COTM1013 - California Tumor Tissue Registry
advertisement

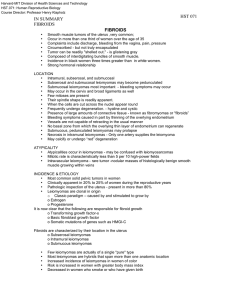
“A 59 year-old Woman With a Painful Leg Nodule” California Tumor Tissue Registry’s Case of the Month CTTR COTM Vol. 16:1 October, 2013 www.cttr.org A 59-year-old healthy woman presented with a solitary painful pink nodule on her right anterior leg. The 1.0 x 0.7 cm nodule had persisted, unchanged, for the last 4 years. An excisional biopsy was performed for symptomatic relief. Microscopically, the tumor was a dermal-based proliferation with a distinct grenz zone, overlying acanthosis, and no obvious connection to the epidermis (Figs. 1, 2a, 2b). It was comprised of fascicles of spindle cells with ample eosinophilic cytoplasm haphazardly intersecting and surrounding nearby adnexal structures, including a hair follicle (Figs. 2a, 2b, 2c). Nonencapsulated and poorly circumscribed, the packets of spindle cells interdigitated with the adjacent normal reticular dermis (Fig. 3). Upon closer inspection, the spindle cells had cigar-shaped, blunt-ended nuclei and were interwoven with bundles of bright red collagen (Figs. 4a, 4b). The tumor cells showed no significant pleomorphism, mitotic activity, nor necrosis. Immunohistochemistry showed positively for desmin and actin. Diagnosis: Leiomyoma of pilar arrector origin Elif L. Akin, M.D. and Donald R. Chase, M. D. Department of Pathology & Human Anatomy Loma Linda University Medical Center, Loma Linda, California Cutaneous leiomyomas were first described in the early 1800s as “painful subcutaneous tubercles” or “tuberculosum dolorosum”. Today, they are usually designated as “leiomyoma of pilar arrector origin” (LPAO) and are clinically grouped with several other cutaneous tumors that may present with localized pain. LPAO is a relatively uncommon lesion that usually occurs on the extensor surfaces or trunk of young adults, with no predilection for gender. Lesions often manifest as multiple, slow-growing, small pink papules. Occasionally, they may follow a dermatomal distribution or coalesce into plaques. Clinically, LPAO is associated with pain (occurring either spontaneously or with applied pressure), sensitivity to cool temperatures, and/or pruritus. These symptoms are thought to be related to either nerve compression or muscle contraction. Of interest, Fisher & Helwig described three patients in 1963 who experienced lesional pain that was apparently elicited by strong emotions. CTTR’s COTM October 2013 Page 1 As it arises from the arrector pili muscle, LPAO is comprised of packets and bundles of smooth muscle cells intersecting in a chaotic, haphazard arrangement. The tumor usually has a clear grenz zone, does not involve the epidermis, but may have overlying epidermal hyperplasia. The smooth muscle cells have ample eosinophilic cytoplasm and cigarshaped or vesicular nuclei. While there may be focal areas of mild atypia related to degenerative changes, significant nuclear pleomorphism, mitotic activity, and necrosis are not typically present. LPAO is usually poorly circumscribed, merging into the surrounding tissue, and is often found near a hair follicle. The mainstay therapy for LPAO is surgical excision and pain management. Even though this is regarded as a benign neoplasm with no potential for malignant transformation, complete surgical excision can be challenging in patients presenting with multiple lesions; otherwise, surgery is usually curative. Alternative therapies including laser ablation and cryotherapy have also been employed. Recently, a small number of patients presenting with multiple cutaneous leiomyomas of pilar arrector origin have been found to have an autosomal dominant syndrome called “multiple cutaneous and uterine leiomyomatosis” (MCUL, aka Reed syndrome), which predisposes women to the early development of uterine leiomyomas. Interestingly, a small subset of patients and families with MCUL also has associated papillary or collecting duct renal cell carcinoma, a condition known as hereditary leiomyomatosis and renal cell cancer (HLRCC). Both MCUL and HLRCC have been linked to a germline loss-of-function mutation of the fumarate hydratase (FH) gene. This gene encodes an enzyme in the Krebs cycle, which normally functions as a tumor suppressor. Alam et al. have concluded that most patients with cutaneous leiomyomas have an underlying FH mutation. This renders the early identification and correct diagnosis of LPAO quite clinically significant, as it may prompt additional work-up for other conditions such as uterine fibroids and/or renal cancer. The differential diagnosis includes a variety of benign and malignant fibrohistiocytic and smooth muscle tumors: Cutaneous fibrous histiocytoma (dermatofibroma) may also demonstrate a haphazard arrangement of cells. Inflammatory cells, giant cells, and xanthoma cells may also be seen, however, they are absent in LPAO. Smooth muscle hamartoma is also comprised of smooth muscle bundles; however, it tends to occur as a single, larger lesion presenting in the lower back of children or young adults and may also be associated with Becker’s nevus. Genital leiomyoma is a more common type of cutaneous leiomyoma, which occurs on the nipple, scrotum, or vulva. Unlike LPAO, it tends to demonstrate increased cellularity and is usually well circumscribed. CTTR’s COTM October 2013 Page 2 Angioleiomyoma usually occurs in females, most often in the lower leg. It is a deeper lesion than LPAO, arising in the superficial subcutis. The smooth muscle cells in an angioleiomyoma surround numerous thick-walled vessels. LPAO, in contrast, does not have prominent vasculature. Leiomyosarcoma usually demonstrates significant nuclear pleomorphism and mitotic activity, features that are, by definition, not associated with LPAO. In summary, leiomyoma of pilar arrector origin is an uncommon benign neoplasm that usually occurs on the extensor surfaces of young adults. While it may occur as a solitary lesion, patients usually present with multiple pink sub-centimeter painful papules/nodules. Surgical excision is typically curative. Correct diagnosis of this lesion is important because it may be a presenting feature of multiple cutaneous and uterine leiomyomatosis and/or hereditary leiomyomatosis and/or renal cell cancer, two hereditary conditions which are associated with germline mutations in the fumarate hydratase gene. Early recognition of these cutaneous leiomyomas can help ensure that patients receive appropriate gynecologic and genitourinary evaluation. Suggested Reading: Alam NA, Olpin S, Leigh IM. Fumarate hydratase mutations and the predisposition to cutaneous leiomyomas, uterine leiomyomas and renal cancer. Br J Dermatol. 2005; 153: 11-17. Calonji E, Brenn T, Lazar A, McKee PH. McKee’s Pathology of the Skin with Clinical Correlations: 4th ed. Elsevier Saunders. 2011; 2: 1696-1697. Chronic unilateral eruption of painful, erythematous papules and nodules. JAMA Dermatol. 2013; ():2. doi:10.1001/jamadermatol.2013.3358a. Fisher WC, Helwig EB. Leiomyomas of the skin. Arch Dermatol. 1963; 88: 510-520. Fletcher CD. Diagnostic Histopathology of Tumors: 3rd ed. Churchill Livingstone Elsevier. 2007: 1562-1563. Stout AP. Solitary cutaneous and subcutaneous leiomyoma. Am J Cancer. 1937; 29: 435469. Weiss S, Goldblum J. Enzinger & Weiss’s Soft Tissue Tumors: 5th ed. Mosby/Elsevier Inc: Philadelphia. 2008: 518-520. CTTR’s COTM October 2013 Page 3