Microalbuminuria Screening in Diabetes
advertisement

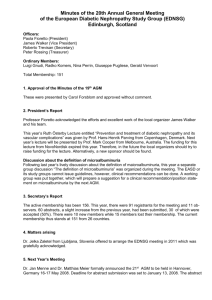
CG10001-1 Microalbuminuria Screening in Diabetes For use in (clinical areas): General Practice and MK General Diabetes Clinic For use by (staff groups): All clinicians For use for (patients): All Adult diabetic patients Document owner: MK Diabetes NSF LIT Status: Approved Purpose of the Guideline The guideline aims to introduce microalbuminuria screening in a standardized way in Milton Keynes, following the NICE guidelines for type 1 and type 2 diabetes.1,2 Contents Definitions Screening Protocol Algorithm page 5 Treatment Main body of document Aims To screen adult patients (>17 years old) with both type 1 and type 2 diabetes annually for proteinuria and microalbuminuria. To measure serum creatinine annually. To treat all patients who are found to have raised levels of albumin in the urine according to NICE guidelines. Introduction Microalbuminuria is a low level of albumin in the urine which is above normal levels, but below what is normally detected by standard urine dipstick. Proteinuria relates to a larger level of protein in the urine, and represents the progression of microalbuminuria. Proteinuria is usually detected with a standard dipstick. Patients with persistent microalbuminuria are at risk of progression to proteinuria, diabetic nephropathy and end stage renal failure. Microalbuminuria also predicts cardiovascular morbidity and mortality in both type 1 and type 2 diabetes. Source: MK Diabetes NSF LIT Status: Approved Issue date: November 2004 Valid until: November 2007 Page 1 of 7 Milton Keynes Hospital Trust CG10001-1 Microalbuminuria Screening in Diabetes Microalbuminuria is measured as a urinary albumin/creatinine ratio (ACR), in a first-voided sample in the morning. There is a 40% day to day variability in albumin excretion, so NICE recommends following up positive tests with two further tests, and only if 2 out of 3 are positive labelling the patient as having microalbuminuria. Definitions Microalbuminuria Albumin/creatinine ratio ≥ 2.5mg/mmol for men ≥ 3.5mg/mmol for women Proteinuria Albumin concentration ≥ 0.2g/l Albumin/creatinine ratio ≥ 30mg/mmol Protocol for microalbuminuria screening (see algorithm) It is anticipated that microalbuminuria screening will be performed from general practice, even for those patients who are attending the hospital diabetic clinic. All adult patients with diabetes should be offered microalbuminuria screening annually with the following exceptions: -pregnant women -type 1 diabetes for less than 5 years duration -patients with pre-existing proteinuria -terminally ill or very frail First pass morning urine specimens should be collected in plain white bottles, and dipped in the practice with a standard dipstick, before being sent to the laboratory. Mark the request card as “other” and add “microalbuminuria”. Serum creatinine should be measured annually. Follow the attached algorithm, and use the Read codes as suggested below. Source: MK Diabetes NSF LIT Status: Approved Issue date: November 2004 Valid until: November 2007 Page 2 of 7 Milton Keynes Hospital Trust CG10001-1 Microalbuminuria Screening in Diabetes Read codes These codes are nGMS contract Quality and Outcomes compliant, and the codes used by the local laboratory for pathology links. 4 byte 46TC Albumin creatinine ratio 46N3 Urine total protein (ie urine protein concentration) C261 DM and persistent proteinuria. C260 DM and persistent microalbuminuria 5 byte 46TC Albumin creatinine ratio 46N3 Urine total protein (ie urine protein concentration) C10EK Type 1 DM and persistent proteinuria C10FL Type 2 DM and persistent proteinuria C10EL Type 1 DM and persistent microalbuminuria C10FM Type 2 DM and persistent microalbuminuria Exemption codes. Patients coded for proteinuria will automatically be exempted from microalbuminuria screening by the quality and outcomes software. Any other patients who are exempted from microalbuminuria screening will need to have an exemption code added. The following code is suggested (4 and 5 byte). 9h41 Exception report diab qual ind: pt uns Source: MK Diabetes NSF LIT Status: Approved Issue date: November 2004 Valid until: November 2007 Page 3 of 7 Milton Keynes Hospital Trust CG10001-1 Microalbuminuria Screening in Diabetes Treatment of microalbuminuria and proteinuria in type 1 and type 2 diabetes. For those patients with confirmed abnormal albumin excretion: Suspect other renal disease if: -particularly high blood pressure -systemic ill health -sudden proteinuria -no progressive retinopathy -significant haematuria Discuss the significance of the findings with the patient. Ensure tight blood glucose control. Target HbA1C <6.5% Start ACE inhibitors (eg. ramipril) and titrate to full dose. (Caution in patients with peripheral vascular disease, or renovascular disease. Caution if creatinine raised. In all patients measure serum creatinine and electrolytes 1 week after initiating ACE inhibitor therapy and after each increase in dose.) If ACE inhibitors are not tolerated, use angiotensin 2 receptor antagonists (eg. losartan or candesartan). Maintain blood pressure below 130/80mmHg. Advise those with kidney damage the advantages of not following a high-protein diet, such as Atkins’ diet. Monitor serum creatinine and refer to nephrologists if serum creatinine >150µmol/l. Treat as high cardiovascular risk. Commence aspirin 75mg daily, once systolic BP <150mmHg. Recommend statin at standard dose. (eg. simvastatin 20mg daily). If intolerant of statins consider fibrates and other lipid lowering drugs. Rationale for main recommendations Work was undertaken by the Milton Keynes Diabetes NSF LIT to compare types of microalbuminuria screening services available their effectiveness and the costs per test. The most cost effective method of organizing microalbuminuria screening is the central laboratory model. Even if prices for GP practice based near-patient testing were lower, there would be a need for a laboratory service to confirm positive results. A hospital laboratory based microalbuminuria screening service will commence from October 2004. References: 1. National Institute for Clinical Excellence. Type 1 diabetes: diagnosis and management of type 1 diabetes in adults. July 2004 www.nice.org 2. National Institute for Clinical Excellence. Management of type 2 diabetes. Renal disease-prevention and early management. Feb 2002. www.nice.org Source: MK Diabetes NSF LIT Status: Approved Issue date: November 2004 Valid until: November 2007 Page 4 of 7 Milton Keynes Hospital Trust CG10001-1 Microalbuminuria Screening in Diabetes Development of the guideline Changes compared to previous document This is the first microalbuminuria screening guideline. Statement of clinical evidence The guideline is based on the NICE guidelines on type 1 and 2 diabetes as referenced. Audit and Monitoring The uptake of micoalbuminuria screening, and prescription of ACE inhibitors or A2 antagonists to those with raised albumin excretion, will be monitored by data collected for the Quality and Outcomes Framework, both at practice and PCT levels. Contributors and peer review Dr C. Paton, Consultant diabetologist. MKH Dr S. Weatherhead, GPwSI diabetes. Dr T. Gamlen, Consultant chemical pathology MKH. Distribution list/dissemination method All GPs All doctors working in MK hospital diabetic clinic. All practice nurses. Diabetes specialist nurses. Document configuration information Author(s): Dr. S. Weatherhead (GPwSI), Dr. C. Paton (Consultant diabetologist) Other contributors: MK Diabetes NSF LIT Consultation: Dr T. Gamlen (chemical pathology) Approved by: Diabetes LIT representing GPs, PNs, Diabetes Specialist Nurses and other AHP groups who care for diabetic patients across the health care sectors. Issue no: 1 (draft) File name: K:\Guidelines\Medicine\Microalbuminuria screening.doc Supercedes: none Additional Information: Joint Trusts Guidelines Steering Group Date Source: MK Diabetes NSF LIT Status: Approved Issue date: November 2004 Valid until: November 2007 Page 5 of 7 Milton Keynes Hospital Trust CG10001-1 Microalbuminuria Screening in Diabetes Microalbuminuria screen Use first morning urine Dip with standard dipstick If normal or +ve for protein If +ve for nitrites or blood Send to lab for urine protein concentration and albumin/creatinine ratio (ACR) Send to lab for M,C and S Protein Concentration ≥ 0.2g/l ABNORMAL ACR ≥2.5mg/mmol for men ACR <2.5mg/mmol for men ACR ≥3.5mg/mmol for women ACR <3.5 mg/mmol for women ABNORMAL NORMAL Repeat 2 further times over next 3 months. If infection, treat and screen again If no infection, consider other causes of haematuria NO 2 out of 3 tests abnormal? YES Protein conc abnormal label as ACR abnormal, label as DM and persistent proteinuria DM and persistent microalbuminuria Treat as high risk Source: MK Diabetes NSF LIT Status: Approved Repeat microalbuminuria screen at 1 year Guideline for microalbuminuria screening Issue date: November 2004 Valid until: November 2007 Page 7 of 7