The Role of Topical and Oral Melatonin in
advertisement

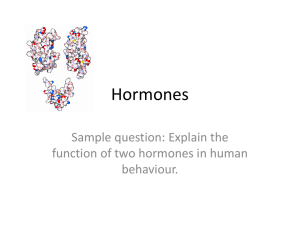
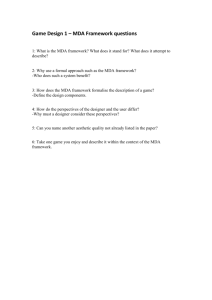
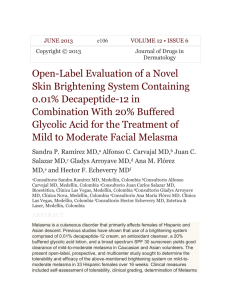
Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 The Role of Topical and Oral Melatonin in Management of Melasma Patients Salim A. Hamadi1, Mohammed Mahmmod Mohammed2, Ashwaq Nejmelden Aljaf3 & Ali Abdulrazak4 1 Faculty of pharmacy & Medical Sciences, Petra University, Amman, Jordan, 2 College of pharmacy, University of Almustansiryah, Baghdad, Iraq, 3 College of pharmacy, University of Baghdad, Baghdad, Iraq, 4 Alkarama teaching hospital, Baghdad, Iraq Dr. Salim A. Hamadi, Faculty of pharmacy & Medical Sciences, Petra University, P.O. Box: 961343, Amman, Jordan E-mail: Hamadi_54@yahoo.com ABSTRACT This novel study was designed to evaluate the possible effects of topically formulated melatonin cream alone or in combination with sunscreen and oral melatonin for the management of melasma patients in comparison with hydroquinone as a standard therapy. This study carried out in the dermatology department at the AL-Karama teaching hospital, Baghdad, Iraq. In a double blind manner, this preliminary clinical study was performed on 36 patients with epidermal melasma and 10 healthy subjects as control. They were diagnosed as having melasma and they were under dermatologist supervision during the entire period of treatment. The patients were allocated into four groups (A, B, C, and D), and treated with topical melatonin only, topical melatonin and sunscreen, topical and oral melatonin, and 4% hydroquinone cream, respectively for a period of 90 days followed by 30 days treatment with placebo. The severity of melasma was evaluated using the Melasma Area & Severity Index (MASI) before starting treatment and after each 15 days for 120 days. To evaluate the oxidative stress status, malondialdehyde (MDA) and glutathione (GSH) levels in plasma were measured before starting treatment and after 45, 90, and 120 days of treatment. At the end of treatment period (90 days); all melasma patients demonstrated significant reduction in MASI score in different levels. In addition, the plasma MDA levels were decreased and plasma GSH levels were increased in different scales after 90 days of treatment. The overall results of this preliminary study suggested that topical melatonin could be used as a hypopigmenting agent in treatment of melasma, and this effect is augmented by the oral administration of the drug and the use of sunscreen, possibly by its antioxidant activity or by other mechanisms unrelated to antioxidant effect. Key ward: Melatonin, Melasma, antioxidant, INTRODUCTION Melasma is one of the most common causes of acquired, symmetric hypermelanosis of the face characterized by irregular light- to gray-brown patches on sun-exposed areas (Grimes, 1995). The most common sites of involvement are the cheeks, forehead, upper lip, nose, chin, and occasionally the forearms (Sivayathorn, 1995). Melasma seen mainly 1 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 in women at any time during the years of reproductive activity, it may be seen in men, and it tends to occur more often in dark skinned individuals ( Bleehen et al., 1992). Melasma usually distributed as one of three clinical patterns; centrofacial, malar, and mandibular ( Sanchez et al., 1981). Melasma can also be divided into three types according to Wood’s light examination of the skin (Grimes, 1995). The epidermal type has increased melanin predominantly in the basal and suprabasal epidermis with accentuation by Wood’s lamp. The dermal type has melanin-laden macrophages in a perivascular distribution in superficial and deep dermis, with no Wood’s lamp accentuation. The mixed type has both elements and appears as a deep brown color, with Wood’s lamp accentuation of only the epidermal component (Pathak, 1986). Various factors and causes are responsible for the pathogenesis of melasma, but UV exposure, genetic influences, and hormonal changes are the most commonly cited etiologic factors (Pathak, 1986). Many therapeutic agents are available but are often unsatisfactory, including sunscreen and hypopigmenting agents like hydroquinone, Tretinoin, and Azelaic acid. The most commonly used hypopigmenting agent for the treatment of melasma is hydroquinone, which reduces the conversion of L-dopa to melanin by inhibiting the enzyme tyrosinase, hydroquinone used alone or in combination with other therapies, such as tretinoin, topical corticosteroids, and/or superficial peeling agents( Balina & Graup, 1991),(Guevara & Pandya, 2001),( Hurly et al., 2002). Recently, it has been demonstrated that the generation of oxygen free radicals in response of skin exposure to the sun light is involved in the pathogenesis of melasma. The administration of antioxidants may decrease the effects of oxidative damage induced by UV radiation on skin pigmentation (Huh et al., 2003). Melatonin is a hormone with multiple functions in human, synthesized and secreted by the pineal gland in response to changes in the darkness and light environment of the human (Brzezinski,1997). It is a powerful antioxidant and the most potent free radical scavenger known (Sener et al., 2003). A distinct dose-response relationship was observed between the topical use of melatonin and the degree of UV-induced damage, melatonin enhances the ability of the skin to repair itself from free radical-induced damage during day light hours (Ryoo et al., 2001). Melatonin, vitamin C, and vitamin E, as antioxidants, may function in melasma by reducing UV-induced free radicals. We chose melatonin not only due to its powerful antioxidant activity, but also for its effect on the hormones that involved in the pathogenesis of melasma, like melanocytes stimulating hormone (MSH), estrogen, and progesterone (Snell & Beschitz, 1960). This study was performed to evaluate the possible effects of melatonin (alone or in combination with sunscreen) in the improvement of melasma patients, and comparing these hypopigmentic effects with those produced by hydroquinone. MATERIALS AND METHODS This preliminary clinical study was carried out on 46 subjects, 36 patients with melasma (22 females and 14 males) aged (17-38) years with a mean of age (26.3 ± 5.2) years, and have a disease duration of (4.6 ±3.2) years. The patients included in this study were diagnosed as having epidermal type of melasma, were free from apparent other diseases. 2 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 The patients were under dermatologist supervision during the period of treatment. All patients were instructed to quit any other depigmenting and sun-protecting medications at least two weeks before starting the treatment. The patients were allocated into four groups and according to the treatment schedule indicated, as follows: Group A: Include 10 patients (3 males and 7 females) treated with 5% melatonin cream prepared for this purpose in a two daily doses at afternoon and night. Group B: Include 10 patients (4 males and 6 females) treated with topical broad-spectrum sunscreen (SPF 50) in a single morning dose, and with 5% melatonin cream in two daily doses at afternoon and night. Group C: Include 10 patients (4 males and 6 females) treated with 5% melatonin cream in two daily doses at afternoon and night and with 3mg/day melatonin tablet in a single daily dose at bedtime. Group D: Include 6 patients (3 males and 3 females) treated with 4% hydroquinone cream in two daily doses at afternoon and night. Ten healthy subjects (2 males and 8 females) with the same age range as that of patients (26.5-35) years with a mean of age (29±3.7) years were selected and served as controls for comparison. In a double blind technique, all patients were received these treatments for three months, and then received a placebo formula for one month. Melasma severity evaluated according to the area involved, color, and homogeneity of melasma using the Melasma Area and Severity Index (MASI) introduced by KimbroughGreen et al., 1994. In this system the face is divided into four areas and each area represent a specified percentage of the whole face, as follow: Forehead = 30%, right malar = 30%, left malar = 30%, and chin = 10%. The MSAI score was calculated by the following equation: MASI = 0.3 (DF + HF) AF + 0.3 (DMR + HMR) AMR + 0.3 (DML + HML) AML + 0.1 (DC + HC) AC. Where D = darkness and H = homogeneity, A = area, F = forehead, MR = right malar, ML = left malar and C = chin The values 0.3, 0.3, 0.3 and 0.1 represent forehead, right malar, left malar and chin percentages of total facial area respectively (14). MASI score was measured before treatment as base line, and every 15 days for 120 days (four months). To evaluate the roles of oxidative stress in the etiology and pathogenesis and the roles of antioxidants in treatment of melasma, fresh blood samples were used for malondialdehyde (MDA) (as a marker of lipid peroxidation), and glutathione (GSH) (as a marker of the antioxidant system) measurements in plasma. Blood samples were collected from patients of groups A, B, C, D, and control group by vein puncture, the first sample was drawn before treatment (as baseline samples), after 45, and 90 days of the 3 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 treatment, and then after 30 days of placebo treatment to evaluate the change in the studied parameters. The student’s t-test and analysis of variance ANOVA were used to examine the degree of significance, and P value less than 0.05 was considered significant, and P value less than 0.01 was considered highly significant. RESULTS The result of this study revealed that all melasma patients in the four groups that treated with different treatment regimens demonstrated significant reduction in MASI score in comparison to baseline after 90 days of the treatment. However, monitoring the follow up period with placebo treatment (for 30 days) showed that group A patients demonstrated non-significant reduction in MASI score in comparison to the baseline value (P>0.05), while group B, C, and D patients demonstrated increased MASI score over that achieved at day 90 which was still significantly different in comparison to baseline value (P<0.05) as shown in Fig. 1. Time (days) 15 30 45 60 75 90 105 120 0 % decrease in MASI score -5 -10 -15 * * ** * * * * * * -20 -25 * * * * gr A * * * -30 -35 * * * * gr B * * gr C gr D * * -40 Fig. 1: Effect of treatment with topical melatonin (group A), topical melatonin-sunscreen (group B), topical melatonin-oral melatonin (group C) and topical 4% hydroquinone cream (group D) on MASI score. = Significantly different with respect to baseline value, P<0.05. When the effects of the four strategies of treatments (A, B, C and D) were compared at the end of treatment period (90 days); patients in groups B, C and D demonstrated significant reduction in MASI score (31.11%, 28.4% and 37.23% respectively) in 4 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 comparison to that elicited by treatment with topical melatonin only, group A (13.83%) (P<0.05) as shown in Fig. 2.. MASI Score Moreover, no significant difference was noticed in the effect produced by treatment with topical melatonin-sunscreen (group B) or treatment with topical melatonin-oral melatonin (group C) on percent reduction in MASI score (P>0.05) as shown in Fig. 2. This figure also revealed that the effect of 4% hydroquinone cream was significant and potent in improving MASI score than therapy received by group B and C (P<0.05). In addition, hydroquinone is shown to be the least one exhibited a relapse phenomenon among all other therapies. 20 18 16 14 12 10 8 6 4 2 0 Baseline After 90 days 30 days placebo a group A b b group B group C c group D Figure 2. Effect of treatment with topical melatonin (A), topical melatonin-sunscreen (group B), topical melatonin-oral melatonin (group C) and topical 4% hydroquinone cream (group D) on MASI score. Data are expressed as mean ± SEM. Treatment with placebo starts after ending of 90 days of different treatment regimens. Non-identical superscripts (a, b, c) among different groups are consider significantly different, P<0.05. P<0.05 with respect to day 90. At the end of 90 days treatment, the results demonstrated highly significant reduction in MDA level in comparison to the baseline level (P<0.01) for group A, B, and C patients. While group D patients that treated with topical hydroquinone showed no significant reduction in the level of MDA during 90 days of treatment (P>0.05) as shown Fig. 3. However, stopping the four treatment regimens and continue treatment with placebo for 5 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 30 days strongly attenuated the effect produced by these four treatment regimens and less reduction in MDA was reported in all group which is not significantly different from the baseline level (P>0.05) as demonstrated in Fig. 3. When the effect of the four treatment regimens is compared at the end of day 90, significant differences in the level of MDA were reported in groups B, C and D (23.37%, 28.15% and 5.25% respectively) from that in group A (14.27%) (P<0.05). Moreover, MDA level in group C is highly reduced but not significantly different from that in group B as demonstrated in Fig. 4. Another oxidative stress marker measured is plasma GSH, after 90 days treatment, significant elevation in the level of GSH is reported when topical melatonin is given alone (group A), or with sunscreen (group B), or with oral melatonin (group C) in comparison to baseline level (P<0.05). Time (days) 45 90 120 % decrease in MDA level 5 0 -5 -10 * * -15 * * gr A -20 -25 -30 * gr B * gr C gr D Fig 3: Effect of treatment with topical melatonin (group A), topical melatonin-sunscreen (group B), topical melatonin-oral melatonin (group C) and topical 4% hydroquinone cream (group D) on the plasma MDA levels. * = Significantly different with respect to baseline value, P<0.05. 6 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 Baseline After 90 days 30 days placebo MDA level (umol/L) 3 2.5 c 2 a b b group B group C 1.5 1 0.5 0 Control group A group D Fig. 4. Effect of treatment with topical melatonin (A), topical melatonin-sunscreen (group B), topical melatonin-oral melatonin (group C) and 4% hydroquinone (group D) on the plasma MDA levels. Data are expressed as mean ± SEM. Treatment with placebo starts after ending of 90 days of different treatment regimens. Baseline values in all treatment groups were significantly different from control. Non-identical superscripts (a, b, c) among different groups are consider significantly different, P<0.05. P<0.05 with respect to day 90. Moreover, treatment with topical 4% hydroquinone cream (group D) showed not significant elevation in the level of GSH during 90 days of treatment (P>0.05) as presented Fig. 5. Again, stopping these four modes of treatment and continuing treatment with placebo for 30 days strongly abolished the previous effects elicited by these four regimens with the result of elevation in GSH levels, a value which not significantly different from the baseline levels (P>0.05) as shown in Fig. 5. When the effect of the four treatment regimens is compared at the end of day 90, significant difference in the level of GSH was reported only in group D (4.28%) which in comparison to that in group A (5.76%), group B (5.22%) and group C (5.38%) (P<0.05) as demonstrated in Fig. 6. 7 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 gr A % decrease in GSH level 7 gr B 6 gr C * * * 5 gr D 4 3 2 * 1 0 -1 45 90 120 Time (days) Fig. 5: Effect of treatment with topical melatonin (group A), topical melatonin-sunscreen (group B), topical melatonin-oral melatonin (group C) and 4% hydroquinone (group D) on the plasma GSH levels. * = Significantly different with respect to baseline value, P<0.05. Correlation analysis between MASI score with the level of both MDA and GSH revealed the followings: In group A, good and highly significant correlation was observed between the decreased MASI score with the decrease in MDA level (r=0.76, P<0.01) (Fig.7A). However, the decrease in MASI score correlated moderately but non-significantly with increased GSH level (r=0.58, P>0.05) (Fig. 7B). 8 GSH level (umol/L) Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 Baseline After 90 days 30 days placebo 0.3 0.28 0.26 0.24 0.22 0.2 0.18 0.16 0.14 0.12 0.1 0.08 0.06 0.04 0.02 0 a Control group A a a group B group C b group D Fig. 6. Effect of treatment with topical melatonin (A), topical melatonin-sunscreen (group B), topical-oral melatonin combination (group C) and 4% hydroquinone (group D) on the plasma GSH levels. Data are expressed as mean ± SEM. Treatment with placebo starts after ending of 90 days of different treatment regimens. Baseline values in all treatment groups were significantly different from control. Non-identical superscripts (a, b, c) among different groups are consider significantly different, P<0.05. P<0.05 with respect to day 90. In group B, the same profile of correlation is noticed as in group A, in that good and significant correlation existed between the decrease in MASI score with decreased MDA level (r=0.73, P<0.05)(Fig.8A). In addition, the decrease in MASI score showed moderate but not significant correlation with increased GSH level (r=0.49, P>0.1) (Fig. 8B). In group C, good and highly significant correlation is reported between decreased MASI score and the decrease in MDA level (r=0.78, P<0.01) (Fig.9A). In addition, the decreases in MASI score were very weakly and non-significantly correlated with the increase in GSH level (r=0.25, P>0.1) (Fig.9B). In group D, non significant correlation is reported between decreased MASI score and the decrease in MDA level (r=0.64, P>0.1) (Fig.10A). In addition, the decrease in MASI score correlated well but not significantly with the increase in GSH level (r=0.66, P>0.1) (Fig.10B). The present study investigated the effectiveness of using melatonin, a powerful antioxidant, topically alone and in combination with sunscreen and oral dose of melatonin in the treatment of melasma patients. The hormone, previously applied to the 9 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 preparations, effectively inhibited α-MSH darkening activity, and was also able to reverse alpha-melanocyte stimulating hormone (α-MSH)-induced darkening (Castrucci et al., 1997). Both cyclic guanosin monophosphate (cGMP) and melatonin blocked the stimulatory effects of cyclic adenosine triphosphate (cAMP) and α-MSH on melanin production but they left the levels of tyrosinase activity unaffected. 20 20 18 r = 0.76, P<0.01 16 16 14 14 MASI Score MASI Score 18 12 10 8 12 10 8 6 6 4 4 2 2 0 0 A0 r = 0.58, P>0.05 0.5 1 1.5 B 2 0 0.05 0.1 0.15 0.2 0.25 GSH (umole/L) MDA (umole/L) Fig. 7. A: Correlation between MASI score and MDA level, B: Correlation between MASI score and GSH level in group A patients. 18 18 16 r = 0.73, P<0.05 14 14 12 12 MASI Score MASI Score 16 10 8 6 10 8 6 4 A 4 2 2 0 0 0 0.5 1 MDA (umole/L) 1.5 r = 0.49, P>0.1 B 0 2 0.05 0.1 GSH (umole/L) 0.15 0.2 0.25 Fig. 8. A: Correlation between MASI scores and MDA level, B: Correlation between MASI score and GSH level in group B patients and MDA level in group B patient. 10 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 18 18 r = 0.78, P<0.01 14 16 12 14 10 12 MASI Score MASI Score 16 8 6 4 r = 0.25,P>0.1 10 8 6 4 2 2 0 0 0.5 1 MDA (umole/L) 1.5 0 2 0.16 0.165 0.17 0.175 0.18 GSH (umole/L) 0.185 0.19 0.195 0.2 B A Fig. 9 A: Correlation between MASI score and MDA level, B: Correlation between MASI score and GSH level in group C patient. 16 14 16 r = 0.64, P>0.1 14 r = 0.66,P>0.1 12 10 MASI Score MASI Score 12 8 6 4 10 8 6 4 2 2 0 1.8 1.9 2 MDA (umole/L) 2.1 0 0.155 2.2 0.16 0.165 GSH (umole/L) 0.17 0.175 0.18 B A Fig. 10 A: Correlation between MASI score and MDA level, B: Correlation between MASI score and GSH level in group D patient. Discussion It is suggested that whereas MSH stimulates melanogenesis through a cAMP-dependent mechanism, their must also be an inhibitory cGMP-dependent mechanism, perhaps activated by melatonin, which operates at some post-tyrosinase step in the melanin biosynthetic pathway ( Weatherhead & Logan 1981). But another study showed that 11 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 melatonin was found to have a small inhibitory effect on tyrosinase activity. Melatonin appeared to act at least at two stages. Pharmacological concentrations of melatonin diminished the number of α-MSH receptors to about 75% of the control values without an apparent effect on receptor affinity, and physiological concentrations of melatonin also appeared to interfere with the intracellular events coupling increased cAMP levels and induction of the tyrosinase (Valverde et al., 1995). Cyclic-AMP has been suggested to transduce the lightening effect of melatonin in frog skin melanophores, and the finding that MSH-induced cAMP increase is a sufficient signal for pigment dispersion and that decrease of cAMP induced by melatonin induce aggregation of melanin-containing granules in perinuclear zone, which result in blanching of the cell (White et al., 1987). Melatonin is now known to be a multifaceted free radicals scavenger and antioxidant. It detoxifies a variety of free radicals including superoxide, hydroxyl radical, peroxynitrite anion, singlet oxygen and nitric oxide (NO). Additionally, it effectively stimulates several antioxidant enzymes, including superoxide dismutase (SOD), glutathione peroxidase (GSH-Px), glutathione reductase (GSH-R) that metabolize active oxygen species to inactive products (Liu & Zheng 2003). When melanocytes synthesize and transfer melanin to the surrounding keratinocytes. Keratnocytes produce paracrine factors that affect melanocytes proliferation, dendricity, and melanin synthesis. The keratinocyte nitric oxide synthase (NOS) is involved in this process, and NO is secreted in response to UVA and UVB radiation, suggesting an important role of NO in UV-induced melanogenesis, and this effect is reversed by NO scavengers (Romero-Graillent et al., 1997). The inhibitory effect of melatonin on NOS may also contribute to its antioxidant capacity ( Pozo & Guerrero 1994). Addition of sunscreen to topical melatonin rapidly and significantly resulted in improving melasma score due possibly to combined action of these two agents in the protection of skin from UV radiation. It has been shown that irradiation of human keratinocytes or melanocytes with UV easy stimulates the synthesis and release of α-MSH and adrenocorticotrophin hormone (ACTH), which induce cAMP formation and increase the proliferation and melanogenesis of human melanocytes (Moro et al 1998). Sunscreen might decrease the effect of UV light on melanocytes and decrease the formation of free radicals induced by UV radiation (Patel & Moy 1992), and this might synergize the antioxidant activity of melatonin in a possible mechanism involving reduction and scavenging of UV-induced free radicals. The great percentage improvement of melasma resulted in the group that treated with combined topical and oral melatonin is strongly suggested that systemic action be predominant especially when the effect of topical melatonin only was compared to that of combined topical-oral regimen. This explanation is supported by the finding that the use of high doses of melatonin may increase its inhibitory effect on MSH and thus on melanogenesis (Valverde et al., 1995). This study indicates that melatonin powerfully reduced MDA level and elevated GSH level when given as topical-oral combination therapy. Melatonin approved to be restoring the amounts of tissue MDA and GSH back to about control levels (Ozacmak et al., 2005). 12 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 Treatment with topical hydroquinone cream demonstrated superior improvement in MASI score over all other treatment regimens. However, hydroquinone remains the most effective topically applied bleaching agent approved by the FDA. Although there is a correlations exist between the decreased MASI score and decreased MDA level, and between the decreased MASI score and increased GSH level, it failed to reach the level of statistical significance (P>0.1). This clearly demonstrated that hydroquinone improves MASI score and melasma by antioxidant unrelated mechanism and that only by inhibition of tyrosinase enzyme. REFERENCES 1. Balina, L. M.; Graupe, K. (1991) The treatment of melasma with 20% azelaic acid versus 4% hydroquinone cream. Int. J. Dermatol.; 30: 893-895. 2. Bleehen, S.S.; Ebling, F.J.G. and Champion, R.H.: Disorder of skin colour. In: Textbook of Dermatology (5th ed.), Champion, R.H.; Burton, J.L. and Ebling, F.J.G. (eds). Oxford, 1992; pp. 1561-1622. 3. Brzezinski, A.(1997) Melatonin in humans. N. Eng. J. Med. 336: 186-206. 4. Castrucci, A. M.; Almeida, A. L.; al-Obaidi, F. A.; Hadly, M. E.; Hruby, V. J.; Staples, D. J. and Sawyer, T. K. (1997) Comparative biological activities of alpha-MSH antagonists in vertebrate pigment cells. Gen. Comp. Endocrinol., 105 (30): 410-6. 5. Grimes, P. E. (1995) Melasma. Etiologic and therapeutic considerations. Arch. Dermatol., 131: 1453-7. 6. Guevara, I. L.; Pandya, A. G.(2001) Melasma treated with hydroquinone, tretinoin, and a fluorinated steroid. Int. J. Dermatol.; 20: 212-215. 7. Huh, C.H.; Seo, K.I.; Park, J.Y.; Lim, J.G.; Eun, H.C. and Park, K.C. (2003) A randomized double-blind, placebo-controlled trial of vitamin C iontophoresis in melasma. Dermatology; 206(4): 316-320. 8. Hurly, M. E.; Guevara, I. L.; Gonzales, R. M.; Pandya, A. G.(2002) Efficacy of glycolic acid peels in the treatment of melasma. Arch. Dermatol.; 138: 1578-1582. 9. Im, S.; Moro, O.; Peng, F.; Medrano, E. E.; Cornelins, J.; Babcock, G.; Nordlund, J. J. and Abdel-Malek, Z. A.(1998) Activation of the cyclic AMP pathway by alphamelanotropin mediates the response of human melanocytes to ultraviolet B radiation. Cancer Res. 1; 58 (1): 47-54. 10. Kimbrough-Green, C. K.; Griffiths, C. E.; Finkel, L. J.; Hamilton, T. A.; BulengoRansby, S. M.; Ellis, C. N. and Voorhees, J. J. (1994) Topical retinoic acid (tretinoin) for melasma in black patients. A vehicle-controlled clinical trial. Arch. Dermatol.; 130 (6): 722-733. 11. Liu, X.; Zhao, J. and Zheng, R.(2003) DNA damage of tumor-associated lymphocytes and total antioxidant capacity in cancerous patients. Nutal. Res.; 5(1-2): 1-8. 12. Ozacmak, V. H.; Sayan, H.; Arslan, S. O.; Altaner, S. and Aktas, R. G. (2005) Protective effect of melatonin on contractile activity and oxidative injury induced by ischemia and reperfusion of rat ileum. Life. Sci.; 76 (14); 1575-88. 13. Patel, N.P.; Highton, A. and Moy, R.L. (1992) Properties of topical sunscreen formulations. J. Dermatol. Surg. Oncol.; 18: 316. 13 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 14. Pathak, M. A. (1986) Clinical and therapeutic aspects of melasma: an overview. In: Brown Melanoderma. Fitzpatrick, T. B.; Wick, M. M.; Toda, K. (eds). Tokyo, Japan; pp. 161-171. 15. Pozo, D.; Reiter, R.J.; Calvo, J.A. and Guerrero, J.M. (1994) Physiological concentrations of melatonin inhibit nitric oxide synthase in rat cerebellum. Life Sci.; 55: 455-460. 16. Romero-Graillet, C.; Aberdam, E.; Clement, M.; Ortonne, J. P. and Ballotti, R. (1997) Nitric oxide produced by ultraviolet-irradiated keratinocytes stimulates melanogenesis. J. Clin. Invest.; 99 (4): 635-42. 17. Ryoo, Y.W.; Suh, S.I.; Mun, K.C.; Kim, B.C. and Lee, K.S. (2001) The effects of the melatonin on ultraviolet-B irradiation cultured dermal fibroblasts. J. Dermatol. Sci.; 27(3): 162-168. 18. Sanchez, N. P.; Pathak, M. A.; Sato, S.; Fitzpatrick, T. B.; Sanchez, J.L.; Mihm, M. C. Jr.: Melasma (1981) a clinical, light microscopic, ultrastructural, and immunofluorescence study. J. Am. Acad. Dermatol; 4: 698-710. 19. Sener, G.; Kacmaz, A.; User, Y.; Ozkan, S. and Tilki, M. (2003) Melatonin ameliorates oxidative organ damage induced by acute intra-abdominal compartment syndrome in rats. J. Pineal Res.; 35(3): 168-8. 20. Sivayathorn, A. (1995) Melasma in orientals. Clin. Drug Invest.; 10: 34-63. 21. Snell, R.S. and Bischitz, P.G. (1960) The effect of large amount of estrogen and progesterone on melanin pigment. J. Invest. Deramatol; 35: 73-87. 22. Valverde, P.; Benedito, E.; Solano, F.; Oaknin, S.; Lozano, J. A. and Garcia-Bor, J. C. (1995) Melatonin antagonizes alpha-melanocyte-stimulating hormone enhancement of melanogenesis in mouse melanoma cells by blocking the hormone-induced accumulation of the c locus tyrosinase. Eur. J. Biochem; 232 (1): 257-63. 23. Weatherhead, B. and Logan, A. (1981) Interaction of alpha-melanocyte-stimulation hormone, melatonin, cyclic AMP and cyclic GMP in the control of melanogenesis of hair follicle melanocyte in vitro. J. Endocrinol; 90 (1): 89-96. 24. White, B. h.; Sekura, R. D. and Rollag, M. D. (1987) Pertussis toxin blocks melatonin-induced pigment aggregation in xenopus dermal melanophores. J. Comp. Physiol. B. Biochem. Syst. Environ. Physiol; 157: 153-159. 14 Hamadi S. et al., Journal of Arab Universities for Basic and Applied Sciences, Vol.8, 2009, 30-42 تأثيرات الميالتونين موضعيا ً وعن طريق الفم في معالجة مرضى الكلف 1سليم حمادي 2,محمد محمود 3,اشواق الجاف 4 ,علي عبد الرزاق 1كلية الصيدلة والعلوم الطبية -جامعة البرا -عمان االردن 2,كلية الصيدلة-الجامعة المستنصرية -بغداد -العراق , كلية الصيدلة-جامعة بغداد -بغداد العراق و 4مستشفى الكرامة التعليمي -بغداد-عراق 3 الملخص صممت هذه الدراسة لتقييم التأثيرات الموضعية للميالتونين المحضر على شكل كريم باستعماله لوحده أو مع واقي للشمس أو مع الميالتونين عن طريق الفم في معالجة مرضى الكلف بالمقارنة مع الهيدروكوينون كعالج قياسي . أجريت الدراسة السر يريه التمهيدية بالطريقة العمياء المزدوجة على 36مريضا يعانون من الكلف و 10أشخاص أصحاء للمقارنة ،وقد تم اختيار وتشخيص المرضى في العيادة الخارجية لقسم األمراض الجلدية في مستشفى الكرامة العام وبإشراف مباشر من قبل اختصاصي الجلدية طيلة فترة الدراسة .تم تقسيم المرضى إلى أربعة مجاميع ،ثم عالج مرضى المجموعة األولى موضعيا" بالميالتونين المحضر ومرضى المجموعة الثانية بالميالتونين الموضعي باإلضافة إلى واقي للشمس ،أما مرضى المجموعة الثالثة فعولجوا موضعيا" بالميالتونين المحضر إضافة إلى الميالتونين عن طريق الفم ،وتم عالج مرضى المجموعة الرابعة بالهيدروكوينون الموضعي ،%4استمر العالج مدة 90يوم تبعتها 30يوم من العالج ) (Placeboالمموه .في نهاية فترة العالج ( 90يوم) أظهرت نتائج هذه الدراسة انخفاض ملحوظ في شدة المرض في جميع مرضى الكلف وبنسب متفاوته استنادا الى مقياس MASIوكذلك أظهرت النتائج انخفاض في مستوى المالوندايلديهايد ,وارتفاع في مستوى الكلوتاثايون بعد فترة الدراسة ,في كل المجاميع وبمستويات مختلفة. تقترح الدراسة الحالية إن إلعطاء مرضى الكلف مادة الميالتونين موضعيا أو عن طريق الفم تأثير ايجابي في العالج عن طريق تأثيره المانع لألكسدة أو عن طريق تأثيرات أخرى مختلفة غير متعلقة بتأثيره المانع لألكسدة. 15