Service Change Proposal Proforma
advertisement

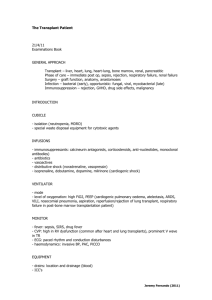
Service Change Proposal Proforma 1. Title of Proposal Proposed Transfer of Cadaveric Renal Transplantation for North of Scotland Patients from Aberdeen Royal Infirmary to Edinburgh Royal Infirmary. 2. Originator Dr Nick Fluck, Head of Service for Renal Services 3. Sponsor Dr Roelf Dijkhuizen, Medical Director 4. Background 4.1 Outline of the Service Currently Provided Aberdeen Royal Infirmary currently offers cadaveric renal transplantation to the end stage renal failure population in the North of Scotland. This includes patients from NHS Grampian, Orkney, Shetland and Highland. With the imminent retirement of the lead transplant surgeon at Aberdeen Royal Infirmary (transplant surgeon will cease to undertake cadaveric renal transplants at Aberdeen Royal Infirmary in December 2003) it is recognised that the cadaveric renal transplant program can no longer be provided locally. The reasons for this are outlined in section 4.4 - key drivers for change. Grampian patients considered for live related and unrelated renal transplantation are initially evaluation in Aberdeen but are then referred to Edinburgh for full assessment and subsequent transplantation. 4.2 Description of the Proposal This paper sets out a proposed framework for providing a comprehensive renal transplantation service outwith the Aberdeen Royal Infirmary. The current favoured option would be to integrate services with the Edinburgh Royal Infirmary Transplant unit. 4.3 Activity Year Total 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 33 19 23 35 21 21 11 31 20 14 15 11 Cadaveric Transplants Grampian Patients in ARI Inverness Patients in ARI 29 17 19 29 15 18 5 18 13 6 4 6 4 2 4 6 6 3 6 9 5 5 5 1 Live Transplants Grampian Patient in Edinburgh Grampian Patients in Edinburgh 0 0 0 0 0 0 0 0 0 0 1 2 0 0 0 0 0 0 0 4 2 3 5 2 40 35 30 25 T ot al Gr ampi an P at i ent s i n A RI 20 I nver ness P at i ent s i n A RI Gr ampi an P at i ent i n E di nbur gh Gr ampi an P at i ent s i n E di nbur gh 15 10 5 0 1990 1992 1994 1996 1998 2000 2002 2004 For service planning purposes a figure of 10 NHS Grampian and 5 NHS Highland cadaveric transplants per annum has been used. 4.4 Key Drivers for Change reducing number of cadaveric transplants being undertaken each year at Aberdeen Royal Infirmary due to national shortage of cadaveric donors. This is set against a requirement for renal transplant surgeons to undertake a critical mass of cases to maintain clinical skills and expertise. National shortage of renal transplant surgeons Retirement of renal transplant surgeon at Aberdeen Royal Infirmary in December 2003. Requirement to make an urgent decision about the future planning of the cadaveric renal transplant service for NHS Grampian patients. Arrangements need to be put in place in advance of the renal transplant surgeon at Aberdeen Royal Infirmary retiring in December 2003. This will allow Grampian patients to be assessed by a new renal transplant team. 5. Aims and Objectives The reasons for this service change are outlined in section 4.4 - key drivers for change. Aim is to provide a proposed framework for providing a comprehensive renal transplantation service outwith the Aberdeen Royal Infirmary 6. Link to strategy Proposed strategy fits in with national guidance that renal transplant centres need to undertake a critical mass of cases to maintain clinical skills and expertise. 7. Public Consultation and Involvement Appendix One provides an overview of the process undertaken by NHS Grampian for public consultation and involvement. It provides a summary of the feedback received from members of the public in response to the proposed service change. 8. Timescales Immediate decision required by NHS Grampian. There is an urgent requirement to put in place arrangements to transfer the cadaveric renal transplant service for Grampian patients from Aberdeen Royal Infirmary to Edinburgh Royal Infirmary in advance of the renal transplant surgeon’s retiral date (December 2003). 9. Indicative Cost (estimated) Enclosed below is a broad indication of the likely cost of transferring cadaveric transplant services from Aberdeen Royal Infirmary to Edinburgh Royal Infirmary. RENAL TRANSPLANTATION - TRANSFER TO LOTHIAN Note Pre Transplant Assessment Clinics Consultant (i) Transplant Co-ordinator (ii) Clinic Support Patient Transport (iii) £'000 14 36 10 4 Transplantation Cost of procedures at LUHT 15 cases @ £32k per case Patient Transport Backfill for SpR (iv) (v) (vi) 480 6 16 Post Transplant Patient Transport to ARI (v) 4 570 (i) Assumed one session for pre dialysis and transplantation (ii) If assessment indicates that co-ordinator is required then discussion to be held with NSD central funding. (iii) Cost for Grampian patients travelling to ARI Clinic for tx assessment (iv) Cost for assumed 10 Grampian and 5 Highland cadaver transplant patients Highland will reduce contract with GUHT accordingly. Excludes costs of live transplant patients as all currently undertaken in Lothian. (v) Grampian patients only (vi) Assumes SpR's required to rotate to Edinburgh for transplantation experience And locum brought in to backfill. 10. Risk Assessment Delay in assessing Grampian patients for renal cadaveric transplants if an agreement has not been reached to transfer the service to Edinburgh Royal Infirmary. The opportunity cost would be NHS Grampian patients missing out on a cadaveric renal transplant, which is qualitatively better for the patient and far more cost effective than maintaining patients on hospital haemodialysis National shortage of renal transplant surgeons – High likelyhood that NHS Grampian would be unable to attract a suitably trained renal transplant surgeon due to limited number of cadaveric transplants being undertaken locally and the lack of a live related and unrelated renal transplantation service in the North of Scotland. The cost of maintaining a renal cadaveric transplant service in Grampian would be significant in comparison to transferring the service to Edinburgh Royal Infirmary where economies of scale around fixed costs will be far greater. 11. Workforce/Staff Development Pre-Transplant Assessment Clinic - Patients will reach this clinic through direct referral from their specific renal consultant. This should follow a defined structured format with reference to unit-based protocols. The clinic will offer recipient assessment for all forms of renal transplantation (cadaveric, living donor and kidney/pancreas). Potential living donors will also be evaluated. Re-assessment of patients already on the transplant waiting list would be carried out in this clinic. The clinic will be based in the Aberdeen Royal Infirmary and would be staffed by transplant surgeons from the Edinburgh transplant unit together with an Aberdeen based recipient renal transplant co-ordinator. Additional supporting clinic staff would also be required. A similar clinic based in Dundee manages to assess around 5-6 patients per session (Typical case mix, 1 potential Living donor/recipient pair, 2 new patients and 2-3 listed follow-up patients). This requires 2 transplant surgeons from the base unit and 1 transplant co-ordinator from the local unit. The current demand from the Aberdeen patient population would support a clinic every 2 weeks. Re-evaluation of currently wait-listed patients before transfer to the Edinburgh list would require a more intense clinic schedule, perhaps weekly. Information Management - It is vital that up to date comprehensive patient information is available to the Edinburgh transplant team. Co-ordination of data should be managed by the Aberdeen recipient transplant co-ordinator in collaboration with their Edinburgh counterparts. Investment in IT infrastructure may be required to make existing database system fit for purpose. Transplantation and post operative care - following transplantation patients will be cared for in the Edinburgh unit until fit for in patient transfer back to the Aberdeen Renal Unit. This would usually be no earlier than post op day 5 and most often between 1 and 2 weeks after surgery. Once in Aberdeen post op surgical problems will all be initially discussed with the Edinburgh transplant surgeons and the patient returned if required. If urgent intervention is required precluding transfer then designated support needs to be arranged with a group of local surgeons, most probably a subset of the vascular team. Biopsy decisions and treatment of acute rejection will be handled by the Aberdeen renal team with histology assessed by the local renal pathology team. SpR Support to Renal Service delivery within ARI - the transfer of renal transplantation away from Aberdeen Royal Infirmary will impact on current and future Nephrology Specialist Registrar experience. There are currently 3 SpR posts and 1 lecturer position with SpR status. It is likely that each trainee will need to spend at least 2 months in the Edinburgh Royal Infirmary transplant unit during the latter phase of their training. This will have significant direct costs and indirect ones relating to support of the renal service in Aberdeen Royal Infirmary. These are included in section 8 – indicative costs. Renal Transplant Outpatient care - All post transplant outpatient follow up would remain in the current Aberdeen transplant clinics. Specific late surgical issues relating to the transplant will be initially discussed with the Edinburgh transplant team. 12. Option Appraisal Option 1 - Transfer Cadaveric Renal Transplant Service from Aberdeen Royal Infirmary to Edinburgh Royal Infirmary. Option 2 - Maintain Cadaveric Renal Transplant Service at Aberdeen Royal Infirmary Section 10 - Risk Assessment, sets out why option 1 is the preferred option. Option two is not clinically viable due to the imminent retirement of the renal transplant surgeon at Aberdeen Royal Infirmary, the national shortage of renal transplant surgeons and the requirement for renal transplant surgeons to undertake a critical mass of cases to maintain clinical skills and expertise. Appendix One Public Consultation and Involvement Introduction NHS Grampian is committed to underpinning any service change with the principles and values of Patient Focus and Public Involvement (PFPI). A public involvement plan was prepared to support this proposal, as follows: Stage 1 informing all stakeholders of the current and impending position, and what NHS Grampian believes is the best way forward and why engaging with them, offering the opportunity to give their views and suggestions on the proposed way forward responding to the above, plus any queries or particular concerns feeding in all contributions to the NHS Board feeding back the final proposal, the views and decision of the Board Stage 2 working in partnership with renal patients and their families to design the future service ongoing dialogue with patients and families, as part of continual learning and improving of all services Process A consultation paper, with covering letter, was sent to the following stakeholders: Shetland, Orkney and Highland NHS Boards for distribution to their staff, MSPs, Health Council, GPs, interest groups etc Patients on the ARI renal transplant waiting list (individual letters) Grampian GPs Grampian Local Health Council Grampian MSPs and MPs National and local interest organisations (Grampian Kidney Patients Association, Scottish Federation of Kidney Patients Associations, National Kidney Federation, UK Transplant) A news release was sent to all NE media outlets, and placed on the NHS Grampian intranet for staff. A public notice was placed in the Press and Journal. Consultation Views were sought on the proposal that: NHS Grampian enter into discussions with NHS Lothian on extending the already-established arrangement with the Edinburgh Transplant Unit to provide all kidney transplant operations for patients from Grampian, Orkney and Shetland. the Aberdeen renal team works with patients, families, and other interested groups to design the future service, so that we best meet the needs of local patients, including practical arrangements and follow-up. Consultees were asked: what do you believe to be the best way forward? do you agree that NHS Grampian should discuss extending the current arrangement with the Edinburgh Transplant Unit? do you have any particular suggestions, views or issues? We acknowledged all contributions, and responded to specific queries and requests for clarification. Responses A total of 17 responses have been received, from: 7 members of the public, patients and relatives 1 Grampian GP 3 Grampian MSPs 1 Grampian Local Health Council Grampian Kidney Patients Association (GKPA) Orkney Kidney Patients Association (OKPA) Scottish Federation of Kidney Patients Associations National Kidney Federation UK Transplant All responses are available in full for Board Members. 1. Patients/relatives/members of public Main views Disappointment at the scarcity of suitable donor organs, and the need for stronger efforts to encourage people to be donors. The dramatic improvement in quality of life that patients experience after receiving a new kidney. Aberdeen is most convenient, but reluctant acceptance of the present situation, and that ‘centres of excellence’ do make sense. Importance of maximising pre- and post care in the familiar surroundings and staff at ARI. Support of family is vital during this time (and for family to support each other). Praise for the Aberdeen team from those who had received kidneys at ARI. Praise for the Edinburgh service from a patient who had received kidney there (living donation). Issues Strain on patient’s family, and difficulty of supporting each other at a distance. Financial cost of partner’s travel and accommodation in Edinburgh, and childcare arrangements. Not knowing the Edinburgh staff, and being in unfamiliar surroundings. Might follow-up at ARI also disappear in time? Logistical problems, will there be sufficient time to get down to Edinburgh so that a kidney is not wasted? The disappointment of travelling to Edinburgh, to discover - at the last moment - that the kidney is unsuitable. Suggestions Aberdeen could concentrate its resources on vital aftercare. An Edinburgh surgeon could travel to Aberdeen regularly to meet patients and possibly also do transplants. An offer from Grampian Local Health Council to work with patients to design the new service. 2. Responses from MSPs All three MSPs are supportive of the proposal, while also raising issues relevant to their constituents (including transport, accommodation and followup), and a number of queries which have been responded to. 3. Responses from organisations and interest groups Grampian Kidney Patients Association circulated a questionnaire to its members and submitted a collation of individual responses. There was a 5:1 ratio in favouring of retaining service in Aberdeen. Ease of access for family was the main reason. Main issue with Edinburgh was time and cost of travel and accommodation. Also concern that renal services at ARI could be downgraded if transplant service moves. Orkney Kidney Patients Association supports the proposal, acknowledging the superb previous service at ARI, while realising that the decline in transplant numbers means that surgical standards cannot be maintained. OKPA also raises issues relating to transport, inpatient care and follow-up for Orkney patients. Grampian Local Health Council supports the proposal, welcomes the active involvement of patients in developing the new service, and offers to assist with this. The Health Council raises the issue of arrangements for family members, and the costs of transport and accommodation. The Scottish Federation of Kidney Patient Associations concurs with the proposal, while raising the issue of accommodation for next-of-kin and the importance of their support in the recovery process. The National Kidney Federation supports the general philosophy of trying to keep transplant units open, and is pressing for an increase in the number of surgeons and medical staff to ensure that these units remain operating. UK Transplant supports the proposal to transfer the service from Aberdeen to Edinburgh, citing national standards that transplant units should generally serve a population of at least two million.