerns support from the project team, led by our Before implementing IR, we anticipated practice development nurse, was essential that staff would see the system as too timeconsuming. We therefore reviewed potenin the early stages of implementation. In addition to reducing call bell usage, tial problems identified in each of the six IR care domains in the pilot. It became IR has increased patient satisfaction. Musgrove Park Hospital uses many apparent that most patients required little methods of collecting patient feedback, in the way of intervention (90% of rounds one of which is a system of feedback cards did not require any problems to be to identify any concerns or recognition of addressed), but patients valued being good practice. The cards are completed asked (feedback card responses valued the voluntarily by patients or relatives and visibility of staff ). The majority of interventions/problems deposited in a post box before discharge. In the pilot MAU, we received nine exit were resolved by the next round (85% in the card responses (eight beds) over a three- trial period audit). In addition, persistent problems are week period compared with just four from the rest of the ward (12 beds). In the first more readily identified and documented, three weeks after IR had been implemented and, since the effectiveness of intervenacross the whole unit (20 beds), we received tions becomes clear quite quickly, this www.nursingtimes.net / Vol 108 No 3 / Nursing Times 17.01.12 15 Al Grant 5 Nursing Practice Innovation Box 1. Staff comments “Since the implementation of IR, there has been a marked improvement on the MAU. Our complaints have reduced, the unit has a feel of calmness. “I have worked on the unit for two years and never witnessed a quiet period after lunch, when patients could have a quiet hour. Since implementing IR, we are now able to turn the lights off on the unit from 1.00-2.00pm … “I have witnessed first hand where pain control issues have been identified quite early as a result of IR ... IR has enabled better safer practice on MAU to be established, we have reduced our complaints, falls, and pressure area care has been monitored. “This service improvement has brought clinical governance alive in the workplace. Our standards on MAU are improving.” Jackee Phillips, junior sister, June 2011 “Since starting IR on the MAU, we have seen a significant increase in the number of thank-you cards and many positive comments on the exit cards. We have also seen the number of complaints greatly reduced.” Amanda Carr, MAU sister, June 2011 “It is very reassuring to know that every single patient will be checked upon every two hours, regardless of their needs – so any changes in their clinical conditions are going to be rapidly detected. ” Andrew Thompson, MAU consultant, July 2011 improves management and reduces the risk of simply repeating interventions that have not worked. For example, systematic evaluation and documentation of pain management means analgesia is more likely to be altered as needed. While some staff cite the time taken up by IR as a concern, it is difficult to quantify how long it takes to manage failings in care such as avoidable pressure ulcers, or to deal with complaints. Providing IR is implemented consistently, the time taken to carry it out can be offset against time savings from improved patient management. However, this requires staff to support the initiative and to adapt their working practices. Initially, there was resistance by a small majority of staff primarily driven by time concerns. Over time, this resistance has diminished with the active intervention of the ward manager, matron and director of nursing. This issue was also highlighted in similar work carried out on an orthopaedic ward at Whipps Cross University Hospital (Lucas et al, 2010). Staff evaluation A questionnaire was circulated to staff at the time of rollout (January 2011) asking questions on their perceptions of patient care; a follow-up sent out in June 2011 included additional questions directly comparing how they scored care out of 10 before IR and after IR. The response rate for the first survey was 28%, which improved slightly to 36% for the follow-up. The results were mixed. There was no perceived change in the ability to provide individualised care during the initial pilot phase of implementing IR. Surprisingly, staff perceived they had less time to spend with each patient. Some comments from the questionnaire suggest that performing IR on well patients is seen to be to the detriment of those who are unwell as it takes staff away from these patients. Staff were also asked to rate their own satisfaction with the care they were able to provide. Data appeared to show that staff were less satisfied since the implementation of IR. However, despite the negative evaluations of the impact of IR on staff time and satisfaction, when they were asked to compare the quality of care in January with that in June, they appear to report a significant improvement since IR was implemented. Other comments on the questionnaires suggested that some staff did not fully understand the concept of IR. For example, several staff interpreted hydration to mean simply offering hot beverages at twohourly intervals, which would be difficult to achieve and is neither necessary nor the purpose of including hydration as an element of IR. We did, however, receive a significant number of positive comments, some of which are shown in Box 1. Staff buy-in to IR is essential for successful implementation. It is imperative that all staff are provided with education and training before implementation and the director of nursing and senior nursing team are IR champions. Staff perceptions of the IR process need to be managed carefully and it should be emphasised that the patient should always be at the heart of the organisation. As with any change process, there is always an element of resistance, which has to be managed sensitively. 16 Nursing Times 17.01.12 / Vol 108 No 3 / www.nursingtimes.net Conclusion Although some staff expressed concerns about the appropriateness of IR on a busy MAU, it has proved effective and not required additional staff. The only obvious costs so far have been around the production and supply of the IR tool, and in maintaining the audit process. However, the latter is minimal as we already had a well-established ward audit process. With minimal organisational cost but a fundamental shift in ward routine, huge improvements in care have been achieved through implementing IR to the rest of the organisation over the past year. The key to success is to reorientate ward activity to fit around the system rather than trying to fit IR into existing activity. Conducting checks on patients simply with the intention of filling in a form will not resolve their problems. Perversely, it will take valuable time and will act as selffulfilling prophecy for those wishing to dismiss the system as a paper exercise. This is still a problem in a small group of staff, despite clear evidence showing that when IR is done properly and consistently, patient experience significantly improves and improvements in the quality of care can be achieved. It is also important that senior management recognise that staff need to be supported in implementing IR, through the provision of continued training. The system requires a cultural change so managers cannot assume that, because IR focuses on fundamental care, it is easy to achieve. NT References Care Quality Commission (2011) Dignity and Nutrition Inspection Programme. London: CQC. tinyurl.com/CQC-dignity-report Department of Health (2010) Robert Francis Inquiry report into Mid-Staffordshire NHS Foundation Trust. London: DH. tinyurl.com/ mid-staffs-inquiry Fitzsimmons B et al (2011) Intentional rounding: its role in supporting essential care. Nursing Times; 107: 27, 18-21. Health Service Ombudsman (2011) Care and Compassion? Report of the Health Service Ombudsman on Ten Investigations into NHS Care of Older People. London: Health Service Ombudsman. tinyurl.com/care-compassion Lucas et al (2010) Report on – Proactive Patient Rounding: Developing Nursing Practice to Improve the Quality of Patient Care. Whipps Cross University Hospital Trust, London. Meade CM, Bursell LK (2006) Effects of nursing rounds on patients’ call light use, satisfaction and safety. American Journal of Nursing; 106: 9, 58-70. Studer Group (2007) Best Practices: Sacred Heart Hospital, Pensacola, Florida. Hourly Rounding Supplement. Gulf Breeze, FL: Studer Group. Tea C et al (2008) Proactive patient rounding to increase customer service and satisfaction on an orthopaedic unit. Orthopaedic Nursing; 27: 4, 233-240.