Male and Female Urethral Catheterisation
advertisement

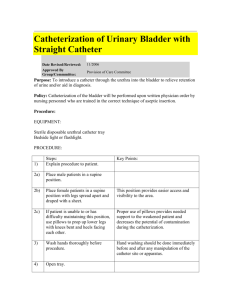
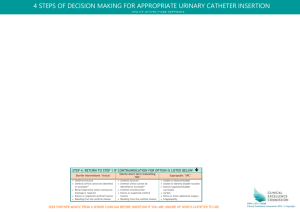
Male and Female Urethral Catheterisation What is it? Catheterisation is the aseptic insertion of a sterile tube (catheter) into the urinary bladder for the purpose of instilling or draining fluid. Catheters are usually inserted urethrally however if this is not possible due to blockage or for reasons of patient choice the suprapubic route may be used. In this case the catheter is inserted through the abdomen and into the bladder. Why are they used? To empty the bladder prior to surgery. To monitor renal function post-operatively. To drain the bladder in urine retention. To monitor renal function in critically ill patients. To instill fluid, irrigation or cytotoxic drugs. To perform bladder function tests. As a last resort for incontinence if all other methods fail. What are the main risks? Insertion of a urinary catheter carries a high risk of infection and should only be used if considered to be clinically essential. Insertion can also cause bruising and trauma to the urethral mucosa which then acts as entry points for micro-organisms into the blood and lymphatic system. Scar tissue is also easily formed as a result of trauma. Further Information Further information is available from: NHS Quality Improvement Scotland (2004) Best Practice Statement. Urinary Catheterisation and Catheter Care. www.nhshealthquality.org Pratt RJ et al (2007) epic2: National Evidence-Based Guidelines for Preventing Healthcare-Associated Infections in NHS Hospitals in England. Journal of Hospital Infection February 65S:S1-S64 Please ensure you refer to local policy before undertaking any procedure Please ensure you refer to local policy before undertaking any procedure Flow chart to aid assessment of patient need for catheterisation Have all alternative methods of management been considered? YES NO – do not catheterise Can you justify the reason for this clinically invasive procedure? NO – do not catheterise YES Why does the patient require a catheter? To empty the bladder prior to surgery or investigations Doctor/MDT Specialist to document justification To allow irrigation of the bladder Doctor/MDT Specialist to document justification To introduce cytotoxic drugs Doctor/MDT Specialist to document justification To enable bladder function tests to be performed Doctor/MDT Specialist to document justification To measure urinary output accurately e.g. patient in shock Doctor/Outreach to document justification Incontinence affecting wound healing Doctor/Tissue Viability Specialist to document justification To relieve incontinence Refer to continence advisor for continence assessment To determine residual urine Use a bladder scanner (residual above 500ml - catheterise) To bypass an obstruction flow e.g. constipation Use a bladder scanner (residual above 500ml - catheterise) To relieve retention of urine Use a bladder scanner (residual above 500ml - catheterise) Please ensure you refer to local policy before undertaking any procedure Catheterised patients should be reviewed regularly and the catheter removed as soon as possible Chart to aid choice of catheter Patient preference should be considered and consent is essential What is the catheter required for 1st choice = intermittent catheter To empty the bladder once – intermittent catheter Bladder emptying is incomplete but can store urine – intermittent catheter Urethral strictures – intermittent catheter Bladder substitution – intermittent catheter Intermittent catheterisation unsuitable – urethral catheter Continuous irrigation – urethral catheter Continuous urine measurement – urethral catheter Incontinence all alternatives explored – urethral catheter Residual above 500ml due to retention or obstruction – urethral catheter Urethral catheterisation not possible – supra-pubic catheter Intractable bypassing of long term urethral catheter - supra-pubic catheter How long is it needed for? To empty the bladder once – intermittent catheter 1 day to 4 weeks – use PTFE 4 weeks to 12 weeks – use Hydrogel Continuous irrigation – Silicone 3 way catheter If the patient is allergic to latex use a silicone catheter Alternatives to catheterisation for incontinence Potential complications of catheterisation Trauma Continence assessment Urinary tract infection Pelvic floor exercises Stricture formation Regular toileting Urethral perforation ConvenePlease ensure you refer to local policy before undertaking any procedure Encrustation Bladder calculi Fluid intake advice Neoplastic changes Please ensure you refer to local policy before undertaking any procedure Types of Catheter PTFE - 4 weeks SILICONE - 12 weeks HYDROGEL – 12 weeks INTERMITTENT Please ensure you refer to local policy before undertaking any procedure Catheter Care Bundle Please ensure you refer to local policy before undertaking any procedure Ongoing Care Please ensure you refer to local policy before undertaking any procedure Please ensure you refer to local policy before undertaking any procedure Name…………………………………… WMS No……………………….. T- DOCS: Male Urethral Catheterisation Please insert a urethral urinary catheter into this patient’s bladder. Washes Hands Understands indications & anatomy Obtains informed consent Explanation to patient, often including complications Communication skills Appropriate preparation Appropriate analgesia Technical ability especially with any special equipment and sharps Aseptic technique Seeks help as appropriate Post procedure management Professionalism Overall ability to perform procedure Hand wash with water and soap using the Ayliffe technique. Urinary retention/ pre-op/ critically unwell Aware of different positioning and angles that may be required to pass catheter through urethra. Aware of length of urethra and position of prostate Introduce themselves. Gains informed consent. Clear explanation of procedure, e.g. “I am going to pass a tube into your bladder, it will go into the bladder via the urethra which is the tube in your penis that allows urine to drain from your bladder”. Chaperone Assessment throughout the procedure and allows patient to ask questions. Cleans trolley correctly, places equipment on bottom shelf Selection of equipment: trolley, appropriate catheter type and size, instillagel 11mls, sterile gloves x 2 pairs, apron, alcohol rub, 10ml syringe, catheter bag, sterile water 10ml, Normasol, waste bag, sterile gauze and catheterisation pack Prepares patient and maintains privacy and dignity Ensures use of 11ml instillagel for men, aware the gel may cause stinging sensation on initial administration. Use aseptic technique throughout. Applies sterile gloves retracts the foreskin and cleans shaft, glans and urethral meatus using Normasol solution. Arranges sterile drape, administers instillagel 11mls, maintain penile position upright and meatus closed for 3 to 5 minutes to allow instillagel to take effect. Washes hands and applies new pair of gloves, opens catheter, slowly inserts catheter smoothly until urine begins to drain and then passes catheter up to bifurcation point. Attaches bag and inflates balloon. Repositions foreskin Cleaning of trolley, placing of equipment on bottom shelf, opening packets correctly and aseptic technique throughout. Reasons for failure to catheterise: e.g. stricture, spasm Discusses complications e.g. haematuria, paraphimosis Discusses what to do if no urine drains Waste disposal Explain that instillagel will take an hour to wear off Documents time, date, clinical reason, aseptic technique, instillagel, catheter size, type and expiry date, any problems, amount of urine drained and colour. Communicate to team members Thanks staff Thanks patient and ensures they are dry and comfortable. Assess globally, would you be happy for this student to be supervised to insert a catheter on a real patient? Overall Grade BE B S AE Please ensure you refer to local policy before undertaking any procedure T-DOCS: For Medical Students Clinical Skill ……………………………….. Name of Student Areas of good practice 1. 2. 3. Areas for improvement 1. 2. 3. Below Expectation Skills labs Supervised Global assessment: Borderline Satisfactory Skills labs Unsupervised Job Title Name Please print: Patient Safe Supervised Assessor signature: Date Above Expectation Teaching Potential Signature How suitable do you think this assessment is for undergraduate medical students? Not Suitable Highly Suitable 1 □ □ □ □ □ □ □ □ □ □ 2 3 4 5 6 7 8 9 Any other Comments: Free text please use! 10 Please ensure you refer to local policy before undertaking any procedure Name……………………………………………………….WMS No……………………….. T-DOCS: Female Urethral Catheterisation Please insert a urethral urinary catheter into this patient’s bladder. Washes Hands Understands indications & anatomy Obtains informed consent Explanation to patient, often including complications Communication skills Appropriate preparation Appropriate analgesia Technical ability especially with any special equipment and sharps Aseptic technique Seeks help as appropriate Post procedure management Professionalism Overall ability to perform procedure Hand wash with water and soap, alcohol gel alone not sufficient for aseptic technique. Urinary retention/ pre-op/ critically unwell Aware of different positioning and angles that may be required to pass catheter through urethra. Aware of length of urethra Introduces themselves. Gains informed consent. Clear explanation of procedure, e.g. “I am going to pass a tube into your bladder, it will go into the bladder via the urethra to allow the urine to drain out”. Chaperone Assessment throughout the procedure and allows patient to ask questions. Cleans trolley correctly, places equipment on bottom shelf Selection of equipment: trolley, appropriate catheter type and size, instillagel 6mls, sterile gloves x 2 pairs, apron, alcohol rub, 10ml syringe, catheter bag, sterile water 10ml, Normasol, waste bag, sterile gauze and catheterisation pack Prepares patient and maintains privacy and dignity Ensures use of 6ml instillagel for women, aware the gel may cause stinging sensation on initial administration. Use aseptic technique throughout. Applies sterile gloves separates labia and cleans urethral orifice using Normasol solution. Arranges sterile drape, administers instillagel 6mls, waits for 3 to 5 minutes to allow instillagel to take effect. Washes hands and applies new pair of gloves, opens catheter, slowly inserts catheter smoothly until urine begins to drain and then passes catheter up to bifurcation point. Attaches bag and inflates balloon. Cleaning of trolley, placing of equipment on bottom shelf, opening packets correctly and aseptic technique throughout. Reasons for failure to catheterise: e.g. stricture, spasm Discusses complications e.g. haematuria Discusses what to do if no urine drains Waste disposal Explain that instillagel will take an hour to wear off Documents time, date, clinical reason, aseptic technique, instillagel, catheter size, type and expiry date, any problems, amount of urine drained and colour. Communicate to team members Thanks staff Thanks patient and ensures they are dry and comfortable. Assess globally, would you be happy for this student to be supervised to insert a catheter on a real patient? Overall Grade BE B S AE Please ensure you refer to local policy before undertaking any procedure T-DOCS: For Medical Students Clinical Skill ……………………………….. Name of Student Areas of good practice 1. 2. 3. Areas for improvement 1. 2. 3. Below Expectation Skills labs Supervised Global assessment: Borderline Satisfactory Skills labs Unsupervised Job Title Name Please print: Patient Safe Supervised Assessor signature: Date Above Expectation Teaching Potential Signature How suitable do you think this assessment is for undergraduate medical students? Not Suitable Highly Suitable 1 □ □ □ □ □ □ □ □ □ □ 2 3 4 5 6 7 8 9 Any other Comments: Free text please use! 10 Please ensure you refer to local policy before undertaking any procedure