a predictor of more severe growth impairment in achondroplasia
advertisement

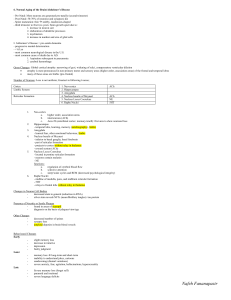
Oral vascular network pattern abnormalities in the unaffected parents of children with achondroplasia CLAUDIO DE FELICE1* , GIORGIO BIANCIARDI3*, STEFANO PARRINI4, PETER SHERIDAN DODDS7, KENNETH SHIRRIFF8, GIOVANNI DI MAGGIO2, RICARDO N. LAURINI9, AND GIUSEPPE LATINI5,6 …………………………………………………………………………………………… 1 Neonatal Intensive Care Unit, Section of Preventive Paediatrics and Neonatology and 2Section of Paediatric Surgery, Department of Paediatrics, Obstetrics and Reproductive Medicine, Siena, Italy 3 Institute of Pathological Anatomy and Histology, Siena, Italy 4 Department of Odontostomatological Sciences, Siena, Italy 5 Division of Paediatrics, Perrino Hospital, Azienda Ospedaliera A. Di Summa, Brindisi, Italy 6 Clinical Physiology Institute (IFC-CNR), National Research Council of Italy, Lecce Section, Italy 7 Department of Earth Sciences, Columbia University, New York, USA 8 (……….)Berkeley (?), California, USA 9 Department of Obstetrics and Gynaecology, University Hospital San Joao, Porto, Portugal * These authors contributed equally to the work Correspondence should be addressed to C.D.F.; email: defelice.claudio@libero.it 2 ABSTRACT Achondroplasia (ACH) (OMIM 100800), the most frequent form of skeletal dysplasia in humans1, is usually associated with a missense mutation resulting in a Gly 380Arg (G380R) amino acid change in the transmembrane domain of the fibroblast growth factor receptor-3 (FGFR3) gene2, and is transmitted as an autosomal dominant disorder. However, approximately 90% of the ACH cases are sporadic as the result of a de novo mutation3, and no phenotypical markers for the unaffected ACH parents are known. An abnormal vascularization in ACH patients4 and ACH animal models5,6 has been previously reported. The 2-D vascular network geometry of the venous plexus of the oral mucosa was analysed in a reproducible manner in the unaffected parents of ACH children. The ACH parents showed significantly higher network density, fractal dimension, and minimum-path dimension and significantly lower vessel-free area size compared to controls. Density and vessel-free area size were highly accurate in identifying subjects with an ACH offspring (97.1 to 100% sensitivity, 100% specificity). The findings indicate the presence of a previously unrecognised, vascular network abnormality of the oral mucosa in the unaffected parents of children with ACH, and provide a useful clinical marker for identifying couples potentially at risk for ACH offspring. 3 RESULTS The oral vascular network patterns of the unaffected ACH parents appeared to be significantly more complex than those of control parents (Fig. 1), in the absence of other macroscopical differences. The ACH children and the unaffected ACH parents showed significantly higher vascular density, D(1-46),D (1-15)and Dmin, together with a lower vessel-free area size than age- and sex-matched controls (Table 1). In particular, vascular density in the ACH parents was 1.81 0.14 times higher and vessel-free area size was 3.33 0.069 times lower than that of control parents. No statistically significant differences in the examined vascular pattern characteristics between the vascular networks of the unaffected ACH parents and those of the ACH children were found (P 0.29). Oral vascular network of the unaffected ACH fathers exhibited a significantly higher complexity than those of the unaffected ACH mothers, with higher vascular density (P=0.0004), D(1-46) (P=0.0002), D (1-15)(P=0.012)and Dmin (P<0.00001), as well as a lower vessel-free area size value (P<0.00001). A vascular network density >10.65% and a median vessel-free area size 56,832 m2 were found to accurately discriminate the unaffected ACH parents from the control parents (Table 2),with adequate model calibration (2 0.02, df = 1, p 0.90). No statistically significant difference between these two AUCs was observed (AUC difference: 0.0025 0.016 [95% CI: 0.004, 0.08]; p=0.10). Conversely, fractal dimensions [ (D(1-46), D (1-15) ] showed lower accuracy as compared to the other network parameters (AUC difference range 0.025 0.016 to 0.038 0.021; p≤ 0.073). DISCUSSION The main findings of this study indicate the presence of a previously unrecognised venous vascular pattern abnormality in the oral mucosa of the unaffected parents of children with FGFR3G380R mutation-associated ACH. This observation can be used as a clinical marker to identify couples potentially at risk for ACH offspring. An aberrant vascularization is a known feature of diagnostic significance in the growth plate of ACH patients4, and FGFR-3G380R transgenic ACH mouse model5. In addition, evidence of markedly dilated retinal veins6 for the cn mice model7 of ACH has been described. Angiogenesis is of crucial importance for the normal development of endochondral bone formation and a delicate balance between the rate of formation of calcified cartilage and its vascularization must be maintained in order for bone development to proceed normally8. On the other hand, little is known about the control of angiogenesis at the growth plate9. Our findings of an abnormal vascularization in ACH patients in anatomical sites different from the growth plate cartilage suggest the presence of ACH-associated mesenchymal changes more generalized than previously thought. A marked paternal age effect is a well-known feature of ACH10 and the predominat paternal origin of new mutations has been documented11. Our observation of a more significant vascular network abnormality in the unaffected ACH fathers compared to the unaffected ACH mothers appears to confirm the importance of a paternal effect in the disease. In the present study, fractal geometry was applied as a tool to assess the oral vascular networks’ complexity. It has been previously shown that fractal dimension (D), and other fractal characteristics can be used to identify abnormal vascular patterns, including corneal12, retinal13, and tumor-associated neovascular growth14,15. The D(1-46) and Dmin results for the vascular networks of the ACH parents and patients dysplay intermediate characteristics from the diffusion-limited aggregation-like16 behaviour of control networks to the percolation-like scaling17 of tumorassociated vascular growth14. 4 A more generally relevant question concerning the forces controlling the spatial arrangement of vascular networks is to be addressed. The supracellular structures of a multicellular organism are essentially the product of a stochastic process under incomplete mechanical restriction, where the constituent units are piled up in an arrangement required from the second law of thermodynamics to minimise the potential energy of the system. This leads to equilibrium space division (ESD), as a general principle of supracellular structures18. As blood vessels are localised predominantly on the edges of ESD, vascular geometry largely depends on ESD, where a uniform centripetal force is generated mostly by the tension of the connective tissue18. Therefore, we speculate that the aberrant oral vascularization observed in the unaffected ACH parents might be related to a hitherto unrecognised, systemic mesenchymal abnormality. The mechanism underlying the observed association between the mesenchymal changes in the parents and the occurrence of ACH in the offspring is currently unknown. The findings of the present study (i) indicate that a previously unrecognised, vascular network pattern abnormality of the oral mucosa is present in the unaffected parents of children with ACH and can provide a useful clinical marker for identifying potential couples potentially at risk for ACH offspring; and (ii) generate the testable hypothesis that geometrical pattern abnormalities of either oral or extra-oral vascular networks may occur in mesenchymal pathology-associated diseases other than ACH. 5 METHODS Subjects Nonconsanguineous, unaffected parents (n=30; M:15, age: 34.6 ± 6.5 years; F:15, age: 31.5 ± 6.3 years) of ACH children with typical phenotype and G-to-A transition at nucleotide 1138 of the FGFR3 gene, a total of 15 unrelated children with sporadic ACH and FGFR3 G380R mutation (M: 9, F: 6; age 6.5 ± 2.2 years ; mean height-SD 0.36 ± 1.01, according to ACH growth charts19) together with a population of 45, genetically unrelated sex- and age-matched control subjects (fathers, age: 34.1 ± 5.6 years, n=15; mothers, age: 30.8 ± 5.5 years, n=15; children, M:9; F:6; age 6.4 ± 2.0 years, n=15) participated to the study. Informed consent was obtained from all the subjects or their parents. The study was approved by the Italian National Association for the study of ACH (A.I.S.ac.). The clinical, biological and demographic data for each subject were obtained by two operators who were unaware of the oral vascular findings. Vascular Network Imaging and Analysis A ~704 mm2–size area (~32 x 22 mm) of the lower vestibular and free gingival oral region was photographed for each subject (1:1 ratio; orthogonal projection) 20,21. This particular anatomical area was selected due to the high-visibility of the vasculature pattern and easy accessibility to photographic documentation. All photographs were taken by a single operator with the use of a Yashica Dental Eye model photocamera equipped with an automated annular flash and a 55 mm, f 1:4 Yashica lens (Yashica-Kyocera Co., Kyoto, Japan). Kodak Elite Chrome 100 ISO/21 DIN films (KodakEastman Kodak Co., Rochester, New York, USA) were used and the positives developed according to the standard E-6 procedure. Direct prints from 35 mm slides were obtained according to the standard Ilfochrome procedure (Ilfochrome-Chugai Photo Chemical Co, Tokyo, Japan). Images were digitised using a HP Scanjet 4C (color resolution: 300 d.p.i.) scanner (Hewlett-Packard, Palo Alto, California, USA), with a Windows ’98 operating system (Microsoft Co., Redmond, Washington, USA). Manual outline of the vascular networks’ trajectories was performed using Adobe Photoshop ver. 5.0 (Adobe Systems Inc., San Jose, California, USA) on a Sony 19” Trinitron Multiscan G420 screen (Sony Co., Tokyo, Japan) (resolution: 16-m/pixel) by two independent operators who were unaware of the subjects clinical findings. Non-readable areas were always <5% of the total digitised image area and were excluded from analysis. The obtained two-dimensional vascular networks were analysed using the Image Pro-Plus ver. 1.3 image analysis software (Image Pro-Plus-Media Cybernetics, Inc., Silver Spring, Maryland, USA). Images were processed to threshold the vessel network without background interference and the networks were subsequently converted into an outline of single pixels. Density of the vessel network and vessel-free area (inter-vessel “islands”) size were determined automatically using the software histogram and counting functions, respectively. A total of 14,169 areas were evaluated (unaffected ACH parents, n=8,105; ACH children, n=2,830; control parents, n= 1,756; and control children, n=1,478). The fractal dimension of the skeletonized images was measured using the box-counting algorithm22 using a software program written by one of the authors. As the natural fractals show upper and lower limits, the local fractal dimension (D) was determined for two regions: box lengths <740 m (pixels 1-46, D(1-46) and <140 m pixels 1-15, D (115). The measuring procedure was calibrated against shapes of known fractal dimension (square, circle and quadric Koch island) with accuracy ± 2 %. The fractal dimension of the minimum path, Dmin, was computed for each vascular cluster from the power law lc = r Dmin, where Dmin is the exponent that governs the dependence of the minimum path length between two points (lc) on the Pythagorean distance (r) between them17.The lc value was determined using the algorithm by Herrmann & Stanley23. The whole procedure was found to be reproducible with mean intra- and interobserver coefficients of variation (CV%) < 5% and <10%, respectively [vascular network density, intra-observer CV%: 4.64 ± 0.85, inter-observer CV% : 9.63 ± 6.16; D (1-46), intra-observer CV%: 0.74 ± 0.51, inter-observer CV% : 1.14 ± 0.70; D(1-15), intra-observer CV%: 2.81 ± 1.39, inter-observer CV% : 3.76 ± 2.32; Dmin, intra-observer CV%: 2.64 ± 1.99 ; inter-observer CV%: 7.52 ± 3.22); and vessel-free area size (A), intra-observer CV%: 3.22 ± 2.51; inter-observer CV%: 5.69 ± 1.41) ( n=6 replicate observations)]. Statistical Analysis Data were expressed as mean ± s.d. for continuous normally distributed data and median with interquartile range [25th and 75th percentiles] for non normal distributions. The t-test or Wilcoxon’s test were used to compare continuous normally distributed data and nonparametric continuous data, respectively. Discrimination (the ability of the model to identify unaffected ACH parents and control parents) was tested using receiver characteristic (ROC) curves and an area under the curve (AUC) value >0.80 was accepted to indicate good discrimination 24. Comparison of the AUCs were evaluated by the DeLong method25. Model calibration was evaluated using 2 to compare the observed frequency with the expected frequency of the unaffected ACH parents according to the examined oral vascular network characteristics. A two-sided P value of <0.05 was considered to be statistically significant, and the Bonferroni corrected significance levels were used for multiple t-tests. Acknowledgements 6 We thank Laura De Felice (helpful discussion and inspiration); Gordon B. Avery, Emeritus Professor of Paediatrics, Children’s Hospital, Washington (critical reading of a preliminary draft of the manuscript); the Cartiera di Crusinallo SPA–Gruppo Favini (help in shape analysis); Alessandra Lombardi, MD and Laura Valdambrini, MD (help in data collection); and all the ACH and control families who accepted to participate in the study and Mrs. Donatella Valerio Sessa on behalf of the the Italian National Association for the study of ACH (A.I.S.ac.). C.D.F. would like to dedicate this paper to his first clinical teacher, Bruna Marchi, MD. 7 REFERENCES 1. Online Mendelian Inheritance in Man, OMIM (TM). Johns Hopkins University, Baltimore, MD. MIM Number: #100800. Date last edited: 5/23/2001. World Wide Web URL: http://www.ncbi.nlm.nih.gov/omim/ 2. Shiang R., Thompson L.M., Zhu Y.-Z., Church D.M., Winokur S.T. & Wasmuth J.J. Mutations in transmembrane domain of FGFR3 cause the most common genetic form of dwarfism, achondroplasia. Cell 78, 335-342 (1994) 3. Iannotti J.P., Goldstein S., Kuhn J. Lipiollo L. & Kaplan F.S. Growth plate and bone development. In: Simon S.R. (ed.), Orthopaedic Basic Science. American Academy of Orthopaedic Surgeons, Rosemont, IL, pp. 185-217 (1994). 4. Rimoin D.L., Hughes G.N., Kaufman R.L., Rosenthal R.E., McAlister W.H. & Silberberg R. Endochondral ossification in achondroplastic dwarfism. N. Engl. J. Med. 183, 728-735 (1970) 5. Segev O., Chumakov I., Nevo Z., Givol D., Madar-Shapiro L., Sheinin Y., Weinreb M. & Yayon A. Restrained chondrocyte proliferation and maturation with abnormal growth plate vascularization and ossification in human FGFR-3G380R transgenic mice. Hum. Mol. Genet. 9, 249-258 (2000) 6. Hawes N.L., Smith R.S., Chang B. Davisson M, Heckenlively J.R. & John S.W.M. Mouse fundus photography and angiography: a catalogue of normal and mutant phenotypes. Mol. Vis. 5, 22 (1999). 7. Doolittle D.P., Davisson M.T., Guidi J.N. & Green M.C. Catalog of mutant genes and polymorphic loci. In: Lyon M.F., Rastan S., Brown S.D.M. (eds.), Genetic Variants and Strains in the Laboratory Mouse. 3rd ed. Oxford: Oxford University Press. pp. 17-854 (1996). 8. Descalzi Cancedda F., Melchiorri A., Benelli R., Gentili C., Masiello L., Campanile G., Cancedda R.. & Albini A. Production of angiogenesis inhibitors and stimulators is modulated by cultured growth plate chondrocytes in vitro differentiation: dependence on extracellular matrix assembly. Eur. J. Cell. Biol. 66, 60-68 (1995) 9. Vu T.H., Shipley J.M., Bergers G., Berger J.E., Helms J.A., Hanahan D., Shapiro S.D., Senior R.M. & Werb Z. MMP-9/gelatinase B is a key regulator of growth plate angiogenesis and apoptosis of hypertrophic chondrocytes. Cell 93, 411-422 (1998) 10. Orioli I.M., Castilla E.E., Scarano G. & Mastroiacovo P. Effect of paternal age in achondroplasia, thanatophoric dysplasia, and osteogenesis imperfecta. Am. J. Med. Genet. 59, 209-217 (1995). 11. Wilkin D.J., Szabo J.K., Cameron R., Henderson S., Bellus G.A., Mack M.L., Kaitila I., Loughlin J., Munnich A., Sykes B., Bonaventure J. & Francomano C.A. Mutations in fibroblast growth-factor receptor 3 in sporadic cases of achondroplasia occur exclusively on the paternally derived chromosome. Am. J. Hum. Genet. 63, 711-716 (1998). 12. Daxter A. & Ettl. Corneal vascularization and its relation to the physical properties of the tissue: a fractal analysis. Curr Eye Res 14, 263-268 (1995). 8 13. Daxter A. The fractal geometry of proliferative diabetic retinopathy: implications for the diagnosis and the process of retinal vasculogenesis. Curr Eye Res 12, 1103-1109 (1993). 14. Gazit Y., Berk D.A., Leunig M., Baxter L.T. & Jain R.K. Scale-invariant behavior and vascular network formation in normal and tumor tissue. Phys. Rev. Lett. 75, 2428-2431 (1995). 15. Gazit Y., Baish J., Safabakhsh N., Leunig M., Baxter L.T. & Jain R.K. Fractal characteristics of tumor vascular architecture during tumor growth and regression. Microcirculation 4, 395-402 (1997). 16. Witten TA, Sander LM.. Diffusion-Limited Aggregation, a kinetic critical phenomenon. Phys. Rev. Lett. 47, 1400-1403 (1981). 17. Meakin P., Majid I., Havlin S., & Stanley H.E. Topological properties of diffusion limited aggregation and cluster-cluster aggregation. J. Phys. A: Math. Gen. 17, L975-L981 (1984). 18. Suwa N. Supracellular structural principle and geometry of blood vessels. Virchows Arch A 390, 161-179 (1981). 19. Horton W.A., Rotter J.L., Rimoin D.L., Scott C.I. & Hall J.G. Standard growth curves for achondroplasia. J. Pediatr. 93, 435-8 (1978). 20. De Felice C, Di Maggio G, Zagordo L, Parrini S, Toti P, Tota G & Bagnoli F. Hypoplastic or absent mandibular frenulum: a new predictive sign of infantile hypertrophic pyloric stenosis. J. Pediatr. 136, 408-410 (2000). 21. De Felice C, Toti P., Di Maggio G., Parrini S. & Bagnoli F. Absence of the inferior labial and lingual frenula in Ehlers-Danlos syndrome. Lancet 357, 1500-1502 (2001). 22. Peitgen H., Jurgens H. & Saupe D. Area and dimension: measuring complexity and scaling properties. In: Chaos and Fractals: New Frontiers of Science. Peitgen H., Jurgens H. & Saupe D. (eds), Springer Verlag: New York. pp. 182-228 (1992). 23. Herrmann H.J. & Stanley H.E. The fractal dimension of the minimum path in two- and threedimensional percolation. J. Phys. A: Math Gen 21, L829-L833 (1988). 24. Hanley J.A. & McNeil B.J. The meaning and use of the area under the receiver operating characteristic (ROC) curve. Radiology 143, 29-36 (1982). 25. DeLong E.R., DeLong D.M. & Clarke-Pearson D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44, 837-845 (1988). 9 Fig. 1 Oral venous plexus vascular networks of the unaffected parents of ACH offspring show a significantly higher complexity than those of control parents. a, Representative skeletonized oral vascular pattern of an unaffected ACH father and b, a control father. Binary forms were generated after conversion from the original networks (photographs of the lower oral vestibulum and free gingival oral region, orthogonal projection; 1:1 ratio). . Table 1 Unaffected ACH parents and ACH children display an abnormal oral vascular network pattern Fathers ACH (n=15) Density (%) D [1-46] D [1-15] Dmin 13.48 ± 0.72 1.84 ± 0.02 1.41 ± 0.05 1.31 ± 0.08 Vessel-free size (m2) area 30,720 [29,696-32,256] Controls (n=15) 7.05 ± 2.39 1.59 ± 0.15 1.13 ± 0.11 1.07 ± 0.04 P<0.00001 P<0.00001 P<0.00001 P<0.00001 Mothers ACH (n=15) 12.37 ± 0.80 1.78 ± 0.05 1.35 ± 0.07 1.16 ± 0.07 Controls(n=15) 7.25 ± 2.07 1.60 ± 0.12 1.14 ± 0.09 1.09 ± 0.03 100,864 [87,188-116,480] P<0.00001 37,376 [29,696-35,462] P<0.00001 P<0.00001 P<0.00001 P=0.0013 Children ACH (n=15) 13.45 ± 1.07 1.82 ± 0.07 1.40 ± 0.08 1.33 ± 0.07 Controls (n=15) 11.35 ± 1.06 1.77 ± 0.02 1.28 ± 0.12 1.14 ± 0.11 P<0.00001 P=0.013 P=0.0032 P<0.00001 126,208 [113,920139,776] P<0.00001 30,720 [29,184-32,256] 89,715 [84,454-94,973] P<0.00001 Data are presented as mean ± s.d. with the exception of vessel-free area size in which median with interquartile range are used. Statistical analysis was performed with a two-tailed, paired, Student’s t-test, with the exception of vessel-free area size in which a two-tailed Wilcoxon test was used. 10 Table 2 Low vessel-free area size and high vascular network density accurately discriminate between unaffected ACH parents from control parents Variable Density (%) D (1-46) D (1-15) Vessel-free area size (m2) Cut-off AUC ± s.e.m. Sensitivity (%) Specificity (%) Criterion (95% C.I.) (95% C.I. ) (95% C.I.) > 10.85 0.998 ± 0.006 97.1 100 (0.936-1.0) (85.0-99.5) 0.959 ± 0.025 85.7 92.6 (0.875-0.993) (69.7-95.1) (80.3-99.4) 0.973 ± 0.020 88.6 96.2 (0.894-0.996) (73.2-96.7) (80.3-99.4) 1.0 100 100 > 1.75 > 1.28 56,832 Data are the result of a receiver-operating characteristic curve analysis 11 Corresponding Author: Claudio De Felice, MD, U.O. Terapia Intensiva Neonatale, Sezione di Pediatria Preventiva e Neonatologia, Dipartimento di Pediatria Ostetricia e Medicina della Riproduzione, Azienda Ospedaliera Senese, Viale M. Bracci 16, I-53100 Siena, Italy. Phone: +39 0577 586542; Fax:+39 0577 586155; e-mail: defelice.claudio@libero.it 12 13